
Ichigo USLME Med Test P2
1) A 55-year-old woman comes to her primary care physician with complaints of pain, itching and red streaks in her left arm. She feels that her arm is "simply not the same". She had a similar episode in her chest almost 2 weeks ago, but it went away on its own. She has no other complaints, except for heartburn and some upper abdominal pain that has been there for a few months. She takes antacids for it, but has never got over it completely. She thinks that she has lost some weight but she feels happy about it, as she always wanted to lose weight. Her vitals are stable and there is mild epigastric tenderness. She has tender, erythematous, cord like veins palpable over left arm and some over the chest. She smokes 1-2pack/day for 15years and drinks alcohol, only on parties. What is the next best step in this patient?
. Upper GI endoscopy with barium swallows
. Colonoscopy
. Antibiotics and reassurance
. CT scan abdomen
. Spiral CT chest
2) A 51-year-old man comes to the office for his annual examination. He is apparently healthy, and does not have any complaints. His diet is normal, and he exercises regularly. He experiences some stress at work, but says that he is "strong and can fight it out." His father died of a heart attack 4 years ago, and his mother has Alzheimer's disease. His brother has recently been diagnosed with colonic polyps. His vital signs are stable. Hematology and chemistries are within normal limits, but the fecal occult blood test (FOBT) is positive. What is the best next step in the management of this patient?
. Perform screening sigmoidoscopy
. Perform double contrast barium enema
. Do colonoscopy
. Advise him to change his diet and examine him next week
. Order abdomen radiograph for air under the diaphragm
3) A 35-year-old man presents with gastrointestinal complaints for the last 4 months. He currently has fever, bloody diarrhea, nausea, and severe abdominal cramps. He has lost 20 lb (9kg), and has also been feeling fatigued and anorexic. His temperature is 37.3°C (99.1° F), blood pressure is 110/74 mm Hg, pulse is 98/min, and respirations are 22/min. Physical examination reveals tenderness in the right lower quadrant. Digital rectal examination is positive for occult blood. His blood work shows: WBC 11,600 /mm3, Hemoglobin 9.6 g/dl, Hematocrit 30%, Platelets 214,000 /mm3. Flexible sigmoidoscopy reveals larger areas of ulceration within the colon. What is the best next step in the management of this patient?
. Refer him for procto-colectomy
. Dietary modification and reassurance
. Give sulfasalazine
. Perform a biopsy of the colon lesion
. Give a bolus of corticosteroids
4) A 34-year-old man presents to your office for a routine check-up. He has no current complaints except for being "a little stressed out." He works as an executive officer and travels a lot within the country. He does not smoke and consumes alcohol occasionally. He currently takes no medications. His family history is insignificant. His blood pressure is 130/80 mmHg and heart rate is 80/min. Chest examination is unremarkable. The liver span is 8 cm and the spleen is not palpable. There is no cervical lymphadenopathy. Laboratory studies show: Erythrocyte count 5 million/mm3, Hemoglobin 14.0 g/dL, Leukocyte count 8,000/mm3, Platelet count 80,000/mm3. Which of the following is the best initial test for this patient?
. Epstein-Barr virus titers
. HIV antibody test
. Rapid plasma reagin test
. Schilling test
. Blood folate level
5) A 25-year-old female presents to your office complaining of exertional dyspnea and fatigue. Her past medical history is insignificant. She does not smoke or consume alcohol. Her blood pressure is 110/70 mmHg and heart rate is 90/min. Physical examination reveals pale conjunctiva. The laboratory values are: ESR 15 mm/hr, Hemoglobin 7.5 g/dL, MCV 70 fl, MCHC 29%, Leukocyte count 7,000/cmm, Segmented Neutrophils 55%, Bands 3%, Eosinophils 3%, Basophils 0%, Lymphocytes 32%, Monocytes 7%. What is the best next step in the management of this patient?
. Bone marrow sampling
. Iron studies
. Serum folate level
. Schilling test
. HbA2 measurement
6) A 40-year-old male comes to the office because of progressive knee and shoulder pain, which he describes as 5/10 in intensity and started 6 months ago. He has no other medical problems, except for newly diagnosed diabetes. He admits to "chain smoking" for "all his life" and drinks 1-2 bottles of beer a night. He is faithful to his wife. His mother died of "blood cancer" when he was 3-years-old. His father also has diabetes mellitus. His temperature is 37°C (98.6° F), pulse is 86/min, blood pressure is 134/86 mmHg, and respirations are 16/min. Physical examination reveals slightly swollen and tender knee joints. Mild hepatomegaly is present on abdominal examination. What is the best next step in the management of this patient?
. HbA1C level
. Serum iron studies
. Liver biopsy
. X-ray of the shoulder and knee
. Steroid injection of the joint
7) A 42-year-old male presents to your office complaining of fatigue. His past medical history is insignificant. He does not smoke or consume alcohol. His blood pressure is 120/70 mmHg and heart rate is 85/min. Physical examination is insignificant. Laboratory values are: Hemoglobin 7.7 g/dL, MCV 72 fL, MCHC 28%, Leukocyte count 8,000/cmm, ESR 15 mm/hr. Serum iron and ferritin levels are decreased. What is the next best step in the management of this patient?
. Iron supplementation
. Dietary modifications
. Test for occult blood in the stool
. Work-up for malabsorption
. Bone marrow sampling
8) A 35-year-old male is brought to the emergency room with headaches and confusion for the past 2 days. He denies any focal weakness or sensory symptoms. His past medical history is significant for HIV and hepatitis C infections for which he is not receiving therapy. The remainder of his medical history is unobtainable due to his mental status. On physical exam, he has a temperature of 37.9°C (100.2°F), a blood pressure of 140/86 mm Hg, a pulse of 96/min, and respirations of 16/min. Mild icterus is present. The patient's oropharynx is clear and his neck is supple and without rigidity. Examination of his chest and abdomen are unremarkable. Neurologic examination reveals no focal deficits. Laboratory studies show: Complete blood count:Hemoglobin 7.6 g/L, MCV 85 fl, Reticulocytes 8.1%, Platelet count 80,000/mm3, Leukocyte count 3,500/mm3. Chemistry panel: Blood urea nitrogen (BUN) 30 mg/dL, Serum creatinine 2.2 mg/dL, Serum calcium 10.0 mg/dL, Blood glucose 98 mg/dL. Liver studies:Total bilirubin 3.6 mg/dL, Direct bilirubin 1.0 mg/dL, Alkaline phosphatase 120 U/L, Aspartate aminotransferase (SGOT) 178 U/L, Alanine aminotransferase (SGPT) 255 U/L. Which of the following is the most appropriate next step in the management of this patient?
. Liver biopsy
. Peripheral blood smear
. Right upper quadrant ultrasound
. Lumbar puncture
. CT scan of the head
9) A 46-year-old woman comes to the office and says, "I can't believe I've lost so much weight in the last 2 months because I seem to be eating much more than ever. I also find it odd that I drink lemonade all the time, and I have to rush to the bathroom regularly. It seems like everything in me is vanishing."Her temperature is 37°C (98.6°F), blood pressure is 110/70mm Hg, pulse is 98/min, and respirations are 14/min .Physical examination reveals a lean woman with an erythematous, scaly plaques on her face, and on her buttocks. The laboratory studies reveal: WBC 6,400 /mm3, Hemoglobin 8.7 g/dL, Hematocrit 29%, Platelets 193,000/mm3, Sodium 144 mEq/L, Potassium 3.6 mEq/L, Bicarbonate 21 mEq/L, Blood urea nitrogen 16 mg/dl, Creatinine 0.6 mg/dL, Glucose 245 mg/dL. Which of the following is expected in this patient?
. Increased thyroxine level
. Decreased insulin level
. Increased glucagon level
. Increased gastrin level
. Increased serotonin level
10) A 56-year-old woman comes to the office for the evaluation of an ulcer on her left elbow. The ulcer is a persistent, scaly red patch with irregular borders, and it sometimes crusts or bleeds. She recalls the time when she badly burned her left elbow while learning how to cook pasta at thirteen years of age. She works as a public relations officer in a large marketing company. She is a social smoker, and does not like drinking alcohol. Physical examination of the left elbow reveals a big scar with a firm, nontender, reddened, non-healing indolent, 3cm ulcer in the center. What is the best next step in the management of this patient?
. Surgical excision
. Punch biopsy
. Observation for 3 weeks with antibiotics
. Chemotherapy
. Local radiation
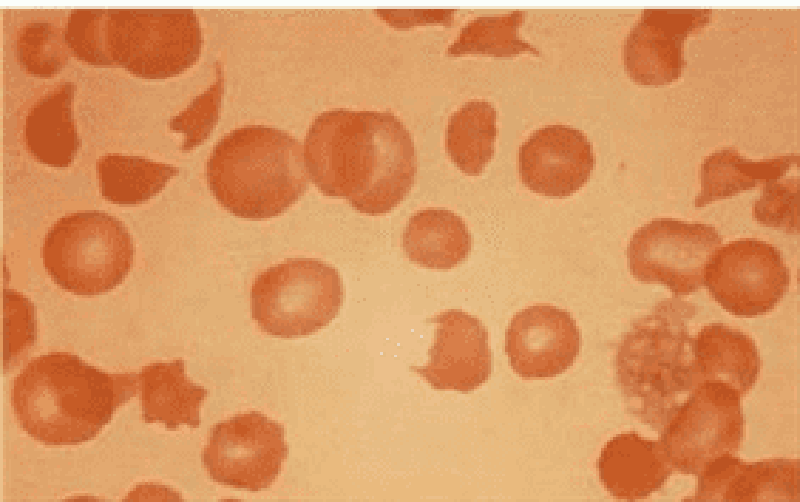
11) A 56-year-old male is being evaluated for increased fatigability. His past medical history is significant for severe aortic stenosis that required aortic valve replacement, diabetes mellitus, and osteoarthritis. Peripheral blood smear findings are shown on the slide below. Which of the following laboratory findings would you most expect to find in this patient?
. Increased total serum iron level
. Decreased serum haptoglobin level
. Increased mean corpuscular volume
. Decreased reticulocyte count
. Decreased serum albumin level
12) A 64-year-old woman comes to the hospital due to an "irritating sore throat for 3 months." She admits to smoking 1 pack of cigarettes daily for the past 29 years, and continues to smoke. She was jailed twice for driving under the influence of alcohol, and went to Alcohol Rehabilitation last year. She currently denies any alcohol intake. She has no fever or any other complaints. She had a complete hysterectomy several years ago for symptomatic fibroids. Her vital signs are stable. Physical examination reveals a 1.5-cm right cervical lymph node. The rest of the examination is normal. Biopsy of the lymph node reveals metastatic squamous cell carcinoma. The CT scan of the chest is negative. What is the best next step in the management of this patient?
. Empirical chemotherapy
. Pan-endoscopy
. Repeat CT in 3 months
. Screening mammogram
. Radical neck dissection
13) A 45-year-old white male comes to the emergency room with "all sorts of things going wrong with him", for the last few months. He has a severe headache, chest and abdominal pain. He is sweating profusely. He has lost weight recently, has diarrhea and palpitations. He is feeling hot all the time. Vital signs reveal BP: 190/100mm of Hg; PR 124/min; RR 18/min; Temperature 37.7° C (99.8°F). On physical examination he has enlarged cervical lymph nodes. Examination of the thyroid reveals multiple thyroid nodules. FNA biopsy reveals thyroid C-cell hyperplasia. Which of the following can also be found on laboratory results?
. Decreased serum calcitonin
. Increased serum phosphorus
. Decreased serum alkaline phosphatase
. Decreased urine metanephrine
. Increased serum calcium
14) A 24-month-old pale child is brought to the office by his mother, who says, "Doc, I think he is under some weird spell. He acts bizarre and always seems tired. He likes to eat wooden, painted toys." The child and her mother live in a relatively poor neighborhood. CBC reveals:WBC 8,600 /mm3, Hemoglobin 7.1 g/dl, Hematocrit 25%, Platelets 166,000 /mm3. His blood lead levels are elevated. Which of the following is most likely seen in this child's peripheral blood smear?
. Megaloblastic anemia and basophilic stippling
. Tear-drop RBCs and hypochromic, microcytic anemia
. Loss of concavity of the RBC and basophilic stippling
. Basophilic stippling and microcytic, hypochromic anemia
. Normochromic, normocytic anemia and basophilic stippling
15) A 42-year-old white female, who has a long history of dysfunctional uterine bleeding, presented with exertional shortness of breath. On examination, she appears very pale and there is a pulmonic flow murmur heard over the second intercostal space. Her vitals are: BP: 130/80mm of Hg; HR: 80/min and regular; RR: 16/min; Temperature 36.7°C (98°F).Initial evaluation reveals hemoglobin of 8.2 gm/dL. WBC count is within normal limits. You are suspecting an iron deficiency anemia secondary to excessive bleeding. Which one of the following studies is most definite for the diagnosis of iron deficiency anemia?
. A low serum ferritin level
. Increased total iron binding capacity
. A low serum iron concentration
. Bone marrow iron staining
. Total iron content of the gastric epithelial cells
16) A 60-year-old Hispanic laboratory technician presents with increasing fatigue and generalized weakness for the last 2 months. He also has chronic pain in the lower back and legs when he walks. He has been smoking 2-3 packs of cigarettes daily for 30 years, and drinks alcohol almost daily. His mother has diabetes, while his father died of a stroke. Physical examination reveals pallor. There is mild hepatomegaly. The neurological examination is completely normal. Complete work-up reveals: CBC: Hemoglobin 9.8 g/L, MCV 85 fl, Platelets 226,000/mm3, Leukocyte count 6,500/mm3, Neutrophils 60%, Eosinophils 1%, Lymphocytes 29%, Lvlonocytes 10%. Chemistry panel: Serum sodium 138 mEq/L, Serum potassium 4.0 mEq/L, Bicarbonate 24 mEq/L, Blood urea nitrogen (BUN) 28 mg/dL, Serum creatinine 2.1 mg/dL, Calcium 11.2 mg/dL, Blood glucose 98 mg/dL. Liver studies: Albumin 4.0 mg/dL, Total protein, serum 9.5 g/dL, Total bilirubin 1.0 mg/dL, Direct bilirubin 0.8 mg/dL, Alkaline phosphatase 110 U/L, Aspartate aminotransferase (SGOT) 58 U/L, Alanine aminotransferase (SGPT) 25 U/L. ESR is 100 mm/h. What is the best next step in the management of this patient?
. ANA and anti-Smith antibodies
. Serum immunoelectrophoresis
. Bone marrow biopsy
. Kidney biopsy
. Bone scan
17) A 57-year-old man comes to the office and complains of long-standing heartburn and chest pain. He describes the pain as burning in nature, and unrelated to eating. For the past week, his interest in things has decreased, and he has been more tired than usual. He has lost almost 40 lbs (18kg) in the last 6 months. He used to smoke 6-10 cigarettes daily, but he quit 4 years ago. He drinks alcohol occasionally. He takes ranitidine for his heartburn. His father died at the age of 67 from lung cancer. His vital signs are stable. Physical examination is unremarkable. The chest x-ray result is within normal limits. What is the best next step in the management of this patient?
. Bronchoscopy
. CT scan of the chest with and without contrast
. Barium swallow followed by endoscopy
. Give omepra zole and follow-up in 2 months
. Test and eradicate Helicobacter pylori infection
18) A 50-year-old woman comes to the office and complains of right shoulder pain which radiates to her hand. She has had cough for many weeks, and feels "more tired than the usual." In addition, her fingers are always swollen, and she now finds it difficult to walk because her knees give way. She has had rheumatoid arthritis for the past 10 years and is used to having pain in her joints; however, she believes that this pain is not due to her arthritis. She takes celecoxib for rheumatoid arthritis. She admits to smoking one pack of cigarettes daily for the past 25 years and to drinking one odd beer every night. All her family members have crippling rheumatoid arthritis. Her vital signs are stable. She is afebrile. Physical examination reveals drooping of the right eyelid and miosis. What is the best next step in the management of this patient?
. CT scan of head and neck
. X-ray of the shoulder
. Steroid therapy
. Chest x-ray
. Nerve conduction study
19) A 54-year-old patient walks into a blood donation camp at a community hospital. His blood report shows an ELISA positive for HIV and HBsAg. He is notified of this finding, and a subsequent western blot test is also positive for HIV. Considering this new diagnosis of HIV, which of the following is indicated in this patient?
. Hepatitis B vaccine
. PPO skin test and anti-Toxoplasma antibody titer
. Serum transaminases and lipid profile
. Trimethoprim-sulfamethoxazole prophylaxis
. Hepatitis C antigen
20) A 25-year-old female presents to her physician with a painful ulcerative lesion on her labia for the past 2 days. She also complains of dysuria. She admits to having sexual intercourse with multiple partners for the last 6 years. Tzanck preparations of one of her lesions reveal multi-nucleated giant cells. She is encouraged to undergo testing for HIV and other STDs. Which of the following is the most appropriate screening test for HIV infection?
. HIV serology by ELISA
. HIV serology by western blot
. HIV viral load
. Absolute CD4 count
. P 24 antigen assay
21) A 27-year-old, HIV-positive man comes to his physician with a two-day history of fever, profuse watery diarrhea, and abdominal cramps. He has been taking zidovudine, didanosine, and indinavir for the past eight months. His temperature is 37.9°C (100.2°F), pulse is 102/min, respirations are 14/min, and blood pressure is 105/70 mm Hg. He is started on fluid and electrolyte support. What is the most appropriate next step in the management of this patient?
. Stop antiretroviral therapy and send stool for Clostridium difficile toxin assay
. Colonoscopy with biopsy of the colonic mucosa
. Stool examination for ova and parasites
. Start empiric treatment for cytomegalovirus
. Loperamide and lactose-free diet until diarrhea subsides
22) A 49-year-old man presents with a three-week history of fever, weight loss, and anorexia. He also reports muscle aches. He has no cough or shortness of breath. He has a thirty pack-year history of cigarette smoking. His temperature is 38.9°C (102°F), blood pressure is 120/76mm Hg, pulse is 90/min, and respirations are 16/min. Lungs are clear to auscultation. The rest of the physical examination is unremarkable. Blood cultures reveal Streptococcus bovis. Echocardiogram reveals vegetations on the mitral valve. Other than antibiotic treatment, what further step is recommended in this patient?
. Cystoscopy
. Colonoscopy
. Bronchoscopy
. Fecal occult blood testing
. CT scan of the head
23) A 43-year-old male presents to a physician with an ulcer on the shaft of his penis. The ulcer is non-tender, with a raised border and a smooth base. There is bilateral inguinal adenopathy. The rest of the examination is unremarkable. Dark field microscopy of a specimen from the ulcer base reveals spirochetes. Which of the following additional screening studies should be performed on this patient?
. VDRL
. FTA-ABS
. HIV antibodies by ELISA
. Proctosigmoidoscopy
. Serum prostate specific antigen
24) A 19-year-old man presents to your office with a one-week history of fever, fatigue, and sore throat. He denies diarrhea or rash. He has no significant past medical history. His brother died of cystic fibrosis at 14 years of age. He admits to occasional cigarette use and alcohol consumption. He has smoked marijuana several times but has never used injectable drugs. He is sexually active with one partner and uses condoms occasionally. Physical examination reveals enlarged tonsils with a whitish exudate and enlarged, slightly tender lymph nodes deep to the sternocleidomastoid muscle bilaterally. The exam is otherwise unremarkable. Which of the following is the best initial test in this patient?
. Rapid plasma reagin (RPR)
. Heterophile antibody test
. HIV antibody determination
. Lymph node biopsy
. Purified protein derivative
25) A 17-year-old man presents with new symptoms of fatigue, malaise, fever, and a sore throat. He has no significant past medical history and is not on any medications. Physical examination is entirely normal except for enlarged, palpable cervical, lymph nodes. He reports no weight loss or night sweats. Laboratory investigations include a normal chest x-ray, negative throat swab, but abnormal blood film with atypical lymphocytes. The hemoglobin is 15.5 g/dL; hematocrit 42%; platelets 290,000/mL; WBC 10500/mL, with 45% segmented neutrophils, 1% eosinophils, and 54% lymphocytes, of which 36% were atypical. Which of the following is the most appropriate initial diagnostic test?
Lymph node biopsy
Bone marrow
Erythrocyte sedimentation rate (ESR)
Heterophil antibody (sheep cell agglutination) test
Hepatic biopsy
26) A 30-year-old male presents with right upper quadrant pain. He has been well except for an episode of diarrhea that occurred 4 months ago, just after he returned from a missionary trip to Mexico. He has lost 7 pounds. He is not having diarrhea. His blood pressure is 140/70, pulse 80, and temperature 37.5°C (99.5°F). On physical examination there is right upper-quadrant tenderness without rebound. There is some radiation of the pain to the shoulder. The liver is percussed at 14 cm. There is no lower-quadrant tenderness. Bowel sounds are normal and active. Which of the following is the most appropriate next step in evaluation of the patient?
. Serology and ultrasound
. Stool for ova and parasite
. Blood cultures
. Diagnostic aspirate
. Empiric broad-spectrum antibiotic therapy
27) A 30-year-old male with sickle cell anemia is admitted with cough, rusty sputum, and a single shaking chill. Physical examination reveals increased tactile fremitus and bronchial breath sounds in the left posterior chest. The patient is able to expectorate a purulent sample. Which of the following best describes the role of sputum Gram stain and culture?
. Sputum Gram stain and culture lack the sensitivity and specificity to be of value in this setting
. If the sample is a good one, sputum culture is useful in determining the antibiotic sensitivity pattern of the organism, particularly Streptococcus pneumoniae
. Empirical use of antibiotics for pneumonia has made specific diagnosis unnecessary
. There is no characteristic Gram stain in a patient with pneumococcal pneumonia
. Gram-positive cocci in clusters suggest pneumococcal infection
28) A 25-year-old male student presents with the chief complaint of rash. He denies headache, fever, or myalgia. A slightly pruritic maculopapular rash is noted over the abdomen, trunk, palms of the hands, and soles of the feet. Inguinal, occipital, and cervical lymphadenopathy is also noted. Hypertrophic, flat, wartlike lesions are noted around the anal area. Laboratory studies show the following: Hct: 40%, Hgb: 14 g/dL, WBC: 13,000/μL, Diff: 50% segmented neutrophils, 50% lymphocytes. Which of the following is the most useful laboratory test in this patient?
. Weil-Felix titer
. Venereal Disease Research Laboratory (VDRL) test
. Chlamydia titer
. Blood cultures
. Biopsy of perianal lesions
29) A previously healthy 19-year-old female university student develops myalgia, headache, fever, and malaise. Blood tests reveal lymphocytosis, with 20% of the lymphocytes being atypical. She remains tired and unwell for 6 weeks, but repeated tests for heterophil antibody are negative. Which of the following is the most likely diagnosis?
Epstein-Barr virus (EBV) infection
Primary HIV infection
Human herpes virus type 7 (HHV-7)
CMV infection
Toxoplasmosis
30) A 20-year-old female college student presents with a 5-day history of cough, low-grade fever (temperature 37.8°C [100°F]), sore throat, and coryza. On examination, there is mild conjunctivitis and pharyngitis. Tympanic membranes are inflamed, and one bullous lesion is seen. Chest examination shows a few basilar rales. Sputum Gram stain shows white blood cells without organisms. Laboratory findings are as follows: Hct: 31, WBC: 12,000/μL, Lymphocytes: 50%, Mean corpuscular volume (MCV): 94 nL, Reticulocytes: 9% of red cells, CXR: bilateral patchy lower lobe infiltrates. Which of the following is the best method for confirmation of the diagnosis?
. High titers of antibody to adenovirus
. High titers of IgM cold agglutinins or complement fixation test
. Methenamine silver stain
. Blood culture
. Culture of sputum on chocolate media
31) A 20-year-old woman complains of headache and discomfort in both sides of her jaw. Physical examination reveals enlarged parotid glands that are slightly tender on palpation. There is reddening of the orifice of Stensen’s duct on intra oral examination; her temperature is 38.3°C, and the pulse rate is 80/min. Laboratory data show hemoglobin 14 g/dL; hematocrit 40%; WBC 11000/mL, with 33% segmented neutrophils, 7% monocytes, and 60% lymphocytes. Which of the following diagnostic tests will help to confirm the diagnosis of epidemic parotitis?
Single blood sample for a specific immunoglobulin G (IgG)
Blood cell count
Blood culture
Single blood test for a specific immunoglobulin M (IgM)
Serum amylase
32) A 19-year-old male presents with a 1-week history of malaise and anorexia followed by fever and sore throat. On physical examination, the throat is inflamed without exudate. There are a few palatal petechiae. Cervical adenopathy is present. The liver span is 12 cm and the spleen is palpable. Throat culture: negative for group A streptococci, Hgb: 12.5, Hct: 38%, Reticulocytes: 4%, WBC: 14, 000/μL, Segmented: 30%, Lymphocytes: 60%, Monocytes: 10%, Bilirubin total: 2.0 mg/dL (normal 0.2 to 1.2), Lactic dehydrogenase (LDH) serum: 260 IU/L (normal 20 to 220), Aspartate aminotransferase (AST): 40 U/L (normal 8 to 20 U/L), Alanine aminotransferase (ALT): 35 U/L (normal 8 to 20 U/L), Alkaline phosphatase: 40 IU/L (normal 35 to 125). Which of the following is the most important initial test combination to order?
. Liver biopsy and hepatitis antibody
. Streptococcal screen and antistreptolysin O (ASO) titer
. Peripheral blood smear and heterophile antibody
. Toxoplasma IgG and stool sample
. Lymph node biopsy and cytomegalovirus serology
33) A 27-year-old man presents with diarrhea. He returned 3 weeks ago from a trip to rural South America. Over the past few days, he has gradually developed lower abdominal pain and diarrhea. Now the symptoms are much worse with eight stools a day consisting mostly of mucus and blood. He is afebrile, the abdomen is tender in left lower quadrant, and the remaining examination is normal. His stool is mostly comprised of blood and mucus. Which of the following is the most appropriate initial diagnostic test?
Stool culture
Stool toxin assay
Examination of a dried stool specimen
Immunofluorescence of stool specimen
Examination of a wet stool specimen
34) A 60-year-old male complains of low back pain, which has intensified over the past 3 months. He had experienced some fever at the onset of the pain. He was treated for acute pyelonephritis about 4 months ago. Physical examination shows tenderness over the L2-3 vertebra and paraspinal muscle spasm. Laboratory data show an erythrocyte sedimentation rate of 80 mm/h and elevated C-reactive protein. Which of the following statements is correct?
. Hematogenous osteomyelitis rarely involves the vertebra in adults
. The most likely initial focus of infection was soft tissue
. Blood cultures will be positive in most patients with this process
. An MRI scan is both sensitive and specific in defining the process
. Surgery will be necessary if the patient has osteomyelitis
35) A 40-year-old school teacher develops nausea and vomiting at the beginning of the fall semester. Over the summer she had taught preschool children in a small town in Mexico. She is sexually active, but has not used intravenous drugs and has not received blood products. Physical examination reveals scleral icterus, right upper quadrant tenderness, and a palpable liver. Liver function tests show aspartate aminotransferase of 750 U/L (normal < 40) and alanine aminotransferase of 1020 U/L (normal < 45). The bilirubin is 13 mg/dL (normal < 1.4) and the alkaline phosphatase is normal. What further diagnostic test is most likely to be helpful?
. Liver biopsy
. Abdominal ultrasound
. IgM antibody to hepatitis A
. Antibody to hepatitis B surface antigen
. Determination of hepatitis C RNA
36) A 24-year-old woman comes to the physician because of a 24-hour history of right flank pain, burning micturition and high-grade fever with chills. Her temperature is 102°F (38.9°C), blood pressure is 90/60 mm Hg, pulse is 130/min, and respirations are 20/min. Physical examination shows costovertebral angle tenderness. Which of the following is the most likely urine dipstick finding in this patient?
. Positive for nitrites and esterase
. Positive for nitrites only
. Positive for esterase only
. Negative for both esterase and nitrites
. Negative for esterase and positive nitrites
37) A 27-year-old woman complains of fatigue, low-grade fevers, anorexia, headaches and skin rash over the past several weeks. She also notes new exertional dyspnea and an unintentional 5-pound weight gain over the past two weeks. On physical examination, her blood pressure is 190/110 mmHg and her heart rate is 90/min. Which of the following is the most likely finding on this patient's urinary tests?
. High VMA excretion
. High daily cortisol excretion
. Red blood cells
. Glucosuria
. Uric acid crystals
38) A 70-year-old man comes to the physician because of nocturia. He states that over the past two years his urinary frequency has increased and he has to strain while passing urine. He also notes dribbling of a few drops of urine at the end of voiding. Sometimes he has to void again within two hours. He has no other symptoms. He has no history of diabetes mellitus, stroke or trauma. He does not take any medication. His father had surgery of the prostate for benign prostatic hyperplasia. He has a 15-pack-years history of cigarette smoking. Rectal examination shows smooth, firm enlargement of the prostate with no induration. Neurological examination shows no abnormalities. Laboratory study shows a serum creatinine of 0.7 mg/dl. Which of the following studies is indicated at this time?
. Blood urea nitrogen
. Ultrasound of kidney, bladder and ureter
. Urinalysis
. Serum prostate specific antigen
. Cystoscopy
39) A 65-year-old man comes to the physician because of increased urinary frequency and urgency, as well as suprapubic discomfort His temperature is 37C(98.6F), blood pressure is 130/75 mm Hg, pulse is 76/min, and respirations are 14/min. Rectal examination shows prostatic induration; physical examination otherwise shows no abnormalities. Urinalysis shows no abnormalities. Expressed prostatic secretions show a leukocyte count of 20 WBCs/HPF (normal is less than 10 WBCs/HPF). They are sent for culture and sensitivity, and fail to grow any bacteria. Serum prostatic specific antigen is 2 ng/ml (normal value is less than 4ng/ml). A diagnosis of nonbacterial prostatitis is suggested. Which of the following is the most appropriate next step in management?
. Perform urinary cytology and cystoscopy
. Repeat urinalysis
. Repeat culture of prostatic secretions
. Treatment with oral erythromycin
. Treatment with oral trimethoprim-sulphamethoxazole
40) A 33-year-old woman comes to the emergency department due to a 4-day history of left-sided flank pain, nausea, vomiting, fevers and chills. Her temperature is 39°C (102°F) and blood pressure is 100/60 mm Hg. Examination shows significant left costovertebral angle tenderness. Urinalysis shows positive nitrites, many WBC and bacteria. Laboratory studies show a WBC count of 17,000/cmm with 8% bands. Which of the following is the most appropriate next step in management?
. Intravenous pyelogram
. Intravenous antibiotics
. Blood cultures
. CT scan of the abdomen
. Ultrasound of the abdomen
41) A 14-year-old boy comes to the physician because of a 2-day history of fever and nasal discharge. He has also had malaise, fatigue and myalgia. His temperature is 38.8°C (101.9°F), blood pressure is 130/70mm Hg, pulse is 90/min, and respirations are 15/min. Examination shows no abnormalities. Urine dipstick testing shows proteinuria but there is no hematuria or pyuria; urinalysis otherwise shows no abnormalities. Which of the following is the most appropriate next step in management?
. Repeat dipstick testing
. BUN and serum creatinine
. 24-hour urinary collection for protein
. Renal ultrasound
. Reassurance
42) A 57-year-old man comes to the physician because of 2 episodes of hematuria. He also complains of cough fatigue and fever for several days. He has smoked two packs of cigarettes daily for 25 years. He does not use alcohol or drugs. Vital signs are stable. Examination shows a left-sided varicocele which fails to empty when the patient is recumbent; examination otherwise shows no abnormalities. Laboratory studies show Hb of 16.2 g/dl and platelets of 480,000/cmm. Which of the following is the most appropriate diagnostic step in management?
. Chest x-ray
. Abdominal CT scan
. Urinalysis
. Serum alfa-fetoprotien levels
. Ultrasonogram of the testicles
43) A patient with benign prostatic hyperplasia has moderately severe symptoms and is started on finasteride. After six months of treatment with finasteride, his symptoms improve remarkably and his prostate has regressed in size. Which of the following histological patterns was most likely present at the time of initiation of treatment?
. Hyperplasia of prostate with predominance of epithelial components
. Hyperplasia of prostate with predominance of muscular element
. Hyperplasia of prostate with predominance of collagen
. Hyperplasia of prostate with predominance of both collagen and smooth muscles
. Hyperplasia of prostate with predominance of glandular tissue
44) A 65-year-old woman comes to the physician because of a two-month history of fatigue and weight gain. She has rheumatoid arthritis and hypertension. She takes hydrochlorothiazide and naproxen. She does not use tobacco, alcohol, or drugs. Her blood pressure is 120/70 mm Hg, pulse is 80/min, and respirations are 14/min. Physical examination shows generalized edema; liver is palpated 2 cm below the costal margin. Urinalysis shows 4+ proteinuria. Ultrasound of the kidneys shows slight enlargement. Renal biopsy was performed. Which of the following is the most likely finding on renal specimen analysis?
. Crescent formation on light microscopy
. Deposits revealed under polarized light
. Linear immunoglobulin deposits revealed on immunofluorescence microscopy
. Granular immunoglobulin deposits revealed on immunofluorescence microscopy
. Normal light microscopy findings
45) A 73-year-old man comes to the physician because of a one-year history of progressively worsening urinary urgency, hesitancy, nocturia, and weak urinary stream. He has no fever, abdominal pain, hematuria, malaise or weight loss. He takes atenolol for essential hypertension. He has no history of diabetes mellitus or ischemic heart disease. He does not use tobacco, alcohol, or drugs. Rectal examination shows a smooth, firm enlargement of the prostate with no induration or asymmetry. Neurological examination shows no abnormalities. Urinalysis shows no abnormalities. Laboratory studies show serum creatinine of 2.1 mg/dl. Which of the following is the most appropriate next step in management?
. Ultrasound of kidneys, ureters, and bladder
. Watchful waiting
. Transurethral resection of prostate
. Treatment with finasteride
. Treatment with prazosin

46) A 30-year-old woman comes to the office due to the recent onset of fever, chills, and dysuria. Her temperature is 38.3°C (101.0°F), blood pressure is 110/70mm Hg, pulse is 68/min, and respirations are 15/min. Examination shows tenderness at the right costovertebral angle. Laboratory studies show WBC count of 16,000/microl with left shift. Urinalysis shows bacteriuria and pyuria. Her urine and blood is collected for culture and sensitivity. She is prescribed oral ciprofloxacin and sent home. After three days, she returns for a follow-up visit. She is still febrile, and the physical examination is unchanged. The blood cultures have no growth after 72 hours of incubation. Results of the urine culture show. Which of the following is the most appropriate next step in management?
. Start intravenous ampicillin and gentamicin
. Start intravenous ciprofloxacin
. Continue oral ciprofloxacin for another 10 days
. Perform renal ultrasound
. Renal CT scan
47) A 57 -year-old woman is admitted to the ICU after being involved in a highway motor vehicle accident. She was hypotensive at the scene and received 7 litters of fluids, which included crystalloids, blood, and fresh frozen plasma. She apparently had significant external blood loss from multiple fractures and skin loss. She undergoes surgery, after which she is transferred to the ICU and receives continuous IV fluids and vasopressors. Her laboratory studies 24 hours after the accident show the following: Hb 9.5 g/dl, WBC 15,000/cmm, Platelets 130,000/cmm, BUN 34 mg/dl, Serum Creatinine 2.2 mg/dl. Which of the following is the most likely microscopic finding on urinalysis?
. Broad cast
. Muddy brown cast
. RBC casts
. WBC casts
. Fatty casts
48) A 46-year-old man comes to the physician because of a 2-day history of fever and chills. His fever was gradual in onset. He also complains of perineal and back pain, which is worse towards the sacral area. He has repeated urges to urinate, along with pain on micturition. Rectal examination shows a boggy, exquisitely tender prostate. Laboratory studies show: Hb 13 g/dl, Hct 40%, WBC 12,000/cmm, Platelets 329,000/cmm, Dipstick urinalysis:, Esterase +++, PH 5.0, Nitrite +++, WBC 50+, Protein +, Blood ++. Which of the following is the most appropriate next step in management?
. Send culture of post-prostatic massage sample
. Send culture of mid-stream urine sample
. Administer alpha blocking agents
. Start empirical treatment on an outpatient basis
. Urethral catheterization
49) A 19-year-old man presents with malaise, nausea, and decreased urine output. He was previously well, and his physical examination is normal except for an elevated jugular venous pressure (JVP) and a pericardial rub. His electrolytes reveal acute renal failure (ARF). Which of the following findings on the urinalysis is most likely in keeping with acute glomerulonephritis (GN)?
Proteinuria
White blood cell casts
Granular casts
Erythrocyte casts
Hyaline casts
50) A 24-year-old woman presents with nausea, vomiting, anorexia, and gross hematuria. She had a sore throat 2 weeks ago that resolved on its own. On examination, her blood pressure is 160/90 mm Hg, pulse 90/min, JVP is 7 cm, heart sounds are normal, there is 1+ pedal edema, and the lungs are clear. She has a renal biopsy. Which of the following electron microscopy findings on the renal biopsy is most likely in keeping with poststreptococcal GN?
Diffuse mesangial deposits
No deposits
Electron-dense endothelial deposits
Closed capillary lumen
Subepithelial humps
51) A 74-year-old man is brought to hospital because of urinary retention. He has a Foley catheter inserted to relieve the obstruction, and 1500 cc of urine is emptied from his bladder. Over the next few hours, he has 200cc/h of urine output. Which of the following urine electrolyte values is most likely in keeping with his diagnosis?
High sodium
Low potassium
High specific gravitylow pH
Low pH
Osmolality > 500 mOsm/kg
52) An 85-year-old man who resides in a nursing home presents with a 3-day history of lower abdominal pain and increasing fatigue and lethargy. He is afebrile, his BP is 160/92 mm Hg, and RR 16/min. His lungs are clear and his heart examination normal. There is diffuse abdominal tenderness on palpation and a large area of fullness and dullness to percussion starting just below the umbilicus and extending to the suprapubic area. His serum sodium is 130 mEq/L, potassium 4.9 mEq/L, BUN 75 mg/dL, and creatinine is 3.5 mg/dL. His baseline BUN and creatinine were 25 and 1.3 respectively as recently as 1 month ago. A Foley catheter is placed and 1200 cc of urine is obtained. What will be the likely clinical course for this patient with regard to his renal function?
. His creatinine will continue to rise slowly for 2 to 3 more days
. His creatinine will return to 1.3 over the next week
. He will require dialysis within 24 hours
. He will produce minimal urinary output for at least 3 days
. His renal function is unlikely to show any improvement in the future and 3.5 will be his new baseline
53) A 64-year-old man presents with symptoms of malaise, shortness of breath, edema, and no urine output for 24 hours. His past medical history is not significant, and his only medication is daily aspirin. On examination his JVP is 4 cm, heart sounds are normal, lungs are clear, and the abdomen is soft. A Foley catheter is inserted into his bladder for 200 cc of urine, which is sent for urinalysis. His urine output still remains low. Which of the following is the most appropriate initial diagnostic test?
Renal ultrasound
Blood cultures
Urine cultures
Inferior vena cavagram with selective renal venogram
Blood urea nitrogen (BUN)/creatinine ratio
54) A 46-year-old woman with nausea and vomiting presents to hospital because of light- headedness when standing and decreased urine output. She looks unwell; the blood pressure supine is 90/60 mm Hg and 80/60 mm Hg when standing. Her abdominal, heart, and lung examinations are normal. Which of the following laboratory values suggests prerenal azotemia in this patient?
Markedly elevated urea, unchanged creatinine
Unchanged urea, elevated creatinine
Little change in either creatinine or urea for several days after oliguria develops
Urea/creatinine ratio of 10
Urea/creatinine ratio of 25
55) A 20-year-old man presents with obtundation. Past medical history is unobtainable. Blood pressure is 120/70 mm Hg without orthostatic change, and he is well perfused peripherally. The neurological examination is nonfocal. His laboratory values are as follows: Na: 138 mEq/L, K: 4.2 mEq/L, HCO3: 5 mEq/L, Cl: 104 mEq/L, Creatinine: 1.0 mg/dL, BUN: 14 mg/dL, Ca: 10 mg/dL. Arterial blood gas on room air: PO2 96, PCO2 15, pH 7.02 Blood glucose: 90 mg/dL. Urinalysis: normal, without blood, protein, or crystals. Which of the following is the most likely acid-base disorder?
. Pure normal anion-gap metabolic acidosis
. Respiratory acidosis
. Pure high anion-gap metabolic acidosis
. Combined high anion-gap metabolic acidosis and respiratory alkalosis
. Combined high anion-gap metabolic acidosis and respiratory acidosis
56) A 17-year-old woman presents with peripheral and periorbital edema. She has previously been healthy and takes no medications. Her blood pressure is 146/92 mm Hg; she is afebrile. The patient has mild basilar dullness on lung examination; her cardiac examination is normal. She has periorbital edema and soft, doughy 3+ edema in her legs. Her serum creatinine is 0.6 mg/dL and her serum albumin is 2.1 g/L. Urinalysis shows 3+ protein, no RBC or WBC, and some oval fat bodies. What is the next best step to take in evaluating this patient?
. Order serum and urine protein electrophoresis
. Request a nuclear medicine renal scan
. Measure plasma aldosterone and renin activity
. Order a 24-hour urine collection to quantitate the degree of proteinuria
. Ask a nephrologist or radiologist to perform a renal biopsy
57) A 56-year-old man is involved in a severe motor vehicle accident. He develops ARF after admission to hospital. One of the possibilities for his ARF is posttraumatic renal vein thrombosis. Which of the following findings is most likely to suggest renal vein thrombosis?
White cell casts on urinalysis
Heme-granular casts
Heavy proteinuria
Urine supernatant pink and tests positive for heme
Specific gravity >1.020
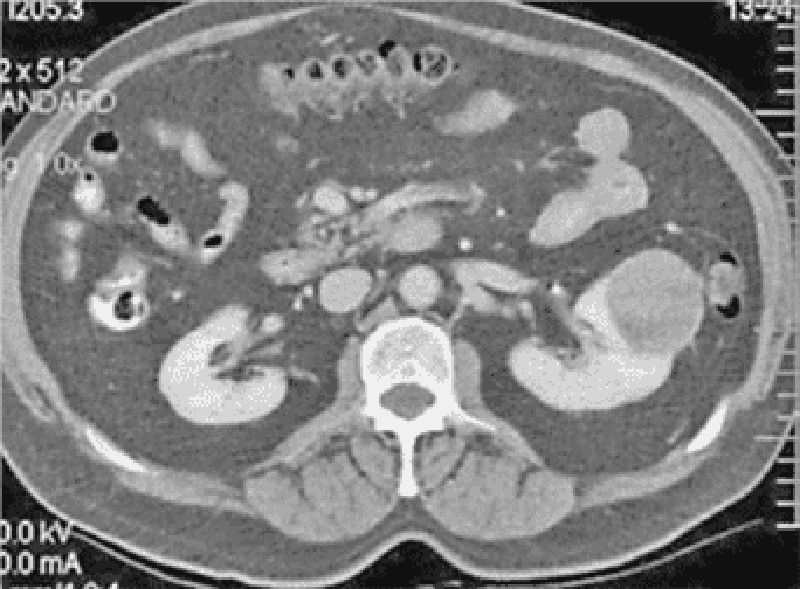
58) A 69-year-old woman presents with left flank pain and hematuria. Physical examination suggests a left-sided abdominal mass. Computerized tomography (CT) scan of the abdomen reveals a 5-cm mass in the left kidney. Which of the following laboratory abnormalities might also be present (See Fig.)?
Polycythemia
Thrombocytopenia
Hypocalcemia
Leukocytosis
High renin hypertension
59) A 60-year-old male who emigrated from Russia comes to you with complaints of dizziness, fatigue and weight loss. A review of systems reveals that the patient experiences daily fevers and cough. He does not use tobacco, alcohol or drugs. He does not take any medication. His blood pressure is 108/64 mmHg while standing. His respiratory rate is 14/min and is unlabored. Laboratory studies reveal the following: Chemistry panel: Serum sodium 130 mEq/L, Serum potassium 5.9 mEq/L, Chloride 102 mEq/L, Serum creatinine 0.8 mg/dL, Blood glucose 58 mg/dL. Complete blood count: Hemoglobin 10.0g/L, Platelets 430,000/mm3, Leukocyte count 4,500/mm3, NeutrophiIs 46%, Lymphocytes 45%, Eosinophils 9%. Chest x-ray shows a right upper lobe cavity. Which of the following acid-base disturbances is expected in this patient?
. Elevated anion gap metabolic acidosis
. Normal anion gap metabolic acidosis
. Metabolic alkalosis
. Respiratory acidosis
. Respiratory alkalosis
60) A 20-year-old white male is found to have an elevated calcium level on routine pre-employment screening blood tests. He denies any polyuria, polydipsia or constipation. He has no significant past medical history and does not take any medication. He does not use tobacco, alcohol or drugs. His pulse rate is 82/min, blood pressure is 110/70 mmHg, temperature is 37.0°C (99°F) and respirations are 14/min. Complete physical examination is unremarkable. Laboratory studies show the following: Serum sodium 140 mEq/L, Serum potassium 4.0 mEq/L, Chloride 103 mEq/L, Bicarbonate 24 mEq/L, Blood urea nitrogen (BUN) 18 mg/dl, Serum creatinine 0.8 mg/dl, Calcium 11.2 mg/dl, Blood glucose 98 mg/dl, Serum PTH level 55 pg/ml (normal 10-65 pg/ml), Urine calcium/creatinine clearance ratio < 0.01. Which of the following conditions is most consistent with this patient's findings?
. Primary hyperparathyroidism
. Vitamin D overproduction
. Multiple myeloma
. Sarcoidosis
. Familial hypocalciuric hypercalcemia
61) A four-week-old male infant is brought to the emergency department because of persistent vomiting immediately after feeding for the past several days. Examination shows an emaciated infant with dry mucus membranes. An olive-shaped mass is palpated in the right upper quadrant of the abdomen. Which of the following acid-base abnormalities is most likely in this patient? pH, PaCO2 (mm Hg), HCO3- (mEq/L)
.7.10, 80, 24
. 740, 40, 24
. 7.55, 46, 42
. 7.62, 21, 21
. 7.62, 30, 30
62) A 35-year-old male with severe persistent bronchial asthma requiring multiple medications presents complaining of weight gain over the past several months despite no changes in appetite, diet, or activity level. He denies alcohol, tobacco, and drug use and has no other significant past medical history. On physical examination, he has a blood pressure of 143/92 mm Hg, a heart rate of 65/min, a temperature of 98.7°F, and a respiratory rate of 16/min. There is moderate supraclavicular fullness, and his skin is thin with areas of bruising and acne. Neurologic exam reveals decreased proximal muscle strength. Which of the following findings is most likely to also be present in this patient?
. Hyperkalemia
. Hypokalemia
. Hypercalcemia
. Hyponatremia
. Hypomagnesemia
63) A 42-year-old woman presents to the emergency department with multiple complaints. She reports that she had been feeling well until approximately one month ago, when she began to feel increasingly fatigued and weak. For the past two weeks, she has had anorexia, nausea, and abdominal pain. In the past three days, she has had two syncopal episodes. Her medical history is unremarkable and she takes no medications. She denies tobacco and drug use and drinks wine only occasionally. Physical exam reveals a temperature of 36.7°C (98°F), blood pressure of 86/52 mmHg, heart rate of 90/min, and respiratory rate of 18/min. Her cardiac exam is normal and her lungs are clear to auscultation bilaterally. You note hyperpigmentation of the skin in the palmar creases. Which of the following additional findings is most likely to be present in this patient?
. Hyperkalemia
. Hypokalemia
. Hypernatremia
. Hypochloremia
. Hypomagnesemia
64) A 42-year-old male is found unconscious in a subway station. He is brought to the emergency department where cardio-pulmonary resuscitation (CPR) is done and IV glucose and thiamine are given. His lab profile shows: Blood pH 7.20, PaO2 90mmHg, PaCO2 30mmHg, HCO3 12 mEq/L. Which of the following is the best next step in the diagnosis of this patient's acid-base status?
. Calculate the plasma anion gap
. Calculate the plasma osmolar gap
. Calculate the urine anion gap
. Calculate the urine osmolar gap
. Obtain venous blood gas
65) A 43-year-old woman presents to the emergency department complaining of confusion. Her other complaints include increased thirst and "using the bathroom more frequently." She denies any fever, chills, headache, chest pain, shortness of breath, or cough. Her past medical history is significant for bipolar disorder that is well-controlled by medication. She does not drink alcohol, smoke cigarettes, or use illicit drugs. Her vital signs are stable, and physical exam is unremarkable. Laboratory studies reveal the following: Sodium 154 mEq/L, Potassium 4.1 mEq/L, Chloride 116 mEq/L, Bicarbonate 28 mEq/L, Glucose 95 mg/dl, Urine osmolality 250 mOsm/L, Plasma osmolality 326 mOsm/L. What is the most likely cause of this patient's symptoms and laboratory findings?
. Dehydration
. Lithium
. Divalproic acid
. Craniopharyngioma
. Head trauma
66) An 87-year-old female is brought to the emergency department for evaluation of altered mental status. Her medical history is significant for multi-infarct dementia, hypertension, stroke, coronary artery disease, severe degenerative joint disease, chronic atrial fibrillation, constipation and urinary incontinence. Her medications include aspirin, acetaminophen, atenolol, nitroglycerin, multivitamins, pravastatin, docusate, senna, digoxin and glucosamine. She lives in a local nursing home, and the people who brought her to the ED deny any history of new symptoms. Her blood pressure is 110/70 mmHg, pulse is 98/min, respirations are 16/min and temperature is 36.1°C (97°F). Physical examination reveals dry mucus membranes and decreased skin turgor. There are no new focal neurologic deficits. Which of the following is most likely to be present in this patient?
. Hyponatremia
. Hypokalemia
. Hypernatremia
. Hyperkalemia
. Hypocalcemia
67) A 56-year-old diabetic male is brought to the emergency department due to nausea and vomiting. While you are examining the patient, a nurse asks if determination of the patient's acid-base status will help ascertain the etiology and subsequent management of the patient's primary problem. Which of the following pairs of laboratory values will help get the best picture of the patient's acid-base status?
. pH and PaCO2
. pH and PaO2
. PaO2 and PaCO2
. Urinary pH and PaCO2
. Urinary pH and HCO3-
68) A 45-year-old female with severe depression, migraine and rheumatoid arthritis is brought in after she was found to have nausea, fever and upper abdominal discomfort. The patient describes severe tinnitus and vertigo. She admits that she overdosed on one of her medications. Her temperature is 38.5°C (101.3°F), blood pressure is 120/76 mm Hg, pulse is 90/min and respirations are 24/min. Physical examination is unremarkable. Which of the following acid-base statuses is most likely in this patient? pH, PaCO2 (mm Hg), HCO3- (mEq/L)
. 7.36, 22, 12
. 7.29, 50, 23
. 7.22, 35, 14
. 7.40, 40, 24
. 7.45, 30, 20
69) As you are walking across the hospital lobby, you stumble upon the arterial blood gas (ABG) results of a patient. The ABG (on room air) results are shown below: Blood pH 7.43, PaO2 100 mm Hg, PaCO2 25 mm Hg, HCO3- 16 mEq/L. Which of the following patients is most likely to have these laboratory values?
. 42-year-old female with aspirin toxicity
. 52-year-old female with persistent vomiting
. 42-year-old patient with severe asthma exacerbation
. 36-year-old patient with pulmonary embolism
. 64-year-old male with excessive diuresis
70) A 27-year-old man complains of difficulty in walking. He noticed leg weakness several days ago, and now he is barely able to walk. He also complains of mild back pain and foot numbness. Two weeks ago, he had an upper respiratory tract infection. Physical examination reveals lower extremity muscle weakness, absent knee and ankle reflexes, and minimal sensory loss. Spinal MRI shows no abnormalities. Which of the following findings would you expect on CSF analysis in this patient? (Protein, WBC, count RBC, count Glucose)
. high, increased, normal, normal
. high, increased, increased, low
. high, increased, normal, low
. high, normal, normal, normal
. normal, increased, increased, normal
71) A 27-year-old man complains of poor appetite, loss of interest in his daily activities, and impaired sleep. He has lost 10 pounds over the last two months. He says that he feels regretful about IV drug abuse in his past, but denies having suicidal or homicidal thoughts. He drinks alcohol occasionally but denies regular alcohol consumption or early morning drinking. He is sexually active with one partner and she uses oral contraceptives. On physical examination, his pulse is 76/min and his blood pressure is 110/70 mm Hg. His heart and lung exams are unremarkable and his abdomen is soft and non-tender. The liver span is 9 cm and the spleen is not palpable. He is fully oriented to person, place and time but performs poorly on memory tests. Which of the following is the best next step in managing this patient?
. Selective serotonin reuptake inhibitors
. Benzodiazepines
. HIV testing
. Thyroid function testing
. Serum iron studies
72) A 23-year-old white man is brought to the emergency department (ED) by an ambulance due to an epileptic seizure. He fell on the sidewalk while going home from a pub, where he had two beers. A witness noted tonic-clonic movements of all four extremities for about one minute. This seizure was his first episode, and lasted 30 minutes. In the ED, he is in a state of partial confusion and disoriented to time, place and person. The physical examination does not reveal any focal neurologic pathology. His eye exam does not show any papilledema. His airway is secured, and his breathing is normal. CBC, serum electrolytes, EKG and chest x-ray are normal. Urine toxicology screen is ordered, and lorazepam is given. What is the most appropriate next step in the management of this patient?
. Psychiatric consultation
. Brain computed tomography without contrast
. Brain computed tomography with contrast
. Lumbar puncture
. Electroencephalogram
73) A 35-year-old bank executive is brought to the emergency department after the sudden onset of a severe (10/10) headache, followed by a brief period of unconsciousness. His headache started while he was at a meeting and shortly thereafter, he vomited and lost consciousness. He regained consciousness soon afterwards, but was quite confused and irritable. His blood pressure is 160/100 mm Hg, pulse is 90/min, temperature is 37.2°C (99°F), and respirations are 16/min. The physical examination reveals a normal pupil size, no congestion or inflammation of the eye, and no focal neurological deficits. The ECG reveals nonspecific ST and T wave changes. The CT scan shows a subarachnoid hemorrhage. What is the most likely expected electrolyte abnormality with the patient's disease?
. Hypokalemia
. Hyperkalemia
. Hyponatremia
. Hypernatremia
. Hypercalcemia
74) A 68-year-old white male comes to the emergency department due to a sudden onset of right-sided hemiplegia, headache and impaired consciousness. There is no prior history of transient ischemic attacks. His medical problems include hypertension, obesity, hypercholesterolemia, tobacco abuse, benign essential tremor, gout, and benign prostatic hyperplasia. His medications include amlodipine, simvastatin, colchicine, propranolol, and doxazosin. The neurological exam shows right-sided weakness and hemi-sensory loss. There is a carotid bruit on his left side. Which of the following is the most appropriate next step in management?
. Anticoagulate with heparin
. Give aspirin
. CT scan of head without contrast
. CT scan of head with contrast
. Perform MRI scan of head
75) A 76-year-old male with a history of mild dementia, hypertension and diabetes mellitus is brought to the emergency department by his daughter because of two days of confusion, disorientation and decreased oral intake. She says that he has been talking to people who are not there and wandering around the house in the middle of the night. His current medications are metoprolol, valsartan and metformin. On physical examination, his blood pressure is 100/60 mmHg and his heart rate is 70/min. Which of the following initial evaluations is most important for this patient?
. Complete blood count and iron studies
. CT scan of the head
. Serum electrolytes and urinalysis
. EKG and serum troponin T level
. Brain MRI
76) A 69-year-old patient is brought to the office by his daughter because his behavior changed progressively for the past several months. He roams in the apartment at night, and forgets his grandchildren's names. Three days ago, he was found by the doorman urinating by the building's gates. His wife died three years ago. He insists that there is nothing wrong with him, and tries to give excuses for what his daughter is reporting. He does not feel particularly fatigued and has a good appetite. He does not smoke, has no history of alcohol abuse, and no history of diabetes. His blood pressure is 155/85 mm Hg, pulse is 90 /min, and respirations are 15/min. Although the neurologic exam was difficult to assess, there were no abnormalities found. The Babinski sign is negative bilaterally. There is no evidence of rectal or bladder incontinence. The mini-mental state examination (MMSE) score is 15/30 (normal > 24). The laboratory studies show: Hb 13.5 g/dl, RBC 4.5 million/mm3, Hct 45%, Leukocyte count 4,500/mm3, Platelet count 230,000/mm3, MCV 83 um3, MCHC 32% Hb/cell, S. calcium 9.0 mg/dl, S. sodium 137 mEq/dL, S. potassium 4.0 mEq/dL, S. creatinine 1.1 mg/dl, S. glucose 100 mg/dl, TSH 3 uU/mL, Total cholesterol 180 mg/dl. CT scan is done. Which of the following abnormalities would you expect to see on the CT scan?
. Normal appearance
. Hypodense images involving different brain regions
. Diffuse cortical and subcortical atrophy
. Enlargement of the ventricle without cortical atrophy
. Marked atrophy of the frontal and temporal cortices
77) A 34-year-old Caucasian man presents to your office with a several day history of difficulty walking. He also describes some "funny" sensations in his feet. He denies any recent skin rash, diarrhea, or joint pain. His past medical history is significant only for a recent mild respiratory infection. He visited his friends in Connecticut one month ago. He smokes one pack of cigarettes a day and admits to occasional IV drug use. He is not sexually active. His temperature is 36°C (98°F), heart rate is 90/min, respirations are 20/min, and blood pressure is 160/100 mmHg. Chest examination is unremarkable. Abdomen is soft and non-tender. The liver span is 8 cm and the spleen is not palpable. Cranial nerves II-XII are intact. Muscle strength is reduced in the lower extremities but well preserved in the upper extremities. Lower extremity sensation is decreased. Stroking the soles of the feet elicits extension of the great toe. Which of the following is most likely to diagnose this patient's condition?
. Electromyography
. CT scan of the brain
. MRI of the spine
. Serologic tests for B. burgdorferi
. Lumbar puncture
78) An 18-year-old girl comes to the office due to a three-week history of headaches that has been disturbing her daily activities, including her sleep. She describes these headaches as pulsatile, diffuse, and occasionally results in vomiting. Her school grades have deteriorated over the past 3 months. She complains of double vision when she looks sideways. Her family history is significant for migraine. She is afebrile. Her neurologic examination is significant for sixth cranial nerve palsy. The pupils are equal, and reactive to light and accommodation. There is no sinus tenderness. Fundoscopy reveals bilateral papilledema. MRI of the brain reveals an empty sella. What is the most appropriate next step in the management of this patient?
. Lumbar puncture
. Sinus imaging
. Refractive testing of the eye
. Trial of prednisone
. Start sumatriptan
79) A 30-year-old white female presents with an attack of common migraine. This is her fourth attack of migraine over the last 4 months. Her attacks previously responded well to aspirin and ibuprofen; however, her current headache is very severe and not relieved by NSAIDs. She has been trying to conceive for the past 2 months. Six years ago, she was treated with isoniazid due to a positive PPD test. Her father died at the age of 45 from an acute myocardial infarction. Before starting therapy with serotonin agonists (e.g., sumatriptan), which of the following tests should be performed in this patient?
. Liver function tests
. Stress echocardiogram
. PPD and chest x-ray
. Pregnancy test
. Visual field testing
80) A 72-year-old male comes to the emergency department (ED) due to a sudden onset of right-sided weakness, aphasia and incontinence. He did not lose consciousness. All his symptoms started suddenly, 1 hour ago. He was previously diagnosed with hyperlipidemia, and is on simvastatin. He is a known smoker and alcoholic. He is taking aspirin as prophylaxis for heart attacks and strokes. His family history is not significant. His blood pressure is 160/88 mm Hg, pulse is 78/min, respirations are 18/min, and temperature is 37.8°C (100°F). He is admitted to the ED, and a patent airway is secured. The cardiac examination and EKG findings are normal. CT of the brain shows no acute hemorrhage. Which of the following interventions will result in the best outcome in this patient?
. IV nitroprusside to reduce blood pressure
. Nimodipine
. Tissue plasminogen activator within 3 hours
. Streptokinase and heparin combination
. IV high dose corticosteroids
81) A 17-year-old girl is brought to the office by her mother due to weakness of her hands and legs. The weakness has been progressively worsening over the past 24 hours, and she now feels that the weakness is affecting her hips. Her mother says she was a bit unwell a couple of weeks ago, but otherwise her past medical history is unremarkable. The physical examination reveals 1/5 power in ankle and knee flexion/extension and 2/5 power in hip flexion. Reflexes are absent in her lower extremities bilaterally. She is admitted to the hospital. Spinal fluid analysis shows albumino-cytologic dissociation. Which of the following tests is the most appropriate for monitoring her respiratory function?
. Arterial blood gas
. Vital capacity
. FEV1/FVC ratio
. Peak expiratory flow rate
. Chest x-ray
82) A 29-year-old female is brought to the emergency department due to paraplegia, urinary incontinence and urgency. She denies any trauma. She has a history of trigeminal neuralgia. The neurological examination shows spasticity and hyperreflexia in the lower extremities, and impaired vibration and proprioception in her left forearm. Which of the following is the most likely finding in this patient's cerebrospinal fluid (CSF) examination?
. Oligoclonal bands
. Albumino-cytologic dissociation
. Increased pressure
. Increased cell count
. Increased total protein concentration
83) A 28-year-old Caucasian female presents to the emergency department (ED) appearing very anxious. She is accompanied by her boyfriend. She woke up this morning with severe weakness over the right side of her body. The weakness came on all of a sudden, but gradually resolved during the day. She denies any sensory symptoms. Her boyfriend reports that her speech was "weird, almost as if she was stuttering or struggling to get her words out." This too has resolved. The patient denies any other symptoms. The only other history of note is that she returned from a holiday in Italy 2 days ago. Vitals signs are unremarkable. The neurological examination is normal. Her chest x-ray is within normal limits. EKG shows normal sinus rhythm with a rate of 82/min. An urgent head CT scan is within normal limits. Which of the following investigations is most likely to reveal the underlying cause of this episode?
. Carotid Doppler ultrasonography
. MRI head
. Psychiatric referral
. Transthoracic echocardiogram
. Cerebral angiography
84) A 76-year-old Caucasian female is brought to the hospital with a one-hour history of confusion. Her husband says that she started to complain of occipital headaches two hours ago and took some acetaminophen; an hour later, he found her confused on the couch and called an ambulance. She has no recent history of fever, chills, ear pain, or upper respiratory infection. Her past medical history is significant for coronary artery disease, diabetes mellitus, hypertension and atrial fibrillation. She had triple vessel coronary artery bypass five years ago. Her current medications include warfarin, metoprolol, diltiazem and lisinopril, plus 25 units of long-acting insulin at bedtime. She lives with her husband and is independent in her activities of daily living. On examination, her blood pressure is 160/90 mmHg and her heart rate is 80/min and irregular. She is unable to follow simple commands or speak. She moves all four extremities. Deep tendon reflexes are symmetric and Babinski reflexes are downgoing bilaterally. Which of the following is the best next step in evaluating this patient?
. Brain MRI
. CT scan of the head without contrast
. Electroencephalogram
. Nerve conduction studies
. Lumbar puncture
85) A 26-year-old white female presents with worsening weakness of her right upper extremity, left lower extremity and ataxia. She also complains of unilateral eye pain and visual loss. The eye pain is worsened by ocular movements. On eye examination, there is a central visual field defect in her right eye. Fundoscopy is normal. Neurological examination shows spastic paraparesis in the right upper extremity and the left lower extremity. What is the most appropriate next step in this patient's management?
. CT scan with contrast
. MRI of the brain
. Lumbar puncture
. Brain biopsy
. PET scan
86) A 52-year-old male comes to the office due to a sudden onset of photophobia, redness around the eye and pain in his right eye. He also has nausea and a terrible headache, which has not responded to ibuprofen. He denies any trauma, and has never had such an episode before. He was watching TV when the event started. The physical examination reveals a non-reactive mid-dilated pupil. The eye appears red with conjunctival flushing. What is the best diagnostic test for this patient's condition?
. Tonometry
. CT scan of the head
. Lumbar puncture
. Fluorescein staining of eye
. Duplex studies of carotid artery
87) A 32-year-old female is brought to the clinic by her husband because he believes she is a malingerer and is "just being difficult." Sometimes, she appears confused and disoriented. Over the past year, she has complained of visual loss, eye pain and inability to do any household chores. Two months ago, she claimed to have lost control of her bladder. Interestingly, she is "her normal self" when it is time to go for summer trips. The wife insists that she does not understand what is happening to her, and adds that she occasionally loses the ability to move her right hand. The physical examination is basically normal. The patient appears, alert, oriented, and is in no distress. Which of the following is the most appropriate next step in management?
. MRI of the brain
. Lumbar puncture
. Tonometry
. Serum immunoglobulins
. Nerve conduction studies
88) A 45-year-old Caucasian male presents in the office with a movement disorder and behavioral disturbance. For the past month, he has been having frequent, sudden, jerky and irregular movements of his upper extremities. He has become irritable, and does not visit his family or friends. He is a business executive, and co-workers have commented on the serious decline in his performance. His father had similar problems and died in a nursing home CT scan is ordered. Which of the following is a typical CT finding in such patients?
. Atrophy of the caudate nucleus
. Diffuse atrophy of the cerebral cortex
. Atrophy of lenticular nucleus
. Atrophy of frontal lobes
. Atrophy of temporal lobes
89) A 69-year-old comatose man is brought to the emergency department by an ambulance. His wife says that he has been hypertensive for the past twenty years, and he is not compliant with his medication. His pulse is 80/min and blood pressure is 240/140 mm Hg. The physical examination reveals reactive pupils, no oculocephalic reflexes, no nystagmus, positive conjugate gaze deviation to the left, and reflexes of 3/4 on the right and 2/4 on the left side. Which of the following is most likely to be seen on computed tomography?
. Bleeding into brain tumor
. Normal brain
. Ruptured aneurysm
. Basal ganglia haemorrhage
. Brain abscess
90) A 75-year-old male comes to the office for the evaluation of a two-month history of intermittent right eye visual loss. Each episode is "painless, lasts a few seconds, and feels like a curtain coming over the eye." He denies any other symptoms. He has never had any trauma to his eye, and does not use any medications. His past medical history is significant for hypertension. He quit smoking 20 years ago, but had smoked for 25 years. On examination, the patient is alert and without neurologic findings. His blood work and chest x-ray are normal. What is the best next step in the management of this patient?
. CT head
. Echocardiography
. Duplex study of neck
. Lumbar puncture
. MRI brain
91) A 60-year-old, obese, diabetic woman comes to the office and complains of "balance problems while walking." She also has tingling and paresthesias in her feet, decreased sensation below the knees, and burning and aching sensations in both legs. She has been very fatigued lately. The neurological examination reveals diminished proprioception peripherally on her feet, "stocking" distribution of hypesthesia from her knees distally, and positive signs of spinal ataxia. What is the best diagnostic test for this patient's condition?
. Evoked potentials
. Repetitive stimulation electromyography
. Electroencephalography
. Regular checking of blood sugar and diabetic diet
. Electromyography and conduction studies
92) A 12-year-old male child comes to the office after being referred for a medical evaluation. His schoolteacher says that he has a problem concentrating during class. He stares in space for a few seconds several times a day, and appears totally absorbed in his thoughts. He is not disruptive in class, but appears forgetful. There is no history of trauma, infection or problems at birth. On examination, the child is alert with stable vital signs. There is no loss of motor or sensory perception. Which of the following can confirm the patient's diagnosis?
. CT scan of the head
. EMG studies
. EEG studies
. Psychiatric evaluation
. Lumbar puncture
93) A 22-year-old white male comes to the office and complains of a noise in his right ear. The noise has been intermittently present for several months, but recently became "very annoying." He also complains of decreased hearing on his right side while using the telephone. His past medical history is insignificant. The physical examination reveals numerous cafe-au-lait spots. What is the best next step in the management of this patient?
. Plain radiographs of the skull
. MRI with gadolinium
. CT with contrast
. Electroencephalogram
. Surgery
94) A 30-year-old male comes to the emergency department screaming, "Something blew into my right eye while I was drilling I' He complains of a foreign body sensation in the right eye, photophobia, and excessive lacrimation. Gross examination of the right eye with a penlight after the application of a topical anesthetic is insignificant. What is the best next step in the management of this patient?
. Tonometry
. Fluorescein examination
. Topical antibiotic
. Ultrasonography
. MRI of the orbits
95) A 60-year-old man with a history of hypertension and migraine headaches presents to the ED with a headache. He describes left-sided headache and eye pain that is associated with nausea and vomiting. The patient has a long history of migraines, but says his migraines do not usually include eye pain. On examination, his temperature is 97.6°F, HR 84 beats per minute, RR 12 breaths per minute, and BP 134/80 mm Hg. His neurologic examination is normal. His left eye is mid-dilated and nonreactive. His cornea is cloudy. His corrected visual acuity is 20/50 in the left eye and 20/20 in the right eye. What is the most appropriate next step in management?
. Administer hydromorphone
. Perform head CT scan
. Check IOP
. Check erythrocyte sedimentation rate (ESR)
. Discharge patient
96) A 65-year-old man presents to your office complaining of progressive breathing difficulty. His past medical history is significant for hypertension, diabetes mellitus, type 2, and myocardial infarction experienced two years ago. His current medications are hydrochlorothiazide, atenolol, glipizide, and aspirin. He does not smoke or consume alcohol. His vital signs are BP 156/96 mmHg, PR 65/min, RR 18/min, T 36.7°C (98°F). Physical examination shows mild symmetric edema of the lower extremities. Hepatojugular reflex is positive. Point of maximal impulse is displaced downward and to the left. Soft blowing systolic murmur is heard on the apex. Breath sounds are diminished on the right side. Serum protein level is 6.5 g/dl and serum LDH is 200 mg/ml. After taking a chest radiograph, you suspect pleural effusion on the right and decide to perform diagnostic thoracocentesis. Which of the following findings, on pleural fluid analysis, is most consistent with this patient's condition?
. LDH level of 180 mg/ml
. Protein level of 5.0 g/dl
. Glucose 60 mg/dl
. pH of 7.35
. High amylase level
97) A 68-year-old female is admitted with a broken hip after a fall. She undergoes a left hip replacement, which was uneventful. After spending two days in bed, she undergoes partial non-weight bearing physiotherapy. Five days later, she has developed shortness of breath and a swollen leg. A deep vein thrombosis is discovered. An arterial blood gas evaluation is done for suspected pulmonary embolism. What is the most consistent finding of pulmonary embolism?
. Elevated PaCO2
. Decreased A-a gradient
. Right axis deviation on ECG
. Decreased PO2
. Pulmonary infarction

98) A 64-year -old African American male presents to you with complaints of a dry cough, weight loss and pain in his right arm. The symptoms started approximately 2 months ago. His past medical history is significant for type 2 diabetes mellitus and hypertension. He smokes 1 pack per day and drinks alcohol occasionally. He denies any drug allergies. Physical examination is unremarkable. ECG reveals normal sinus rhythm. An MRI of his chest is shown below. Which of the following is most likely responsible for this patient's symptoms?
. Aspergilloma
. Bronchial carcinoid
. Superior sulcus tumor
. Cryptogenic organizing pneumonia
. Lung abscess
99) A 45-year-old man presents with two days of bilateral hand pain that is most severe in his wrists. Physical examination reveals bilateral wrist tenderness, thickening of the distal fingers, and convex nail beds. There is nicotine staining of the right index and middle fingers. He states that he has been smoking 2 packs of cigarettes a day for the past 25 years. Chest examination reveals decreased breath sounds and a prolonged expiratory phase. The patient relates the pain's onset to a data entry job he recently started. He notes that his boss believes he is fabricating his pain to get off work. His job records reveal numerous sick leaves. Which of the following is the most appropriate course of action?
. Reassure the patient and prescribe analgesics
. Obtain chest x-ray
. Obtain rheumatoid factor levels
. Recommend psychiatry evaluation
. Order serum calcium and uric acid levels
100) A 45-year-old man presents to the emergency department with a two-day history of fever, chills and productive cough. He reports having had two episodes of pneumonia over the past six months, both of which resolved completely with levofloxacin therapy. He smoked cigarettes for twenty years, but quit recently with the second bout of pneumonia. Today, his temperature is 38.9°C (102°F), pulse is 98/minute, blood pressure is 110/80 mm Hg, and respirations are 18/min. On physical examination, there are crackles and bronchial breath sounds over the right lower lobe of the lung. Chest x-ray shows right lower lobe consolidation; previous x-rays also show consolidation in this area. What is the most appropriate next step in the management of this patient?
. Administer vancomycin
. Administer ciprofloxacin
. Schedule bronchoscopy
. Obtain CT scan of the chest
. Obtain pulmonary function tests
101) A 45-year-old female with a past medical history of rheumatoid arthritis presents to the emergency department with right calf pain and swelling of sudden onset. She denies fever, chills, dyspnea, chest pain, or history of trauma to the leg. She has smoked a half pack of cigarettes daily for 20 years. Her only medicine is methotrexate for her rheumatoid arthritis. On physical examination, her temperature is 37.0°C (98.6°F), pulse is 70/min, blood pressure is 140/80 mmHg, and respirations are 14/min. Her BMI is 30 kg/m2. Examination of the right calf reveals mild redness, warmth and tenderness. Which of the following is the most appropriate next step in the management of this patient?
. Initiate warfarin therapy
. Initiate heparin therapy
. Perform compression ultrasonography
. Perform contrast venography
. Obtain blood cultures and start antibiotics
102) A 53-year-old white male comes to your office with long history of cough, periodic shortness of breath, and wheezing. His family history is significant for asthma in his mother and hypertension and diabetes in his father. He is not taking any medications. He smokes two packs a day ever since he was 16 years of age and consumes alcohol occasionally. Physical examination reveals bilateral scattered expiratory wheezes. Which of the following tests can help you most in differentiating asthma from emphysema in this patient?
. Chest x-ray
. Bronchoscopy with bronchial washings
. FEV1 measurement with and without a bronchodilator
. Serum IgE measurement
. Sputum analysis
103) A 65-year-old female undergoes total right hip replacement after fracturing the neck of her femur. There are no surgical complications, and afterwards she is started on enoxaparin (low molecular weight heparin) for deep venous thrombosis prophylaxis. On the third postoperative day, she suddenly becomes anxious and complains of right sided chest pain and shortness of breath. She has a history of hypertension, diabetes and hyperlipidemia. She has a 20 pack-year smoking history, but quit 10 years ago. On exam, her temperature is 37.2°C (98.9°F), blood pressure is 126/76 mm Hg, pulse is 110/min and respirations are 30/min. Her oxygen saturation is 88% on room air. She is diaphoretic but her chest is clear to auscultation. A portable chest x-ray shows no abnormalities. EKG reveals sinus tachycardia and non-specific ST/T-wave changes. Which of the following studies would most likely reveal the diagnosis?
. Serial cardiac enzymes
. Helical CT pulmonary angiography
. Echocardiogram
. Arterial blood gas analysis
. B-type natriuretic peptide levels
104) A 29-year-old woman presents with chest pain and exertional dyspnea of 10days duration. Her medical history is significant for a normal spontaneous vaginal delivery three months ago, after which she has had frequent episodes of dark bloody vaginal discharge. The most recent bleeding episode was 6 days ago. The patient denies fever, chills, hemoptysis, orthopnea, or leg pain. She does not smoke cigarettes, drink alcohol, or use illicit drugs. Her temperature is 37.7°C (98.9°F), pulse is 80/min, blood pressure is 110/68 mmHg and respirations are 16/min. Examination shows clear lungs. Pelvic examination shows an enlarged uterus. Complete blood count and serum electrolytes are within normal limits. Chest radiographs reveal multiple bilateral infiltrates of various shapes. Which of the following investigations will be most helpful in establishing the diagnosis?
. Ventilation perfusion scan
. Echocardiogram
. Quantitative beta HCG
. Pulmonary function tests
. CT scan of the chest
105) A 55-year-old male presents with face and arm swelling that he says is worst when he wakes in the morning. He also notes a 10-pound unintentional weight loss over the past three months, plus new-onset exertional dyspnea. His past medical history is significant for hypertension, for which he takes hydrochlorothiazide. He has smoked cigarettes for the past 40 years and drinks alcohol occasionally. On physical examination, he is afebrile and his vital signs are within normal limits. His face is plethoric and darkappearing. The veins on the anterior chest wall appear engorged. His abdomen is soft, non-tender, and nondistended, and there is no organomegaly. The lower extremities are non-edematous. What is the most appropriate next step in the management of this patient?
. Echocardiogram
. Doppler ultrasound of the upper extremities
. Chest x-ray
. Urine for 24-hour protein excretion
. Serum albumin level
106) A 34-year-old male is recovering from head trauma sustained in a motor vehicle accident. He is currently in the intensive care unit on mechanical ventilation. His most recent arterial blood gas analysis shows: pH 7.54, PaO2 124 mmHg, PaCO2 20 mmHg, Bicarbonate 17 mEq/L. Which of the following additional findings do you most expect in this patient?
. Low urine bicarbonate excretion
. High urine pH
. High serum aldosterone level
. High serum anion gap
. High serum albumin level
107) A 33-year-old male was involved in a motor vehicle accident with numerous rib fractures. His course in the hospital was complicated by difficulty with deep breathing and later developed pneumonia. The chest x-ray later confirmed that the patient had developed a parapneumonic effusion. Which one of the following laboratory tests on the pleural fluid is currently thought to be most helpful in determining the need for chest tube placement in parapneumonic effusion?
. Lactate dehydrogenase
. WBC count
. Pleural fluid pH
. Total protein
. Color of the pleural fluid
108) A 24-year-old Caucasian man is brought to the emergency room with acute asthma exacerbation. His current medications include inhaled fluticasone and salmeterol. The attack started 10 hours ago and did not respond to numerous albuterol inhalations and systemic steroids. His blood pressure is 120/70 mmHg and heart rate is 110/min. The patient is tachypneic and speaks with difficulty. Lung auscultation reveals decreased breath sounds, prolonged expiration, and bilateral wheezing. Pulse oximetry showed 86% at room air. ABG at room air are: pH 7.43, Po2 68 mmHg, PCO2 40mmHg. The chest x-ray demonstrates hyperinflated lungs. Which of the following findings indicates that the patient is getting worse?
. Lung hyperinflation
. Tachypnea
. Tachycardia
. Hypoxia
. Normal PCO2
109) A 26-year-old Caucasian male comes to the physician because of severe productive cough for the past two months. He also complains of occasional blood in sputum, and dyspnea for the last three weeks. His past medical history is significant for otitis media, two episodes of pneumonia, and sinusitis. He and his wife were recently worked up for infertility. Physical examination shows crackles in the left upper lobe. Chest x-ray shows dilated and thickened airways and irregular peripheral opacities in the left upper lobe. Which of the following is the most appropriate test to make the diagnosis of his condition?
. Sweat chloride test
. DNA studies
. Pulmonary function tests
. Semen analysis
. Bronchoscopy
110) A 31-year-old woman presents to the emergency department complaining of shortness of breath. She denies associated chest pain or palpitations. She tells you that she recently returned from a trip to Thailand. She smokes one pack of cigarettes per day and drinks alcohol occasionally. She is married and uses oral contraceptives. She has no significant past medical history. On physical examination, her blood pressure is 110/70 mmHg and her heart rate is 120/min. A negative result on which of the following tests would best exclude pulmonary venous thromboembolism in this patient?
. Echocardiography
. Chest x-ray
. Venous ultrasound
. Plasma D-dimer
. Electrocardiogram
111) A 32-year-old Caucasian female presents to your office with persistent cough and shortness of breath. She has had three episodes of pneumonia over the last year. She had severe sinusitis one year ago, and an episode of bloody diarrhea that required hospitalization and IV antibiotic therapy six months ago. She does not smoke or consume alcohol. She denies any illicit drug use. She is currently not taking any medications. All her immunizations are up-to-date. Her blood pressure is 130/80 mmHg and heart rate is 90/min. Physical examination reveals fine crackles over the right lower lung lobe. No lower extremity edema is present. Neck palpation does not reveal any lymph node enlargement. The chest x-ray shows right lower lobe infiltrates and left upper lobe fibrosis. The ECG reveals non-specific ST segment and T wave changes. What is the best next step in the management of this patient?
. Measurement of serum alpha-1-antitrypsin level
. Methacholine challenge test
. Quantitative measurement of serum lg levels
. Sweat chloride test
. Ventilation/perfusion lung scan
112) A 25-year-old male presents with progressive shortness of breath over the past 6 months. His past medical history is significant only for neonatal hepatitis that resolved spontaneously when he was 6 months of age. The man has never smoked. On lung auscultation today, there are decreased breath sounds over both lower lobes. Chest x-ray demonstrates emphysematous changes in the bilateral lower lobes. Routine blood work is normal. Which of the following analyses would be most helpful in establishing this patient's diagnosis?
. Open lung biopsy
. Serum alpha-1 antitrypsin level
. Video-assisted lung biopsy
. High resolution CT scan of chest
. Pulmonary function testing
113) A 32-year-old man is intubated and mechanically ventilated after an opioid drug overdose. The ventilator triggers 12 breaths per minute, each delivering 500 ml of tidal volume at a flow rate of 60 L/min. You perform an inspiratory hold for 2 seconds following delivery of the tidal volume, and the airway pressure is measured to be 30 cm H2O. The measured pressure reflects which of the following?
. Upper airway resistance
. Total airway resistance
. Pulmonary compliance
. Expiratory muscle strength
. End-expiratory pressure
114) A 55-year-old man presents to your office with a six-month history of non-productive cough, especially at night. He denies postnasal drip, chest pain, difficulty breathing, or wheezing. His only other complaint is water brash. His past medical history is insignificant, and he is not taking any medications. He does not smoke or consume alcohol. Physical examination is insignificant. Chest x-ray and pulmonary function testing are normal. Esophagoscopy is also normal. What is the next best step in the management of this patient?
. Esophageal mucosal biopsy
. 24-hour pH recording
. Barium swallow
. Bernstein test
. Esophageal manometry
115) A 65-year-old Caucasian male comes to the physician because of shortness of breath, fever, and a productive cough for the last four days. He is a chronic smoker and alcoholic. He quit smoking two years ago. His medical problems include hypertension, chronic obstructive pulmonary disease, paroxysmal atrial fibrillation, and coronary artery disease. He is taking daily-inhaled ipratropium bromide, albuterol, metformin, metoprolol, warfarin, and diltiazem. His temperature is 38.9°C (102°F), blood pressure is 140/88 mmHg, pulse is 110/min, and respirations are 28/min. Pulse oximetry showed 88% on room air. Examination shows decreased breath sounds and crackles over the right lower lobe of the lung. Which of the following is the most appropriate next step in his management?
. Bronchoscopy
. Sputum gram stain
. Chest x-ray
. Mycoplasma serology
. Sputum culture
116) A 32-year-old woman comes to the emergency department complaining of sudden onset shortness of breath accompanied by a non-productive cough and left-sided chest discomfort that increases on inspiration. She denies subjective fever, coughing up blood, wheezing, palpitations, leg pain, and swelling of the lower extremities or any recent travel. Past medical history is significant for an appendectomy at age 15. Her medications include birth control pills and over- the-counter vitamins. She is a known carrier of sickle cell trait. Her father, age 65, has had diabetes for 20 years; mother, age 58, has coronary artery disease. She has never been pregnant, drinks alcohol socially and does not smoke. Her temperature is 99°F (38°C), blood pressure is 110/70 mmHg, pulse 130/min and respirations are 33/min. Pulse oximetry shows an oxygen saturation of 85% on 6 liters of oxygen. Her BMI is 30 kg/m2. She is alert and cooperative without cyanosis or jaundice. Her lungs are clear to auscultation. Her abdomen is soft, nondistended and non-tender. Which of the following is the best test to confirm this patient's diagnosis?
. EKG and cardiac enzymes
. Echocardiogram
. Doppler ultrasound of lower extremities
. Spiral CT-Scan of the chest
. Chest-x ray and sputum cultures
117) A 53-year-old male presents with progressively worsening dyspnea over a 4-month period. He also complains of decreased appetite, weight loss, and nagging epigastric discomfort. His past medical history is significant for a chronic duodenal ulcer for which he takes ranitidine on and off. He does not use tobacco, alcohol or illicit drugs. He has worked as a plumber for the past 30 years. On physical examination, his temperature is 36.9°C (98.4°F), blood pressure is 140/86 mm Hg, pulse is 80/min, and respirations are 15/min. Physical exam reveals fingernail clubbing and bibasilar end-inspiratory crackles on lung auscultation. Chest x-ray demonstrates ground glass opacities of the lower lung fields, multiple pleural plaques, and one 3x3 cm mass in the right lung periphery. CT guided biopsy of the mass is planned. Biopsy is most likely to show which of the following?
. Metastatic stomach cancer
. Metastatic colon cancer
. Metastatic pancreatic cancer
. Bronchogenic carcinoma
. Peritoneal mesothelioma
118) A 50-year-old male presents to his physician complaining of daytime somnolence. He reports that yesterday, he fell asleep while stopped at a red light. His wife adds that he is a habitual snorer, and sometimes seems to stop breathing for seconds at a time while sleeping. His past medical history is significant for hypertension, a 25 pack-year smoking history, and a two beer per day drinking habit. Physical examination reveals an obese, middle-aged man in no apparent distress. His pulse is 88/min, blood pressure is 160/100 mm Hg, and respirations are 14/min. The remainder of the physical examination, including chest auscultation, is within normal limits. Which of the following is the most appropriate next step in the management of this patient?
. Prescribe methylphenidate
. Pulmonary function testing
. MRI of the upper airways
. Nocturnal polysomnography
. Dexamethasone suppression test
119) A 37-year-old male is being evaluated after a motor vehicle accident. He complains of right sided chest pain. Physical examination reveals mild bruising over the right chest wall, and is otherwise unremarkable. Chest x-ray shows no rib fractures but a solitary round lesion is seen in the right upper lobe of the lung. Upon further questioning the patient denies recent weight loss or appetite change. He has never smoked cigarettes. Which of the following is the most appropriate next step in the management of his lung lesion?
. CT-guided biopsy
. CT scan of the chest
. Bronchoscopy
. Obtain previous x-rays to compare
. Obtain whole body CT scan
120) A 25-year-old female presents to the emergency department with sudden-onset severe shortness of breath and wheezing. She has a history of asthma. On examination, she is unable to speak in full sentences and is using accessory muscles of respiration. She is intubated, mechanically ventilated and treated with continuous albuterol nebulization and intravenous methylprednisolone. Within six hours, her condition is improved. She is extubated and treated with hourly nebulizer treatments. The next morning, she complains of muscle weakness. On physical examination, she has difficulty lifting her arms over her head and mild hand tremors. Her vital signs are stable What should be the immediate next step in her management?
. Check peak expiratory flow rate
. Check chest x-ray, PA view
. Check serum TSH level
. Check serum electrolyte panel
. Obtain electromyography (EMG)
121) A 40-year-old black male presents with dyspnea and tachypnea of sudden onset. He says that he was diagnosed with deep venous thrombosis (DVT) of the lower extremities three times before. Ventilation/perfusion scan reveals mismatched perfusion defect. Venous ultrasonography is positive for DVT. You suspect that inherited predisposition to hypercoagulation may be present. Which of the following is the most common form of such a predisposition?
. Protein C deficiency
. Protein S deficiency
. Antithrombin III deficiency
. Factor V Leiden
. Plasminogen disorders
122) A 45-year-old male immigrant from Haiti complains of cough and tenacious mucopurulent sputum for several months. He denies fever or chest pain, but notes shortness of breath and occasional blood-tinged sputum. He has received antibiotic treatment for similar symptoms twice in the past year. He has smoked 1 pack of cigarettes daily for the past 20 years. On physical examination, his temperature is 37.2°C (98.9°F), blood pressure is 120/68 mm Hg, pulse is 80/min, and respirations are 14/min. On lung auscultation there are coarse crepitations at the bilateral bases. Chest x-ray reveals prominent bronchioles in the lower lobes but is otherwise unremarkable. What is the most appropriate next step in the management of this patient?
. High resolution CT scan of the chest
. Bronchoscopy and alveolar lavage
. Bronchography using non-iodinated contrast medium
. Check sputum for acid fast bacillus (AFB)
. Echocardiography
123) A 78-year-old man is seen in the doctor’s office for a nonproductive cough, 9-kg (20-lb) unintentional weight loss, and bilateral breast enlargement, all occurring within the past 6 months. He has smoked two packs per day for the past 40 years. His past medical history is otherwise unremarkable, and he takes no medications. His temperature is 36.7°C (98.1°F), blood pressure is 125/85 mm Hg, pulse is 68/ min and regular, respiratory rate is 15/min, and oxygen saturation is 99% on room air. There are crackles at the left lower lung field and a ridge of symmetric glandular tissue (1 cm in diameter) around the nipple-areolar complexes of both breasts. Complete blood cell count shows a WBC count of 6000/mm³ hemoglobin of 14.7 g/dL, and platelet count of 210,000/ mm³. All other laboratory results are normal. X-ray of the chest shows a focal 5-cm mass lesion in the left lower lung corroborated by CT scan. Which of the following is most likely histologic type of lung cancer present in this patient?
Adenocarcinoma
Bronchoalveolar cell carcinoma
Large cell carcinoma
Small cell carcinoma
Squamous cell carcinoma
124) A 30-year-old patient with a history of mild persistent asthma (baseline peak expiratory flow rate of 85%) presents to the emergency department with shortness of breath and wheezing that has not relieved by her albuterol inhaler for the past 12 hours. She was able to tolerate pulmonary function tests and a set was performed. Which of the following is the most likely test result?
Decreased FEV1, normal/increased FVC, decreased FEV1: FVC ratio, with post- bronchodilator FEV1 increased by 13%
Decreased residual volume and total lung capacity
Increased FEV1, increased FVC, normal FEV1: FVC ratio
Increased residual volume, increased total lung capacity, increased FEV1
Normal FEV1, decreased FVC, increased FEV1: FVC ratio
125) A 27-year-old woman is 7 months pregnant with her first child. Her pregnancy has been uncomplicated to date. She presents to the emergency department complaining of sudden-onset, right-sided chest pain that is exacerbated with deep breathing and shortness of breath, which began 1 hour ago. She denies leg pain and notes that her legs began swelling during the sixth month of her pregnancy but the swelling has not worsened. Her temperature is 37.9°C (100.3°F), blood pressure is 130/87 mm Hg, pulse is 107/min and regular, respiratory rate is 24/min, and oxygen saturation is 90% on room air, increasing to 98% with 4 L oxygen via nasal cannula. Physical examination is significant for crackles at the lower right lung field and a negative Homans’ sign bilaterally. X-ray of the chest appears normal. The D-dimer level is elevated. ECG shows sinus tachycardia, right-axis deviation, S wave in lead I, Q wave in lead III, and an inverted T wave in lead III. Which of the following is the most appropriate next step in diagnosis?
Arterial blood gas analysis
Doppler ultrasound of the lower extremity
MRI of the lower extremity
Pulmonary angiography
Ventilation/perfusion scans
126) A 55-year-old man presents to his physician’s office with increasing dyspnea on exertion. He denies chest pain, diaphoresis, nausea, or vomiting. He has been involved in eight motor vehicle accidents in the past 3 years. Past medical history is significant for hypertension, for which he takes a diuretic. His temperature is 37.2°C (99.0°F), blood pressure is 121/82 mm Hg, pulse is 85/min, respiratory rate is 14/min, and oxygen saturation is 99% on room air. Physical examination is significant for a body mass index of 35 kg/m², a diffuse and laterally displaced point of maximal intensity, and an S3 gallop. Which of the following is the most appropriate next step in diagnosing his most likely underlying condition?
Cardiac catheterization
Echocardiogram
Exercise tolerance test
Polysomnography
X-ray of the chest
127) A 63-year-old woman is seen in the emergency room with acute shortness of breath. There is no history of heart or lung problems in the past. She was recently diagnosed with breast cancer and is undergoing active treatment. On examination, her blood pressure is 120/80 mm Hg, pulse 100/min, and heart and lungs are normal. There are no clinical signs of deep venous thrombosis (DVT). Which of the following investigations is most likely to rule out a pulmonary embolism (PE)?
Normal CXR
Normal electrocardiogram (ECG)
Normal ventilation-perfusion lung scan
Normal ventilation scan
Normal magnetic resonance image (MRI)
128) A 40-year-old woman has been complaining of a 3-year history of increasing dyspnea and fatigue. She has no other medical illness. Physical examination reveals increased jugular venous pressure (JVP) with prominent c-v wave, and a reduced carotid pulse. Precordial examination reveals a left parasternal lift, loud P2, and right- sided S3 and S4. There are no audible murmurs. CXR reveals clear lung fields and an ECG shows evidence of right ventricular hypertrophy. Pulmonary function tests show a slight restrictive pattern. Primary pulmonary hypertension is suspected. Which of the following is the most appropriate test to confirm the diagnosis?
Open lung biopsy
Pulmonary angiography
Cardiac catheterization
Noninvasive exercise testing
Electrophysiologic testing
129) A 58-year-old man is recently diagnosed with bowel cancer. He now complains of vague chest discomfort and shortness of breath. On examination, he is unwell, blood pressure 90/50 mm Hg, pulse 110/min, respirations 26/min, and oxygen saturation 88%. His lungs are normal on auscultation, the JVP is 8 cm, and P2 is loud. There is no edema or leg tenderness on palpation. A quantitative (ELISA) D-dimer assay is positive, ECG reveals sinus tachycardia, and cardiac enzymes are negative. The lung scan is read as high probability for PE. Which of the following tests is most likely to help in guiding emergent therapy?
Echocardiogram
CT scan
Venous ultrasound of the legs
Contrast phlebography
Pulmonary function tests
130) A 28-year-old man presents with coughing up blood and sputum. He gives a history of recur- rent pneumonias and a chronic cough productive of foul-smelling purulent sputum. He has no other past medical history and is a lifetime nonsmoker. On physical examination, there are no oral lesions, heart sounds are normal, and wet inspiratory crackles are heard at the lung bases posteriorly. He also has clubbing of his fingers, but there is no hepatosplenomegaly or any palpable lymph nodes. CXR show fibrosis and pulmonary infiltrates in the right lower lung. Which of the following is the most appro- priate initial diagnostic test?
Chest CT scan
Bronchoscopy
Bronchography
Open thoracotomy
Bronchoalveolar lavage
131) A 5-year old girl is brought to the emergency department in December by her mother, who complains that her daughter seems confused. The mother reports that her daughter has complained of intermittent headaches since the two of them moved into the first floor of an older apartment building 6 months ago. The mother has been at home with the daughter for the past 24 hours and the girl appears lethargic and is complaining of joint aches, nausea, and a headache. Her pulse is 120/min, blood pressure is 130/85 mm Hg, respiratory rate is 25/min, and oxygen saturation is 100% on room air. The girl’s mother also notes having a slight headache that started yesterday. Which of the following diagnostic tests should be most rapidly pursued?
Arterial blood gas
CT scan of the head
Direct laryngoscopy
ECG
Toxicology screen
132) A 34-year-old African American man presents with mild dyspnea on exertion and joint discomfort in his knees, wrists, and ankles. He also has a fever and red tender rash on his shins. Physical examination reveals hepatosplenomegaly, generalized lymphadenopathy, and tender erythematous nodules on his legs. CXR shows bilateral symmetric hilar adenopathy. Which of the following laboratory findings is not characteristic of this condition?
Hyperglobulinemia
Elevated ACE level
Elevated sedimentation rate (ESR)
Elevated serum calcium
Normal gallium scan
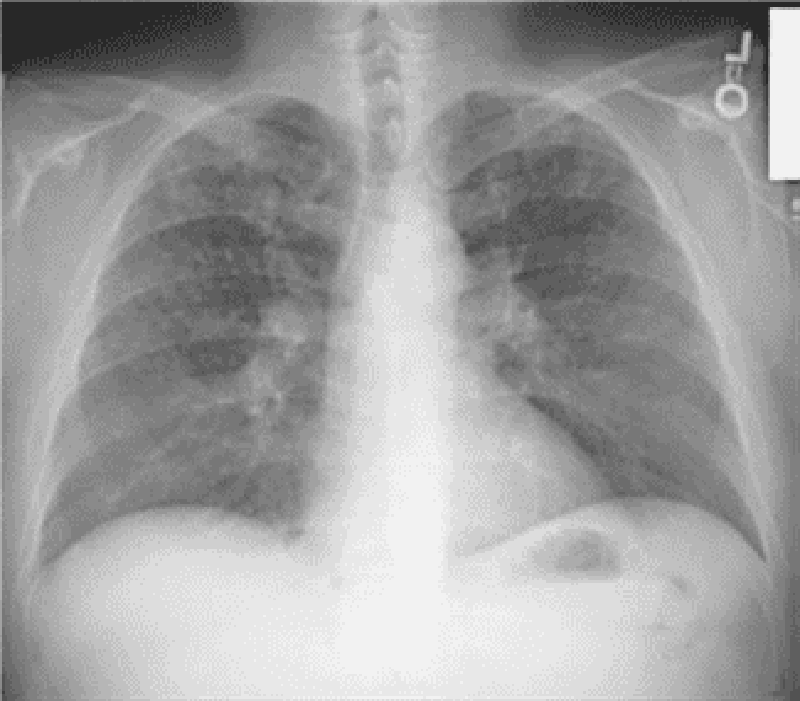
133) A 21-year-old man has a nonproductive cough, shortness of breath, and chest pain, which changes with breathing. He also has pain in the left arm. On examination, there is tender- ness over the left shoulder, heart sounds are normal, and the lungs are clear. CXR reveals a lytic lesion in the left humerus and reticulonodular opacities in the upper and middles lobes. The eosinophil count is normal. Which of the following is the most appropriate initial diagnostic test?
Lung biopsy
Humerus bone biopsy
CT scan of chest
Bronchoscopy
Pulmonary function tests
134) A 33-year-old woman, otherwise perfectly well, presents with recurrent episodes of hemopty- sis. She has no fever, weight loss, cough, or sputum production. Her physical examination is entirely normal. Her CXR, biochemisty, CBC, and coagulation profile are also normal. Which of the following is the most appropriate initial diagnostic test?
Echocardiogram
Gallium scan
CT scan of chest
Bronchoscopy
Pulmonary function tests
135) A 31-year-old man with severe kyphoscoliosis due to cerebral palsy is experiencing worsening shortness of breath with exertion. On examination, he has a severe scoliosis to the left and decreased air entry to that side. His right lung is clear, JVP is 3 cm, and heart sounds are normal. Pulmonary function tests are performed. Which of the following is the most likely abnormality to be seen on the pulmonary function tests?
Increased total lung capacity (TLC)
Increased functional residual capacity (FRC)
Decreased TLC
Increased compliance
Increased vital capacity (VC)
136) An 83-year-old man with Parkinson’s disease presents with low-grade fever and cough for several weeks. Lately, he has been experiencing more rigidity and difficulty with his walking. He is on a levodopa/carbidopa combination for treatment for the past 5 years. On examination, his gait is shuffling and slow. He has a tremor in his left hand at rest, and there is cogwheel rigidity of the forearm. There are crackles in the left lower lung field. CXR reveals a lung abscess in the left lower lobe. Which of the following is the most likely bacteriologic diagnosis for the lung abscess?
Oropharyngeal flora
Tuberculosis
Staphylococcus aureus
Pseudomonas aeruginosa
Candida albicans
137) A 28-year-old African American woman presents with mild dyspnea on exertion. She reports no coughing, sputum production, or wheezing symptoms, but has noticed a red tender rash on her shins. Physical examination reveals hepatosplenomegaly, generalized lymphadenopathy, and tender erythematous nodules on her legs. CXR shows bilateral symmetric hilar adenopathy. Her pulmonary function tests reveal a mild restrictive pattern. Which of the following tests will most likely make a definitive diagnosis?
Tuberculin skin test
Bronchoscopy with transbronchial biopsy
Elevated ACE level
Serum hypercalcemia
Increased uptake on gallium scan
138) A 69-year-old woman has recently returned on an overnight flight from Europe. She now complains of vague chest discomfort and shortness of breath. On examination, she is comfortable, blood pressure 130/80 mm Hg, pulse 90/min, respirations 18/min, and oxygen saturation 97%. Her heart and lungs are normal on auscultation, and there is no edema or leg tenderness on palpation. A quantitative (ELISA) D-dimer assay is positive. Which of the following statements regarding the D-dimer assay is correct?
It is sensitive but not specific
It is specific but not sensitive
It is neither specific nor sensitive
A negative result suggests myocardial ischemia
It is both sensitive and specific
139) A 52-year-old Caucasian male presents complaining of diminished energy for the past three months. He appears very sad and moves slowly. He says that he has been feeling terrible after his wife died in a car accident three months ago. He is filled with thoughts of guilt because he was driving the car when the accident took place. Since then, he has been suffering from disturbed sleep and finds himself unable to focus on his favorite activities, like coin collecting or fishing. He reports being disturbed by repeated flashbacks of the event. He keeps himself aloof and isolated from others because he "just doesn't feel like socializing anymore." He adds that he has a poor appetite and has gained 20 lbs (9.1 kg). He admits to wanting to "end my life in order to escape the memories of that nightmarish day." He is able to contract for safety. What is the most appropriate next step?
. Refer him for psychotherapy for post-traumatic stress disorder
. Reassure him that this is normal bereavement
. Prescribe fluoxetine
. Order blood tests
. Admit him for electroconvulsive therapy
140) A 6-year-old girl is brought to the physician by her mother, who says the child has been falling behind at school. She notes that the girl did not speak until the age of 4. She is friendly at school, but is unable to complete most tasks, even when aided. She is noted to have a very short attention span and occasional temper tantrums at school and at home. Which of the following tests would be most helpful in establishing the diagnosis?
. Electroencephalogram (EEG)
. Hearing test
. IQ testing
. Complete blood count (CBC)
. Lumbar punture
141) A 23-year-old man presents to the emergency room with the history of a fever up to 38°C (100.5°F) intermittently over the past 2 weeks, a persistent cough, and a 10-lb weight loss in the past month. He notes that he has also been becoming increasingly forgetful for the past month and that his thinking is “not always clear.” He has gotten lost twice recently while driving. Which of the following diagnostic tests will be most helpful with this patient?
. EEG
. Liver function tests
. Thyroid function tests
. HIV antibody test
. Skull x-ray
142) A 29-year-old man is brought to the hospital because he was found running around on the streets with no shoes on in the middle of winter, screaming to everyone that he was going to be elected president. Upon admission to the hospital, he was stabilized on olanzapine and lithium and then discharged home. Assuming the patient is maintained on the olanzapine and the lithium, which of the following tests should be performed at least once per year?
. MRI of the brain
. Liver function tests
. Creatinine level
. Rectal exam to look for the presence of blood in the stool
. ECG
143) A middle-aged woman presents with a variety of cognitive and somatic symptoms, fatigue, and memory loss. She denies feeling sad, but her family physician is aware of this patient’s lifelong inability to identify and express feelings. He suspects she is depressed. Which of the following results is most likely to confirm a diagnosis of depression?
. Reduced metabolic activity and blood flow in both frontal lobes on PET scan
. Diffuse cortical atrophy on CAT scan
. Atrophy of the caudate on MRI
. Prolonged REM sleep latency in a sleep study
. Subcortical infarcts on MRI
144) A 40-year-old female presents to your office complaining of the pain in her right hip. She denies trauma and says that the pain began two weeks ago and gradually increased. Her past medical history is significant for systemic lupus erythematosus diagnosed seven years ago. Her current medications include prednisone, hydroxychloroquine, and lansoprazole. There is no local tenderness on physical examination and the range of motion of the right hip is normal. Hip radiograph is normal. What is the next best step in the management of this patient?
. Joint aspiration
. Low-dose NSAIDs
. Increase the dose of prednisone
. MRI of the hip
. Observation
145) A 61-year-old man presents to your office with a two-week history of low back pain. He describes the pain as constant, dull, and aching. It is non-radiating. The pain is not affected by movement and cannot be fully relieved by lying down. He denies fever and urinary frequency or hesitancy. He has started taking sleeping pills because the pain disturbs him during the night. On physical examination, the paraspinal muscles are non-tender. Percussion over the lumbar vertebrae does not elicit tenderness. Knee reflexes are symmetric and he has 5/5 strength in the extremities bilaterally. A straight leg raise test is negative. Which of the following is the best test for this patient?
. Electromyography
. HLA genotyping
. Urethral cultures
. Prostate-specific antigen (PSA)
. Abdominal ultrasonography
146) A 68-year-old Caucasian male complains of right-sided leg pain over the last year. The pain is poorly controlled with over-the-counter pain medications. He also complains of frequent headaches. His past medical history is significant for hypertension and recent hearing loss. An X-ray of the skull shows areas of bone resorption and sclerosis. Which of the following are the most likely findings on laboratory work-up? (Serum calcium, serum phosphate, alkaline phosphatase, Urinary hydroxyproline)
. Normal Normal Normal High
. Normal Normal High High
. High Low High Normal
. High Normal Normal Normal
. Low High Normal Normal
147) A 25-year-old female presents to the physician's office complaining of fatigue, joint pains, and frequent mouth ulcers over the past three months. She has no medical problems and does not take any medications. She does not use tobacco, alcohol or drugs. Her temperature is 37.5°C (99.5°F), blood pressure is 150/100 mmHg and pulse is 78/min. Examination shows erythema over the cheeks and nose. Labs reveal a serum creatinine of 2.8 mg/dl and her urinalysis shows 2+ protein and 20 RBC/HPF. Anti- double stranded antibodies (anti-dsDNA) are positive. Which of the following is the most appropriate next step in management of this patient?
. Kidney biopsy
. Methotrexate
. Methylprednisolone
. Cyclophosphamide
. Cyclophosphamide and methylprednisolone
148) A 43-year-old man was brought to the ED after he was unable to get out of his bed today due to leg weakness. He has been having constant back pain over the past several days. His past medical history is significant for poorly controlled diabetes mellitus and hypertension. His temperature is 38.3°C (101°F), pulse is 100/min, respirations are 18/min, and blood pressure is 150/100 mmHg. On examination, he smells of urine. His back is tender to palpation over L2-L5. Neurologic exam reveals 3/5 strength in the lower extremities with decreased sensation to temperature and light touch. He has an extensor plantar response bilaterally. Which of the following is the best next step in evaluating this patient?
. Electromyography
. CT scan of the spine
. Lumbar puncture
. MRI of the spine
. HbA1c level
149) A 54-year-old man presents to the emergency room with acute pain, swelling and redness of his right knee. He had one episode of gouty arthritis a year ago that resolved quickly with indomethacin. He also has type 2 diabetes, hypertension and chronic renal disease. He does not use any illicit drugs. His temperature is 38.3°C (100.9°F), blood pressure is 110/65 mmHg, and pulse is 110/min. Examination reveals a tender, erythematous effusion of the right knee with decreased range of motion. Which of the following is the most appropriate next step in management?
. Serum uric acid level
. Indomethacin
. X-ray of the knee
. MRI of the knee
. Synovial fluid analysis
150) A 23-year-old man complains of progressive low back pain for the past several months. He has morning stiffness that lasts for one hour. He has no history of trauma to his back and denies any recent illness. He had an episode of pain, blurring, and photophobia of his right eye two years ago that required ophthalmology evaluation. His vital signs are within normal limits. Examination shows tenderness in both sacroiliac joints and reduced range of motion of the lower back. If measured, which of the following is most likely to be present in this patient?
. Rheumatoid factor
. Anti-cyclic citrullinated peptide (CCP) antibodies
. Anti dsDNA antibodies
. HLA B 27 positivity
. Glutamic acid decarboxylase antibodies
151) A 65-year-old man presents with right shoulder pain and weakness after falling on his outstretched hand. The pain is worse when he tries to position his arm above the shoulder level or when he pulls or pushes. He also complains of pain when he lies on the affected shoulder. He has a 40-pack-year history of cigarette smoking. His father died of multiple myeloma. His vital signs are within normal limits. Examination shows limitation of mid arc abduction and external rotation that does not improve after lidocaine injection. There is no swelling, redness or warmth of the joint. Radial pulse is normal. Muscle tone and bulk is within normal limits. Which of the following would be most helpful in confirming the patient's diagnosis?
. X-ray shoulder
. Chest-X ray
. Bone marrow biopsy
. MRI of the shoulder
. MRI of the cervical spine
152) A 49-year-old African American female complains of progressive exertional dyspnea. She also complains of swelling and pain in her finger joints over the last 6 months. She has been treated for severe heartburn with pantoprazole and for hypertension with lisinopril and hydrochlorothiazide. Her blood pressure is 145/100 mmHg and her heart rate is 80/min. Physical examination reveals prominent jugular venous distention. Her lungs are clear to auscultation, and no murmurs are present on cardiac auscultation. Her skin is thickened and discolored over the fingertips and interphalangeal joints. There is mild pitting ankle edema. Which of the following is most likely to be positive in this patient?
. Anti-topoisomerase-1 antibodies
. Rheumatoid factor
. Antimitochondrial antibodies
. Anti-neutrophil cytoplasmic antibodies
. Anti-smooth muscle antibodies
153) A 52-year-old woman presents with gradual-onset weakness in her leg muscles. She has noted difficulty climbing stairs and raising from a chair that has been worsening for the past few years. She initially related her symptoms to simply being "out of shape." She has no problem with chewing food. She has no pain in her muscles and has no skin rash. She takes metoprolol and hydrochlorothiazide for hypertension. She does not use tobacco, alcohol or drugs. Her vital signs are within normal limits. Examination reveals mild weakness of the thigh muscles in both legs. Deep tendon reflexes and sensory examination shows no abnormalities. Babinski sign is negative. Which of the following is most likely abnormal in this patient?
. MRI of the spine
. Electroencephalogram
. Temporal artery biopsy
. Lumbar puncture
. Muscle biopsy
154) A 62-year-old Caucasian female complains of difficulty swallowing solid food. She needs to take sips of water during every meal to help with swallowing. Her past medical history is significant for hypertension controlled with metoprolol. She uses some over-the-counter eye drops for eye dryness. Her blood pressure is 140/90 mmHg and heart rate is 60/min. Physical examination reveals prominent dental caries. There are bilateral firm submandibular swellings present on neck palpation. Which of the following is the best test to confirm this patient's diagnosis?
. Antibodies to Ro/SSA
. Antimitochondrial antibodies
. Barium swallow test
. CT scan of the neck
. Esophageal endoscopy with biopsy
155) A 60-year-old male presents to the emergency room with a two-week history of low back pain and low-grade fever. His past medical history is insignificant. He tried several over-the-counter pain medications with little success. His temperature is 38.3°C (101°F), blood pressure is 120/76 mmHg, pulse is 90/min, and respirations are 16/min. Physical examination reveals percussion tenderness over the lumbar vertebrae and local paravertebral muscular spasm. Neurological examination shows 2+ deep tendon reflexes and 5/5 muscle power. The straight-leg raising test is negative at 90 degrees. Laboratory values are: Hemoglobin 12.2 g/dL, Leukocyte count 10,700/cmm, Segmented Neutrophils 63%, Bands 4%, Eosinophils 3%, Basophils 0%, Lymphocytes 23%, Monocytes 6%, Platelets 400,000/cmm, ESR 75 mm/hr. What is the next step in the management of this patient?
. Plain radiograph
. Bone scan
. MRI of the spine
. Serum rheumatoid factor
. Physiotherapy
156) A 52-year-old man presents with 24 hours of pain and swelling of his right knee. He also reports having constipation, excessive urination, and fatigue for the past several months. He denies fevers, chills, and trauma to the knee. He does not use tobacco, alcohol or drugs. His temperature is 37.2°C (98.9°F), and blood pressure is 130/76 mmHg. Examination shows tenderness, erythema, and swelling of the right knee. His lab values are: Serum sodium 138 mEq/L, Serum potassium 4.0 mEq/L, Serum creatinine 1.1 mg/dl, Serum calcium 11.9 mg/dl, Serum phosphorous 1.9 mg/dl, Blood glucose 98 mg/dl. Which of the following would synovial fluid analysis from the knee most likely reveal?
. Needle shaped crystals with negative birefringence
. Coffin lid shaped crystals
. Rhumboid shaped crystals with positive birefringence
. Numerous polymorphs filled with gram positive cocci
. Numerous lymphocytes and budding yeast
157) A 24-year-old Caucasian male undergoes pulmonary function testing. The following values are obtained: FEV 80% of predicted, FEV1/FVC 85%, FRC 110% of predicted. He has no current complaints except for occasional low back pain treated with naproxen. He smokes one pack per day and drinks a six-pack of beer each weekend. His ESR is 47 mm/hr. Which of the following best explains the pulmonary function test findings in this patient?
. Emphysema
. Small airway obstruction
. Pulmonary fibrosis
. Chest wall motion restriction
. Pulmonary vascular disease
158) A 58-year-old woman has had bilateral hip and knee pain for the past several months. The pain is worse with activity and better with rest. Recently she has noticed swelling of the right knee. She reports morning stiffness of about 10-15minutes duration. She denies fever or weight loss. Her past medical history is significant for hypertension, type 2 diabetes, gastroesophageal reflux disease, and obstructive sleep apnea. She takes hydrochlorothiazide, lisinopril, omeprazole, insulin and aspirin. She does not use tobacco, alcohol or drugs. Her temperature is 37.2°C (98.9°F), and blood pressure is 146/86 mmHg. Examination shows a mild effusion, tenderness, and decreased range of motion of the right knee. Synovial fluid analysis reveals the following: Cell count 1100/ml, Gram stain negative, Crystals absent. Plain films of her knee joint would most likely reveal?
. Punched out erosions with a rim of cortical bone
. Periarticular osteopenia and joint margin erosions
. Narrowing of joint space and osteophyte formation
. Normal joint space with soft tissue swelling
. Calcifications of cartilaginous structures
159) A 23-year-old white woman presents complaining of 6 months of progressive low back pain. She complains of morning stiffness that lasts one hour, and says her symptoms improve with physical activity. She denies rash, eye pain, urinary problems, and diarrhea. Her past medical history is significant only for an appendectomy at the age of 16 years. She has been taking birth control pills for the past two years. She is afebrile with normal weight and height. Examination reveals reduced forward flexion of the lumbar spine and tenderness over the sacroiliac joints. The remainder of the physical examination is normal. Which of the following is the most appropriate next step in the management of this patient?
. HlA-827 testing
. ANA and rheumatoid factor levels
. Bone scan
. MRI of the spine
. X-ray of the sacro-iliac joints

160) A 33-year-old African-American woman presents with one week of painful skin lesions on her legs. She has no cough, shortness of breath or bowel symptoms, and denies any recent illness or travel. She has no other significant past medical history and does not take any medication. She smokes one pack of cigarettes and drinks one glass of wine daily. She denies a history of sexually transmitted diseases and has been married to a monogamous partner for the past eight years. Her mother was diagnosed with ovarian cancer at age 65. Her temperature is 37.2°C (98.9°F), and blood pressure is 126/76 mmHg. On examination, she has multiple tender pink to reddish nodules noted below the knee on the extensor surface, as shown below. Which of the following is the most appropriate next step in her management?
. CT scan of the abdomen
. HIV testing
. Chest x-ray
. Rectal swab for culture
. Colonoscopy
161) A 60-year-old male presents to your office complaining of right-sided neck pain and numbness over the posterior surface of the forearm. He had several such episodes over the last two years that responded to NSAIDs and physical therapy. Physical examination reveals limited neck rotation and lateral bending. There is decreased pinprick sensation on the posterior aspect of the right forearm, but no muscle weakness is present. Triceps reflex is normal. Which of the following is the most likely finding on the neck radiography of this patient?
. Reversed lordotic curve
. Bony spurs
. Vertebral body osteoporosis
. Osteolytic lesions
. Compression fracture
162) A 40-year-old school teacher comes to the physician's office complaining of joint pain. Her symptoms began 10 days ago and consist of pain in the metacarpophalangeal (MCP) joints, proximal interphalangeal (PIP) joints, wrists, knees and ankles, bilaterally. She describes joint stiffness lasting 10 to 15 minutes after a prolonged rest. She denies fever, malaise, weight loss and skin rash. Her past medical history is insignificant. She does not take any medications. On examination, there is no evidence of swelling, redness or tenderness of the involved joints. The remainder of the physical examination is unremarkable. Which of the following is most likely elevated in this patient?
. Rheumatoid factor
. Anti-B19 IgM antibody
. Anti-dsDNA
. Erythrocyte sedimentation rate
. Antinuclear antibodies
163) A 40-year-old woman complains of 7 weeks of pain and swelling in both wrists and knees. She has several months of fatigue. After a period of rest, resistance to movement is more striking. On examination, the metacarpophalangeal joints and wrists are warm and tender. There are no other joint abnormalities. There is no alopecia, photosensitivity, kidney disease, or rash. Which of the following is correct?
. The clinical picture suggests early rheumatoid arthritis, and a rheumatoid factor should be obtained.
. The prodrome of lethargy suggests chronic fatigue syndrome.
. Lack of systemic symptoms suggests osteoarthritis.
. X-rays of the hand are likely to show joint space narrowing and erosion.
. An aggressive search for occult malignancy is indicated.
164) A 70-year-old man complains of fever and pain in his left knee. Several days previously, he suffered an abrasion of his knee while working in his garage. The knee is red, warm, and swollen. An arthocentesis is performed, which shows 200,000 leukocytes/μL and a glucose of 20 mg/dL. No crystals are noted. Which of the following is the most important next step?
. Gram stain and culture of joint fluid
. Urethral culture
. Uric acid level
. Antinuclear antibody
. Antineutrophil cytoplasmic antibody
165) A 60-year-old woman complains of dry mouth and a gritty sensation in her eyes. She states it is sometimes difficult to speak for more than a few minutes. There is no history of diabetes mellitus or neurologic disease. The patient is on no medications. On examination, the buccal mucosa appears dry and the salivary glands are enlarged bilaterally. Which of the following is the best next step in evaluation?
. Lip biopsy
. Schirmer test and measurement of autoantibodies
. IgG antibody to mumps virus
. A therapeutic trial of prednisone for 1 month
. Administration of a benzodiazepine
166) A 45-year-old woman has pain in her fingers on exposure to cold, arthralgias, and difficulty swallowing solid food. What is the best diagnostic test?
. Rheumatoid factor
. Antinucleolar antibody
. ECG
. BUN and creatinine
. Reproduction of symptoms and findings by immersion of hands in cold water
167) A 65-year-old man develops the onset of severe knee pain over 24 hours. The knee is red, swollen, and tender. He has a history of diabetes mellitus and cardiomyopathy. An x-ray of the knee shows linear calcification. Definitive diagnosis is best made by which of the following?
. Serum uric acid
. Serum calcium
. Arthrocentesis and identification of positively birefringent rhomboid crystals
. Rheumatoid factor
. ANA

168) Over the last six weeks a 45-year-old nurse has developed progressive difficulty getting out of chairs and climbing stairs. She can no longer get in and out of the bathtub. She has no muscle pain and takes no regular medications. She does not use alcohol and does not smoke cigarettes. On examination she has a purplish rash that involves both eyelids (see figure). There is weakness of the proximal leg muscles. What is the best next diagnostic test?
. Vitamin B12 level
. Chest x-ray
. HLAB27
. MRI scan of the lumbar spine
. CPK
{"name":"Ichigo USLME Med Test P2", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"1) A 55-year-old woman comes to her primary care physician with complaints of pain, itching and red streaks in her left arm. She feels that her arm is \"simply not the same\". She had a similar episode in her chest almost 2 weeks ago, but it went away on its own. She has no other complaints, except for heartburn and some upper abdominal pain that has been there for a few months. She takes antacids for it, but has never got over it completely. She thinks that she has lost some weight but she feels happy about it, as she always wanted to lose weight. Her vitals are stable and there is mild epigastric tenderness. She has tender, erythematous, cord like veins palpable over left arm and some over the chest. She smokes 1-2pack\/day for 15years and drinks alcohol, only on parties. What is the next best step in this patient?","img":"https://cdn.poll-maker.com/20-809336/tp2-11.png?sz=1200"}
More Quizzes
Όλα για τον Κωστή
740
Quiz para el Presente
840
Macaw Quiz: Test your knowledge.
5218
Training Account
1367
Free Civil War: Test Your Knowledge
201026155
Do I Have COPD or Asthma - Free COPD Knowledge Test
201024776
Free Java Boolean & If Statement
201026155
Think You Know Languages? Take the Ultimate Language!
201047289
Free SC Biology EOC Practice Test
201028028
Hidden Political Figures: Uncover Untold Political Legacies
15826658
Ultimate Cos: Master Cosine & Sine Rule Like a Pro
201049350
Ace Your AP Biology Unit 1 with This Free Practice Test
201044533