
Quiz 1 Ep13
20) Patient de 34 ans est admis aux urgences ce matin pour accident de la circulation. Il a son coude gauche gonflé et sa main gauche est soutenue par sa main droite. Toute tentative de mobilisation provoque de douleur intense et un bruit de craquement. Radiographie montre fracture supra-condylienne de l’humérus gauche. Concernant son traitement orthopédique, quelle est la complication souvent rencontrée par une immobilisation en hyper flexion?
Paralysie du nerf radial
Paralysie du nerf cubital
Paralysie du nerf médian
Syndrome de Volkmann
Consolidation vicieuse
21) Une femme âgée de 35 ans, droitier a senti une douleur latérale du coude gauche après avoir nettoyé un sous-sol inondé et fait essorage des chiffons imbibés d'eau. Les résultats de la radiographie sont négatifs. Il y a une douleur et un légère gonflement sur l'épicondyle latéral de l'humérus. Anatomiquement, cette condition peut être expliqué par lequel des éléments suivants?
Entorse du ligament collatéral latéral du coude
Rupture du muscle triceps
Tendinite de l'extenseur du poignet
Synovite de l'articulation du coude gauche
Rupture du muscle rond pronateur
22) Un homme de 40 ans est admis aux urgences ce matin pour accident par chute sur la main en l’extension. A l’examen Clinique toute tentative de mobilisation provoque de douleur, élargissement du coude dans le sens antéro-postérieur, raccourcissement apparent de l’avant bras et saillie de l’olécrane en arrière, pas d’ echomose .Quel est le diagnostic le plus probable?
Fracture supra-condylien de l’humérus
Luxations postérieure du coude
Luxation antérieure du coude
Fracture de l’olécrane
Fracture de la tête radiale
23) Un homme de 40 ans est admis aux urgences ce matin pour accident par chute sur la main gauche en l’extension. A l’examen clinique, avant bras en l’extension, mobilisation provoque de douleur, élargissement du coude dans le sens antéro- postérieur, raccourcissement apparent de l’avant bras et saillie de l’olécrane en arrière. Résultats radiographie aux urgences est luxation du coude gauche. Parmi les variétés des luxations du coude suivantes, quelle est la plus fréquente?
Antérieure
Latérale interne
Latérale externe
Luxations divergentes
Postérieure
24) Un homme de 40 ans est admis aux urgences ce matin pour accident par chute sur la main gauche en’ extension. A l’examen clinique, avant bras en l’extension, mobilisation provoque de douleur, élargissement du coude dans le sens antéro- postérieur, raccourcissement apparent de l’avant bras et saillie de l’olécrane en arrière. Résultats radiographie aux urgences est luxation postérieur du coude gauche. Quel est la complication la plus souvante rencontrée?
Syndrome de volkmann
Ostéome post-traumatique du coude
Raideur post-traumatique
Arthrite septique
Syndrôme algodystrophique
25) Un homme de 40 ans est admis aux urgences ce matin pour accident par chute sur la main gauche en l’extension. A l’examen clinique, avant bras en extension, mobilisation provoque de douleur, élargissement du coude dans le sens antéro- postérieur, raccourcissement apparent de l’avant bras et saillie de l’olécrane en arrière. Résultats radiographie aux urgences est la luxation postérieur du coude gauche. La réduction est indiquée en urgence mais elle est incoercible. Quelle est la lésion associée?
Fracture du col du radius
Fracture de l’apophyse coronoïde
Fracture de l’apophyse coracoïde
Rupture du ligament collatérale ulnaire
Rupture du ligament collatérale radial
26) Une femme de 35 ans vient aux urgences pour douleur du coude droite, œdème et impotence fonctionnelle du membre supérieure droit. Ce patient, sans antécédents particulier, est tombé sur le coude droit au cours de montée de l’ escalier. Résultats de la radiographie aux urgences est la fracture de l’olécrane droit. Une proposition sur le signe clinique est correcte, laquelle?
Crépitation du coude à la palpation
Prono-supination de l’avant bras est impossible
Flexion active de l’avant bras est impossible
Extension active de l’avant bras est impossible
Ecchymose n’est pas importante
27) Une femme de 35 ans vient aux urgences pour douleur du coude droite, œdème et impotence fonctionnelle du membre supérieure droit à la suite de glissement au cours de monter l’ escalier et est tombé sur le coude droit. Le résultats de la radiographie aux urgences est fracture type II de l’olécrane droit. Parmi les propositions suivantes, une proposition est correcte, laquelle ?
Fracture comminutive, non déplacé
Fracture simple, avec luxation du coude en avant
Fracture comminutive instable
Fracture déplacée avec luxation du coude
Fracture déplacée de l’ olécrâne mais stable
28) Un jeune homme âgé de 20 ans vient aux urgences pour douleurs, déformation de l’avant bras gauche après accident de la voie publique, le résultats de la radiographie est fracture du tiers moyen des deux os de l’avant bras gauche très déplacée. L’ indication thérapeutique est chirurgicale par le fixateur externe. Quel est le diagnostic le plus appropriée pour ce patient?
Fractures avec lésions musculaires et cutanées septiques
Fractures ouvertes type II
Fractures ouverte type IIIA
Fractures à double foyer,
Fractures avec fragment intermédiaire
29) Un jeune homme âgé de 20 ans vient aux urgences pour douleurs, déformation de l’avant bras gauche après accident de la voie publique, résultats de la radiographie est la fracture du tiers moyen des deux os de l’avant bras gauche très déplacée. L’ indication thérapeutique est chirurgicale mais le patient refuse notre traitement. Quelle est la complication tardive le plus fréquence rencontrée?
Raideur du poignet
Raideur du coude
Syndrome algodystrophique
Trouble de prono-supination
Pseudarthrose
30) Une femme âgée de 40 ans, chute sur la terrasse avec une main droite en hyper- extension. Juste après, un gonflement et une douleur du poignet apparaissent rapidement, les radiographies du poignet droit en d'urgence sont negatives. L’ IRM du poignet droite montre une fracture du scaphoïde. Quel est le signe clinique qu’ il faut rechercher?
Douleur à la flexion du pouce
Douleur à l’extension du pouce
Douleur à la pression sur la base du premier métacarpien
Douleur à la pression sur tabatière anatomique
Crépitation au mouvement du pouce
31) Une femme âgée de 40 ans, chute sur la terrasse avec une main droite en hyper- extension. Juste après, un gonflement et une douleur du poignet apparaissent rapidement, les radiographies du poignet droit en d'urgence sont negatives. Le diagnostic est fracture du scaphoïde après avoir refait des radiographies de contrôle du poignet au 14em jours. Un an plutard, le patient présente de l’ arthrose du poignet droit. Quel est le facteur le plus souvent favorise d’évolution vers l’arthrose du scaphoïde?
Fracture non déplacée
Fracture du 1/3 moyen
Fracture avec désaxation
Fracture du pole inférieur
Fracture du pole supérieur
32) Une femme âgée de 42 ans est entrée au service urgence après un traumatisme violence du poignet gauche. La radiographie montre une luxation antérieure du semilunaire. Quel est le signe clinique qui montre une luxation antérieure du semi-lunaire?
Impotence fonctionnelle du poignet
Comblement de la tabatière anatomique
Raccourcissement de la hauteur du poignet
Paresthésies palmer du 1er, 2ème et 3ème doigt
Paresthésie dorsale du 1er commissure
33) A 12 years old boy receiving long term treatment for spring catarrh, developed defective vision in both eyes. The likely cause is?
. Posterior subcapsular cataract
. Retinopathy of prematurity
. Optic neuritis
. Vitreous hemorrhage
. Acute anterior uveitis
34) A young child suffering from fever and sore throat began to complain of lacrimation. On examination, follicles were found in the lower palpebral conjunctiva with tender preauricular lymph nodes. The most probable diagnosis is?
. Trachoma
. Staphylococal conjunctivitis
. Adenoviral conjunctivitis
. Phlyctenular conjunctivitis
Streptococal conjuntivitis
35) A female patient 18 years old, who is contact lens wearer since two years, is complaining of redness, lacrimation and foreign body sensation of both eyes. On examination, visual acuity was 6/6 with negative fluorescein test. The expected diagnosis can be?
. Acute anterior uveitis
. Giant papillary conjunctivitis
. Bacterial corneal ulcer
Acute congestive glaucoma
. Staphylococal conjunctivitis
36) A 30 years old male presents with a history of injury to the eye with a leaf 5 days ago and pain, photophobia and redness of the eye for 2 days. What would be the most likely pathology?
. Anterior uveitis
. Conjunctivitis
. Fungal corneal ulcer
. Corneal laceration
. Bacterial corneal ulcer
37) After 48 hours of a cataract extraction operation, a patient complained of ocular pain and visual loss. On examination, this eye looked red with ciliary injection, corneal oedema and absent red reflex. The first suspicion must be?
. Secondary glaucoma
. Anterior uveitis
. Bacterial endophthalmitis
. Acute conjunctivitis
. Corneal laceration
38) A one-month old baby is brought with complaints of photophobia and watering. Clinical examination shows normal tear passages and clear but large cornea. The most likely diagnosis is?
. Congenital dacryocystitis
. Interstitial keratitis
. Keratoconus
Buphthalmos
. Corneal laceration
39) A young patient with sudden painless loss of vision, with systolic murmur and ocular examination reveals a cherry red spot with clear AC, the likely diagnosis is?
. Central Retinal Artery Occlusion
. Central Retinal Vein Occlusion
. Diabetes Mellitus
. Branch Retinal Vein Occlusion
. Optic neuritis
40) A patient of old standing diabetes mellitus noticed sudden muscae volitanes. On examination, the red reflex was dim, with no details of fundus could be seen. He might have?
. Non proliferative diabetic retinopathy
. Cystoid macular edema
. Vitreous hemorrhage
. Central retinal vein occlusion
. Optic neuritis
41) Un enfant de 6 ans est vu en consultation parce qu’il présente une médiocre vision découverte par la médecine scolaire. L’interrogatoire précise qu’il présente une photophobie. La vision n’est pas ameliorable à plus de 3/10 de chaque oeil de loin. L’hospitalisation est décidée parce qu’il suit mal sa scolarité. Quel diagnostic doit être envisagé ?
. Glaucome congénital.
cataracte congénitale
. Tumeur chiasmatique.
. décollement de rétine.
. rétinoblastome.
42) Vous êtes amené à voir en garde une femme de 70 ans pour des céphalées sus orbitaires violentes, s’accompagnant de vomissements et d’un état de choc modéré. La patiente se plaint de ne plus voir d’un oeil brutalement depuis quelques heures. A l’examen, cet oeil est rouge de facon diffuse. Ces seuls signes orientent vers ?
. Une occlusion intestinale.
. Une méningite bactérienne.
. Une crise de glaucome aigu.
. Une névralgie faciale.
. Aucune des propositions précédentes.
43) Vous diagnostiquez une crise de glaucome aigu par fermeture de l’angle chez une femme de 75 ans. Parmi les éléments cliniques suivants, un seul ne fait pas partie de la crise de glaucome aigu. Lequel?
. céphalée unilatérale
. Rougeur péricornéenne
. cataracte
. Hypertonie oculaire
. Baisse de l’acuité visuelle
44) Un homme de 17 ans consulte pour une surdité unilatérale droite. On découvre une otite séreuse droite et des adénopathies cervicales bilatérales. Quel diagnostic doit être évoqué ?
. Carcinome de l’oreille moyenne
. Carcinome indifférencié du cavum
. Carcinome de la base de la langue
. Zona auriculaire
. Polypose naso-sinusienne
45) Une femme de 60 ans présente au niveau d’une hémiface des douleurs très violents déclenchée par pense la tête en avant, rhinorrhée purulent gauche. Quel diagnostic évoquezvous?
. Une sinusite aigue maxillaire gauche
. Une sinusite chronique maxillaire gauche
. Une polypose naso-sinusienne
. Rhinite allergique
. Pansinusite chronique
46) Un enfant de 3 ans présente une rhinorrhée muco-purulente permanente bilatérale, une obstruction nasale avec ronflement nocturne, une respiration bouche ouverte et a présenté trois otites aiguës dans les 2 derniers mois. Quel diagnostic envisager?
. Sinusite maxillaire
. Adénoïdite chronique
. Imperforation choanale
. Corps d’étranger
. Ethmoïdite
47) Un adulte de 50 ans présente une obstruction nasale progressive accompagnée d'épistaxis récidivantes. Quel diagnostic doit-on envisager ?
. Végétations adénoïdes
. Ectasie de la tache vasculaire
. Polypose nasale
. Fibrome naso-pharyngien
. Tumeur de l'ethmoïde
48) Un barman de 60 ans, gros fumeur, est enroué depuis 4 semaines, se racle la gorge continuellement, à une sensation de corps étranger intralaryngé. Quelle est l’affection la plus probable ?
. Diverticule de l’hypopharynx
. Paralysie récurrentielle
. Carcinome du larynx
. Goître
. Laryngite
49) Un stridor inspiratoire passager, sans toux et sans fièvre peut être dû, chez un nourrisson, à une ?
. Fistule trachéobronchique
. Trachéobronchite
. Trachéomalacie
. Asthme
. Laryngomalacie
50) Un jeune garçon de 6 ans, sans antécédents pathologiques, est amené par ses parents pour une dysphonie datant de quelques semaines etqui s’est nettement aggravée après la rentrée scolaire. Il n’y a pas de dyspnée et l’examen fait par le médecin généraliste est normal. Parmi les cinq prépositions suivantes, quel est celle que vous retenez en premier ?
. Epiglottite chronique
. Angiome sous-glottique
. Paralysie récurrentielle
. Papillomatose laryngée
. Dysphonie fonctionnelle
51) Un enfant de 2 ans présente une dyspnée inspiratoire avec tirage et température à 40°C, abondante salivation. Toute tentative pour l’allonger aggrave sa dyspnée. Quel diagnostic évoquez-vous ?
. Angine
. Laryngite sous-glottique
. Pneumopathie
. Épiglottite
. Asthme à commande infectieuse
52) Un enfant de 4 ans est hospitalisé en raison d’un état asphyxique par dyspnée laryngée. Vous êtes frappé par le refus de l’enfant de se mettre en décubitus dorsal. Quel en est, probablement, la cause ?
. Laryngite striduleuse
. Aucune de ces prépositions
. Corps étranger laryngé
. Epiglottite aiguë
. Laryngite sous-glottite
53) Un homme de 50 ans, suite à une chute sur le verglas, a présenté une fracture métaphysaire inférieure du radius avec déplacement de type de Goyrand-Smith. Cette fracture a été réduite sous anesthésie locorégionale et immobilisée à l'aide d'une attelle plâtrée maintenant le poignet en extension modérée. Dans les jours qui suivent, il se plaint progressivement de douleurs dans les doigts et de dysesthésies. L'extension complète des doigts reste possible et peu douloureuse. Les symptômes sont plus marqués la nuit. Quel diagnostic évoquez-vous d'abord ?
. Un syndrome de Volkman
. Un syndrome du canal carpien
. Un syndrome du canal de Guyon
. Une lésion nerveuse lors de l'anesthésie locorégionale par infiltration du plexus brachial
. Une névralgie cervico-brachiale favorisée par un étirement du plexus brachial
54) Un enfant de 2 ans mesurant 70 cm se présente à la salle d'urgence avec une fracture du fémur à la suite d'une chute banale de sa hauteur. A l'examen clinique vous remarquez une coloration bleue des sclérotiques et une hyper laxité ligamentaire. Le diagnostic que vous évoquez est ?
Un rachitisme
. Une ostéodystrophie rénale
. Une maladie de Marfan
. Une ostéopétrose idiopathique juvénile
. Une ostéogenesis imperfecta
55) Un enfant de 10 mois vous est montré pour une cyphose thoraco-lombaire proéminente. En plus de la cyphose, l'examen révèle un nanisme rhizomélique (membres courts, tronc quasi normal). Le diagnostic évoqué est ?
. Maladie de Lobstein
. Dysplasie fibreuse
. achondroplasie
. rachitisme
. Nanisme hypophysaire
56) A la suite d'une chute sur le menton, un patient présente une limitation douloureuse d'ouverture buccale avec impossibilité d'avancer la mandibule et une béance incisive. Le diagnostic est ?
Fracture de l'os hyoïde
Fracture symphysaire
Disjonction crâniofaciale
Fracture sous-condylienne bilatérale de la mandibule
Fracture des apophyses coronoïdes
57) Une femme de 50 ans présente depuis plusieurs années une tuméfaction sous maxillaire évoluant par poussées. L'interrogatoire révèle la notion d'épisodes aigus avec tumefaction douloureuse et inflammatoire. Parfois, une tumefaction apparait au cours du repas. Qu'évoquezvous?
Lithiase de la glande sous-maxillaire
Parotidite chronique
Adénite inflammatoire
Infections récidivantes d'un kyste apical dentaire
Adénome pléimorphe
58) Une fille âgée de 6 mois a présenté une infection urinaire. L’échographie de l’abdomen a montré une dilatation de l’uretère droite avec une dilatation pyélique. La cystographie retrograde réalisée après la stérilité des urines est normale. Quel le diagnostique probable évoquez vous?
. La maladie de jonction pyélo-urétérale
. Mégauretère primitive
. Reflux vésico-urétéral
. Duplicité urétérale
. Valve de l’urètre postérieur
59) Une fille âgée de 3 ans a présenté une infection urinaire. L’échographie de l’abdomen a montré une dilatation de l’uretère droite totale. Le parenchyme rénal est normal. La cystographie retrograde ne trouve pas l’anomalie. Quel EST le diagnostique?
. La maladie de jonction pyélo-urétérale
. Mégauretère primitive
Reflux vésico-urétéral
. Duplicité urétérale
. Valve de l’urètre postérieur
60) Une fille âgée de 3 ans a présenté une infection urinaire. L’échographie de l’abdomen a montré une dilatation de l’uretère droite totale. Le parenchyme rénal est normal. L’urographie intraveineuse est normale. Quel est le diagnostic?
. La maladie de jonction pyélo-urétérale
. Mégauretère primitive
. Reflux vésico-urétéral
. Duplicité urétérale
. Valve de l’urètre postérieur
61) A 28 days old male newborn presents with nonbilious vomiting. One week ago, he weighed 4 kg; his current weight is 3.6 kg. On examination his anterior fontanelle is flattened and his mucous membranes are dry. Between episodes of crying an olive-sized epigastric mass is palpable. Laboratory data include: Na 133. K 3.6 CI 93, CO2 28, and capillary pH 7.51. The most likely diagnosis is?
. Meningitis
. Hypertrophic pyloric stenosis
. Antral web
. Intestinal atresia
. Hiatal hernia
1) Quelle est la proposition la plus correcte devant un cancer obstructif du colon sigmoide chez un home de 65 ans?
. Admis le patient au service de chirurgie et completer le bilan d’extention et attend la decision de reunion multidisciplinaire
. Faire la sigmoidectomie et anastomose colo-rectale en premier temps
. Completer le bilan preoperatoire et bilan d’extention, puis transferer le patient au bloc pour faire la sigmoidectomy et colostomie terminale gauche
. Demander la coloscopie total et biopsie de la masse tumorale pour l’examen anatomopathologique
. Admis le patient au service de reanimation et traitement medical
2) Un patient de 75 ans a subi une cholécystectomie il y a un an.On découvre maintenant un calcul cholédocien résiduel de 7 mm.Quel est le traitement que vous proposeriez parmi les propositions suivantes?
. Réintervention pour cholédocotomie et extraction calcul
. Sphintérotomie endoscopique
. Lthotrithie extra-corporelle
. Traitement medical par Ursolvan
. Pas de traitement
3) Chez une femme de 40 ans ayant fait une première crise de colique hépatique régressive sous traitement symptomatique, l'échographie abdominale montre une lithiase vésiculaire simple. Quelle est la conduite à tenir?
. La prise régulière de Spasfon
un traitement dissolvant par l'acide ursodésoxycholique (Delursan 250 3 cp/j) pendant 6 mois
. Un cathétérisme rétrograde avec sphinctérotomie endoscopique
. Une cholécystectomie
. L'abstention thérapeutique
4) A l'occasion d'un syndrome douloureux de l'hypochondre droit chez une femme de 30 ans en excellent état général, vous découvrez une lithiase biliaire vésiculaire à l'échographie. En cholécystographie, la vésicule est perméable, les calculs font entre 5 et 8 mm. Que pensez-vous devoir proposer?
. Rien
. Un traitement cholérétique
. Un traitement dissolvant par l'acide ursodésoxycholique
. Une cholécystectomie
. Un régime hypocholestérolemiant
5) Une femme de 56 ans, sans antécédents notables, présente des crises de colique hépatique qui se répètent de façon rapprochée. Un cliché de l'abdomen sans préparation montre trois images radio-opaques dont l'échographie confirme qu'il s'agit de calculs mobiles dans la vésicule biliaire?
. Vous conseillez une cholécystectomie
. Vous prescrivez une cure d'acide ursodésoxycholique
. Vous proposez une sphinctérotomie endoscopique
. Vous prescrivez une antibiothérapie et un régime
. Vous conseillez l'abstention de toute thérapeutique
6) Chez une patiente de 35 ans, en bon état général, jamais opérée et présentant deux calculs dans la VBP, totalement asymptomatique, quelle est la meilleure attitude à adopter ?
. Abstention et surveillance
. Traitement dissolvant par acide ursodésoxycholique
. Cholécystectomie+ extraction des calculs de la voie biliaire principale par cholédocotomie
. Sphinctérotomie endoscopique
. Cholédocotomie avec extraction des calculs

7) Une femme âgée de 72 ans est présentée aux Urgences pour une douleur de l’aine droite, suite à une chute de sa hauteur il y a une semaine. Comme ATCD, elle est sous traitement antihypertenseur depuis des années. A domicile, elle a été traitée par médicaments antalgiques et AINS et la douleur est calmée de manière intermittente. La raisons pour laquelle elle a été emmenée à hôpital. L’examen clinique révèle une douleur intense de la hanche droite avec impotence fonctionnelle du membre. Il est en position de rotation externe et adduction avec raccourcissement de 4cm. La radiographie du bassin a été faite. Le moyen de traitement pour cette patiente a Fracture du col fémoral?
. Extension continue
. Prothèse céphalique
. Fixateur externe
. Vissage percutané par 3 vis
. Plaque DHS
8) Quelle est la méthode thérapeutique de choix chez un sujet de 30 ans présentant une fracture déplacée du col fémoral en coxa vara?
Réduction orthopédique et immobilisation plâtrée
. Ostéosynthèse par 3 vis
. Ostéosynthèse par clou-plaque
. Prothèse d'emblée
. Ostéosynthèse par clous de Ender
9) Un homme de 28 ans a subi un traumatisme du bassin. Il a été transféré immédiatement au service d’accueil urgent de votre l’hôpital. Sa conscience est conservée. Ces signes vitaux sont stables. Il présente une petite hématurie macroscopique. Quel est votre geste à faire face à ce symptôme?
. Mise en place d’un sondage urinaire
. Urographie intraveineuse en urgence
. Scanner abdominal et bassin pour trouver la lésion
. Surveillance de la coloration d’urine et diurèse
. Prévoir d’une transfusion sanguine
10) Un homme de 34 ans a fait une fracture du bassin avec une hématurie. Une mise de sondage vésical est impossible. Quel est votre geste à faire en ce moment?
. Remettre un sondage rigide
. Surveillance de l’urination
. Glaçage s’il y a un globe vésical
. Cystostomie
. Urétéroscopie
11) Une jeune femme de 25ans est entrée pour un traumatisme du bassin avec état de choc. Après un certain remplissage, la tension artérielle est devenue stable. Un examen radiologique urgent montre une disjonction de la symphyse pubienne de 5 cm. Quelle est votre conduite thérapeutique?
. Ostéosynthèse par plaque vissée
. Continuer remplissage vasculaire
. Abstention chirurgicale
. Extension continue
. Fixateur externe de fermeture
12) Un jeune homme de 34 ans est transféré de province de Banteay Meanchey pour une fracture ouverte de jambe droite causée par accident de la voie publique. L’accident s’est déroulé il y a 12 heures et il est transféré directement à l’hôpital. L’examen clinique révèle un délabrement très importent des parties molles avec exposition osseuse au niveau de la jambe droite. Il y a une grande plaie environ 8cm, lésions extensives de masse musculaire avec presence de débris de terre dans la plaie. Les pouls distaux sont perceptibles, la radiographie montre une fracture au 1/3 moyen avec petite comminution osseuse et déplacement en chevauchement. La classificatrion est Gustilo Type IIb. Les Principes de traitement de ce type de fracture sont suivants, sauf une?
. Parage chirurgical de plaie et fixation osseuse
. Aponévrotomie
. Urgence chirurgicale
. Antibiothérapie
. Prévention de tétanos
13) Un jeune homme de 34 ans est transféré de province de Banteay Meanchey pour une fracture ouverte de jambe droite causée par accident de la voie publique. L’accident s’est déroulé il y a 12 heures et il est transféré directement à l’hôpital. L’examen clinique révèle un délabrement très importent des parties molles avec exposition osseuse au niveau de la jambe droite. Il y a une grande plaie environ 8cm, lésions extensives de masse musculaire avec presence de débris de terre dans la plaie. Les pouls distaux sont perceptibles, la radiographie montre une fracture au 1/3 moyen avec petite comminution osseuse et déplacement en chevauchement. Le moyen d’immobilisation osseuse le plus adapté pour ce patient est?
Plâtre cruro-pédieux
. Fixateur externe
. Enclouage centromédullaire
. Plaque vissée
. Extension continue
14) Un jeune l’homme de 20 ans, ayant un accident par chute sur le moignon de l’épaule gauche, une impotence fonctionnelle du membre supérieur gauche avec attitude vicieuse. Radiographie montre une fracture de la clavicule gauche avec chevauchement minime. Pour ce patient l’indication est le traitement orthopédique, quelle est la proposition le plus raisonnable pour cette indication?
Le déplacement n’est pas important
La consolidation avec des cals vicieuses moins fréquentes
La consolidation avec moins de pseudarthrose
Bonne fonctionnement après la consolidation vicieuse
Par de risqué d’infection
15) Un jeune l’homme de 20 ans, ayant un accident par chute sur le moignon de l’épaule gauche. Après l’ accident il a très mal de l’épaule gauche, impotence fonctionnelle du membre supérieur gauche avec attitude vicieuse, et à l’inspection un fragment fracturaire de la clavicule est basculé en haut. Radiographie montre une fracture de la clavicule gauche avec chevauchement importance (3cm). L’indication pour ce patient est d’ostéosynthèse. Quel type d’ostéosynthèse indquez –vous pour avoir une contention solide pour ce patient?
Embrochage centro-médulaire
Cerclage
Vissage
Plaque vissé
Enclouage centromédullaire
16) Un patient âgé de 35ans admis en urgent à la suite de l’accident de la voie publique. Il est en attitude du blesse du membre supérieur gauche, une épaule gonflée ecchymotique et parfaitement conscience. Il nous explique que le choc a été brutalement touché sur l’épaule gauche. Radiographie montre une fracture de l’extrémité supérieur de l’humérus gauche de type de NEER III. Concernant l’indication thérapeutique, quel est le traitement le plus approprié?
Chirurgie par broches
Orthopédique par bandage
Chirurgie par plaque vissée
Chirurgie par fixateur externe
Prothèse inversée
17) Un l’homme de 35 ans vient au service urgente pour la douleur, déformation et une plaie du bras gauche après l’ accident de la voie publique, résultats de la radiographie du bras gauche montre une fracture comminutive du tiers moyen de l’humérus gauche. Ce patient a subit un traitement orthopédique. Concernant le traitement orthopédique, parmi les propositions suivantes, laquelle la plus raisonnable?
Plâtre thoraco-brachial est confortable pour le patient
Plâtre pendant est mis sur le patient alité
Immobilisation du member atteint est de 9 semaines
Le résultat du traitement orthopédique est rarement bon
Extension continue au zenith pour la fracture comminutive
18) Un l’homme 35 ans vient au service urgente pour douleurs, déformation du bras gauche après accident du voie public. Le résultat de la radiographie du bras gauche montre une fracture du tiers moyen de l’humérus gauche très déplacée. L’ indication chirurgicale est posée. Concernant cette indication, parmi les propositions suivantes, une est plus correcte, laquelle?
Pour permettre une mobilisation précoce
Pour éviter de cal vicieux
Pour permettre une réduction anatomique
Pour éviter les complications nerveuses
Pour éviter le dépériostage
19) Patient de 34 ans est admis aux urgences ce matin pour l’ accident de la circulation. Il a son coude gauche gonflé et sa main gauche est soutenue par sa main droite. Toute tentative de mobilisation provoque de douleur intense et un bruit de craquement. Radiographie montre fracture supra-condylienne de l’humérus gauche. Concernant le traitement chirurgical, parmi les propositions suivantes, une est exacte, laquelle?
Voie d’ abord la plus souvent est médiale
Voie d’ abord la plus soulante est latérale
La voie d’ abord la plus souvent utilisée est médiane postérieure
Embrochage et haubanage est utilisé
Repérer le nerf médian au niveau de la gouttière épitrochléo-olécrânien
20) Patient de 34 ans est admis aux urgences ce matin pour accident de la circulation. Il a son coude gauche gonflé et sa main gauche est soutenue par sa main droite. Toute tentative de mobilisation provoque de douleur intense et un bruit de craquement. Radiographie montre une fracture supra-condylienne de l’humérus gauche sans déplacée. Le traitement orthopédique est la mise une gouttière plâtrée postérieure. Quelle est la durée la plus convenable?
3 à 4semaines
7 à 8 semaines
4 à 5semaine
5 à 6semaines
6 à 7semaines
21) Un homme de 35 ans vient aux urgences pour douleur du coude droite, œdème et impossible extension active de l’avant bras droit, après chute sur son coude. La radiographie montre une fracture du tiers moyen de l’ olécrâne à sa partie moyen. Quel est le moyen de traitement chirurgical le plus approprié?
Haubannage pour la fracture transverse
Vissage pour la fracture comminutive
Plaque vissée pour la fracture à trait transverse
Olécraniectomie pour la fracture de la base de l’olécrâne
Vissage appuyé pour la fracture comminutive
22) Un jeune homme âgé de 20 ans vient aux urgences pour douleurs, déformation de l’avant bras gauche après accident de la voie public, résultats du radiographie est une fracture d’un tiers moyen des deux os de l’avant bras gauche très déplacée. L’ indication therapeutique est chirurgicale. Concernant l’indication du traitement, parmi les propositions suivantes, laquelle est la plus appropriée?
Plaque vissé pour le radius et cubitus
Embrochage pour le radius et cubitus
Fixateur externe pour les radius et cubitus
Plaque vissé du radius et embrochage de cubitus
Embrochage du radius et plaque vissée du cubitus
23) Un garçon âgé de 10 ans vient aux urgences pour douleurs, déformation de l’avant bras gauche après accident de la voie publique, résultats de la radiographie est une fracture du tiers moyen des deux os de l’avant bras gauche non déplacée. L’ indication therapeutique est orthopédique. Concernant l’indication du traitement, parmi les propositions suivantes, laquelle est la plus appropriée?
Plâtre antibrachial palmaire
Immobilisation de l’épaule et du coude
Immobilisation de l’épaule et du poignet
Durée d’immobilisation est de 3 semaines
Plâtre brachio-antibrachial palmer
24) Un garçon âgé de 10 ans vient aux urgences pour douleurs, déformation de l’avant bras gauche après accident du voie public. Le résultats du radiographie est la fracture du tiers moyedes deux os de l’avant bras gauche très déplacée avec des traits de fracture transverses. L’ indication du thraitement est chirurgicale. Concernant l’indication therapeutique, parmi les propositions suivantes, laquelle est la plus appropriée?
Plaque vissé pour le radius et cubitus
Embrochage pour le radius et cubitus
Fixateur externe pour les radius et cubitus
Plaque vissé du radius et embrochage de cubitus
Embrochage du radius et plaque vissée du cubitus
25) Un jeune homme âgé de 20 ans vient aux urgences pour douleurs, déformation de l’avant bras gauche après accident de la voie publique, résultats du radiographie est une fracture des deux os de l’avant bras gauche très déplacée. L’ indication thérapeutique est chirurgicale et la voie d’ bord est antérieure de HENRY pour le radius. Concernant l’indication du traitement, parmi les propositions suivantes, laquelle est la plus appropriée?
Fracture du col du radius et tête cubitale
Fracture proximale des 2 os de l’avant bras
Fracture du 1/3 inférieur de la diaphyse radiale et 1/3 moyen de la diaphyse cubitale
Fracture proximale du cubitus et fracture de la tête radiale
Fracture du 1/3 moyen de la diaphyse cubital et 1/3 supérieur de la diaphyse du radius
26) Un jeune homme âgé de 20 ans vient aux urgences pour douleurs, déformation de l’avant bras gauche après accident de la voie publique, résultats du radiographie est fracture du tiers moyen des deux os de l’avant bras gauche très déplacée. L’ indication thérapeitique est chirurgicale et la voie d’ abord est antérieur de HENRY. Concernant l’indication du traitement, quelle est la proposition la plus appropriée?
La voie d’ abord entre premier radial et le deuxième radial
La voie d’ abord entre fléchisseur propre du pouce et le fléchisseur commun profond des doigts
La voie d’ abord entre le premier radial et le fléchisseur commun superficiel des doigts
La voie d’ abord entre le long supinateur et le grand palmer
La voie d’ abord entre le grand palmer et le petit palmer
27) Une dame âgée de 40 ans, femme de ménage, chute sur la terrasse avec une main en hyperextension. Juste après, un gonflement et une douleur du poignet apparaissent rapidement, mais les radiographies en 'urgence sont négatives. En plus, il y a limitation de flexion dorsale du poignet et de flexion palmaire ainsi qu’une douleur au niveau de la tabatière anatomique à la base du pouce. Quel est la conduite thérapeutique le plus approprié?
Appliquer une gouttière plâtrée du poignet pendant 4 jours jusqu'à l’œdème et la douleur au poignet est diminuées
Appliquer un plâtre au poignet et refaire des radiographies contrôle du poignet au 14ème jours
. Appliquer un plâtre au poignet pendant 8 semaines
Appliquer un orthèse au poignet et retirez tous les jours pour faire de mouvement et de l'exercice dans l'eau chaude
. Chirurgie d’exploration du poignet
28) Une femme âgée de 40 ans, chute sur la terrasse avec une main droite en hyper- extension. Juste après, un gonflement et une douleur du poignet apparaissent rapidement, les radiographies du poignet droit en d'urgence sont negatives. On fait l’ IRM du poignet droite qui présente de fracture du scaphoïde sans déplacé. Quel est la méthode du traitement orthopédique le plus approprié?
Laissant libre tous les inters métacarpo-phallangiens
Laissant libre les 4 derniers inters métacarpo-phalangiennes
Laissant libre le premier inter métacarpo-phalangienne
Laissant libre le deuxième inter métacarpo-phalangienne
Laissant libre le dernier inter métacarpo-phalangienne
29) Une dame de 65 ans est tombée de l’ escaliers sur la main droite en hyper-extension, elle vous est adressée avec de radiographie par son médecin traitant. Le résultat de la radiographie est la fracture de l’extrémité distale du radius droite sans déplacé. L’ indication thérapeutique est orthopaedique. Concernant la méthode de traitement, laquelle est la plus appropriée?
Réduction sous anesthésie générale
Gouttière plâtré anti-brachiopalmer
Désimpaction avant de traction dans son axe
Inclinaison radiale de la main
Immobilisation dans une durée de 6 semaines
30) 3 months old infant with watering lacrimal sac on pressing causes regurgitation of mucopus material. What is the appropriate treatment?
. Dacryocystorhinostomy
. Probing
. Probing with syringing
. Massage with antibiotics up to age of 6 months
. Dacryocystectomy
31) Chez un malade atteint de crise de glaucome aigu traité, l’examen ophtalmologique après guérison de la crise, montre une réouverture parfait de l’angle iridocornéen et une normalisation complète de la tension oculaire, de l’acuité visuelle et du segment antérieur. Quelle attitude fautil adopter pour éviter les récidives ?
Surveillance simple
. Ablation du cristallin
. Prescription des myotiques
. trabéculectomie
. Iridectomie périphérique
32) Une jeune femme est amenée chez son généraliste après avoir recu de l’ammoniaque dans les deux yeux. Elle souffre, présente un blépharospasme, et est photophobe. A l’ouverture forcée des paupières, on constate une hyperhémie conjonctivale et une cornée opalescente. Quel est le geste primordial à effectuer en urgence par le généraliste?
. Pansement occlusif sur les deux yeux
. Instillation d’un collyre antibiotique
. Lavage abondant au sérum des deux yeux
. Instillation d’un collyre myotique
. prélèvement des sécrétions afin de determiner le pH de la solution pour préparer une solution tampon
33) Plusieurs facteurs de risques peuvent favoriser la survenue d’une rétinopahie diabétique et accélérer sa progression, sauf une. Laquelle ?
l’ancienneté du diabète est le facteur de risque le plus important. Après 15 ans d’évolution de la maladie, plus de 80% des diabétes sont atteints de rétinopathie.
un mauvais équilibre de la glycémie est correlé à la présence de la rétinopathie diabétique. La normalisation de la glycémie est toujours bénéfique
L’hypertension artérielle, le tabagisme, la dyslipidémie sont susceptible de favoriser la survenue ou la progression de rétinopathie diabétique
elle est indépendante de la régulation de l’équilibre glycémique
Durant la grossesse, la femme diabétique est exposée à un risque accru de la progression de la rétinopathie diabétique.
34) Un nourrisson de 18 mois a depuis l’âge de 10 mois des otites aiguës récidivantes survenant en moyenne dans les 2 mois et traitées à chaque fois soit par antibiotique, soit par paracentèse suivie d’une antibiothérapie. Dans l’intervalle des otites, les tympans sont rétractés : l’audiométrie est normale. Quel traitement est-on en droit de proposer en premier ?
. Antibiothérapie au long cours
. Mastoïdectomie
. Immunomodulateurs
. Adénoïdectomie
. Corticothérapie au long cours
35) Un sujet jeune présente une otorrhée chronique fétide. L’otoscopie nous montre une perforation tympanique située au niveau du Schrapnel. L’aspiration ramène quelques lamelles de cholestéatome. Quelle attitude thérapeutique vous semble préférable ?
. Geste chirurgical
. Radiothérapie
. Traitement médical local et surveillance
. Traitement médical par voie générale
. Aspiration répétées du cholestéatome
36) Un enfant présentant un stridor respiratoire aigu qui s’aggrave vous est amené en urgence. Vous diagnostiquez un pseudo-croup. Votre premier traitement est ?
. Une laryngotomie
. Des corticoïdes intraveineux à hautes doses
. Une injection de morphine
. Une trachéotomie en urgence
. Une intubation
37) Il s’agit d’un nourrisson de 8mois présentant cliniquement, la triade symptomatique (vomissement bilieux, douleur abdominale paroxystique et selles sanguinolentes) depuis 12 heures et l’échographie montre une image de boudin d’invagination à 10heure du soir. Devant ce patient, quelle est votre indication?
Équilibrer les troubles hydro-électrolytiques à la normale
Essayer de faire une réduction pneumatique de boudin d’invagination
Opérer urgent après avoir fait le bilan préopératoire
Garder ce patient pour opérer le jour du lendemain
Réhydratation ce malade à la normal
38) Une fille âgée de 5 ans a présenté un reflux vésico-urétéral droit de grade 3. Elle a déjà fait 2 fois d’infection urinaire dans son antécedant. Quel est votre traitement?
Surveillance simple
Surveillance avec antibioprophylaxie
Chirurgie endoscopique
Chirurgie ouverte: opération de Cohen
Néphrectomie droit
1) Un jeune l’homme de 20 ans, ayant un accident par chute sur le moignon de l’épaule gauche. Après l’ accident, il a très mal de l’épaule gauche, impotence fonctionnelle du membre supérieur gauche avec attitude vicieuse, et à l’inspection un fragment fracturaire de la clavicule est basculé en haut. Pour confirmer cette fracture et dégager des autres reliefs de l’épaule, quelle incidence radiologique plus probablement?
La seule radiographie de profil
La seule radiographie de face
La seule radiographie d’oblique
La radiographie de face et profile
La radiographie de profile et oblique
2) Une dame de 65 ans est tombée de l’ escaliers sur la main droite, elle vous est adressée avec des radiographies par son médecin traitant. En basant sur les résultats radiographiques, vous suspectez la fracture de l’extrémité distale du radius droite. Concernant les imagerie, parmi les propositions suivantes, laquelle est la plus appropriée?
Radiographie de face est pour localiser la rupture des ligaments inter-carpiens
IRM est pour visualiser le déplacement de la fracture
Le scanner est pour visualiser la fracture de la surface articulaire
La radiographie de profil est pour localiser la rupture du ligament triangulaire
Echographie est pour visualiser la rupture des vaisseaux
3) Une dame de 65 ans est tombée de l’ escaliers sur la main droite en hyper-extension, elle vous est adressée avec des radiographies par son médecin traitant. Le résultats de la radiographie est une fracture de Pouteau colles. Parmi les propositions suivantes, une est correcte, laquelle?
La fracture épiphyse distale du radius à déplacement postérieur
La fracture épiphyse distale du radius à déplacement antérieur
La fracture métaphyse distale du radius à déplacement antérieur
La fracture métaphyse distale du radius à déplacement postérieur
La fracture métapho-épiphysaire distale à déplacement postérieur
1) A 74-year-old man presents to your office for a routine. He has no present complaint. His medical history is significant for right knee osteoarthritis. He takes naproxen occasionally, to relieve knee pain. He does not smoke or consume alcohol. His BP is 165/75 mmHg and PR is 70/min. The physical examination showed a mild systolic ejection type murmur at the base of the heat to the right. An E-KG revealed left ventricular hypertrophy and secondary ST segment and T wave change. Moderate left ventricular hypertrophy, without any flow abnormalities, was demonstrated on echocardiography. The ejection fraction was 60%. What is the most probable cause of hypertension in this patient?
Rigidity of the arterial wall
. Increased intravascular volume
. Increased cardiac output
. Aortic insufficiency
. Elevated plasma renin activity
2) A 47-year-old woman loses consciousness for 2 minutes while shopping in a supermarket. In the emergency room, she recounts feeling nausea and warmth spreading over her body immediately before passing out. She has never had a similar episode before. She has not seen a doctor for several years anddoes not take any medications, nor does she use tobacco, alcohol or drug. Her family history is unremarkable. Which of the following most likely caused this episode?
Cardiac arrythmia
. Orthostatic hypotension
. Heat valve disease
. Neurocardiogenic syncope
. Seizure
3) A 25-year-old woman experiences sudden-onset palpitations and generalized weakness. During this episode, her blood pressure is 100/60 mmHg and her heat rate is 160/min and regular. She has no significant past medical history and does not take any medications. She reports having a few similar episodes in the past which she has self-treated by immersing her face in cold water. Generally, she says, cold water immersion relieves her symptoms within several minutes. This cold water therapy works by affecting which of the following?
Vascular tone
. Ventricular myocardium contractility
. Purkinje fiber conduction
. Atrioventricular node conductivity
. Sinoatrial node automatism
4) A 67-year-old man is evaluated for hypertension. He complains of occasional morning headaches. His past medical history is also significant for type 2 diabetes mellitus, coronary artery disease, and a stroke with residual left-sided weakness. He underwent coronary artery bypass surgery seven years ago and carotid endarterectomy five years ago. His current medication list includes lisinopril hydrochlorothiazide, amlodipine, metoprolol, aspirin, metformin and glyburide. His blood pressure is 190/120 mmHg on the right arm and 170/110 mmHg on the left arm. His heat rate is 65/min Physical examination reveals a periumbilical systolic-diastolic bruit. The latter finding is best explained by which of the following?
. Abdominal aortic aneurysm
. Aorto-enteric fistula
. Renal artery stenosis
. Aortic coarctation
. Aortic dissection
5) A 67-year-old male is brought to the emergency department after a syncopal episode. He lost consciousness while shopping in the mall. He denies any nausea, diaphoresis, chest pain, or shortness of breath. He has had two episodes of lightheadedness over the last month but has not seen a doctor. His past medical history is significant for long-standing hypertension, which is being treated with enalapril. His blood pressure is 135/90 mmHg while supine, and 130/85 mmHg while standing. His heat rate is 64/min. ECG shows a sinus rhythm with high voltage, prolonged PR interval, prolonged QRS interval, normal QT interval and occasional premature ventricular contractions (PVC). Echocardiography reveals left ventricular hypertrophy and an ejection fraction (EF) of 55%. Which of the following is the most likely cause of this patient's syncope?
. Bradyarrhythmia
. Ventricular premature beats
. Autonomic dysfunction
. Torsades de pointes
. Decreased myocardial contractility
6) A 47-year-old male presents to your office with a two-month history of lethargy and decreased libido. His medical records reveal that he has been treated for joint pain and swelling over the last six months and was diagnosed with diabetes mellitus one year ago. Physical examination reveals hepatomegaly and testicular atrophy. Which of the following cardiac abnormalities is most likely to also be present in this patient?
Atrial septal defect .
. Hypertrophic cardiomyopathy
Aortic stenosis
. Cardiac conduction block
. Endocardial fibroelastosis
7) A 50-year-old woman presents to your office complaining of lower extremity edema that stated several weeks ago, and slowly progressed thereafter. Her past medical history is significant for hypertension, treated with metoprolol for 2 years. Amlodipine was added recently because of inadequate control of BP with metoprolol alone. She does not smoke or consume alcohol. She has no known drug allergies. Her blood pressure is 130/80mmHg and her heart rate is 64/min. The physical examination reveals bilateral symmetric 3+ pitting edema of both lower extremities, without any skin changes or varicosities. Her neck vein pulsation is normal. Other physical findings are within normal limits. Her laboratory studies reveal the following: Serum albumin 4.5 g/dL, Total serum bilirubin 0.8 mg/dL, Serum sodium 140 mEq/L, Serum potassium 4.0 mEq/L, Serum creatinine 0.8 mg/dL. Urinalysis is within normal limite. What is the most likely cause of the edema in this patient?
Heart failure
. Side effect of her medications
. Venous insufficiency
. Renal disease
. Liver disease
8) A 63-year-old man presents to the ER with substernal chest pain and diaphoresis. The pain stated one hour ago and did not remit with antacids. He has a past medical history of asthma for which he uses inhaled fluticasone and peptic ulcer disease for which he takes omeprazole. His family history is significant for prostate cancer in his father and breast cancer in his mother. Physical examination reveals a blood pressure of 160/100 mmHg and a heat rate of 90/min. A bruit is heard over the right carotid artery and a mild systolic murmur is present at the cardiac apex. Sublingual nitroglycerin and aspirin are administered in the. Within minutes, the patient reports decreased pain. Which of the following most likely accounts for this improvement in his symptoms?
. Increased left ventricular compliance
. Decreased left ventricular volume
. Decreased left ventricular contractility
. Increased systemic afterload
. Increased cardiac preload
9) A 38-year-old female comes to your office complaining of occasional palpitations. She describes feeling a fast and irregular heartbeat. Over the past two months, she has had three such episodes, each lasting about two hours. She denies any associated chest pain, shortness of breath cough or ankle swelling. She drinks alcohol on social occasions and does not smoke cigarettes. She has no other medical problems and is not taking any medications. On physical examination, her temperature is 37.1°C (98.9°F), pulse is 80/min, blood pressure is 130/70mmHg, and respirations are 14/min. On auscultation of her heat the apical impulse is displaced and there is an S3. You also hear a pansystolic murmur, which is loudest at the apex and radiates to the axilla. Which of the following is the most likely cause of her symptoms?
Mitral valve prolapse
. Infective endocarditis
. Mitral annular calcification
. Rheumatic heat disease
. Myocardial ischemia
10) A 42-year-old woman is evaluated for depression, mood swings and poor. She also complains of mild headaches and muscle weakness. She has had two ER visits for kidney stones over the past year. She denies any illicit drug use. Her blood pressure is 160/105 mmHg and her heat rate is 85/min. Her laboratory findings are shown below: Sodium 140mEq/L, Potassium 3.6 mEq/L, Chloride 101 mEq/L, Bicarbonate 24 mEq/L, BUN 13 mEq/L, Creatinine 0.9 mEq/L, Glucose 98 mEq/L, Calcium 11.7 mg/dL. Which of the following is the most likely cause of this patient's hypertension?
Renal parenchymal disease
. Parathyroid gland disease
. Hypothyroidism
. Aortic dissection
. Renal vascular stenosis
11) A 14-year-old African American male is referred to your office after his older brother experienced sudden cardiac arrest during hiking trip. He has no current complaints. He denies any illicit drug use. His blood pressure is 110/60 mmHg and his heat rate is 75/min. Neck is supple, no jugular venous distention is appreciated. Carotid pulse seems to have dual upstroke. Lungs are clear. There is strong apical impulse and a systolic ejection type murmur along the left sternal border. Which of the following is most likely to increase the murmur intensity in this patient?
Squatting
. Leg raising
. Recumbency
. Sustained handgrip
. Valsalva maneuver
12) A 60-year-old male is brought to ER by his son because he had an episode of syncope. He was watching TV in an arm-chair when suddenly lost his consciousness without any warning sign. He had several clonic jerks while unconscious. He never had such an episode before. His past medical history is significant for acute myocardial infarction six months ago and well-controlled hypertension. His current medications include captopril metoprolol hydrochlorothiazide, clopidogrel and aspirin. His blood pressure is 130/85 mmHg and heat rate is 80/min with frequent ectopic beat. Physical examination revealed mild holosystolic apical murmur radiating to the axilla. Which of the following is the most probable pathophysiologic mechanism for his syncopal episode?
Vasovagal reaction
. Postural hypotension
. Seizure
. Autonomic dysfunction
. Arrhythmia
13) A 54 year-old male comes to the physician because of abdominal distention. He thinks his big belly is making it hard for him to breathe. He received radiation therapy for Hodgkin lymphoma several years ago and was told that he is cured. He drinks alcohol on a regular basis. His temperature is 36.7°C (98°F), blood pressure is 120/76 mm Hg, pulse is 80/min and respirations are 20/min. Examination shows a jugular venous pressure 7 cm above the sternal angle. Dullness to percussion and decreased breath sounds are noted in the right lung base. The abdomen is quite distended with an obvious fluid wave. Mild hepatomegaly is present. Extremities have 2+ lower extremity edema. Initial laboratory studies are shown below: Serum creatinine 08 mg/dL, Alburnin 4.0 mg/dL, Total bihrubin 1.0 mg/dl, Prothrombin time 11 sec. Urinalysis is within normal limits. Which of the following is the most likely cause of his condition?
. Urinary protein loss
. Thoracic duct obstruction
. Inelastic pericardium
. Portal vein compression
. Portal vein thrombosis
14) A 32-year-old woman presents with progressively worsening dyspnea on exertion one month after returning from a vacation in Texas. She says that her symptoms have progressed to the point that she now wakes during the night with a choking sensation that improves only with sitting up. Recently her shortness of breath has required her to significantly limit her physical activity. She denies having associated chest pain, skin rash or joint pain. She has no significant past medical history. Family history is significant for thyroid cancer in her aunt and lung cancer in her father, a heavy smoker. On physical examination, her temperature is 37.2°C (99°F), pulse is 96/min, blood pressure is 110/70 mmHg, and respirations are 14/min. Bilateral pitting ankle edema is present. Her liver is enlarged 2 cm below the right costal marginal. Lung auscultation reveals decreased breath sounds at the bilateral bases. Cardiac exam reveals the presence of a third heat sound. Chest x ray shows an enlarged cardiac silhouette and small bilateral pleural effusion. EKG is unremarkable. Which of the following is the most likely cause of her symptoms?
. Atherosclerosis
. Autoimmune disease
. Coccidioidomycosis
. Lyme disease
. Viral infection
15) An 88-year-old female nursing home resident is brought to the hospital with a one-week history of moaning, decreased oral intake and decreased ambulation. Physical examination reveals a very thin female who is moaning and appears to be in pain. She opens her eyes spontaneously but does not respond to questions. Her blood pressure is 75/43 mmHg, pulse is 105/min, temperature is 35.5°C (96°F), and respirations are 22/min. Oxygen saturation (pulse oximetry) is 97% on room air. Her skin and oral mucosa are dry and her neck veins are flat. There is no lymphadenopathy. On chest auscultation, there are crackles in the right upper lung lobe. Abdomen is soft and non-distended. There is 2+ pitting presacral and lower extremity edema, and a deep pressure ulcer in the sacral area. Laboratory analysis reveals the following: Sodium 155mEq/L, Potassium 5.3 mEq/L, Glucose 88mg/dL, Bicarbonate 14mEq/L, BUN 151mg/dL, Creatinine 3.1mg/dl. Which of the following is the most likely cause of her lower extremity edema?
. Increased plasma hydrostatic pressure
. Decreased lymphatic drainage
. Increased interstitial oncotic pressure
. Renal water and sodium retention
. Decreased plasma oncotic pressure
16) A 64-year-old man complains of palpitations and progressive shortness of breath over the past several hours. He says that he also develops a choking sensation every time he tries to lie down. His medical history is significant for hypertension for the past 20 years and medication non-compliance. He also has a 35-year smoking history. He reports that his father died of a heart attack at age 70 and his mother suffered from asthma. On physical examination, his blood pressure is 170/100 mmHg and his heat rate is 130/min and irregularly irregular. Lung exam reveals bibasilar crackles. There is 2+ pitting edema of the lower extremities. Bedside echocardiography shows a left ventricular ejection fraction of 55%. Which of the following is most likely responsible for his symptoms?
Cardiogenic shock
. Increased lung compliance
. Small airway bronchoconstriction
. High-output heat failure
. Diastolic dysfunction
17) A 55-year-old Caucasian male presents to your office with muscle pain of recent onset. His past medical history is significant for hypertension and an acute myocardial infarction experienced 2 months ago. His current medications include metoprolol captopril, aspirin and simvastatin. His blood pressure is 130/80 mmHg and heat rate is 60/min. Liver function tests are slightly abnormal. Serum creatine kinase level is elevated. You suspect a drug-induced reaction. Which of the following is the most possible mechanism of drug-induced reaction in this patient?
. Immune-mediated reaction
. Damage of membrane-bound lipids
. Synthetic reaction inhibition
. Extracellular enzyme blockage
. Cell surface receptor blockage
17) A 55-year-old Caucasian male presents to your office with muscle pain of recent onset. His past medical history is significant for hypertension and an acute myocardial infarction experienced 2 months ago. His current medications include metoprolol captopril, aspirin and simvastatin. His blood pressure is 130/80 mmHg and heat rate is 60/min. Liver function tests are slightly abnormal. Serum creatine kinase level is elevated. You suspect a drug-induced reaction. Which of the following is the most possible mechanism of drug-induced reaction in this patient?
Immune-mediated reaction
. Damage of membrane-bound lipids
. Synthetic reaction inhibition
. Extracellular enzyme blockage
. Cell surface receptor blockage
18) A 70-year-old man is brought to the Emergency Room because he lost his consciousness while working in the garden. He says that he had several episodes of near-syncope on exertion recently. His past medical history is insignificant. He is not taking any medications. His blood pressure is 110/85 mmHg and heat rate is 80/min. Point of maximal impulse is increased in intensity. Cardiac auscultation reveals ejection type systolic murmur at the base of the heat with radiation to the carotid arteries. ECG demonstrates left ventricular hypertrophy, and secondary ST segment and T wave change. What is the most probable cause of this patient's condition?
. Rheumatic endocarditis
. Age-related sclerocalcific changes
. Congenital anomaly
. Hypertension
. Bacterial endocarditis
19) A 32-year-old male complains of progressive weakness and exertional dyspnea. His past medical history is significant for a knife injury to the right thigh two months ago. He has been arrested several times for robbery. He consumes alcohol regularly, and smokes crack occasionally. His younger brother died of cystic fibrosis. His blood pressure is 160/60 mmHg, and heart rate is 100/min. His extremities are warm and flushed. Carotid upstroke is brisk. The point of maximal impulse is displaced to the left, and a soft, holosystolic murmur is heard over the cardiac apex. The murmur does not change with the Valsalva maneuver. Which of the following is the most likely cause of this patient's symptoms?
Decreased cardiac output
. Pulmonary hypertension
. Papillary muscle dysfunction
. Increased cardiac preload
. Hypertrophic cardiomyopathy
20) A 22-year-old college student went to the health clinic complaining of a fever over the last 5 days, fatigue, myalgias, and a bout of vomiting and diarrhea. The clinic doctor diagnosed him with acute gastroenteritis and told him to drink more fluids. Three days later, the student presents to the ED complaining of substernal chest pain that is constant. He also feels short of breath. His temperature is 100.9°F, HR is 119 beats per minute, BP is 120/75 mmHg, and RR is 18 breaths per minute. An ECG is performed revealing sinus tachycardia. A chest radiograph is unremarkable. Laboratory tests are normal except for slightly elevated WBCs. Which of the following is the most common cause of this patient’s diagnosis?
Streptococcus viridans
. Cocaine abuse
. Atherosclerotic disease
. Coxsackie B virus
. Influenza A
21) A 60-year-old man is brought to the ER by his wife because he lost consciousness in the bathroom at night. He says that he woke up, went to the bathroom to urinate, and fainted there. He rapidly recovered his consciousness without any indication of disorientation. He has never had such an episode before. He admits' problems with urination,' including difficulty with initiating urination and frequent awakening to void at night. He does not take any medication. His past medical history is insignificant. He smokes 2 packs of cigarettes per day and does not consume alcohol. His blood pressure is 130/80 mmHg while supine, and 132/80 mmHg while standing. His heart rate is 70/min. His physical examination is within normal limits. The ECG is normal. What is the most probable cause of the syncopal episode in this patient?
Arrhythmia
. Transient ischemic attack (TIA)
. Seizure
. Situational syncope
. Postural hypotension
22) A 73-year-old man presents to the ED after a syncopal episode. He had been resting in bed for approximately one week after injuring his right knee. This morning, his knee felt better and he attempted to get up from bed. However, upon attempting to stand, he sustained a brief loss of consciousness. He had no symptoms or medical history prior to the knee injury. Medications include acetaminophen and ibuprofen for knee pain. On exam, his pulse is 73/min, respirations are 14/min, and blood pressure is 136/83 mmHg. Which of the following is the most likely cause of this patient's syncope?
Cardiac arrhythmia
. Valvular obstruction
. Hyperventilation
. Vagal nerve hyperactivity
. Orthostatic hypotension
23) A 46-year-old woman is hospitalized for agitation, restlessness and poor sleep. She has been complaining of headaches recently and has gained 14 pounds over the past three months. She denies any illicit drug use. Her blood pressure is 160/110 mmHg and her heart rate is 90/min. Her laboratory findings are shown below: Sodium 142 mEq/L, Potassium 3.2 mEq/L, Chloride 98 mEq/L, Bicarbonate 26 mEq/L, BUN 12 mg/dl, Creatinine 0.9 mg/dl, Glucose 205 mg/dl, Calcium 94 mg/dl. Which of the following is the most likely cause of this patient's hypertension?
Renal parenchymal disease
. Parathyroid gland disease
. Hypothyroidism
. Adrenal cortical disease
. Adrenal medullary disease
24) A 53-year-old man presents to the emergency room with squeezing chest pain that started two hours ago. He also complains of shortness of breath that is worse when lying down. He has never had pain like this before. He has no significant past medical history and he takes no medications. A routine health maintenance visit two weeks ago was normal. On physical examination in the ER, his blood pressure is 140/90 mmHg and his heart rate is 100/min. Chest auscultation reveals a grade II/VI blowing systolic murmur at the cardiac apex and bibasilar crackles in the lungs. ECG shows ST segment elevations in leads I, aVL, and v1-v3. Which of the following is most likely increased in this patient?
Left atrial pressure
. Right ventricular preload
. Left ventricular ejection fraction
. Left ventricular compliance
. Left atrial size
25) A 35-year-old woman who has recently emigrated from Asia presents to the emergency room with acute onset of dyspnea. She denies any cough, chest pain, or fever. She has a history of rheumatic heart disease as a teen. On examination, she has an irregular pulse of 97/min, blood pressure of 125/75 mmHg and temperature of 37.2°C (98.9°F). The first heart sound is loud and a mid-diastolic rumble is heard at the apex. Crackles are present in both lung fields. ECG shows an irregularly, irregular heart rhythm and the absence of 'P' waves. Which of the following is the most likely cause of this patient's abnormal heart rhythm?
Left atrial dilatation
. Pulmonary hypertension
. Left ventricular hypertrophy
. Left ventricular dilatation
. Right atrial dilatation
26) An 82-year-old male presents for evaluation of chronic back pain. On physical examination, he is found to have a blood pressure of 160/85 mmHg while supine and 135/70 mmHg while standing. He is otherwise healthy; his only medicine is occasional ibuprofen for back pain. Which of the following agerelated changes best explains the observed finding?
. Increased left ventricular wall stiffness
. Decreased glomerular filtration rate
. Decreased stress-mediated catecholamine release
. Decreased baroreceptor responsiveness
. Decreased left ventricular contractility
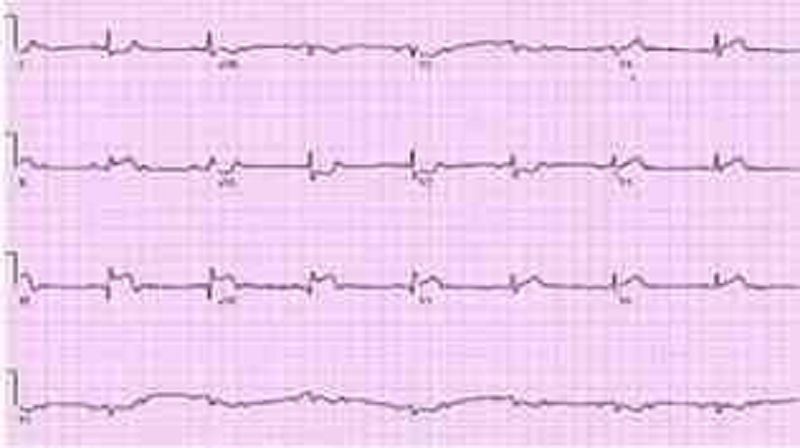
27) A 70-year-old Caucasian man comes to the emergency department because of the sudden onset of nausea, vomiting, diaphoresis, and chest pain. His other medical problems include hypertension, diabetes mellitus-type 2, and aortic stenosis. He has smoked one-and-a-half packs of cigarettes daily for 30 years and drinks 4 ounces of alcohol daily. His temperature is 37.2°C (99°F), blood pressure is 100/60 mmHg, pulse is 60/min, and respirations are 18/min. The patient's pulse oximetry showed 98% at room air. Examination shows normal first and second he sounds. Lungs are clear to auscultation. His EKG is shown below. Which of the following is the most likely mechanism of this patient's condition?
Occlusion of the right coronary artery
. Vasospasm of the left circumflex artery
. Inflammation of the pericardium
. Occlusion of the left anterior descending artery
. Occlusion of the left circumflex artery
28) A 24-year-old male experiences syncope while shovelling snow. He regained consciousness within one minute. He has been having some shortness of breath and chest pains recently, mostly related to exercise. He denies any illicit drug use. His temperature is 37.2°C (98.9°F), and blood pressure is 126/76 mmHg, pulse is 76/min and respirations are 14/min. Physical examination shows a well-built male in no apparent distress. Lungs are clear. A crescendo-decrescendo systolic murmur is heard along the left sternal border without carotid radiation. Chest X-ray is normal. Which of the following is the most likely cause of his syncopal episode?
Atrioventricular conduction delay
. Mitral valve degeneration
. Coronary atherosclerosis
. Aortic dissection
. Left ventricular hypertrophy
29) A 33-year-old woman is undergoing an elective, open cholecystectomy after 2 episodes of acute calculous cholecystitis. She suddenly becomes hypotensive, and a generalized rash is noted. Her past medical history is significant for a hypotensive episode 8 weeks ago while having protected sex with her new partner. Which of the following is the most probable cause of this patient's condition?
Acute blood loss
. Pulmonary embolism
. Septic shock
. Allergic reaction
. Coagulation abnormality
30) A 72-year-old male comes to the office with intermittent symptoms of dyspnea on exertion, palpitations, and cough occasionally productive of blood. On cardiac auscultation, a low-pitched diastolic rumbling murmur is faintly heard at the apex. What is the most likely cause of the murmur?
Rheumatic fever as a youth
. Anemia from chronic blood loss
. A congenital anomaly
. A silent MI within the past year
. Long-standing hypertension
31) A 53-year-old male presents to your office with a two-day history of right calf pain and swelling. He describes the pain as constant and states that it is exacerbated by knee flexion. He has a history of past IV drug abuse, endocarditis, and stroke. He is currently wheelchair-bound secondary to stroke-related left-sided hemiparesis. On physical examination, his blood pressure is 140/90 mmHg and his heart rate is 100/min. There is no jugular venous distention or hepato-jugular reflux. His chest is clear to auscultation but his abdomen is enlarged with shifting dullness and a fluid wave, suggestive of ascites. His liver is palpable 3 cm below the right costal margin. His spleen is also palpable. On examination of his lower extremities, you note right-sided calf swelling and tenderness. Which of the following is the most likely cause of this patient's ascites?
. Right-sided heart failure
. Paradoxical embolism
. Chronic liver disease
. Protein C deficiency
. Pulmonary embolism
32) A 60-year-old white man comes into the Emergency Room with intensive retrosternal pain that began ten minutes ago. He has never had such pain before. His past medical history is significant for diabetes mellitus, type 2, controlled with diet. His blood pressure is 150/95 mmHg and HR is 80/min. You give him one chewable tablet of aspirin and two sublingual tablets of nitroglycerin with a 5-minute interval. After the second tablet of nitroglycerin, the pain is greatly relieved. What is the most important mechanism responsible for pain relief in this patient?
Increase in coronary blood flow
. Change in the activity of baroreceptors
. Dilation of capacitance vessels
. Dilation of resistance vessels
. Increased cardiac contractility
33) A 34-year-old male who recently immigrated from Brazil presents with a 5-month history of exertional dyspnea without associated chest pain, palpitations, dizziness, or syncope. His past medical history is significant for an episode of megacolon, which was treated 2 years ago. On physical examination, there is 1+ pedal edema and mild jugular venous distention. Cardiac exam is significant for the presence of an S3, but no murmurs are heard. Chest x-ray reveals prominent cardiomegaly. Based on these findings, which of the following is most likely causing his symptoms?
Diphtheric myocarditis
. Protozoal disease
. Coronary artery disease
. Giant cell myocarditis
. Rickettsial myocarditis
34) A 12-year-old African American male is found to have a murmur during a routine sports physical. He has a family history of sudden death at a young age. It is a harsh crescendo-decrescendo murmur that begins after S1 and is best heard at the left lower sternal border. Valsalva maneuver intensifies the murmur. Which of the following is the most likely mitral valve abnormality in this patient?
Dilated mitral valve annulus
. Prolapse of the mitral valve
. Mitral annulus calcifications
. Abnormal mitral leaflet motion
. Rupture of chordae tendinae
35) A 63-year-old woman with a long history of hypertension faints after experiencing the sudden onset of severe chest pain that radiates to her back. She is rushed to the emergency room. Upon arrival she is agitated and demands quick pain relief. Her heart rate is 110/min and blood pressure is 90/50 mmHg. Jugular veins are distended. An intra-arterial catheter shows significant variation of systolic blood pressure related to the respiratory cycle. Chest x-ray reveals widening of the mediastinum. Which of the following is the most likely cause of this patient's syncope?
. Papillary muscle dysfunction
. Cardiac tachyarrhythmia
. Vagal hyperactivity
. Pericardial fluid accumulation
. Intravascular volume loss
36) A 47-year-old male was brought to the emergency room with chest pain of acute onset. The pain was associated with nausea, vomiting, and diaphoresis. He has a history of diabetes, hypertension, and hyperlipidemia. ECG reveals ST segment elevation in the anterolateral leads and ventricular premature beats (VPBs). The patient dies within the first hour after the arrival to emergency room. What is the most likely pathophysiologic mechanism responsible for this patient's death?
Electro-mechanic dissociation
. Asystole
. Increased automaticity
. Full conduction block
. Reentry
37) A 57-year-old male presents to your office with a two week history of fever, chills, and generalized weakness. His medical history is significant for a hospitalization for pyelonephritis requiring IV antibiotics six months ago. He also recently underwent cystoscopy for evaluation of persistent dysuria. His past medical history is also significant for an episode of rheumatic fever as a child and Hodgkin's lymphoma treated with chemotherapy 10 years ago. On examination, his temperature is 37.8°C (100°F), blood pressure is 150/86 mmHg, pulse is 98/min and regular, and respirations are 16/min. The patient appears slightly diaphoretic. You note a new II/VI systolic murmur and tender erythematous lesions affecting several fingertips. The remainder of the physical examination is unremarkable. Which of the following bacteria is most likely responsible for his present illness?
. Streptococcus pyogenes
. Coxiella burnetii
. Viridans streptococci
. Enterococci
. Staphylococcus epidermidis
38) A 65-year-old man complains of lower leg swelling, fatigue and poor appetite. His past medical history is significant for recurrent chest infections, wheezing, cough, recent pyelonephritis, and arterial hypertension. He smokes 1 pack of cigarettes a day but denies alcohol or intravenous drug use. His physical examination reveals a barrel-shaped chest with bilateral scattered wheezes. His abdomen is distended and his liver edge is palpated 4 cm below the right costal margin. You note pitting edema and dilated, tortuous, superficial veins over the bilateral lower extremities. Manual pressure on the abdomen causes persistent distention of the jugular veins. The patient's serum sodium level is 135 mEq/L and his creatinine concentration is 1.2 mg/dl. An abnormality of which of the following is most likely to explain his edema?
. Serum albumin level
. Urinary protein excretion
. Portal venous resistance
. Pulmonary capillary wedge pressure
. Pulmonary artery systolic pressure
39) A 60-year-old male presents to the emergency room with the chief complaint of progressive exertional dyspnea and fatigue. He denies any chest pain, syncope, cough, or edema. He suffered an acute anterior wall myocardial infarction one month ago. Chest auscultation reveals bilateral crackles in his lower chest. Cardiac auscultation reveals a pansystolic murmur at the apex with radiation to the axilla. ECG shows previously present unchanged Q waves and a persistent ST segment elevation in the anterior leads. Based on these findings, what is the most likely underlying cause of his symptoms?
. Interventricular wall rupture
. Ventricular free wall rupture
. Right ventricular infarction
. Recurrent ischemia
. Ventricular aneurysm
40) A 68-year-old white female presents to the ER complaining of sudden onset chest pain associated with two episodes of vomiting. She has hypertension for which she takes atenolol and hydrochlorothiazide. Her pulse is 60/min, blood pressure is 80/50 mmHg and respirations are 14/min. Examination shows elevated jugular venous pressure and a positive Kussmaul's sign. Her lungs are clear to auscultation. Her EKG shows 2 mm ST segment elevation in leads II, III and aVF and 1 mm ST segment depression in leads I and aVL. Which of the following is the most likely cause of this patient's hypotension?
Pulmonary thromboembolism
. Intravascular volume depletion
. Variant angina
. Interventricular septum rupture
. Right ventricular infarction
41) A 53-year-old man presents to your office complaining of weakness and exertional dyspnea over the last week. He denies chest pain and palpitations. He has no other past medical history. His father died of a myocardial infarction at age 55. On exam, his heart rate is 100/min and blood pressure is 90/60 mmHg. Internal jugular venous pulsation is observed 7 cm above the sternal angle. Lungs are clear to auscultation. Heart sounds are muffled. Which of the following is the most likely cause of this patient's complaints?
Decreased cardiac contractility
. Increased right ventricular compliance
. Pulmonary hypertension
. Decreased left ventricular preload
. Left ventricular outflow obstruction
42) A 34-year-old man rushes into the ER complaining of severe substernal chest pain that began abruptly 30 minutes ago. He says that he also feels as though his heart 'is racing,' but denies any shortness of breath, cough or fever. He has never experienced pain like this before. His past medical history is significant for an appendectomy one year ago. The patient reports that his father died at age 64 due to "some heart problem" and his mother died of ovarian cancer. On physical examination, the patient is agitated and sweating profusely. His pulse is 110/min, blood pressure is160/100 mmHg, and respirations are 14/min. Physical examination is normal except for dilated pupils and a small amount of blood at the external nares. EKG shows ST elevations in leads v1-v4. What is the most likely explanation for his symptoms?
Atherosclerotic vascular disease
. Aortic dissection
. Drug-induced vasospasm
. Pleurodynia
. Acute pericarditis
43) A 50-year-old white male comes into your office for a routine check-up. He has no present complaints. His past medical history is significant for hypertension controlled with a low-dose thiazide diuretic. His family history reveals non-fatal myocardial infarction in his father at the age of 47. The patient does not smoke or consume alcohol. His blood pressure is 130/75 mmHg and his heart rate is 70/min. His previous records show that his HDL level is persistently low in spite of acceptable total cholesterol and LDL levels. You prescribe niacin to raise HDL level. The patient returns in a week complaining of intensive generalized pruritis and flushing. What is the most probable cause of the patient's complaint?
Hypersensitivity reaction
. Psychogenic reaction
. Drug-induced vasoconstriction
. Drug interaction
. Prostaglandin-related reaction
44) A 63-year-old male is admitted for sudden onset severe chest pain. His ECG reveals ST elevation in leads V2-V6. He is treated with thrombolytic therapy, heparin, aspirin, metoprolol, morphine, and nitrates. A coronary angiogram performed after thrombolytic therapy reveals 50% obstruction of the left anterior descending artery. On the third day of hospitalization, the patient suddenly develops severe shortness of breath at rest and hypotension. Examination reveals a soft S1, an apical pansystolic murmur radiating to the axilla, and bibasilar crackles. His temperature is 37.8°C (100°F), blood pressure is 92/58 mmHg, heart rate is 102/min, and respirations are 31/min. An echocardiogram performed on the second hospital day reveals an akinetic region of the anterior wall. What is the most likely explanation for this patient's deterioration?
Pericardia! tamponade
. Acute aortic dissection
. Papillary muscle dysfunction
. Rupture of ventricular septum
. Pulmonary embolism
45) A 34-year-old female presents to your office complaining of pressure-like, substernal chest pain that has been affecting her recently when she plays active sports. Resting consistently alleviates the pain. She denies any associated nausea, vomiting, diaphoresis, dyspnea, palpitations or syncope. Family history is non-contributory. On physical examination, her pulse is 79/min and blood pressure is 130/70 mmHg. Cardiac auscultation reveals a high-pitched 3/6 systolic murmur best heard at the second right intercostal space. The lungs are clear to auscultation. Chest x-ray shows a normal sized heart and clear lung fields. What is the most likely cause of this patient's chest pain?
. Anomalous origin of the right coronary artery
. Stretching of the papillary muscles
. Increased myocardial oxygen extraction
. Increased myocardial oxygen demand
. Atherosclerotic narrowing of the coronaries
46) A 48-year-old Caucasian male presents to your office complaining of progressive exertional dyspnea. It has become especially bothersome over the past two months. Presently, he becomes short of breath after climbing one flight of stairs. He denies any significant problems in the past. He is not taking any medications and he denies smoking or drinking alcohol. His temperature is 37.2°C (98.9°F), pulse is 78/min, blood pressure is 130/75 mmHg and respirations are 14/min. Chest examination reveals a harsh systolic murmur that is best heard at the right second intercostal space with radiation along the carotid arteries. An S4 is heard at the apex. Based on these findings, what is the most likely cause of this patient's symptoms?
. Hypertrophic cardiomyopathy
. Senile calcific aortic stenosis
. Bicuspid aortic valve
. Rheumatic heart disease
. Myxomatous valve degeneration
47) A 45-year-old man presents to the emergency department because of dyspnea, fatigue, poor appetite and weight gain over the past several weeks. He says that about four weeks ago he began to develop worsening shortness of breath with exertion and more recently has been waking at night with breathlessness. He also notes that it is sometimes difficult for him to open his eyes in the morning due to facial edema. He has no significant past medical history and he takes no medications. On physical examination, his blood pressure is 200/120 mmHg and his heart rate is 100/min. You note generalized bodily edema and distention of his jugular veins while he is sitting upright. On lung auscultation you hear bibasilar rales. Urinalysis shows trace protein, no nitrites, trace leukocyte esterase, 50+ red blood cells and occasional neutrophils. Which of the following is the most likely cause of this patient's edema?
. Renal hypoperfusion
. Hypothyroidism
. Portal hypertension
. Extensive glomerular damage
. Hypoalbuminemia
48) A 14-year-old African American male collapses and dies while playing basketball at a school tournament. He has no known past medical history. Which of the following is the most likely underlying disease in this patient?
Hypertrophic cardiomyopathy
. Bicuspid aorta
. Ventricular septal defect
. Aortic aneurysm rupture
. Coronary atherosclerosis
49) A 46-year-old man complains of exertional dyspnea and dry cough. He also describes occasional episodes of a suffocating night-time cough that is relieved only when he stands up. His medical history is significant for a myocardial infarction six months ago. His current medications are metoprolol, aspirin and simvastatin. He does not use tobacco but drinks alcohol on social occasions. His father died of a stroke and his mother suffers from diabetes mellitus. His blood pressure is 150/100 mmHg and his heartrate is 60/min. Chest examination reveals bibasilar rales. His cardiac apex is palpated in the sixth intercostal space. The liver span is 12 cm. Bilateral pitting leg edema is also present. Which of the following most likely contributes to his edema?
. Constriction of the renal arterioles
. High portal venous resistance
. Increased renal potassium loss
. Increased renal blood flow
. High sodium delivery to the distal tubule
50) A 54-year-old man with a 20-year history of chronic obstructive lung disease has a heave that is palpable at the lower left sternal border at the third, fourth, and fifth intercostal spaces. Which of the following best explains the etiology of the heave?
. It is probably a displaced point of maximum impulse (PMI)
. It means the patient has a pericardial effusion
. It means the patient has right ventricular hypertrophy
. It means that the patient has aortic stenosis
. It means the patient has congestive heart failure
51) A 55-year-old man presents to the ED with chest pain and shortness of breath. His BP is 170/80 mmHg, HR is 89 beats per minute, and oxygen saturation is 90% on room air. Physical examination reveals crackles midway up both lung fields and a new holosystolic murmur that is loudest at the apex and radiates to the left axilla. ECG reveals ST elevations in the inferior leads. Chest radiograph shows pulmonary edema with a normal sized cardiac silhouette. Which of the following is the most likely cause of the cardiac murmur?
Critical aortic stenosis
. Aortic dissection
. CHF
. Pericardial effusion
. Papillary muscle rupture
52) A 66-year-old retired carpenter presents with chronic shortness of breath upon exertion. He has smoked one pack of cigarettes per day for the past 5 years and drinks alcohol regularly. Physical examination reveals a displaced point of maximal impulse and hepatosplenomegaly. His medications include pantoprazole for gastroesophageal reflux and sertraline for depression. Echocardiogram reveals an ejection fraction of 30% and dilated left and right ventricles. Laboratory tests show: Na+: 129 mEq/L, K+: 5.2 mEq/L, Cl−: 101 mEq/L, Blood urea nitrogen: 45 mg/dL, Creatinine: 1.3 mg/dL, Glucose: 134 mg/dL, Aspartate aminotransferase: 220 U/L, Alanine aminotransferase: 140 U/L, Alkaline phosphatase: 280 U/L. Which of the following is the most likely cause of his cardiac findings?
Borrelia burgdorferi
Cigarette smoking
Coxsackie B virus
Ethanol
Pantoprazole toxicity
53) A 47-year-old woman who is 2 weeks post triple bypass surgery presents to the emergency department with a chief complaint of sudden onset, sharp chest pain for several hours. She is fatigued and short of breath. On physical examination she has distended neck veins that grow more distended on inspiration. Muffled heart sounds are heard. Her temperature is 37.0°C (98.6°F), pulse is 133/min, blood pressure is 70/50 mmHg, respiratory rate is 30/ min, and oxygen saturation is 100% on room air. An echocardiogram shows a large pericardial effusion and chamber collapse; therefore, pericardiocentesis is performed. Although a large amount of blood is aspirated, the patient’s clinical picture acutely worsens. Her pain level increases substantially; pulse is 150/min, blood pressure is 60/41 mm Hg, respiratory rate is 30/ min, and oxygen saturation is 100%. Repeat echocardiography shows an even larger pericardial effusion with chamber collapse. Which complication of pericardiocentesis is most likely in this patient?
Acute left ventricular failure with pulmonary edema
Aspiration of 10 mL air into the pericardium
Laceration of a coronary vessel
Pneumothorax
Puncture of the left ventricle
54) A 29-year-old man is brought to the ED by EMS for a syncopal episode that occurred during a basketball game. A friend states that the patient just dropped to the ground shortly after scoring a basket on a fast break. On examination, you note a prominent systolic ejection murmur along the left sternal border and at the apex. An ECG reveals left ventricular hypertrophy, left atrial enlargement, and septal Q waves. You suspect the diagnosis and ask the patient to perform the Valsalva maneuver while you auscultate his heart. Which of the following is most likely to occur to the intensity of the murmur with this maneuver?
. Decrease
. The intensity stays the same, but the heart skips a beat
. Disappear
. Remain unchanged
. Increase
55) A 32-year-old man is brought to the emergency department by paramedics after being found wandering downtown, apparently delirious and agitated. During transport to the hospital the patient becomes diaphoretic and tremulous and has a blood pressure to 163/100 mmHg, pulse of 102/min, and temperature of 39°C (102.2°F). On examination the patient has dilated pupils and ulcerations of his nasal septum mucosa with the residue of a white powder along the nasal alae in addition to his tachycardia, hypertension, hyperthermia, and agitation. Which of the following is the reason why nonselective βblockers should be avoided in this patient?
Increased risk of late vasospasm
Risk of acutely worsening hypertension through vasoconstriction
Risk of causing acute hypotension
Risk of causing dyspnea
Risk of ventricular arrhythmia
56) A 72-year-old woman had a pacemaker inserted 4 years ago for symptomatic bradycardia because of AV nodal disease. She is clinically feeling well and her ECG shows normal sinus rhythm at a rate of 68/min but no pacemaker spikes. Her pacemaker only functions when the ventricular rate falls below a pre-set interval. Which of the following best describes her pacemaker function?
Asynchronous
Atrial synchronous
Ventricular synchronous
Ventricular inhibited
Atrial sequential
57) A 47-year-old man is found to have edema, ascites, and hepatosplenomegaly. The examination of his neck veins reveals elevated venous pressure with a deep y descent. Heart size on x-ray is normal. Which of the following etiologies is not a possible explanation for this syndrome?
Rheumatic fever
TB
Unknown cause
Previous acute pericarditis
Neoplastic involvement of the pericardium
58) A 62-year-old man has progressive symptoms of dyspnea, and more recently noticed difficulty lying supine. Examination shows an elevated JVP at 8 cm, with a third heart sound, pedal edema, and bibasilar crackles on auscultation. Which one of the following may be implicated in fluid retention for this condition?
Decreased renin
Increased aldosterone
Increased estrogen
Increased growth hormone
Decreased vasopressin
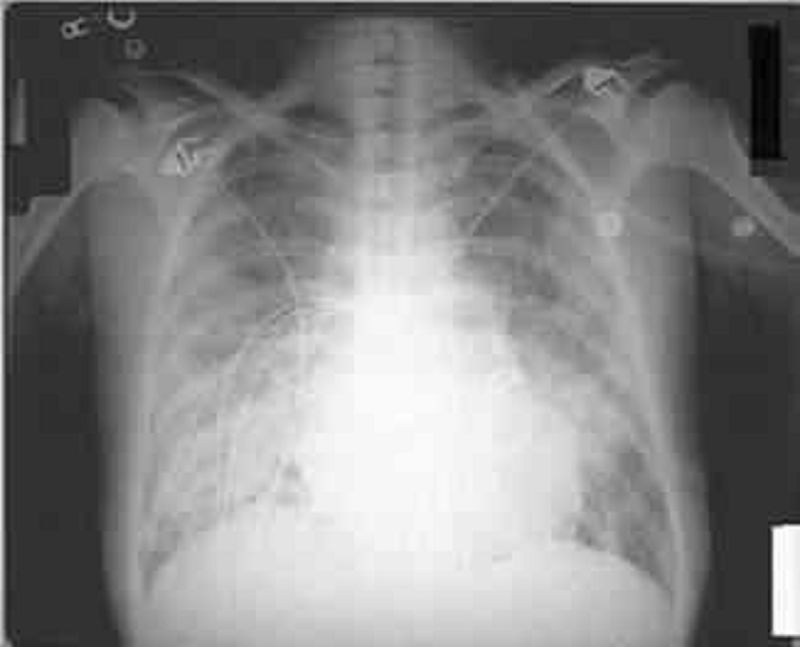
59) A 80-year-old man with Type II diabetes and hypertension presents with increasing dyspnea. He appears short of breath, blood pressure is 170/95 mmHg, pulse 100/min and regular. The JVP is at 7 cm; there is a loud second heart sound and a systolic ejection murmur at the right sternal border, which does not radiate. The lungs have bibasilar crakles up to the scapula. The CXR has bilateral infiltrates and vascular redistribution. His echocardiogram reports aortic sclerosis, concentric left ventricular hypertrophy (LVH), and normal ejection fraction. Which of the following is the most likely mechanism for this condition?
Valvular heart disease
Diastolic dysfunction
Systolic dysfunction
Hibernating myocardium
Hypertrophic obstructive cardiomyopathy (HOCM)
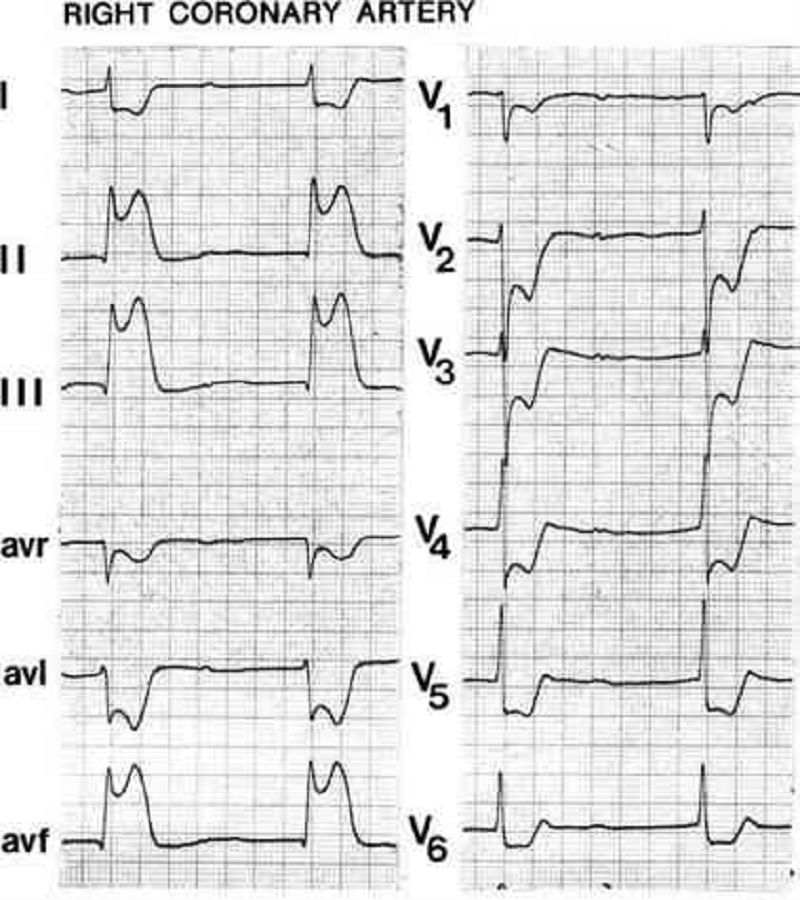
60) A 68-year-woman with hypertension and dyslipidemia presents with 30 minutes of retrosternal chest pain radiating to her neck. She is diaphoretic and in moderate distress. The ECG shows ST-segment elevation in the inferior leads. Which of the following mechanisms is the most likely cause of her condition?
Coronary plaque rupture
Aortic inflammation
Pericardial inflammation
Vasculitis
Myocarditis
61) A 72-year-old man with coronary artery disease and hypertension is hospitalized after suffering a myocardial infarction 5 days ago. He suddenly complains of severe chest pain. His blood pressure is 90/60 mmHg and heart rate is 65/min. Auscultation reveals no murmurs or rubs. An ECG reveals sinus rhythm with an acute ST-segment elevation in the anteroseptal area. Urgent bedside echocardiography showed anteroseptal, lateral, and apical akinesis, mild left ventricular systolic dysfunction, and severe pericardial effusion. Within 20 minutes he is unconscious with undetectable pulses and blood pressure. What is the most likely cause of the patient’s sudden decompensation?
Free wall rupture
Left ventricular thrombus
Mitral regurgitation
Pericarditis
Ventricular septal rupture
62) While palpating the pulse of a patient, you note that the pulse wave has two peaks. You auscultate the heart and are certain that there is only one heartbeat for each two pulse waves. Which of the following best describes this finding?
Pulsus alternans
Dicrotic pulse
Pulsus parvus et tardus
Pulsus bigeminus
Pulsus bisferiens
63) A 62-year-old man with a prosthetic aortic valve develops fevers and malaise. His valve was replaced 5 years ago because of aortic stenosis from a bicuspid valve. He has a systolic ejection murmur but no other abnormalities on examination. Blood cultures are most likely to grow which of the following?
Fungi
Bartonella
Diptheroids
Staphylococcus epidermidis
Streptococcus bovis
64) A 28-year-old man with a history of intravenous drug abuse presents to the emergency department with a 2-day history of fever, chills, and shortness of breath. On physical examination the patient has a new heart murmur, small retinal hemorrhages, and subungual petechiae. Which of the following is the most likely causative organism?
Group A Streptococcus
Mycobacterium tuberculosis
Staphylococcus aureus
Streptococcus viridans
Staphylococcus epidermidis
65) A 91-year-old woman presents to the emergency department with a chief complaint of shortness of breath over the past 2 days. She has a history of hypertension and coronary artery bypass surgery 25 years earlier. Her blood pressure is 178/92 mmHg and she has jugular venous distension, hepatomegaly, and 3+ lower extremity edema. ECG is remarkable for left ventricular hypertrophy, no ST-segment elevations or depressions, no Q waves, and no T wave abnormalities. Echocardiogram reveals an ejection fraction of 60% and left atrial dilatation. There is universal left ventricular thickening. No valvular regurgitation or stenosis was noted. Which of the following underlying conditions is the most likely cause of this patient’s symptoms?
Hypertensive heart disease
Hypertrophic obstructive cardiomyopathy
Ischemic heart disease
Mitral valve prolapse
Myocarditis
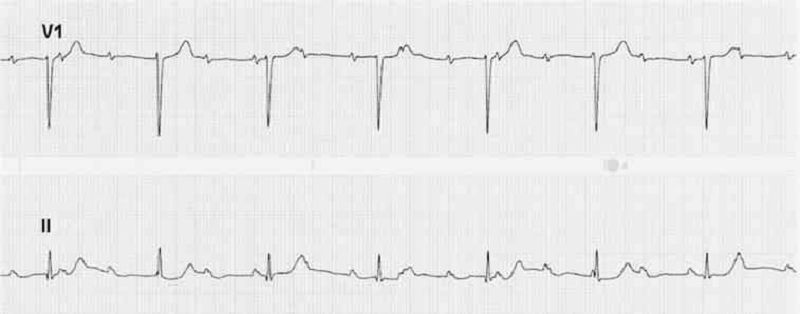
66) A 69-year-old woman complains of easy fatigue and one episode of presyncope. On examination of the jugular venous pressure (JVP), there are irregular large a waves. The ECG has fixed PP and RR intervals but varying PR intervals. Which of the following conditions is this most likely caused by?
Surgical removal of an atrium
Independent beating of atria and ventricles
A reentry phenomenon
A drug effect
A heart rate under 60 beats/min
67) A 47-year-old woman has new-onset transient right arm weakness and word finding difficulty symptoms lasting 3 hours. She is also experiencing exertional dyspnea, and had a syncopal event 1 month ago. Her echocardiogram reveals a cardiac tumor in the left atrium, it is pendunculated and attached to the endocardium. Which of the following is the most likely cause of this lesion?
Myxoma
lipoma
Fibroma
rhabdomyoma
Sarcoma
68) A 23-year-old man develops sharp left-sided chest pain, fever, and a friction rub heard at the lower left sternal border, unaffected by respiration. The pain is also aggevated by lying down and relieved by sitting up. He is otherwise well with no other symptoms and the remaining physical examination is normal. Which of the following is the most likely cause for his symptoms?
Rheumatic fever
Tuberculosis (TB)
Herpes simplex virus
MI
Coxsackievirus
69) A 17-year-old girl develops exertional dyspnea, but has no cough, sputum, or wheezing symptoms. On examination, she has a fixed splitting of her second heart sound and a 3/6 systolic ejection murmur heard best over the left sternal border. An echocardiogram confirms the condition. Which of the following is the best physiologic explanation for her condition?
Pulmonary blood flow is greater than systemic blood flow
Pulmonary blood flow is less than systemic blood flow
Pulmonary blood flow is equal to systemic blood flow
The left ventricle is enlarged
The systemic blood pressure is elevated
70) A 65-year-old man comes to the office and complains of pain and a rash with blisters over the left side of his chest. He has experienced pain over the area for the past 2 days. This morning, he noticed blisters while changing his shirt. He also complains of malaise and headache. His pulse is 82/min, blood pressure is 140/90 mmHg, respirations are 14/min and temperature is 36.8°C (98.4°F). Physical examination reveals grouped, tense vesicles arranged in a band along the left side of his chest. Which of the following is the most likely etiology of his condition?
. Herpes simplex virus
. Varicella zoster virus
. Poison ivy
. Human papilloma virus
. Poxvirus
71) A 65-year-old man comes to the office with a six-month history of a non-healing ulcer on his right forearm. Physical examination demonstrates a scaling plaque with central ulceration and 1.5 cm diameter. The biopsy shows polygonal cells with atypical nuclei at all levels of the epidermis with zones of keratinization. What is the single most important risk factor for this condition?
. Sunlight
Arsenic
. Chronic scars
. Chronic osteomyelitis
. Aromatic hydrocarbons
72) A 35-year-old Caucasian male with aplastic anemia undergoes bone marrow transplantation. The donor is an HLA-matched sibling. Two weeks after the procedure, he develops a maculopapular pruritic rash that is predominantly found on his face, hands, and feet. He also complains of diarrhea. The stool is positive for occult blood. Liver function tests are abnormal. Which of the following is the most likely pathophysiologic mechanism of this patient's condition?
. Activation of the donor T lymphocytes
. Depression of the donor myelopoiesis
. Virus-induced lymphocyte proliferation
. Activation of the host T lymphocytes
. Activation of the donor 8-lymphocytes
73) A 36-year-old male AIDS patient comes in due to a painful red eye. He complains of pain, discharge and redness in his left eye for the past 10 days. On physical examination, you notice redness in his left eye as well as multiple skin lesions on his face, left eyelid, inner thighs, penis and pubis. The lesions are painless, pale, shiny, dome-shaped papules with a central umbilication measuring 2-5mm in diameter. These lesions were not present on his previous visit. His CD4 count thirty days ago was 100/uL. What is the most likely etiology of this patient's skin lesions?
Human herpes virus 8
. Human papilloma virus
. Herpes simplex 1
. Poxvirus
. Staphylococcus
74) A 25-year-old woman comes to the office for the evaluation of pale patches of skin around her mouth. She noticed these lesions a few months ago, but they have become more prominent now. There is no itching, burning, or numbness over the patches. Her vital signs are stable. On examination, you notice pale white patches symmetrically distributed around her mouth. The borders of these macules are well-circumscribed and hyperpigmented. Similar lesions are also found over the areola of her breasts. She denies any history of trauma or infection. Which of the following best explains the pathology of her condition?
. Post inflammatory
Destruction of melanocytes
. Superficial fungal infection
. Infection with mycobacterium leprae
. Inherited absence of melanocytes
75) An 8-year-old boy is brought to the office by his mother for a routine check-up. He has fair skin, blond hair and blue eyes. His past medical history is insignificant. His mother wants to know what the best possible photo-protection is for her son, because "his skin has always been sensitive to the sun, and he is almost unable to tan." He had two episodes of sunburn recently. Physical examination reveals several junctional nevi. Which of the following is the best response to this patient's mother?
Reassure and provide routine care
. Emphasize that clothing is typically useless for sun protection
. Rest under trees or umbrellas during the day
. Minimize sun exposure in the middle of the day
. Recommend applying sunscreens before sun exposure
76) A 30-year-old female presents with a circumferential pruritic rash over her right wrist. The rash has been present for the last two days, and she denies ever having a similar rash before. She bought a new bracelet two weeks ago, and has been wearing it on her right forearm since. Which of the following metals in jewellery is most likely to cause such symptoms?
Copper
. Nickel
. Platinum
. Gold
. Silver

77) A 31-year-old male presents to your office with a velvety skin rash in his axilla as shown on the slide below. Which of the following is the most likely cause of this patient's condition?
Vitamin D resistance
. Serotonin hypersecretion
. Insulin resistance
. Testosterone unresponsiveness
. Calcitonin hypersecretion
78) A 9-year-old boy is brought to the office by his mother because of itching, burning and oozing skin lesions on both of his legs. The boy appears tanned. When asked if he had been spending time outdoors, he replies with great excitement that he just returned yesterday from a camping trip in the woods with his dad. Physical examination of both lower limbs reveals vesicles with erythema arranged in a linear fashion. Weepy and crusted lesions and edema are also present. What type of reaction is responsible for this boy's lesions?
IgE mediated hypersensitivity
. Woods biopsy
. Cell mediated hypersensitivity
. Immune complex mediated hypersensitivity
. Antibody mediated hypersensitivity
79) A 15-year-old male is brought to the emergency department due to sudden-onset difficulty breathing for the past 45 minutes. He also complains of nausea, colicky abdominal pain and a swollen face. He has been suffering from bronchitis for the past 4 days, and his condition had been improving. His mother says that he had a similar episode when he had a tooth extraction 2 year ago. On examination, there is an edematous swelling of his face including the lips, hands, arms, legs, and genitals. His pulse is 82/min, blood pressure is 120/80 mmHg, respirations are 18/min and temperature is 36.8°C (98.4°F). Which of the following best explains the pathological process of his condition?
Depressed C1q
. Cell mediated hypersensitivity
. Immune complex mediated hypersensitivity
. C 1 inhibitor deficiency
. Antibody mediated hypersensitivity
80) A 32-year-old Asian female presents to the office with a mole on her foot that recently became darker. She has always had skin that is very sensitive to sunlight. She is unable to tan, and has had several sunburns when she did not use sunscreens. Her past medical history is insignificant. Her mother had 'a kind of skin cancer.' Physical examination reveals a dark mole with irregular borders on the left foot. Which of the following is the strongest risk factor for malignancy in this patient?
Asian race
. Previous sunburns
. Sun sensitivity
. Recently changed mole
. Age
81) A 25-year-old complains of fever and myalgias for 5 days and now has developed a macular rash over his palms and soles with some petechial lesions. The patient recently returned from a summer camping trip in Tennessee. Which of the following is the most likely cause of the rash?
. Contact dermatitis
. Undercooked pork
. Contaminated water
. Tick exposure
. Sexual exposure
82) A 53-year-old female presents to the clinic with an erythematous lesion on the dorsum of her right hand. The lesion has been present for the past 7 months and has not responded to corticosteroid treatment. She is concerned because the lesion occasionally bleeds and has grown in size during the past few months. On physical examination you notice an 11-mm erythematous plaque with a small central ulceration. The skin is also indurated with mild crusting on the surface. Which of the following is true about this process?
It is a malignant neoplasm of the keratinocytes with the potential to metastasize
. It is the most common skin cancer
. It is a malignant neoplasm of the melanocytes with the potential to metastasize
. It is a chronic inflammatory condition, which can be complicated by arthritis of small and medium- sized joints
. It is an allergic reaction resulting from elevation of serum IgE

83) A 46-year-old construction worker is brought to the clinic by his wife because she has noticed an unusual growth on his left ear for the past 8 months (see photo below). The patient explains that, except for occasional itching, the lesion does not bother him. On physical examination, you notice an 8-mm pearly papule with central ulceration and a few small dilated blood vessels on the border. What is the natural course of this lesion if left untreated?
This is a benign lesion and will not change
. Disseminated infection resulting in septicemia
. Local invasion of surrounding tissue and metastasis via lymphatic spread
. Regression over time
. Local invasion of surrounding tissue
84) A 34-year-old homosexual male with a history of HIV presents to the clinic complaining of a wheezing and multiple violaceous plaques and nodules on his trunk and extremities. Physical examination of the oral mucosa reveals similar findings on his palate, gingiva, and tongue. Chest x-ray is also significant for pulmonary infiltrates. What is the most likely pathogenesis of this process?
Proliferation of neoplastic T cells
. Disseminated HSV infection
. Angioproliferative disease caused by infection with human herpesvirus 8
. Infection with Mycobacterium avium due to decreasing CD4 count
. Infection with human herpesvirus 6
85) A 40-year-old female presents with altered mental status and confusion. Last year, she was diagnosed with rheumatoid arthritis, for which she is currently using indomethacin and methotrexate. Her temperature is 37°C (98.6°F), pulse is 75/min, blood pressure is 110/70 mmHg, and respirations are 15/min. She is disoriented and irritable. Mucus membranes are moist. There is no jugular venous distention. Lungs are clear to auscultation. Abdomen is soft, nontender and not distended. There is no peripheral edema. Serum chemistry reveals: Sodium 122 mEq/L, Potassium 3.7 mEq/L, Bicarbonate 22 mEq/L, Blood glucose 90 mg/dL, BUN 9.0 mg/dL, Uric acid 3.0 mg/dL. Serum osmolality is 265mOsm/kg, while urine osmolality is 500 mOsm/kg. What is the most likely cause of this patient's hyponatremia?
Mineralocorticoid deficiency
. Diabetes insipidus
. Syndrome of inappropriate ADH secretion
. Nephrotic syndrome
. Advanced renal failure
86) A 25-year-old woman comes into the office with a three-month history of weight loss, irritability, insomnia, and palpitations. Her past medical history is insignificant. She is not taking any current medications and denies drug abuse. Her blood pressure is 155/70 mmHg and heart rate is 110/min. Physical examination reveals lid retraction, fine tremor of the hands, and increased neck circumference. The most probable cause of hypertension in this patient is?
. Hyperdynamic circulation
. Increased peripheral vascular resistance
. Sodium retention
. Increased intravascular volume
. Decreased vascular compliance
87) A 55-year-old Caucasian male presents to the office for a routine check-up. He has no present complaints. His past medical history is significant for a long history of hypertension. He does not smoke or consume alcohol. His current medications are enalapril and hydrochlorothiazide. His blood pressure is 140/90 mmHg and heart rate is 80/min. Physical examination reveals a moderately overweight man (BMI = 27 kg/m2) with a waist circumference of 41 inches. The laboratory studies show: Fasting blood glucose 112 mg/dl, Total cholesterol 220 mg/dl, LDL cholesterol 140 mg/dl, Triglycerides 240 mg/dl. Which of the following is the most important pathogenic factor for this patient's condition?
Impaired secretion of insulin
. Insulin-mediated vasodilatation
. Sympathetic hyperactivity
. Insulin resistance
. Low absolute values of insulin
88) A 38-year-old Mexican male presents to the emergency department with a history of weight loss, fever, cough with sputum, nausea, abdominal pain, and postural dizziness for the last three months. Adrenal insufficiency is suspected, and cosyntropin (synthetic ACTH) stimulation test is performed. The rise of serum cortisol following an injection of cosyntropin is grossly subnormal. CT scan of the abdomen shows calcification of both adrenal glands. What is the most likely cause of this patient's adrenocortical insufficiency?
Human immunodeficiency virus infection
. Adrenal haemorrhage
. Adrenal tumor
. Autoimmune adrenalitis
. Tuberculosis
89) A 60-year-old Caucasian male is brought to the emergency department by his daughter due to a 2day history of confusion and lethargy. According to his daughter, he had been complaining of fatigue, anorexia, polyuria and constipation for the last several weeks. He smokes two packs of cigarettes daily, and consumes alcohol occasionally. His blood pressure is 130/90 mmHg and heart rate is 90/min. Physical examination reveals a somnolent patient who is not oriented in time. His lab values are: Serum Na 140 mEq/L, Serum K 4.0 mEq/L, Serum chloride 100 mEq/L, Serum bicarbonate 22 mEq/L, Serum creatinine 1.6 mg/dl, Serum calcium 13.4 mg/dL, Serum phosphorus 2.2 mg/dL, Blood glucose 100 mg/dL, Alkaline phosphatase 80 U/L. Chest x-ray demonstrates a right middle lobe mass and perihilar adenopathy. What is the most probable cause of this patient's symptoms?
Elevated PTH
. Local cytokine production
. Increased vitamin D production
. Metastatic osteolysis
. Parathyroid hormone-like peptide
{"name":"Quiz 1 Ep13", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"20) Patient de 34 ans est admis aux urgences ce matin pour accident de la circulation. Il a son coude gauche gonflé et sa main gauche est soutenue par sa main droite. Toute tentative de mobilisation provoque de douleur intense et un bruit de craquement. Radiographie montre fracture supra-condylienne de l’humérus gauche. Concernant son traitement orthopédique, quelle est la complication souvent rencontrée par une immobilisation en hyper flexion?, 21) Une femme âgée de 35 ans, droitier a senti une douleur latérale du coude gauche après avoir nettoyé un sous-sol inondé et fait essorage des chiffons imbibés d'eau. Les résultats de la radiographie sont négatifs. Il y a une douleur et un légère gonflement sur l'épicondyle latéral de l'humérus. Anatomiquement, cette condition peut être expliqué par lequel des éléments suivants?, 22) Un homme de 40 ans est admis aux urgences ce matin pour accident par chute sur la main en l’extension. A l’examen Clinique toute tentative de mobilisation provoque de douleur, élargissement du coude dans le sens antéro-postérieur, raccourcissement apparent de l’avant bras et saillie de l’olécrane en arrière, pas d’ echomose .Quel est le diagnostic le plus probable?","img":"https://cdn.poll-maker.com/11-511311/7.jpg?sz=1200"}
More Quizzes
Space
520
Tutorial Assessment
9466
Which Experiential Learning Opportunity is Best for You?
9417
ΑΠΘ - Reunion 2017
740
General Knowledge - ProProfs Challenge (Free)
201028050
Are Lithium-Ion Batteries Wet-Cell? True or False
201023461
Is My Child Spoiled - Free Parent Self-Check
201019756
Am I Emo - Emo, Poser or Normal? Free Results
201021093
The Weeknd - Test Your Fan Knowledge
201029367
6th Grade Reading Comprehension Test - Free Practice Online
201020621
What Is My House Sigil? Free to Find Yours
201022126
How to Speak Pig Latin - Test Your Skills Free
201020621