
DES 2016. Final (Part 16)
23) A 21-year-old woman visits her physician because of 3 weeks of a flu-like‖ illness. She reports symptoms of malaise, fever, fatigue, and a sore throat. There is no weight loss or night sweats, and she has not traveled out of country. Her past medical history is not significant and she is not taking any medications. Physical examination is normal except for enlarged cervical lymph nodes. Laboratory data show hemoglobin 13.2 g/dL; hematocrit 42%; platelets 380,000/mL; WBC 8500/mL, with 35% segmented neutrophils, 1% eosinophils, and 64% lymphocytes, of which 36% were atypical. A heterophil antibody (sheep cell agglutination) test is negative. Which of the following is the most likely causative organism?
Herpes simplex
Echovirus
CMV
Coxsackievirus
Reovirus
24) A 4-year-old boy is sent to the emergency room because of clinical suspicion of meningitis. He has been ill for 2 days with fever and lethargy. On examination, he is febrile, the neck is stiff, and papilledema is present. There is no rash, the lungs are clear, and heart sounds normal. Which of the following is the most likely causative organism?
Neisseria meningitidis
Streptococcus pneumoniae
Haemophilus influenzae
Staphylococcus
Listeria species
25) A 24-year-old woman presents with chills and rigors. She looks unwell, and her temperature is 39.4°C, blood pressure 100/60 mm Hg, pulse 110/min, and oxygen saturation 95%. There is a 3/6 pansystolic murmur at the right sternal border, which increases with inspiration. Her arms have multiple tattoos and needle marks from injection drug use. Blood cultures (2/2 sets) are positive for S. aureus, and she is started on appropriate antibiotics. Her renal function is mildly impaired and her urinalysis is positive for protein, and microscopy reveals red cell casts. Which of the following mechanisms is the most likely explanation for her renal abnormalities?
Septic emboli
Cardiac failure with prerenal azotemia
A high level of circulating immune complexes
Fungal disease
Inevitable progression to renal failure
26) A recent outbreak of severe diarrhea is currently being investigated. Several adolescents developed bloody diarrhea, and one remains hospitalized with acute renal failure. A preliminary investigation has determined that all the affected ate at the same restaurant. The food they consumed was most likely to be which of the following?
Pork chops
Hamburger
Gefilte fish
Sushi
. Soft-boiled eggs
28) An 18-year-old man develops fever, neck stiffness, and headache. On examination, his blood pressure is 105/80 mm Hg, pulse 100/min, temperature 38.7°C, and neck flexion is very painful. The ears, throat, and sinuses are normal; there are no focal neurologic signs, and the remaining examination is normal. His is the second case of meningitis in his university dormitory building. Which of the following is the most likely causative organism?
Neisseria meningitidis
Streptococcus pneumoniae
Haemophilus influenzae
Staphylococcus
Listeria species
121) A 43-year-old woman with congestive heart failure, rheumatoid arthritis and chronic hepatitis C complains of abdominal discomfort and difficulty breathing. Physical examination shows dullness to percussion at the right lung base. Chest x-ray reveals a large right-sided pleural effusion. Thoracentesis yields pleural fluid with a glucose content of 30 mg/dl and an LDH of 192units/L. Which of the following explains the pleural fluid glucose concentration?
Increased pleural membrane permeability
Increased capillary hydrostatic pressure
Increased permeability of the right hemidiaphragm
High white blood cell content of the pleural fluid
High amylase content of the pleural fluid
27) A 23-year-old woman presents with a painless chronic vulvar ulcer. She recently arrived to study in the United States from Southern India. The lesion began as a papule and then ulcerated. It has persisted for several months. Currently, physical examination reveals a painless elevated area of beefy red, friable granulation tissue. She has been sexually active for several years. Which of the following is the most likely causative organism?
Spirochete
Gram-positive coccus
Intracellular Gram-negative bacteria
Chronic viral infection
Fungus
29) A 19-year-old woman was traveling in a rural area of South America. She returned 3 weeks ago and, over the past few days, has gradually developed lower abdominal pain and diarrhea. Now the symptoms are much worse with 10 stools a day consisting mostly of mucus and blood. She is afebrile, the abdomen is tender in left lower quadrant, and the remaining examination is normal. Her stool is mostly comprised of blood and mucus. Which of the following is the most likely causative organism?
Escherichia coli infection
Salmonella infection
Shigella infection
Vibrio parahaemolyticus infection
E. Histolytica infection
30) An 18-year-old man develops fever, neck stiff- ness, and headache. On examination, his blood pressure is 110/80 mm Hg, pulse 100/min, temperature 38.7°C, and neck flexion is very painful. The ears, throat, and sinuses are normal; there are no focal neurologic signs; and the remaining examination is normal. There are no reported similar cases in the community. Which of the following is the most likely causative organism?
Neisseria meningitides
Streptococcus pneumoniae
Haemophilus influenzae
Staphylococcus
Listeria species
31) A previously well 28-year-old female has developed gradual onset of fever and malaise over 2–3 weeks. She also complains of arthralgias and myalgias. Repeated measurement of her temperature reveals a low grade fever between 38°C and 39°C. Physical examination reveals an oval retinal hemorrhage with a clear, pale center; a pansystolic cardiac murmur heard best at the apex; and small, tender nodules on her fingertips. Which of the following is the most likely causative organism?
Staphylococcus aureus
Viridans streptococci
S. epidermidis
Enterococcus
Candida
32) A 70-year-old patient with long-standing type 2 diabetes mellitus presents with complaints of pain in the left ear with purulent drainage. On physical examination, the patient is afebrile. The pinna of the left ear is tender, and the external auditory canal is swollen and edematous. The white blood cell count is normal. Which of the following organisms is most likely to grow from the purulent drainage?
Pseudomonas aeruginosa
Streptococcus pneumoniae
Candida albicans
Haemophilus influenzae
Moraxella catarrhalis
33) Three hours after a church social, eight people develop severe diarrhea. Other symptoms included nausea, vomiting, and abdominal cramps. Food served included chicken salad and cream-filled pastries. All affected individuals had the chicken salad. Which of the fol- lowing is the most likely causative organism?
Staphylococcal enterotoxin
C. botulinum
Clostridium perfringens
Salmonella species
Ptomaine poisoning
34) A 9-year-old boy has a severe sore throat with fever and dysphagia. On examination, there are grayish-white papulovesicular lesions on an erythematous base that ulcerate. They are located on the soft palate, anterior pillars of the tonsils and uvula. There are no lesions on the gingiva, tongue, or lips. A clinical diagnosis of herpangina is made. Which of the following is the most likely causative organism?
Measles (Morbillivirus)
Rubella (rubivirus)
Coxsackievirus A
HSV-1
HSV-2
35) A 10-year-old boy presents with fever, headache, photophobia, and neck discomfort in the middle of summer. He is alert and oriented, but has neck pain with flexion and extension of the head. His fundi are normal, and there are no focal neurologic findings or skin changes. A lumbar puncture reveals normal protein and glucose with a cell count of 240/mL (90% lymphocytes). Which of the following is the most likely causative organism?
Enterovirus (coxsackievirus or echovirus)
Streptococcus pneumoniae
Neisseria meningitides
Listeria monocytogenes
HSV-1
36) A 60-year-old man presents with fever and malaise 6 weeks after mitral valve replacement. On examination, his temperature is 38°C, blood pressure 130/80 mm Hg, pulse 80/min, and a loud pansystolic murmur at the apex, which radiates to the axilla. He has no skin or neurologic findings. Which of the following is the most likely causative organism?
Staphylococcus aureus
A fungus
Staphylococcus saprophyticus
Pneumococcus
Staphylococcus epidermidis
37) A previously healthy 25-year-old music teacher develops fever and a rash over her face and chest. The rash is itchy and, on examination, involves multiple papules and vesicles in varying stages of development. One week later, she complains of cough and is found to have an infiltrate on x-ray. Which of the following is the most likely etiology of the infection?
Streptococcus pneumoniae
Mycoplasma pneumoniae
Histoplasma capsulatum
Varicella-zoster virus
Gonococcus pneumoniae
38) A 19-year-old male has a history of athlete’s foot but is otherwise healthy when he develops sudden onset of fever and pain in the right foot and leg. On physical examination, the foot and leg are fiery red with a welldefined indurated margin that appears to be rapidly advancing. There is tender inguinal lymphadenopathy. The most likely organism to cause this infection is which of the following?
Staphylococcus epidermidis
Tinea pedis
Streptococcus pyogenes
Mixed anaerobic infection
Alpha-hemolytic streptococci
39) A 60-year-old woman comes to the physician because of a 3-month history of worsening fatigue and back pain. She has had diabetes mellitus for the past three years, and hypertension for the past ten years. Laboratory studies show: Hb 9.0 mg/dL, Serum calcium 11.2 mg/dL, Serum phosphorus 3.5 mg/dL, BUN 38 mg/dL, Serum creatinine 2.0 mg/dL. Which of the following is the most likely cause of this patient's renal failure?
. Hypertension
Diabetes mellitus
Para protein
Primary hyperparathyroidism
Renal artery stenosis
40) A 70-year-old man comes to the physician due to a 4-6 month history of "almost continuous urinary dribbling." This symptom is present both day and night, and is progressively getting worse. He denies dysuria and hematuria. He has a 20-year history of diabetes mellitus-type 2, hypertension, alcoholic hepatitis and coronary artery disease. He had a gastric emptying study done a few weeks ago because of continuous nausea and early satiety. He had laser photocoagulation of both eyes for diabetic retinopathy. He has smoked one pack of cigarettes daily for 50 years, and drinks 4 to 6 beers daily. He takes NPH insulin, regular insulin, metformin, aspirin, metoprolol, lisinopril and metoclopramide. His vital signs are stable. Physical examination shows a well-appearing man. Pertinent physical findings are a normal sized prostate, decreased sensation in both legs below the knees, and absent Achilles tendon and knee reflexes bilaterally. Fecal occult blood test is negative. Postvoid residual volume is 550 ml. Urinalysis shows: Specific gravity 1.020, Blood trace, Glucose positive, Ketones negative, Protein moderate, Leukocyte esterase negative, Nitrites negative, WBC 1-2/hpf, RBC 3-4/hpf. Which of the following is the most likely cause of this patient's incontinence?
Multiinfarct dementia
Overflow incontinence due to detrusor weakness
Overflow incontinence from bladder outlet obstruction
. Urinary tract infection
Overflow incontinence due to medication
41) A 46-year-old man complains of right flank discomfort. He describes decreased urination over the last week with occasional episodes of high urine output and weakness. He is otherwise healthy. There is no family history of renal disease. On physical examination, his blood pressure is 140/90 mmHg and his heart rate is 80/min. The serum creatinine level is 2.1 mg/dl. Urinalysis shows few red blood cells, white blood cells, trace protein, and no casts. Which of the following is the most likely cause of his complaints?
Hematologic malignancy
Renal artery stenosis
Inherited renal disease
Interstitial nephritis
Urinary outflow obstruction
42) A 17-year-old man comes to the emergency department and complains of intensive left flank pain that radiates to the groin. He refers to his symptom as "stone passage," which he has experienced "for so many times since childhood." His uncle has the same problem. Urinalysis shows hexagonal crystals. The urinary cyanide nitroprusside test is positive. Which of the following is the most likely cause of this patient's condition?
Amino acid transport abnormality
Parathyroid adenoma
Abnormality of uric acid metabolism
Excessive intestinal reabsorption of oxalate
Infection
43) A 12-year-old girl comes to the physician because of a 2-day history of periorbital edema and abdominal distention. She has no other complaints. She has never been diagnosed with hypertension. Her father died at the age of 40, with renal failure. Her temperature is 37.1°C (98.9°F), blood pressure is 125/75 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows facial puffiness, shifting dullness, and 1+ bilateral pitting pedal edema. Urinalysis shows 3+ proteinuria and lipid laden casts. 24-hour urinary protein excretion is 5 g/day, total serum protein is 4.5 g/dl and serum albumin is 2.3 g/dl. Which of the following is this patient at increased risk of developing?
Macrocytic normochromic anemia
. Accelerated atherogenesis
Hypergammaglobulinemia
. Hypercalcemia
. Hypoparathyroidism
44) A 20-year-old man is brought to the emergency department by his mother because of a one-day history of fever, headache, and altered mental status. He has no history of medical illness. Herpes simplex encephalitis is suspected after cerebral spinal fluid analysis shows lymphocytic pleocytosis, elevated protein level, and normal glucose level; in addition, CT scan shows contrast enhancement in the temporoparietal area. High-dose intravenous acyclovir therapy is started. Two days after the beginning of the therapy, the neurologic status improves, but the patient develops oliguria. Laboratory studies show: Serum sodium 140 mEq/L, Serum potassium 4.5 mEq/L, Serum creatinine 2.8 mg/dl, BUN 25 mg/dl. Which of the following is the most likely cause of renal damage in this patient?
Prerenal azotemia
. Renal tubular obstruction
Glomerular injury
Interstitial nephritis
Bladder neck obstruction
45) A 65-year-old male has been having a non-productive, hacking cough for over a week. He takes an over-the-counter medication containing guaifenesin and diphenhydramine in an effort to improve his symptoms. The next day, he complains of lower abdominal discomfort and difficulty voiding. Which of the following most likely accounts for this patient's new complaint?
Detrusor inactivity
Urethral obstruction
Detrusor-sphincter dyssynergia
Overactive bladder
Abdominal muscle weakness
46) A 12-year-old girl is brought to the clinic due to a 2-month history of headaches. Her headaches last 1-2 hours and have no fixed time of occurrence. She denies nausea, vomiting, chills or fevers. She has no other medical problems and takes no medication. Her family history is significant for hypertension and diabetes. Her blood pressure is 156/90 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows an alert child in no distress. There is a soft to-and-fro bruit heard at the right costovertebral angle. Which of the following is the most likely cause of her hypertension?
Coarctation of aorta
Renal artery atherosclerosis
Pheochromocytoma
Fibromuscular dysplasia
Conn's syndrome
47) A 59-year-old man comes to the physician because of dysuria, urinary urgency, and frequency. He also complains of hematuria, nocturia, decreased force of stream, and a feeling of incomplete voiding. These symptoms have been present for more than a month. For the past few days he has been experiencing dull, non-radiating suprapubic pain. He has also been having low-grade fever and malaise for the past couple of days. He has been taking analgesics for osteoarthritis of his right knee for more than 10 years. He has a 40-pack-years history of cigarette smoking and does not use alcohol or drugs. Rectal examination shows a smooth, firm enlargement of the prostate without induration or asymmetry. Neurological examination shows no abnormalities. Urinalysis shows hematuria with isomorphic red blood cells. Laboratory studies show a serum creatinine of 1.5 mg/dl, and a PSA of 2 ng/ml. Which of the following is the most likely explanation for this patient's symptoms?
Benign prostatic hyperplasia
Carcinoma of bladder
Carcinoma of prostate
Urethral stricture
Neurogenic bladder
48) An 80-year-old female is brought from a nursing home with a two day history of poor oral intake and lethargy. Her past medical history is significant for hypertension, diabetes mellitus, coronary artery disease with coronary stenting two years ago and Alzheimer's disease. She was hospitalized six months ago with pneumonia. Her current medications are aspirin, lisinopril, metoprolol, hydrochlorothia zide, metformin and memantine. Her blood pressure is 95/60 mmHg and heart rate is 90/min. Physical examination reveals fine crackles at the right lung base. Her mucous membranes are dry. Her laboratory findings are significant for WBC of 15,000/mm3, creatinine of 2.1 and BUN of 61 mg/dl. Her creatinine was 0.9 mg/dl during the last admission. Which of the following is the best explanation for the abnormal laboratory findings in this patient?
Age-related renal function decline
Renal inflammatory infiltration
Renal tubular dysfunction
Renal vasoconstriction
Obstructive uropathy
49) A 60-year-old man comes to the physician because of worsening fatigue and nausea. He had a carotid angiogram for the evaluation of symptomatic carotid artery stenosis 15 days ago, and was discharged home three days after the procedure. His medical problems are hypercholesterolemia, coronary artery disease, intermittent claudication, hypertension for 18 years, and diabetes mellitus for 15 years. Physical examination shows painless, reddish-blue mottling of the skin of the extremities. Laboratory studies show: Hb 10.5 g/dl, WBC 10,000/cmm with 12% eosinophils, BUN 46 mg/dl, Serum creatinine 3.0 mg/dl, Serum C3 level Decreased. Urinalysis:pH Normal,Esterase Negative, Nitrite Negative, Protein 1+, WBC Many eosinophils, RBC 1-2/HPF. Which of the following is the most likely cause of this patient's findings?
Contrast nephropathy
Cholesterol embolism
Diabetic nephropathy
Post streptococcal glomerulonephritis
Acute allergic interstitial nephropathy
50) A 40-year-old man comes to the physician because of a two-week history of fatigue, lower extremity edema and dark urine. He has no history of serious illnesses. He takes no medications. He does not use tobacco, alcohol, or drugs. His blood pressure is 130/80 mm Hg and pulse is 80/min. Physical examination shows symmetric pitting edema of lower extremities. Laboratory studies show a serum creatinine level of 1.1 mg/dl. Urinalysis shows 4+ proteinuria and microhematuria. Light microscopy of the specimen obtained from kidney biopsy shows dense deposits within glomerular basement membrane that stain for C3, not immunoglobulins. Which of the following is the most likely pathophysiologic mechanism that explains this patient's condition?
Anti-GBM antibodies
Circulating immune complexes
Persistent activation of the alternative complement pathway
Cell-mediated injury
Non-immunologic damage
51) A 65-year-old male comes to the physician's office after noticing blood in his urine. He denies any abdominal pain or dysuria. He denies any recent illness. The review of systems is otherwise unremarkable. His past medical history is significant for hypertension and a transient ischemic attack. He takes a baby aspirin and hydrochlorothiazide daily. His temperature is 36.7°C (98°F), blood pressure is 130/86 mm Hg, pulse is 80/min and respirations are 16/min. A complete physical examination is unremarkable. Which of the following is the most likely cause of his symptoms?
Polycystic kidney disease
Renal cell carcinoma
Bladder mass
Acute glomerulonephritis
Schistosoma infection
52) A 62-year-old woman presents to your office complaining of urinary frequency and burning during urination. She denies fever, chills, nausea, back pain or abdominal pain. Her past medical history is significant for a long history of diabetes mellitus and hypertension. She does not use tobacco or consume alcohol. Her blood pressure is 160/100 mmHg and her heart rate is 70/min. Her hematocrit is 43% and her WBC count is 8,500/mm3 Urinalysis reveals the following: Glucose negative, Ketones negative, Nitrates positive, Protein 2+, WBC 20-25/hpf, RBC 3-5/hpf. She is given a three-day course of levofloxacin. Urinalysis two weeks later reveals 2+ protein but no nitrates, WBCs, or RBCs. Which of the following is most likely responsible for her persistent urinalysis abnormality?
Atherosclerotic narrowing of the renal arteries
Glomerular basement membrane changes
Cystic transformation of the renal parenchyma
Parenchymal atrophy due to calyceal dilation
Insoluble crystal precipitation in the tubular lumen
53) A 60-year-old man comes to the physician because of a 2-day history of fever and left-sided scrotal pain. The pain has progressed in severity and it radiates to the flank. His has also had increased urinary frequency and urgency along with dysuria. His temperature is 38.1°C (100.8°F), blood pressure is 130/75mm Hg, pulse is 86/min, and respirations are 15/min. Physical examination shows left scrotal swelling and a tender scrotal mass; there is no urethral discharge. Rectal examination shows a tender prostate. Laboratory studies show a WBC count of 14,000/microl with a left shift. Urinalysis shows bacteriuria and pyuria. Which of the following is the most likely organism responsible for this patient's findings?
Escherichia coli
Pseudomonas
Chlamydia trachomatis
Gonococcus
Staphylococcus aureus
54) A 40-year-old man comes to the physician because of increasing urinary frequency and urgency. He has had these symptoms in the past, but they are more troublesome now. He has also had urinary hesitancy and interruption of flow. His temperature is 37°C (98.6°F), blood pressure is 130/75mm Hg, pulse is 76/min, and respirations are 15/min. Physical examination shows no abnormalities except increased tone of the anal sphincter and mild periprostatic tenderness. Urinalysis and urine culture shows no abnormalities and expressed prostatic secretions show a leukocyte count of four WBCs/HPF (normal is less than 10 WBCs/HPF). Serum prostate-specific antigen is 2 ng/ml (normal value is less than 4ng/ml). Which of the following is the most likely diagnosis?
Chronic bacterial prostatitis
Inflammatory chronic prostatitis
Non-inflammatory chronic prostatitis
Prostatic cancer
Acute bacterial prostatitis
55) A 16-year-old girl presents with a 2-day history of lower abdominal discomfort, burning micturition and increased frequency of urination. She had her first sexual intercourse last week. Her vital signs are stable. Examination shows suprapubic tenderness. Urinalysis shows positive nitrites, positive esterase, 50+ WBC, and many bacteria. Which of the following is the most likely mechanism responsible for her clinical condition?
Sexual transmission
Hematogenous spread of infection
Lymphatic spread of infection
Poor genital hygiene
. Ascending infection
56) A 68-year-old Caucasian man is admitted with a diagnosis of left lower lobe pneumonia, and is started on gatifloxacin. He has a long history of diabetes, hypothyroidism, hypercholesterolemia, and hypertension. He also has diabetic retinopathy, peripheral neuropathy, and nephropathy. He has an arterio-venous fistula placed for a possible dialysis. His medications are insulin, furosemide, atorvastatin, metoprolol and levothyroxine. After having his blood drawn for some laboratory studies today, he bleeds persistently. Laboratory studies show: Hb 11.5 g/dl, Platelets 160,000/cmm, Blood glucose 178 mg/dl, BUN 56 mg/dl, Serum creatinine 3.5 mg/dl. His baseline creatinine level is between 3.2-3.5 mg/dl. Which of the following is the most likely cause of his bleeding?
Disseminated intravascular coagulation
Platelet dysfunction
Factor VIII deficiency
Consumptive coagulopathy
Thrombocytopenia
57) A 56-year-old male with a long history of diabetes mellitus complains of nocturnal urinary frequency, occasional dribbling and difficulty completing his stream. His past medical history is significant for a myocardial infarction two years ago and moderately decreased visual acuity. On physical examination, his blood pressure is 160/100 mmHg and his heart rate is 70/min. There is a carotid bruit auscultated on the left side as well as trace ankle edema. Post-void bladder catheterization yields 60 ml of urine. Dipstick urinalysis reveals 2+ protein and 3-4 WBC/hpf. The patient's serum creatinine level is 2.4 mg/dl. Which of the following is the most likely cause of his renal dysfunction?
Ascending infection
Obstructive uropathy
Microangiopathy
Renal hypoperfusion
Cystic kidney disease
58) A 62-year-old man presents to the emergency department with severe back pain that began suddenly after he attempted to lift a heavy box. He says the pain radiates down his right thigh and leg and that coughing and moving make the pain “unbearable” The patient also complains of an inability to urinate since the pain started. On physical examination, he has no focal lower extremity weakness or numbness, and pinprick testing in the perianal area elicits a quick spasm of the anal sphincter. Rectal exam reveals an enlarged, smooth, nontender prostate. Which of the following best explains this patient's urinary retention?
. Severe pain
Nerve root injury
Detrusor instability
Hypertonic bladder
Urethral injury
59) A 25-year-old woman presents with nausea and vomiting of 2 days duration. She is not on any medications and was previously well until now. Her physical examination is normal except for a postural drop in her blood pressure from 110/80 mm Hg supine to 90/80 mm Hg standing. Her serum electrolytes are sodium 130 mEq/L, potassium 3 mEq/L, chloride 90 mEq/L, bicarbonate 30 mEq/L, urea 50 mg/dL, and creatinine 0.8 mg/dL. Which of the following electrolytes is most likely to be filtered through the glomerulus but unaffected by tubular secretion?
Potassium
Sodium
Bicarbonate
Urea
Creatinine
60) A 29-year-old man with HIV, on a highly active antiretroviral therapy (HAART) regimen including the protease inhibitor indinavir, presents with severe edema and a serum creatinine of 2.0 mg/dL. He has had bone pain for 5 years and takes large amounts of acetaminophen with codeine, aspirin, and ibuprofen. He is on prophylactic trimethoprim-sulfamethoxazole. Blood pressure is 170/110 mm Hg; urinalysis shows 4+ protein, 5 to 10 RBC, 0 WBC; 24-hour urine protein is 6.2 g. The serum albumin is 1.9 g/L (normal above 3.7). Which of the following is the most likely cause of his renal disease?
Indinavir toxicity
Analgesic nephropathy
Trimethoprim-sulfamethoxazole–induced interstitial nephritis
Focal glomerulosclerosis
. Renal artery stenosis
61) A 74-year-old man presents with fatigue, short- ness of breath on exertion, and back and rib pain, which is made worse with movement. Investigations reveal he is anemic, calcium, urea, and creatinine are elevated. X-rays reveal multiple lytic lesions in the long bones and ribs, and protein electrophoresis is positive for an immunoglobulin G (IgG) paraprotein. Which of the following is the most likely mechanism for the renal injury?
Plasma cell infiltrates
Tubular damage by light chains
Glomerular injury
Vascular injury by light chains
Uric acid crystals
62) A 23-year-old woman with no other past medical history was diagnosed with hypertension 6 months ago. She was initially treated with hydrochlorothiazide, followed by the addition of lisinopril, followed by high doses of a beta-blocker, but her blood pressure has not been well controlled. She assures the provider that she is taking all of her medicines. On examination her blood pressure is 165/105 mm Hg in each arm, and 168/105 mm Hg when checked by large cuff in the lower extremities. Her pulse is 60. Cardiac examination reveals an S4 gallop but no murmurs. She has a soft mid-abdominal bruit. Distal pulses are intact and equal. She does not have hyperpigmentation, hirsutism, genital abnormalities, or unusual distribution of fat. Her sodium is 140, potassium 4.0, HCO3 22, BUN 15, and creatinine 1.5. Which of the following is the most likely cause of her difficult-to-control hypertension?
Primary hyperaldosteronism (Conn syndrome)
Cushing syndrome
Congenital adrenal hyperplasia
Fibromuscular dysplasia
. Coarctation of the aorta
63) A 60-year-old woman with heart failure and normal renal function is started on furosemide (Lasix) 80 mg/day. She notices a good diuretic response every time she takes the medication. A few weeks later, she is feeling unwell because of fatigue and muscle weakness, but her heart failure symptoms are better. Which of the following is the most likely explanation for her muscle weakness?
Hyponatremia
Hypernatremia
Hypokalemia
Hyperkalemia
Anemia
64) A 65-year-old diabetic man with a creatinine of 1.6 was started on an angiotensin-converting enzyme inhibitor for hypertension and presents to the emergency room with weakness. His other medications include atorvastatin for hypercholesterolemia, metoprolol and spironolactone for congestive heart failure, insulin for diabetes, and aspirin. Laboratory studies include: K: 7.2 mEq/L, Creatinine: 1.8 mg/dL, Glucose: 250 mg/dL, CK: 400 IU/L. Which of the following is the most likely cause of hyperkalemia in this patient?
Worsening renal function
Uncontrolled diabetes
Statin-induced rhabdomyolysis
Drug-induced effect on the renin-angiotensin-aldosterone system
High-potassium diet
65) A 27-year-old alcoholic man presents with decreased appetite, mild generalized weakness, intermittent mild abdominal pain, perioral numbness, and some cramping of his hands and feet. His physical examination is initially normal. His laboratory returns with a sodium level of 140 mEq/L, potassium 4.0 mEq/L, calcium 6.9 mg/dL, albumin 3.5 g/dL, magnesium 0.7 mg/dL, and phosphorus 2.0 mg/dL. You go back to the patient and find that he has both a positive Trousseau and a positive Chvostek sign. Which of the following is the most likely cause of the hypocalcemia?
. Poor dietary intake
Hypoalbuminemia
Pancreatitis
Decreased end-organ response to parathyroid hormone because of hypomagnesemia
Osteoporosis caused by hypogonadism
66) A 27-year-old woman presents to the emergency room with a panic attack. She appears healthy except for tachycardia and a respiratory rate of 30. Electrolytes include calcium 10.0 mg/dL, albumin 4.0 g/dL, phosphorus 0.8 mg/dL, and magnesium 1.5 mEq/L. Arterial blood gases include pH of 7.56, PCO2 21 mm Hg, and PO2 99 mm Hg. Which of the following is the most likely cause of the hypophosphatemia?
Hypomagnesemia
Hyperparathyroidism
Respiratory alkalosis with intracellular shift
Poor dietary intake
Vitamin D deficiency
67) A 57-year-old male is hospitalized for hyponatremia. Physical examination reveals no signs of fluid overload. Serum analysis reveals a sodium concentration of 125mEq/1, glucose level of 12mg/dl, BUN of 8mg/dl, and creatinine of 0.7mg/dl. The urine osmolarity is 330mOsm/l and urine sodium concentration is 45mEq/1. After a 2L normal saline infusion, the serum sodium is 126mEq/1 and the urine sodium excretion is increased to 90 mEq/1. Which of the following is the most likely cause of this patient's hyponatremia?
Inappropriate ADH secretion
Psychogenic polydipsia
Surreptitious diuretic use
Advanced liver disease
Interstitial renal disease
68) A 27-year-old female is brought into the emergency room by the local paramedics. She was found unconscious at the scene of a house fire. On examination it does not appear that she has suffered any burns. Black soot is noted near her nares and mouth. Her respirations are slow but spontaneous. Her capillary refill time is 4 seconds. Supplemental oxygen by a non-rebreather mask is begun. Her arterial blood gas and preliminary laboratory values are shown below: Blood pH 7.22, PaO2 100 mmHg, PaCO2 39 mmHg, HC03- 11 mEq/L, WBC count 9,000/cmm, Hb 14 mg/dl, Na+ 138 mEq/L, K+ 4 mEq/l, CI- 98 mEq/L, Troponin 0.4ng/ml. Which of the following is the most likely primary cause of the patient's acid-base disturbance?
. Increased metabolic rate
Decreased oxygen delivery to tissue
Reduced oxygen utilization by tissues
Impaired excretion of lactic acid
Increased gut absorption
69) A 32-year-old female is brought to the emergency department with complaints of weakness, tingling and numbness of her extremities. She is not on any medication. Her pulse is 90/min, respirations are 14 /min and blood pressure is 110/70 mm Hg. The physical examination is unremarkable. Her laboratory profile is shown below: Blood pH 7.56, HCO3- 37 mEq/L, Urine Na+ 16 mEq/L, Urine K+ 20 mEq/L, Urine Cl- 7 mEq/L, Serum sodium 135 mEq/L, Serum potassium 2.9 mEq/L, Serum chloride 92 mEq/L, Blood urea nitrogen 22 mg/dl, Serum creatinine 0.9 mg/dl. Which of the following is the most likely cause of this patient's condition?
Surreptitious vomiting
Persistent diarrhea
Bartter's syndrome
Type I renal tubular acidosis
Hyperventilation syndrome.
70) A 55-year-old homeless man presents to the emergency room complaining of muscle cramps and perioral numbing. The patient looks malnourished. He says that he consumed a lot of alcohol recently. His past medical history is significant for chronic and recurrent abdominal pain for which he was advised to quit drinking alcohol. His temperature is 36.7°C (98°F), blood pressure is 110/65 mmHg, pulse is 80/min, and respirations are 18/min. The laboratory values are: Hemoglobin 7.2 g/dl, MCV 105 fl, Leukocyte count 9,000/cmm, Platelets 200,000/cmm, ESR 20 mm/hr, Serum sodium 145 mEq/L, Serum potassium 4.0 mEq/L, Serum calcium 6.8 mg/dl, Serum phosphorus 2.5 mg/dl. What is the most probable cause of hypocalcemia observed in this patient?
Renal failure
Primary hypoparathyroidism
Pseudohypoparathyroidism
. Hypoalbuminemia
. Malabsorption
71) A 24-year-old female is brought to the emergency room because of dizziness and near syncope. She says that every time she stands up, she feels lightheaded. She has no significant past medical problems. She does note having broken up with her boyfriend three months ago, which has caused her to have decreased appetite and an associated ten-pound weight loss. She has also missed her last two menstrual periods. She denies using tobacco, alcohol or drugs. On physical examination, her temperature is 36.7°C (98°F). When lying supine, her blood pressure is 100/70 mm Hg and her pulse is 88/min. When she stands up, her blood pressure is 80/50 mm Hg and her pulse is 120/min. Other than dry skin and mucous membranes, her physical examination is unremarkable. Initial laboratory studies reveal: Serum sodium low, Serum potassium low, Urine sodium increased, Urine potassium increased. This patient's dizziness is most likely due to which of the following?
. Low caloric intake
Self-induced vomiting
Laxative abuse
Diuretic abuse
Mineralocorticoid deficiency
72) A 52-year-old alcoholic man presents to the emergency department because of anxiety and tremors. His last drink of alcohol was 2 days ago. His initial electrolyte panel is: Sodium 132 mEq/L, Potassium 2.9 mEq/L, Chloride 100 mEq/L, Bicarbonate 25 mEq/L. He is treated for alcohol withdrawal, and given aggressive intravenous and oral potassium supplementation. Three days later, his electrolyte panel is: Sodium 135 mEq/L, Potassium 3.1 mEq/L, Chloride 102 mEq/L, Bicarbonate 28 mEq/L. Which of the following explains why this patient's potassium level is so difficult to correct?
Poor oral absorption
Hypophosphatemia
. Alcohol withdrawal
Hypomagnesemia
Thiamine deficiency
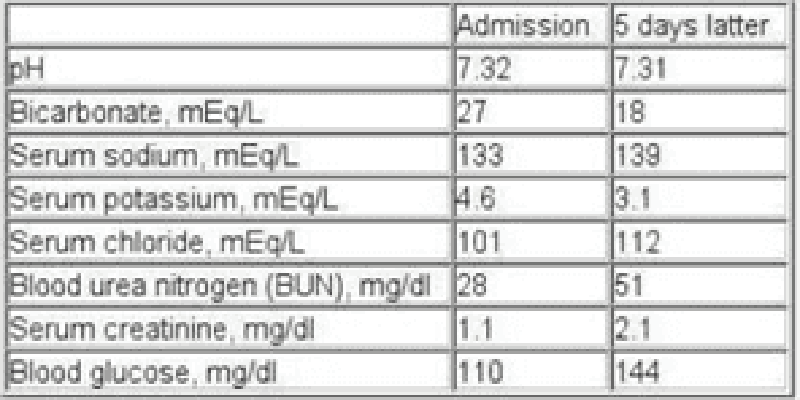
73) A 65-year-old chronic smoker presents to the hospital with increasing shortness of breath for the past few hours. He has been using albuterol occasionally, but it has not been helping him. He has been non-adherent to doctor's appointments and continues to smoke. He is afebrile. His oxygen saturation on room air is 86%. Examination shows elevated jugular venous pressure and lung auscultation reveals diffuse wheezing with no crackles. His heart sounds are muffled. Mild hepatomegaly and bilateral pitting pedal edema is present. Chest x-ray reveals hyperinflated lungs and a flattened diaphragm with no infiltrates. He is started on systemic steroids, bronchodilator nebulization and furosemide. His laboratory studies are shown below at the time of admission and five days later. Which of the following best explains the acid-base status change in this patient?
Acute renal failure
Development of ketoacidosis
Glucocorticoid treatment
Obstructive sleep apnea
Worsening respiratory failure
74) A 32-year-old pregnant female is being evaluated at her 32nd week of gestation. Her lab profile shows the following: Blood pH 7.44, PaO2 100 mmHg, PaCO2 30 mmHg, HCO3- 20 mEq/L, WBC count 9,000/cmm, Hb 11 mg/dl, Na+ 134 mEq/L, K+ 3.6 mEq/1, Cl- 98 mEq/L, BUN 5 mg/dlCreatinine 0.6 mg/dl. Which of the following can best explain her acid-base status?
. Anemia
Pulmonary embolism
. Obesity
Normal phenomenon of pregnancy
Hyperemesis gravidarum
75) A 59-year-old female is hospitalized due to lower gastrointestinal bleeding. Her past medical history includes diabetes mellitus, hypertension, chronic obstructive pulmonary disease, cor pulmonale and recurrent urinary tract infections. Her condition initially stabilized with fluid resuscitation and blood transfusions, but she subsequently developed an acute renal failure. Her urine output has been between 300 and 400 ml per day for the last couple of days. On the 10th day of her hospitalization she is lethargic. Serum analysis reveals: Hemoglobin 10.2 g/dl, Hematocrit 30%, WBC 14,300/mm3, Blood glucose 93 mg/dl, BUN 141 mg/dl, Creatinine 4.1 mg/dl, Sodium 133 mEq/L, Potassium 5.0 mEq/L, pH 7.15, pO2 90 mmHg, pCO2 60 mmHg, HCO3 18 mEq/L. Which of the following is the most likely cause of her lethargy?
Poor tubular bicarbonate reabsorption
Low tubular ammonium production
Renal tubular chloride loss
Decreased anion gap
Hypoventilation
76) A 32-year-old Caucasian male presents to the ER with a 12-hour history of anorexia and vomiting. He says that he feels “a little dizzy”. He denies abdominal pain or diarrhea. His past medical history is insignificant His blood pressure is 110/70 mmHg while supine and 100/60 mmHg while sitting. His heart rate is 90/min. His laboratory values are: Serum sodium 139 mEq/L, Serum potassium 3.1 mEq/L, Serum calcium 8.9 mEq/L, Serum chloride 88 mEq/L, Serum bicarbonate 33 mEq/L, Blood glucose 95 mg/dl, BUN 20 mg/dl, Serum creatinine 1.1 mg/dl. Which of the following is the most likely cause of the decreased chloride level in this patient?
. Gastrointestinal loss
Bicarbonate reabsorption in the kidney
Metabolic alkalosis
Intracellular shift
Volume depletion
77) A 22-year-old female is hospitalized after a car accident. She sustained a hip fracture, fractures of several ribs and a blunt abdominal injury that required a laparotomy. The laparotomy revealed a liver laceration and extensive hemoperitoneum. In the early postoperative period, the patient is noted to have hyperactive deep tendon reflexes. Which of the following electrolyte abnormalities may be responsible for this condition?
Hypokalemia
. Hyperkalemia
Hyponatremia
Hypocalcemia
Hypermagnesemia
78) A 44-year-old obese female undergoes an open cholecystectomy for a complicated acute cholecystitis. On her third post-operative day, her temperature is 36.7°C (98.2°F), blood pressure is 110/80 mm Hg and pulse is 92/min. Her arterial blood gas shows the following: Blood pH 7.28, PaO2 62 mmHg, PaCO2 54 mmHg, HCO3- 30 mEq/L. What is the most likely cause of acidosis in this patient?
Alveolar hypoventilation
Acute pulmonary embolism
Atelectasis
Pulmonary edema
Pleural effusion
79) A 32-year-old male with type 1 diabetes and severe depression is brought to the emergency department because of a 2-day history of nausea and abdominal pain. His temperature is 37.6°C (99.7°F), blood pressure is 122/86 mmHg, respirations are 25/min and pulse is 88/min. His lab values are as follows: Blood pH 7.31, PaO2 90mm Hg, PaCO2 29 mmHg, HCO3- 14 mEq/L, Blood glucose 450 mg/dl, Serum sodium 132 mEq/L, Serum potassium 5.0 mEq/L, Serum chloride 85mEq/L, Blood urea nitrogen 19 mg/dl, Serum creatinine 1.1 mg/dl. Which of the following best describes this patient's acid-base status?
Primary metabolic acidosis with respiratory compensation
Primary metabolic acidosis without compensation
Respiratory acidosis with compensation
Primary metabolic alkalosis with renal compensation
. Normal acid base status
80) A 28-year-old primigravida is admitted to the hospital at 10weeks gestation. Her right leg is swollen. Her BMI is 30 Kg/m2. Her temperature is 36.7°C (98.2°F), respirations are 12/min and pulse is 96/min. Her ABG shows the following: pH 7.49, PaCO2 50 mm Hg, HCO3- 44 mEq/L. Which of the following is the most likely cause of her abnormal arterial blood gas?
Normal phenomenon of pregnancy
Pulmonary embolism
. Obesity
Aspiration pneumonitis
. Hyperemesis gravidarum
81) A 54-year-old woman presents to your office complaining of difficulty walking. She describes severe weakness and occasional pain in her thigh muscles. She has stumbled and fallen several times over the last week. Her past medical history is significant for hypertension treated with hydrochlorothiazide and metoprolol. She consumes two to three cans of beer on weekends. Her younger brother died of a neurological disease when he was 20 years old. Her mother suffers from hypertension and diabetes mellitus. Her heart rate is 90/min and blood pressure is 170/100 mmHg. Chest examination is within normal limits. A bruit is heard over the left carotid artery. Neurologic examination reveals hyporeflexia and decreased strength in all muscle groups. Her ESR is 12 mm/hr. ECG shows flat and broad T waves with occasional premature ventricular contractions. Which of the following is the most likely cause of this patient's current complaints?
. Ischemic stroke
Epidural hematoma
Subdural hematoma
Lumbar spinal stenosis
Electrolyte disturbance
82) A 73-year-old Caucasian man is brought to the office by his daughter, who is concerned that he might be depressed. He is a retired surgeon, and has lived alone ever since his wife died a year ago. His daughter visits him every 6 months; she feels bad about not being able to visit him more frequently because her job and family keep her very busy. He denies having any feelings of sadness, guilt, weight loss, loss of appetite, suicidal ideation, deafness, vertigo, and decreased or blurred vision. His medical problems include hypertension, diabetes mellitus-type 2 and a myocardial infarction 10 years ago. His current medications are glyburide, aspirin and enalapril. He denies the use of tobacco, alcohol, or drugs. His vital signs are within normal limits. He appears withdrawn, less energetic than usual, and walks stiffly. He sits with a stooped posture. He has a fixed facial expression, and his voice sounds monotonous. His deep tendon reflexes are 2+. Sensations and motor strength are normal. There is increased resistance to passive flexion. Which of the following types of gait is most likely to be present in this patient?
. Cerebellar ataxia
Hypokinetic gait
Waddling gait
Spastic gait
Gait disequilibrium
83) A 65-year-old woman complains of periodic headaches in the temporal region, visual disturbances, and neck stiffness. Treatment is initiated early and biopsy of a scalp artery is consistent with arteritis. Two months later, the patient presents to your office with weakness. She says that her headaches are gone but she has difficulty climbing stairs and getting up from a chair. Her serum CK level and ESR are normal. Which of the following is the most likely cause of this patient's current complaints?
Polymyalgia rheumatica
Mononeuritis multiplex
Symmetric polyneuropathy
Inflammatory myositis
Drug-induced myopathy
84) A 54-year-old female complains of muscle weakness. She describes difficulty getting up from a chair and combing her hair. She does not use tobacco, alcohol or drugs. She takes no medication. Her vital signs are within normal limits. Physical examination reveals bilateral ptosis. Which of the following is the most likely cause of this patient's complaints?
Ischemic stroke
Epidural hematoma
Subdural hematoma
Thyroid myopathy
Neuromuscular junction disease
85) A 56-year-old male complains of occasional dizziness. He gets a brief spinning sensation while getting out of bed. He sometimes feels dizzy while turning in bed or looking up. He denies any nausea, diaphoresis, chest pain or tinnitus. His past medical history is significant for long-standing hypertension, which is being treated with hydrochlorothiazide, and hyperlipidemia, which is being treated with simvastatin. His father died of a stroke at the age of 62 years. His blood pressure is 130/80 mmHg while supine, and 135/85 mmHg while standing. His heart rate is 77/min. A grade II/VI ejection murmur is heard over the aortic area. ECG reveals left ventricular hypertrophy and premature ventricular contractions. Which of the following is the most likely cause of this patient's complaints?
Transient ischemic attacks
Labyrinthine dysfunction
Aortic stenosis
Extracellular sodium loss
Cardiac arrhythmia
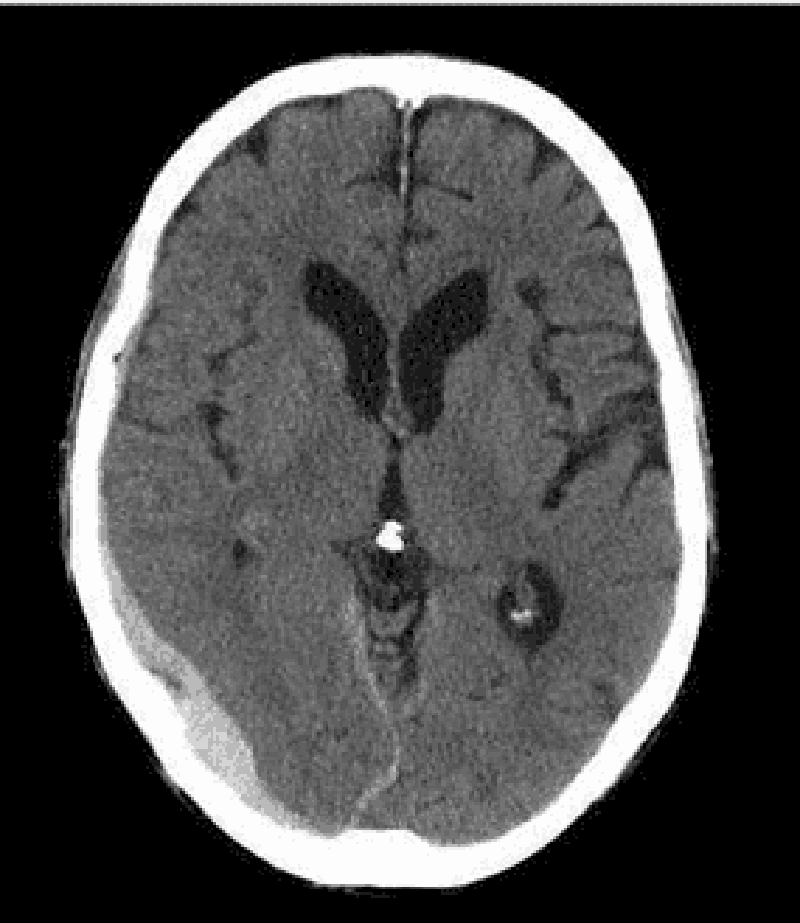
86) A 74-year-old Caucasian woman is brought to the emergency department after a fall. Her husband is concerned since she is on "blood thinners." Her other medical problems include hypertension, hearing loss, congestive heart failure, coronary artery bypass graft, transient ischemic attack, and atrial fibrillation. She does not use tobacco, alcohol, or drugs. Her medications include aspirin, metoprolol, digoxin, furosemide, and warfarin. Her temperature is 37.2°C (99°F), blood pressure is 140/90 mmHg, pulse is 72/min, and respirations are 14/min. CT scan of the head without contrast is shown below. Which of the following is the most likely cause of her condition?
. Tearing of middle meningeal artery
Tearing of bridging veins
Hypertensive hemorrhage
Rupture of an aneurysm
Tumor of the arachnoid granulation
87) A 43-year-old man is being evaluated for one month of blurred vision, frontal headaches and occasional falls. He reports that the blurry vision is worse when he leans forward. He relates his symptoms to a recent break-up with his girlfriend. On physical examination, his blood pressure is 160/100 mmHg and his heart rate is 60/min. Which of the following is most likely responsible?
Bitemporal muscle contraction
High intraocular pressure
Vascular dilatation
Intracranial hypertension
Meningeal irritation
88) A 19-year-old man is brought in to the emergency department after being stabbed in the back. He has no past medical history and takes no medications. Muscle strength is absent and tone is decreased in the right leg. The right patellar and Achilles reflexes are absent. Babinski sign is present on the right. There is a loss of vibratory sense and toe joint position on the right. There is a loss of pain and temperature sensation below T12 on the left. Which of the following will cause a loss of pain and temperature sensation on the left side, beginning at T12?
. Damage to left-sided lateral spinothalamic tracts at T10
Damage to left-sided lateral spinothalamic tracts at T12
Damage to left-sided lateral spinothalamic tracts at L1
Damage to right-sided lateral spinothalamic tracts at T10
Damage to right-sided lateral spinothalamic tracts at T12
89) A 64-year-old woman presents to your office after falling in the grocery store earlier today. She says she was doing her usual shopping when she felt weak in her legs and fell down. She denies hitting her head, headache, or loss of consciousness, but does complain of low back pain. Her past medical history is significant for diabetes mellitus, hypertension, severe osteoporosis, chronic neck pain and congestive heart failure. She has had three transient ischemic attacks, each lasting 15-20 minutes and characterized by slurred speech, in the past. Her medications include insulin, lisinopril, carvedilol, alendronate, aspirin, and acetaminophen. Her blood pressure is 160/90 mmHg and her heart rate is 73/min. Physical exam reveals muscular weakness, increased deep tendon reflexes, and mildly decreased pinprick sensation in both lower extremities. Which of the following is most likely responsible?
Ischemic stroke
Intracranial bleeding
Spinal cord compression
Polyneuropathy
Neuromuscular junction disease
90) A 76-year-old man presents with several months of urinary incontinence. He denies associated dysuria, nocturia, or penile discharge, and has otherwise been feeling well aside from moderate left arm pain following a fall three days ago. He denies headache or head trauma. His medical history is significant for osteoarthritis and glaucoma, which are controlled with medications. On exam, his vital signs are within normal limits. His heart, lungs, and prostate are unremarkable. The cranial nerves are all intact, fundoscopic exam is normal, and there is no tremor. His gait is wide-based and shuffling, and he scores 24/30 on the Folstein mini-mental status exam. His muscle power is 5/5 in all four extremities and the deep tendon reflexes are normal. What is the most likely cause of his current condition?
Increased CSF production
Small vessel cerebral ischemia
Decreased CSF absorption
Amyloid protein deposits in the brain
Spinal cord compression
91) A 33-year-old white female comes to the office for the evaluation of weakness in her upper extremities. She thinks she is unable to feel pain or heat, because she recently noted some burn wounds on her fingertips, and does not know how she got them. She denies weakness in her lower limbs, as well as any history of trauma, headache, bowel or bladder problems, neck pain or facial pain. Examination reveals absent reflexes in her upper limbs. There is absent pain and temperature sensation on the nape of neck, shoulders and upper arms in a 'cape' distribution. Vibration and position sensations are preserved. Which of the following is the most likely pathology of the patient's condition?
Caudal displacement of the cerebellar tonsils and vermis
. Caudal displacement of the fourth ventricle
. Cord cavitation
Focal cord enlargement
Disc herniation and cord compression
92) A 67-year-old woman is being evaluated for periodic confusion, insomnia, and frequent falls as well as episodes of decreased alertness and visual hallucinations. On physical examination, she has increased lower extremity muscle tone but downgoing Babinski reflexes bilaterally. Which of the following pathologic findings most likely underlies her condition?
Neurofibrillary tangle
Lewy bodies
Impaired CSF absorption
Multiple lacunar strokes
Corticospinal tract demyelinization
93) A 65-year-old man was brought to the emergency department after his wife and son were unable to wake him up this morning. His past medical history is significant for hypertension for the past 7 years. For the past year, he has had several episodes of chest pain, which was triggered by physical activity and relieved by rest. His current medications are nitrates and "baby aspirin." His blood pressure is 140/80 mm Hg, heart rate is 85/min, and respirations are 15/min. The physical examination reveals an obese man with impaired consciousness. He has a Glasgow score of 6, asymmetric pupils, and brisk deep tendon reflexes in the left extremities. Plantar stimulation provokes extension of the left great toe. The EKG shows no abnormalities. His CK-MB serum levels are within the normal range, and his LDL cholesterol level is 150 mg/dl. What is the most likely etiopathology of this patient's symptoms?
Atherosclerotic emboli obstructing a major cerebral artery
Acute left ventricular failure with decreased cerebral perfusion
Thrombus migration from the left side of the heart
Hemorrhagic stroke resulting from hypertensive crisis
Chronic subdural hematoma
94) An 84-year-old female is hospitalized with right-sided hemiplegia secondary to an ischemic stroke. She has a complex past medical history including hypertension, diabetes mellitus, hypercholesterolemia and mild Alzheimer disease. Her current medications include lisinopril, metoprolol, insulin glargine, simvastatin and aspirin. On physical examination, her blood pressure is 140/60 mm Hg and her heart rate is 62/min. Her neck is supple and without jugular venous distension. Her lungs are clear to auscultation and her abdomen is soft and non-distended. She cannot move her right arm or right leg. There is a partial thickness ulcer on her right heel. Her wound is most likely the result of which of the following?
Poor glucose control
Ischemia
Venous thrombosis
Bacterial infection
Denervation
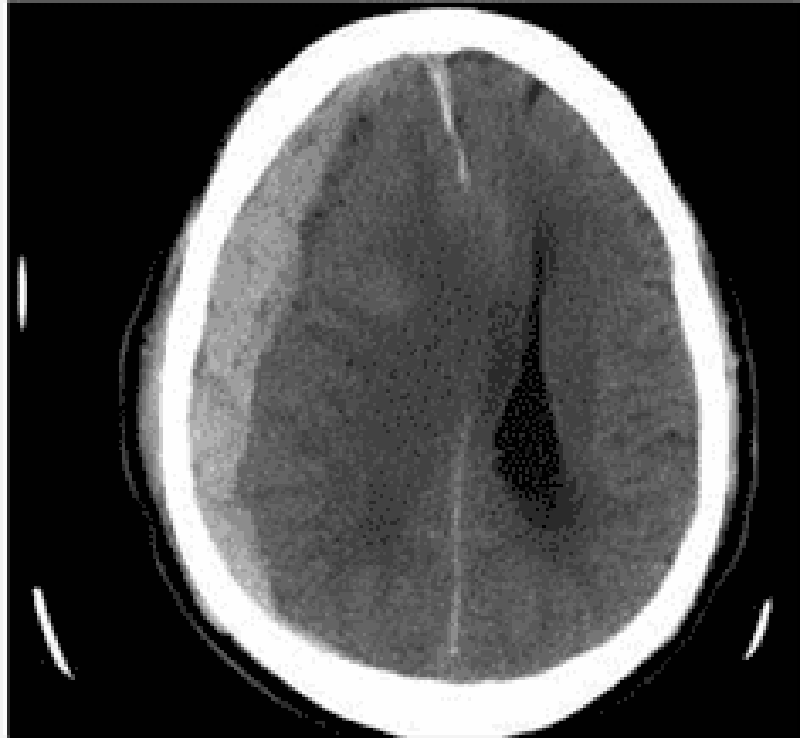
95) A 76-year-old man is brought to the emergency department by his son who found him confused in his apartment. The son also reports that his father has been limping for the past two days. The patient's past medical history is significant for hypertension, diabetes mellitus, and cataract surgery six months ago. His medications are metoprolol, enalapril, and glyburide. He has also been taking ibuprofen for recent headaches. A head CT scan is obtained and is shown below. Which of the following is the most likely cause of this patient's condition?
Carotid artery atherosclerosis
Small vessel hyalinosis
Blunt head trauma
Ruptured aneurysm
Recent eye surgery
96) A 59-year-old male presents to the ER with diplopia that started several hours ago. He has no other complaints. His past medical history is significant for long-standing diabetes with poor glycemic control, right knee osteoarthritis, and peptic ulcer disease. Physical examination reveals right-sided ptosis with the right eye looking down and out. Pupils are equal and reactive to light. This patient's condition is most likely due to which of the following?
Nerve compression
. Nerve ischemia
Nerve inflammation
Lacunar stroke
Muscle infiltration
97) A 52-year-old male is referred to the neurology clinic for the evaluation of EEG abnormalities. He presented with rapidly increasing memory impairment, and denied any history of seizures or head trauma. The physical examination revealed no abnormalities, except a myoclonus. An extensive work-up ruled out the presence of any medical illness; however, the EEG report revealed sharp, triphasic and synchronous discharges. Which of the following abnormalities is most likely in this patient?
Defect in an autosomal dominant gene on chromosome 4
Spongiform encephalopathy caused by a prion
Loss of nigrostriatal dopaminergic neurons
Histopathological findings of neurofibrillary tangles and amyloid plaques
Neurodegeneration of frontal and temporal lobes
98) A 67 -year-old male presents to the emergency department with severe dizziness and the inability to walk. He complains of repetitive vomiting and occipital headache. The symptoms started two hours ago when he was playing golf in sunny weather with his friends. His past medical history is significant for hypertension and diabetes. He underwent coronary stenting two years ago for recurrent chest pain. His current medications are aspirin, glipizide, enalapril and metoprolol. His blood pressure is 210/110 mmHg, heart rate is 78/min, temperature is 37.8°C (100°F), and respirations are 18/min. Muscle strength is preserved in all four extremities, and there are no sensory abnormalities. Which of the following is the most likely cause of this patient's symptoms?
. Heat stroke
Vestibular neuronitis
Posterior cerebral artery occlusion
Cerebellar haemorrhage
Meniere disease
99) A 24-year-old athlete was running a marathon on a bright sunny and humid day, when he suddenly collapsed. He was disoriented at the scene. He has no medical history and takes no medication. He does not use tobacco, alcohol or drugs. Family history is insignificant. On arrival to the emergency room, his temperature is 41°C (105.8°F), blood pressure is 90/60mm Hg, pulse is 140/min, and respirations are 22/min. Mucous membranes and skin are dry. Neck is supple. Auscultation of the chest is unremarkable. Abdomen is soft and non-tender. Muscle tone and reflexes are within normal limits. Labs show a hematocrit of 52%. Chest x-ray is within normal limits. Urinalysis shows large blood but no red blood cells. Which of the following is the most likely underlying pathophysiology of his current condition?
Systemic cytokine activation
Failure of thermoregulatory center
Uncontrolled efflux of calcium from sarcoplasmic reticulum
Inadequate fluid and salt replacement
Cardiac outlet obstruction
100) A 21 -year-old male has been experiencing severe headaches for the past week. He also describes difficulty grasping objects in his right hand and difficulty getting dressed, which both started today. CT scan of the head shows a ring-enhancing lesion in the left frontal lobe and a fluid collection in the left maxillary sinus. Tissue biopsy of the brain lesion is most likely to demonstrate which of the following?
Neoplastic cells
Anaerobic bacteria
Toxoplasma trophozoites
Staphylococcus aureus
Acid-fast bacilli
101) A 30-year-old Caucasian male comes to the office due to symmetric weakness of his lower extremities. He also has paresthesias in his toes and fingers, and lower back pain. The neurological examination shows symmetric weakness, diminished reflexes, and intact sensation in his lower extremities. Orthostatic hypotension is also noted. Electrophysiological studies show slowed nerve conduction velocities. Lumbar puncture reveals normal opening pressure. CSF examination shows few cells, and a protein concentration of 90 mg/dL. Which of the following organisms is involved in the pathogenesis of this disorder?
Campylobacter jejuni
Chlamydia
Shigella
. Salmonella
E coli (O157: H7)
102) A 65-year-old Caucasian male presents to your office complaining of an episode of slurred speech and clumsiness of his right hand. The episode lasted 15 minutes and resolved spontaneously. He had a similar episode one week ago. His past medical history is significant for moderate hypertension, diabetes mellitus (OM) type 2 and osteoarthritis of the right knee. He has smoked one pack of cigarettes daily for 35 years, and drinks 1-2 glasses of wine daily. His current medications include metoprolol, glyburide and naproxen. His blood pressure is 160/95 mmHg, pulse is 65/min, respirations are 16/min, and temperature is 36.7°C (98°F). The physical findings are within normal limits. The lab studies show: Fasting blood glucose 200 mg/dl, Total cholesterol 240 mg/dl, LDL cholesterol 140 mg/dl, HDL cholesterol 76 mg/dl. What is the most important risk factor for a stroke in this patient?
Hypertension
Smoking
Elevated cholesterol level
Alcohol consumption
. Diabetes mellitus
103) A 65-year-old bedridden woman is brought in with complaints of weight loss, weakness and malaise. Her past medical history includes chronic obstructive pulmonary disease (diagnosed fifteen years ago) and hypertension of ten years' duration. She quit smoking two years ago, but previously smoked three packs of cigarettes daily since she was 20 years of age. Her vital signs are stable. Her physical examination reveals severe weakness in her proximal muscles, and loss of deep tendon reflexes. Chest x-ray shows a right upper lung mass with mediastinal lymphadenopathy. Which of the following is the most likely cause of her weakness?
Autoantibodies against post synaptic receptors
. Immune mediated muscle inflammation
Upper and lower motor neuron degeneration
Multicentric CNS inflammation and demyelination
Antibodies to voltage gated calcium channels
104) A 16-year-old female complains of headaches and visual impairment for the past month. She says that the headaches are worst in the morning and are associated with nausea. Her medical history is also significant for severe acne for which she takes oral isotretinoin. On physical examination, her temperature is 36.7°C (98°F), blood pressure is 130/80 mm Hg, pulse is 70/min, and respirations are 15/min. She has papilledema and decreased visual acuity. There is no neck stiffness. Motor examination shows 5/5 power, 2+ deep tendon reflexes, and a normal plantar response. Sensory examination is unremarkable. CT scan of the head is within normal limits. Lumbar puncture reveals the following: Opening pressure 250 cm H20, CSF glucose 40 mg/dL, CSF protein 40 mg/dL, WBC 3/mm3. Which of the following is the most likely cause of her symptoms?
Normal pressure hydrocephalus
Classic migraine
Cluster headaches
Multiple sclerosis
Medication side effect
105) A 26-year-old man comes to the emergency department because he is "suffering from the worst headache of his life." He feels nauseated and is photosensitive. His blood pressure is 160/90 mm Hg, heart rate is 88/min, and temperature is 36.5°C (97.7°F). The physical examination reveals no focal neurological symptoms, except for some meningismus and vertigo, which is not localized to either side. CSF examination reveals the presence of xanthochromia. What is the major cause of morbidity and mortality in a patient with the above condition?
Post-angiographic complications
Vasospasm with symptomatic ischemia and infarction
Secondary infection
Post-surgical complications
Nimodipine use
106) A 53-year-old man comes to the office because of difficulty reading fine print over the last year. He now has to hold books, menus, and magazines at an arm’s length in order to read them. He has never had visual problems before. Which of the following is most likely abnormal in this patient?
. Corneal shape
. Lens elasticity
Lens opacity
Macula
Peripheral retina
107) A 35-year-old HIV-positive male is complaining of deterioration of his vision over the past week. He initially experienced eye pain and mild conjunctivitis, followed by rapid progressive visual loss. Examination of his eyes reveals marked keratitis. Funduscopy shows widespread, pale, peripheral retinal lesions and central necrosis of the retina. Which of the following is the most likely causative organism of this patient's condition?
Pseudomonas
Cytomegalovirus
. Herpes simplex
Candida albicans
Epstein Barr virus
108) A 57-year-old female with a history of type 2 diabetes mellitus complains of fatigue, urinary frequency, increasingly blurred vision and worsening leg cramps over the past week. She reports that the symptoms all began following an upper respiratory infection 7 or 8 days ago. She does not take any medications, but adheres to a diet low in saturated fat and simple carbohydrates to manage her diabetes. On physical examination, her blood pressure is 160/90 mmHg and her heart rate is 90/min. Her mucous membranes are dry. Her urine is positive for glucose but negative for ketones. Which of the following is the most likely cause of this patient's vision impairment?
Cataracts
. Diabetic retinopathy
Arterial hypertension
Hyperosmolarity
Eye infection
109) A 34-year-old obese Caucasian female complains of periodic visual obscurations. She has episodes during which she "goes blind" for several seconds when standing up or stooping forward abruptly. She also describes frequent morning headaches over the last two months for which she has had to take ibuprofen or aspirin almost every morning. She takes no other medications. Past medical history is insignificant aside from one uncomplicated vaginal delivery. She denies use of alcohol, tobacco, or illicit drugs. She is afebrile with a blood pressure of 138/88 mmHg and pulse of 93/min. Visual field testing shows enlarged blind spots. There are no other significant findings on neurologic examination. Which of the following is the most likely cause of this patient's symptoms?
Optic neuritis
Glaucoma
Cataract
Papilledema
Amaurosis fugax
110) A 30-year-old man is concerned about "floating spots" and blurred vision in his right eye. He had a serious injury of his left eye several weeks ago, which eventually led to vision loss in that eye. Inspection reveals a moderate perilimbal flush. What is the most probable cause of this patient's condition?
Reagin-mediated disease
Circulating immune complexes
Non-caseating granulomas
Uncovering of 'hidden' antigens
Non-immune injury
111) A 67-year-old Caucasian male complains of progressive visual loss in his right eye over the past several months. He has a history of hypertension and type 2 diabetes mellitus. Current medications include a daily baby aspirin, hydrochlorothiazide, lisinopril, and metformin. There is no family history of visual problems. He has a 35 pack year smoking history and admits to occasional alcohol use. He is afebrile with a blood pressure of 137/82 mmHg and pulse of 73/min. Cardiac and pulmonary examinations are unremarkable. A neurologic examination demonstrates no focal motor or sensory abnormalities. The patient is asked to cover his left eye and to look at a small spot on a grid made of parallel vertical and horizontal lines. He describes the vertical lines as being bent and wavy. Which of the following is the most likely cause of this patient's complaints?
Lens opacity
Enlarged blind spot
Increased intraocular pressure
Macular degeneration
Peripheral retinal degeneration
112) A 35-year-old white female is complaining of blurry vision and pain with eye movements. She is on no medications and denies any trauma. Last year, she developed bladder incontinence and an episode of leg weakness, which both improved without therapy. Physical examination reveals reduced vision and swollen optic discs. The one diagnosis that may explain her symptoms is:
Parkinson disease
Myasthenia gravis
Multiple sclerosis
Subdural hematoma
Transient ischemic attacks
113) A 67-year-old male presents with a one-month history of dyspnea on exertion and chest pain. He denies hemoptysis, cough, fever, night sweats or weight loss. His past medical history is significant for hypertension and chronic obstructive pulmonary disease. He has a 48 pack-year smoking history but quit six years ago. He works as a salesman. On physical examination, the patient has a temperature of 38.2°C (100.8°F), blood pressure of 128/72 mm Hg, pulse of 92/minute, and respirations of 20 breaths/minute. His complete blood count, chemistry panel, and hepatic function tests are all within normal limits. A chest x-ray and computed tomography scan of the chest reveal a right-sided pleural effusion and calcified nodules in both upper lobes. The patient undergoes thoracentesis. Characteristics of the pleural fluid are given below: Total protein 5.2 g/dl, Glucose 83 mg/dl, Adenosine deaminase 98.5 U/L. Cytologic examination reveals 600 white blood cells/mm3, 1% macrophages and 99% leukocytes. Of the leukocytes, 45% are neutrophils, 50% are lymphocytes, and 5% are monocytes, with no basophils or eosinophils. No neoplastic cells are found. Which of the following is the most likely mechanism underlying development of this pleural effusion?
Elevation of hydrostatic pressure
Decreased plasma osmotic pressure
Increased capillary permeability
Passage of fluid through openings in the diaphragm
Reduction of pleural space pressures

114) A 61-year-old man is being evaluated for progressive exertional dyspnea and decreased exercise tolerance. He has also noticed some ankle swelling. The patient has a 40 pack-year smoking history but denies illicit drug use or occupational exposures. His chest x-ray is shown below. The abnormal diaphragmatic contour seen here most likely results in which of the following?
Higher inspiratory flow
Reduced expiratory effort
Increased work of breathing
Increased thoracic wall recoil
Decreased lung compliance
115) A 65-year-old man complains of two years of persistent cough. He says that he coughs up whitish sputum almost every morning on waking, and then continues coughing throughout the day. He also complains of exertional shortness of breath that becomes disabling if he gets an upper respiratory infection. He has smoked one pack of cigarettes daily for the past 40 years. Pulmonary function testing reveals a vital capacity that is 65% of his predicted. Which of the following best explains this finding?
Alveolar-capillary membrane thickening
Decreased functional residual capacity
Air trapping during expiration
Decreased lung distensibility
Respiratory muscle fatigue
116) A 71-year-old man is brought to the ER after a witnessed tonic-clonic seizure. He is somnolent and intermittently combative on exam. No past medical history is available. His arterial blood gas (ABG) at room air is given below: pH 7.23, pCO2 69 mmHg, pO2 57 mmHg, HCO3 28 mmHg. Which of the following best explains the acid-base disturbances in this patient?
Lactic acid accumulation
Hypoventilation
Pulmonary embolism
Renal failure
Protracted vomiting
117) A 60-year-old white male presents to the Emergency Room with sudden onset of dyspnea. He is a truck driver and just returned from a long trip. His past medical history is insignificant. He is not taking any medications. His blood pressure is 110/70 mmHg and heart rate is 110/min. Physical examination reveals a moderately overweight man with tachypnea. Lungs are clear on auscultation. ECG shows right axis deviation. You order ventilation/perfusion scanning. Which of the following findings will help you the most to confirm the diagnosis?
An area of ventilation defect without perfusion defect
. An area of perfusion defect without ventilation defect
An area of ventilation and perfusion defect
Several small perfusion and ventilation defects
Absence of ventilation and perfusion abnormalities
118) A 74-year-old nursing home resident is brought to the ER with a low-grade fever, cough and shortness of breath for the last two days. The cough is productive of small amounts of greenish sputum. His past medical history is significant for hypertension, diabetes mellitus type 2, COPD, hypercholesterolemia and mild dementia. His blood pressure is 152/78 mmHg and his heart rate is 89/min, regular. Physical examination reveals decreased breath sounds, coarse rhonchi, and increased fremitus over the lower left lung field. His oxygen saturation is 92% on room air when lying on his right side but drops to 84% when he lies on his left. Which of the following best explains this finding?
Increased dead space ventilation
Decreased cardiac output
Decreased oxygen diffusion capacity
Increased arterio-venous shunting
Effort-dependent hypoventilation
119) A 60-year-old man comes to the office with worsening shortness of breath over the last 5 months. He has had two episodes of bronchitis over the last 12 months. He now has a mild nonproductive cough. He denies any fever, chills, hemoptysis, chest pain, or difficulty breathing while lying on his back. His medications include an ipratropium inhaler, aspirin, and amlodipine. He was hospitalized twice in the last 3 years due to an exacerbation of his chronic obstructive pulmonary disease. He has been smoking 1 pack of cigarettes per day for the last 40 years. His temperature is 99°F (37.2°C), blood pressure is 130/86 mm Hg, pulse is 98/min, and respirations are 18/min. Examination shows a thin man in mild respiratory distress with increased anteroposterior chest diameter, diffuse expiratory wheeze and loud S2. Chest X-ray shows hyperinflation of bilateral lung fields with diaphragm flattening and small heart size. Which of the following is the most effective measure to decrease mortality in this patient?
Adding a short acting beta-agonist inhaler
Adding an inhaled corticosteroid
Adding a long-acting beta agonist
Adding systemic corticosteroids
Smoking cessation
120) A 64-year-old man presents to the emergency department with progressive exertional dyspnea that worsened after he contracted an upper respiratory infection. He also complains of bilateral ankle swelling. He has a 40 pack-year history of smoking. Physical examination reveals a mildly overweight patient in mild respiratory distress. Lung auscultation reveals bilateral wheezes and a prolonged expiratory phase. His white blood cell count is 14,500/mm3 and his hemoglobin level is 16 mg/dl. Arterial blood gas analysis reveals the following: pH 7.37, pO2 65mmHg, pCO2 60mmHg. Absence of marked acidosis in this patient is best explained by which of the following?
Increased minute ventilation
Increased dead space ventilation
Pulmonary vasoconstriction
Renal tubular compensation
Erythrocyte chloride shift
121) A 43-year-old woman with congestive heart failure, rheumatoid arthritis and chronic hepatitis C complains of abdominal discomfort and difficulty breathing. Physical examination shows dullness to percussion at the right lung base. Chest x-ray reveals a large right-sided pleural effusion. Thoracentesis yields pleural fluid with a glucose content of 30 mg/dl and an LDH of 192units/L. Which of the following explains the pleural fluid glucose concentration?
Increased pleural membrane permeability
Increased capillary hydrostatic pressure
Increased permeability of the right hemidiaphragm
High white blood cell content of the pleural fluid
High amylase content of the pleural fluid
{"name":"DES 2016. Final (Part 16)", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"23) A 21-year-old woman visits her physician because of 3 weeks of a flu-like‖ illness. She reports symptoms of malaise, fever, fatigue, and a sore throat. There is no weight loss or night sweats, and she has not traveled out of country. Her past medical history is not significant and she is not taking any medications. Physical examination is normal except for enlarged cervical lymph nodes. Laboratory data show hemoglobin 13.2 g\/dL; hematocrit 42%; platelets 380,000\/mL; WBC 8500\/mL, with 35% segmented neutrophils, 1% eosinophils, and 64% lymphocytes, of which 36% were atypical. A heterophil antibody (sheep cell agglutination) test is negative. Which of the following is the most likely causative organism?, 24) A 4-year-old boy is sent to the emergency room because of clinical suspicion of meningitis. He has been ill for 2 days with fever and lethargy. On examination, he is febrile, the neck is stiff, and papilledema is present. There is no rash, the lungs are clear, and heart sounds normal. Which of the following is the most likely causative organism?, 25) A 24-year-old woman presents with chills and rigors. She looks unwell, and her temperature is 39.4°C, blood pressure 100\/60 mm Hg, pulse 110\/min, and oxygen saturation 95%. There is a 3\/6 pansystolic murmur at the right sternal border, which increases with inspiration. Her arms have multiple tattoos and needle marks from injection drug use. Blood cultures (2\/2 sets) are positive for S. aureus, and she is started on appropriate antibiotics. Her renal function is mildly impaired and her urinalysis is positive for protein, and microscopy reveals red cell casts. Which of the following mechanisms is the most likely explanation for her renal abnormalities?","img":"https://cdn.poll-maker.com/10-482472/22222.png?sz=1200"}
More Quizzes
Värmelära
25120
Political Parties
26130
Edebiyat Seminerleri Tablet Ödüllü Anket
520
Swamps
630
Brain Anatomy - Label Lobes and Functions (Free)
201019805
Which Incredibles Character Are You? Study Habits
201020563
Madoka Magica - Free Anime Trivia Challenge
201028709
Tooth Numbering - Dental Charting Practice (Free)
201020794
Biotechnology: Advances and Innovations (Free)
15818158
Shyness Test - How Shy Are You? Free Self-Assessment
201018492
Haber vs Tener - Test Your Spanish Verb Usage
201027458
Painter of the Night Character - Which Are You?
201019405