(New) Part 3 "510-764" Na IV (638-678)
44) A 65-year-old man comes to the physician's office with a 2-month history of dysphagia. He initially had difficulty swallowing solids, but now this includes liquids. He has occasional heartburn, which usually responds well to antacids. He has lost 20 lbs of weight in the past 2 months. He has a 40 pack- year history of smoking. He has been a chronic alcoholic for 20 years. His temperature is 36.7°C (98°F), blood pressure is 110/80 mmHg, pulse is 66/min, and respirations are 14/min. Physical examination shows no abnormalities. Barium studies show a minimally dilated esophagus with beak-shaped narrowing. Manometry shows increased lower esophageal sphincter tone. Which of the following is the most likely diagnosis?
Achalasia
Esophageal cancer
Scleroderma
Peptic stricture
Diffuse esophageal spasm
45) Ms. Lee, a 62-year-old Chinese woman, comes with yellowness in her eyes for the past 6 weeks. She is generally feeling tired, has lost some weight, and occasionally had some nausea. She denies any altered bowel habits. She is a non-smoker but drinks 2-3 beers each night. Her dad is suffering from high cholesterol and also has had stroke. She had a dilatation and curettage for an abnormal pap smear 15 years ago. Her vitals are stable and she is afebrile. She has marked scleral icterus. An abdominal examination reveals normal bowel sounds and no organomegaly. Her stools were occult blood negative. Her liver function tests and enzymes were ordered and the results are: Total protein 6.1 g/dl, Albumin 39 g/dl, AST 67U/L, ALT 52U/L, Alkaline phosphatase 290 U/L, Total bilirubin 96 mg/dl, Direct bilirubin 89 mg/dl, Serum lipase is 46 U/L, Anti-mitochondrial antibodies negative. Which of the following is the most likely cause of these findings?
Primary biliary cirrhosis
Chronic pancreatitis
Viral hepatitis
Pancreatic carcinoma
Hepatocellular carcinoma
46) A 64-year-old white male with a history of severe stable angina and peripheral vascular disease undergoes coronary artery bypass surgery. His post-operative course is complicated by hypotension, which is treated successfully; however, a few hours later, he experiences abdominal pain followed by bloody diarrhea. His temperature is 37.8°C (100°F), blood pressure is 110/60 mmHg, pulse is 110/min, and respirations are 20/min. Abdominal examination is benign. Laboratory studies show a WBC count of 15,000/cmm with 7% bands. The lactic acid level is elevated. A CT scan is ordered. Which of the following areas of the colon will most likely show abnormal findings?
Sigmoid colon
Splenic flexure
Ascending colon
Mid transverse colon
Hepatic flexure
47) A 52-year-old man presents to your office after passing a black stool. He also describes occasional abdominal discomfort and nausea but denies hematemesis. He says that food seems to help his abdominal pain, so he eats frequently during the day and keeps some snacks on his night stand. As a consequence, he has gained 5 pounds over the last year. He admits that his diet is lacking in vegetables and fruit. He drinks one to two cans of beer nightly, but does not smoke or use illicit drugs. He says that his father died of colon cancer and his mother died from a stroke. Physical examination reveals a right-sided carotid bruit. The fecal occult blood test is positive. Which of the following is the most likely cause of his condition?
Mesenteric ischemia
Mallory-Weiss tear
Inflammatory bowel disease
Erosive gastritis
Peptic ulcer disease
48) A 35-year-old Caucasian female presents to your office with several months history of heartburn. She also describes a periodic 'sticking sensation' in her throat during the meal. Her past medical history is significant for asthma that is controlled with inhaled steroids, and acoustic neuroma that was removed 2 years ago. She does not smoke or consume alcohol. She denies any recreational drug use. She is not allergic to any medications. She works as a secretary at a private firm, and considers her work moderately stressful. Her family history is significant for breast cancer in her mother and prostate cancer in her father. Endoscopic evaluation shows mild hyperemia in the distal esophagus. Esophageal manometry reveals absent peristaltic waves in the lower two-thirds of the esophagus and a significant decrease in lower esophageal sphincter tone. Which of the following is the most likely cause of this patient's complaints?
Achalasia
GERD with or without hiatal hernia
Scleroderma
Non-ulcer dyspepsia
Diffuse esophageal spasm
49) A 42-year-old male comes to the physician's office for evaluation of skin rash and hair loss. He has a long history of Crohn's disease and has had extensive small bowel resection resulting in short bowel syndrome. He is currently receiving total parenteral nutrition. When he does try to eat, he complains that the food does not taste good. His vital signs are stable. Examination shows alopecia and bullous, pustular lesions around the perioral and periorbital areas. Which of the following is the most likely cause of his current symptoms?
Celiac disease
Zinc deficiency
Vitamin A deficiency
Vitamin B 12 deficiency
Systemic lupus erythematosus
50) A 45-year-old Hispanic male comes to the emergency department because of a two-day history of intermittent abdominal pain and bloody diarrhea. He has had four similar episodes in the past year. He is subsequently admitted to the floor. Radiographic and endoscopic evaluations show extensive disease from the terminal ileum to the rectum with multiple ulcerations and pseudopolyps. Biopsy of the lesion shows noncaseating granulomas and crypt abscess. Which of the following is the most characteristic feature which favors the diagnosis of Crohn's disease against that of ulcerative colitis?
Crypt abscess
Abdominal pain and bloody diarrhea
Non-caseating granulomas
Disease from terminal ileum to rectum
Pseudopolyps
51) A 54-year-old male presents to the emergency department with a 1-week history of abdominal pain. His other symptoms are nausea, vomiting, low-grade fever, and loss of appetite. He does not use alcohol. He has a seizure disorder, for which he takes a "prescription drug." X-ray films of his chest and abdomen show no abnormalities. His abdominal CT scan is shown below. Which of the following is the most likely explanation for this patient's abdominal symptoms?

Gall bladder pathology
Kidney pathology
Pancreas pathology
Air in the stomach
Liver pathology
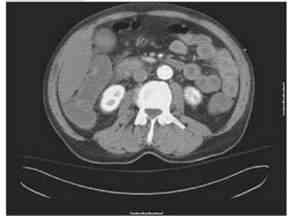
52) A 70-year-old male presents to the emergency room complaining of weakness, dizziness and back pain. He denies nausea, vomiting, diarrhea, chest pain, palpitations, shortness of breath, urinary symptoms, or black stools. His past medical history is significant for diabetes mellitus, diabetic nephropathy and retinopathy, hypertension, atrial fibrillation and chronic leg cellulitis. He takes warfarin for chronic anticoagulation. On physical examination, his blood pressure is 139/75 mmHg and his heart rate is 110 and irregular. His WBC count is 10,500/mm3, hemoglobin level is 7.0 mg/dl and platelet count is 170,000/mm3. An abdominal CT image is shown on the slide below. Which of the following is the most likely diagnosis?

Renal cell carcinoma
Vertebral fracture
Retroperitoneal hematoma
Hydronephrosis
Mesenteric ischemia
53) A 43-year-old man is evaluated for a one-year history of chronic abdominal pain. He describes episodes of epigastric and left upper quadrant pain that last for hours and are not relieved by antacids. Certain foods can precipitate the pain. He also complains of occasional diarrhea. The patient has lost 10 pounds over the last 6 months. Four years ago he was hospitalized for three days with acute abdominal pain. He smokes one pack of cigarettes a day and consumes alcohol regularly. His family history is significant for diabetes mellitus in his mother and prostate cancer in his father. Which of the following is most likely to diagnose this patient's condition?
D -xylose absorption test
Serum amylase and lipase
Radioisotope (HIDA) scans
CA 19-9 and CEA levels
Stool elastase
54) A 50-year-old woman comes to clinic due to several episodes of severe watery diarrhea for the past 15 days. There is 4/10 pain all over her abdomen but she has not noticed any blood in her stools. She has normal diet and has not travelled anywhere recently. She denies any one around her having similar complaints. She also had occasional cramps in her leg muscles and feels dehydrated. She smokes one to two cigarettes a day and drinks socially. Her temperature is 36.8°C (98.1°F), blood pressure is 108/64 mmHg, pulse is 118/min, and respirations are 18/min. On examination her abdomen is slightly tender. Laboratory results are as follows. WBC 5600mm3, Hemoglobin 13.6, Hematocrit: 41%, Platelets 209,000mm3, Sodium 138mEq/L, Potassium: 2.1mEq/L, Bicarbonate: 35mEq/L, Blood urea nitrogen: 16 mg/dl, Creatinine: 0.8 mg/dl, Glucose 106 mg/dl. A CT abdomen is ordered which shows a mass in the head of pancreas. What is the most probable diagnosis?
Pancreatic adenocarcinoma
Glucagonoma
Insulinoma
VIPoma
Gastrinoma
55) An 83-year-old woman presents with a 1-year history of progressively severe crampy abdominal pain after eating. She has started avoiding food because of the pain. The pain is often associated with bloating, nausea, and occasional diarrhea. She has had a 15 kg (33 lb) weight loss over the past year. Her other medical problems include hypertension, diabetes mellitus-type 2, hypercholesterolemia, peripheral vascular disease, coronary artery disease and myocardial infarction. Social history is not significant. Abdomen is soft, nontender and non-distended. Abdominal x-ray and CT scan are unremarkable. Which of the following is the most likely diagnosis?
Chronic pancreatitis
Atherosclerosis of the mesenteric arteries
Crohn' s disease
Irritable bowel syndrome
Celiac disease
56) A 65-year-old woman presents with painless intermittent rectal bleeding. The bleeding is bright red in color. She does not have abdominal pain, nausea, or vomiting. She has a history of hypertension, diabetes mellitus, and hypercholesterolemia. Her temperature is 36.7°C (98° F), blood pressure is 140/80 mmHg, pulse is 80/min, and respirations are 16/min. Physical examination shows a systolic ejection murmur in the right second intercostal space; examination is otherwise unremarkable. Sigmoidoscopy shows no abnormalities. Which of the following is the most likely diagnosis?
Vascular ectasia
Diverticulosis
Ischemic colitis
Carcinoma colon
Hemorrhoids
57) A 45-year-old white male comes to your office for evaluation of diarrhea of 8-months duration. He says that he has lost almost 15 lbs during the past 8 months. He denies any blood in the stools. 24-hour stool collection reveals fecal fat of 10 gm/day. Stool microscopy reveals no pathogens and no leucocytes. D-xylose test was performed which shows that less than 2 grams of D-xylose is excreted in urine in 5 hours. D-xylose test was re-performed after 4-week treatment with antibiotics but excretion is still less than 2 grams in 5 hours. Based on these findings, what is the most likely diagnosis in this patient?
Lactose intolerance
Bacterial overgrowth
Pancreatic insufficiency
Celiac disease
Terminal ileal disease
58) A 27-year-old male presents with a history of intermittent abdominal distention, flatulence and greasy stools. He also complains of fatigue. He has no other medical problems. His family history is unremarkable. He does not use tobacco, alcohol or smoking. His vital signs are within normal limits. Physical examination shows a pruritic, papulovesicular rash over the extensor surfaces of the extremities and over the trunk, scalp and neck. His abdomen is soft, nontender and non-distended. Stool for occult blood testing is negative. Lab studies show: Hemoglobin 10.0 g/L, MCV 75 fl, Platelets 340,000/mm3, Leukocyte count 4,500/mm3, Neutrophils 56%, Eosinophils 1%, Lymphocytes 33%, Monocytes 10%. Which of the following is the most likely diagnosis of his skin condition?
Guttate psoriasis
Dermatitis herpetiformis
Pityriasis rose a
Seborrheic dermatitis
Bullous pemphigoid
59) A 49-year-old woman presents with a two-week history of lower abdominal pain and severe diarrhea. The stools are watery without blood or mucus. The abdominal pain is mild and unrelated to her stools. She has had recent episodes of flushing. She has not had fever. There is no history of travel. She does not smoke or drink alcohol. Her past surgical history includes a fracture repair of her right leg 3 years ago. Her temperature is 36.6°C (97.8°F), blood pressure is 106/68 mm Hg, pulse is 103/min, and respirations are 20/min. Oxygen saturation is 99% on room air. Physical examination shows facial flushing, a prominent jugular venous pulse and expiratory wheezes. Which of the following is the most likely diagnosis?
Diverticulitis
Infectious gastroenteritis
Inflammatory bowel disease
Carcinoid syndrome
Irritable bowel syndrome
60) A 55-year-old male comes to the physician with a history of diarrhea, weight loss, bloating, and excessive flatulence. His symptoms began soon after having "stomach surgery" two years ago. He has a history of gastric ulcers. Physical examination shows scarring associated with past surgery, and abdominal distention with identifiable succussion splash. Laboratory studies show anemia with MCV of 100fl. Which of the following is the most likely diagnosis?
Short bowel syndrome
Bacterial overgrowth
Peptic ulcer disease
Crohn's disease
Ulcerative colitis
61) A 50-year-old female presents with a 3-year history of abdominal pain and diarrhea. She has not been evaluated by a physician. Recently, her symptoms have been progressively worsening. Endoscopy shows multiple ulcerations of the duodenum and prominent gastric folds. Secretin stimulation test shows increased gastrin secretion. Which of the following is most likely associated with this patient's condition?
Medullary thyroid cancer
Pheochromocytoma
Primary hyperparathyroidism
Neuromas
Marfanoid habitus
62) A 27-year-old Caucasian woman presents with abdominal pain, diarrhea and a 4.5 (2kg) weight loss for the past two months. She describes the abdominal pain as intermittent, moderate-to-severe, and located in the right lower quadrant. Over the past 48 hours, the pain has intensified. Her temperature is 37.6°C (99.6°F), blood pressure is 120/70 mm Hg, pulse is 100/min, and respirations are 14/min. Several shallow ulcers are present in her mouth. Abdominal examination shows tenderness in the right lower quadrant without rebound. Rectal examination shows mucus. Rectosigmoidoscopy is unremarkable. An x-ray film of the abdomen shows gas in the small and large bowels. Laboratory studies show: Hb 10.2 g/dL, WBC 16,500/cmm, Platelet count 530,000/cmm, ESR 48/hr. Which of the following is the most likely diagnosis?
Diverticulitis
Celiac disease
Irritable bowel syndrome
Crohn's disease
Ulcerative colitis
63) A 65-year-old man treated for heart failure with enalapril and digoxin presents to the emergency department (ED) with palpitations. His blood pressure is 160/100 mmHg, and heart rate is 110/min. His rhythm is irregular. His lungs are clear on auscultation. His abdomen is soft and non-distended. Mild epigastric tenderness is elicited on deep palpation. ECG shows atrial fibrillation without acute ischemic changes. Cardiac enzyme levels are normal. Treatment with warfarin and verapamil is initiated, and the patient is eventually discharged home. After two weeks, he returns to the ED to complain of profound anorexia. Which of the following is the most likely cause of his current complaint?
Gastric irritation
Pancreatitis
Drug interaction
Occult carcinoma
Gastrointestinal bleeding
64) A 52-year-old Caucasian male comes to you for a routine health check-up. You decide to do age-appropriate screening in this patient and order a colonoscopy. The colonoscopy is normal, except for a 1.5cm polyp in the left descending colon. A colonoscopic polypectomy is done and the biopsy results are pending. The patient is anxious to know the expected biopsy results and the risk of cancer. Which of the following types of polyps is considered to be most premalignant?
Hamartomatous polyp
Hyperplastic polyp
Villous adenoma
Tubulovillous adenoma
Tubular adenoma
65) A 50-year-old white male comes to the physician's office because of diarrhea, abdominal pain and weight loss. He has bulky, foul-smelling stools, abdominal distension and flatulence. He also has arthralgias and a chronic cough. His temperature is 37.8°C (100°F), blood pressure is 120/80 mm Hg, pulse is 80/min, and respirations are 18/min. Physical examination shows generalized lymphadenopathy, skin hyperpigmentation and a diastolic murmur in the aortic area. Small bowel biopsy shows villous atrophy with numerous PAS-positive materials in the lamina propria. Which of the following is the most likely diagnosis?
Celiac disease
Tropical sprue
Crohn's disease
Whipple's disease
Cystic fibrosis
66) A 27-year-old male returning home after a three-month visit to Puerto Rico presents with diarrhea for the past 6 weeks. Other accompanying symptoms include cramps, gas, fatigue and progressive weight loss. Abdominal auscultation shows hyperactive bowel sounds, and borborygmi. The family history is unremarkable for intestinal disease. Laboratory studies show anemia with a hematocrit of 25% and MCV of 105fl; stool examination for ova and parasites is negative. Small intestinal mucosal biopsy shows blunting of villi with infiltration of chronic inflammatory cells, including lymphocytes, plasma cells, and eosinophils. Which of the following is the most likely diagnosis?
Celiac disease
Amoebiasis
Tropical sprue
Bacterial overgrowth
Giardiasis
67) A 37-year-old male prisoner has been complaining of fever, chills and abdominal pain over the last week. He vomited once before reaching the emergency room. On physical examination, his blood pressure is 112/63 mmHg and his heart rate is 115/min. Breath sounds are diminished at the left lung base and there is marked left upper quadrant tenderness. Laboratory values are given below:WBC count 23,500/mm3, Neutrophils 65%, Bands 11%, Hemoglobin 12.5 mg/dL, Platelets 250,000/mm3, Total bilirubin 3.1 mg/dL, AST 46 units/L, AL T 70 units/L, Alkaline phosphatase 120 units/L. CT scan of the abdomen reveals a fluid collection within the spleen. Which of the following is the most likely diagnosis?
Functional asplenia
Infectious endocarditis
Inflammatory bowel disease
Portal hypertension
Infectious mononucleosis
68) A 40-year-old female presents with a 12-month history of episodes of chest pain and dysphagia. The episodes last from a few seconds to a few minutes. She has not had weight loss, fevers or chills. Chest-x ray, ECG and barium swallow show no abnormalities. Manometric studies show simultaneous high amplitude contractions with normal relaxation of the lower esophageal sphincter. Which of the following is the most likely diagnosis?
Zenker's diverticulum
Diffuse esophageal spasm
Achalasia
Scleroderma
Infectious esophagitis
69) A 29-year-old man presents to the ED complaining of RLQ pain for 24 hours. He states that the pain first began as a dull feeling around his umbilicus and slowly migrated to his right side. He has no appetite, is nauseated, and vomited twice. His BP is 130/75 mm Hg, HR is 95 beats per minute, temperature is 100.9°F, and his RR is 16 breaths per minute. His WBC is 14,000/μL. As you palpate the LLQ of the patient’s abdomen, he states that his RLQ is painful. What is the name of this sign?
Blumberg sign
Psoas sign
Obturator sign
Raynaud sign
Rovsing sign
70) A 55-year-old man with hypertension and end-stage renal disease requiring hemodialysis presents with 2 days of painless hematochezia. He reports similar episodes of bleeding in the past, which were attributed to angiodysplasia. He denies abdominal pain, nausea, vomiting, diarrhea, and fever. His vitals include HR of 90 beats per minute, BP of 145/95 mm Hg, RR of 18 breaths per minute, and temperature of 98°F. His abdomen is soft and nontender and his stool is grossly positive for blood. Which of the following statements are true regarding angiodysplasia?
They are responsible for over 50% of acute lower GI bleeding
They are more common in younger patients
Angiography is the most sensitive method for identifying angiodysplasias
They are less common in patients with end-stage renal disease
The majority of angiodysplasias are located on the right side of the colon
71) A 70-year-old woman presents to the ED with dark stool for 3 weeks. She occasionally notes bright red blood mixed with the stool. Review of systems is positive for decreased appetite, constipation, and a 10-lb weight loss over 2 months. She denies abdominal pain, nausea, vomiting, and fever, but feels increased weakness and fatigue. She also describes a raspy cough with white sputum production over the previous 2 weeks. Examination reveals she is pale, with a supine BP of 115/60 mm Hg and HR of 90 beats per minute. Standing BP is 100/50 mm Hg, with a pulse of 105 beats per minute. Which of the following is the most likely diagnosis? .
Hemorrhoids
Diverticulitis
Mallory-Weiss tear
Diverticulosis
Adenocarcinoma
72) A 52-year-old man has episodes of severe chest pain associated with dysphagia. He has been seen twice in the emergency room, and both times the symptoms responded to sub-lingual nitroglycerin. He then had a full cardiac evaluation including electrocardiogram (ECG), cardiac biomarkers, and an exercise stress test, which were all normal. Which of the following is the most likely diagnosis?
herpetic infection
a motor disorder
midesophageal cancer
peptic stricture
external esophageal compression
73) A 16-year old girl has recently been referred to your family practice. She is a recent immigrant from Southeast Asia, and has been taking isoniazid (INH) and rifampin for uncomplicated tuberculosis. Routine blood tests are unremarkable, except for an elevated direct bilirubin. Other liver enzymes and function tests are completely normal. Which of the following is the most likely diagnosis?
hemolytic anemia
INH toxicity
Crigler-Najjar syndrome type I
rifampin toxicity
Rotor’s syndrome
74) A 78-year-old woman is brought to the ED by EMS complaining of vomiting and abdominal pain that began during the night. EMS reports that her BP is 90/50 mm Hg, HR is 110 beats per minute, temperature is 101.2°F, and RR is 18 breaths per minute. After giving her a 500 mL bolus of NS, her BP is 115/70 mm Hg. During the examination, you notice that her face and chest appear jaundiced. Her lungs are clear to auscultation and you do not appreciate a murmur on cardiac examination. She winces when you palpate her RUQ. An ultrasound reveals dilation of the common bile duct and stones in the gallbladder. What is the most likely diagnosis?
Cholecystitis
Acute hepatitis
Cholangitis
Pancreatic cancer
Bowel obstruction
75) A 62-year-old man with a history of hypertension presents to the ED with severe constant mid-epigastric pain for the past hour. Over the last several months, he has had intermittent pain shortly after eating, but never this severe. He states he now has generalized abdominal pain that began suddenly about 15 minutes ago. He has no history of trauma, has never had surgery, and takes no medications. His vitals include HR of 115 beats per minute lying supine, increasing to 135 when sitting up, BP of 170/105 mm Hg supine, falling to 145/85 mm Hg when sitting up. He appears pale. His abdomen is rigid and diffusely tender with guarding and rebound. Bowel sounds are absent and stool hemoccult is positive. The white blood cell (WBC) count is 8500/μL, hemoglobin 8.5 mg/dL, hematocrit 27%, and platelets 255/μL. Which of the following is the most likely diagnosis?
Boerhaave syndrome
Perforated gastric ulcer
Abdominal aortic aneurysm (AAA)
Inflammatory bowel disease (IBD)
Diverticulosis
76) The physician on call is called to the well-baby nursery because a full-term, African-American boy who is 49 hours old has not passed meconium. The pregnancy was uncomplicated. The neonate’s blood pressure is 70/50 mm Hg, heart rate is 140/min, and respiratory rate is 36/ min. The neonate is crying but is easily consolable. His abdomen is markedly distended. A barium enema is ordered, which shows dilated proximal bowel and a narrowed distal segment. Which of the following would provide a definitive diagnosis in this child?
Absent ganglion cells on rectal biopsy
Absent ligament of Treitz on upper gastro- intestinal series
Air bubbles in the stomach and duodenum on x-ray film of the abdomen
Positive sweat test
Telescoping of bowel on air contrast barium enema
77) A pregnant 16-year-old girl with no prior pre-natal care presents to the emergency department in labor. A male infant is delivered precipitously. Prenatal laboratory test results are unknown. There is no meconium. He has a birth weight of 3 kg (6 lb 10 oz). He is pink and is crying, heart rate is 130/min, and respiratory rate is 36/min, with good respiratory effort. The emergency medicine resident notices the infant has ascites and a membrane-covered anterior abdominal mass at the base of his umbilical cord. Which of the following is the most likely diagnosis?
Duodenal atresia
Gastroschisis
Hirschsprung’s disease
Meckel’s diverticulum
Omphalocele
78) A 50-year-old man is brought to the ED by ambulance with significant hematemesis. In the ambulance, paramedics placed two large-bore IVs and began infusing normal saline. In the ED, his HR is 127 beats per minute, BP is 79/45 mm Hg, temperature is 97.9°F, RR is 24 breaths per minute, and oxygen saturation is 96%. On physical examination, his abdomen is nontender, but you note spider angiomata, palmar erythema, and gynecomastia. Laboratory results reveal WBC 9000/μL, hematocrit 28%, platelets 40/μL, aspartate transaminase (AST) 675 U/L, alanine transaminase (ALT) 325 U/L, alkaline phosphatase 95 U/L, total bilirubin 14.4 mg/dL, conjugated bilirubin 12.9 mg/dL, sodium 135 mEq/L, potassium 3.5 mEq/L, chloride 110 mEq/L, bicarbonate 26 mEq/L, blood urea nitrogen (BUN) 20 mg/dL, creatinine 1.1 mg/dL, and glucose 150 mg/dL. Which of the following is the most likely diagnosis?
Perforated gastric ulcer
Diverticulosis
Splenic laceration
Esophageal varices
Ruptured AAA
79) An 81-year-old diabetic woman with a history of atrial fibrillation is transferred to your emergency department (ED) from the local nursing home. The note from the facility states that the patient is complaining of abdominal pain, having already vomited once. Her vital signs in the ED are temperature 100.1°F, blood pressure (BP) 105/75 mm Hg, heart rate (HR) 95 beats per minute, and respiratory rate (RR) 18 breaths per minute. You examine the patient and focus on her abdomen. Considering that the patient has not stopped moaning in pain since arriving to the ED, you are surprised to find that her abdomen is soft on palpation. You decide to order an abdominal radiographic series. Which of the findings on plain abdominal film is strongly suggestive of mesenteric infarction?
Sentinel loop of bowel
No gas in the rectum
Presence of an ileus
Pneumatosis intestinalis
Air fluid levels
80) A 71-year-old obese man is brought to the ED complaining of constant left mid quadrant (LMQ) abdominal pain with radiation into his back. His past medical history is significant for hypertension, peripheral vascular disease, peptic ulcer disease, kidney stones, and gallstones. He smokes a pack of cigarettes and consumes a pint of vodka daily. His BP is 145/80 mm Hg, HR is 90 beats per minute, temperature is 98.9°F, and RR is 16 breaths per minute. Abdominal examination is unremarkable. An ECG is read as sinus rhythm with an HR of 88 beats per minute. An abdominal radiograph reveals normal loops of bowel and curvilinear calcification of the aortic wall. Which of the following is the most likely diagnosis?
Biliary colic
Nephrolithiasis
Pancreatitis
Small bowel obstruction (SBO)
Abdominal aortic aneurysm
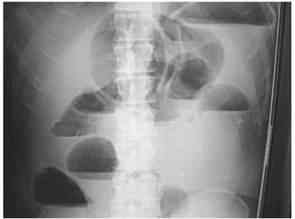
81) A 73-year-old man is seen in the ED for abdominal pain, nausea, and vomiting. His symptoms have progressively worsened over the past 2 to 3 days. The pain is diffuse and comes in waves. He denies fever or chills, but has a history of constipation. He reports no flatus for 24 hours. Physical examination is notable for diffuse tenderness and voluntary guarding. There is no rebound tenderness. An abdominal radiograph is seen below. Which of the following is the most likely diagnosis?
Constipation
SBO
Cholelithiasis
Large bowel obstruction
Inflammatory bowel disease
82) A 63-year-old man is brought to the ED by EMS complaining of severe abdominal pain that began suddenly 6 hours ago. His BP is 145/75 mm Hg and HR is 105 beats per minute and irregular. On examination, you note mild abdominal distention and diffuse abdominal tenderness without guarding. Stool is heme positive. Laboratory results reveal WBC 12,500/μL, haematocrit 48%, and lactate 4.2 U/L. ECG shows atrial fibrillation at a rate of 110. A CT scan is shown below. Which of the following is the most likely diagnosis?
Abdominal aortic aneurysm
Mesenteric ischemia
Diverticulitis
SBO
Crohn disease
83) A 2-year-old boy is brought to the emergency department. His mother reports that the patient had been well until 3 days ago, when he developed a fever and nasal congestion. He was diagnosed with otitis media in his right ear, and was started on amoxicillin with clavulanic acid by his pediatrician. He appeared to be improving until this morning, when he began to complain of abdominal pain. The pain has been intermittent, with episodes occurring every 20 minutes for several minutes each time. However, the episodes appear to be worsening and lasting longer with increasing pain. Thirty minutes ago he had an episode of nonbloody, nonbilious emesis that was followed by passage of blood- and mucus-stained stools. He is currently in no acute distress, and his vital signs are normal. A firm sausage-shaped mass is palpable in the RUQ of his abdomen. A rectal examination yields bloody mucus. He does not have any skin lesions or rashes. X-ray of the abdomen is shown in the image. Which of the following is the most likely diagnosis?

Cystic fibrosis
Enterocolitis
Henoch-Schönlein purpura
Idiopathic intussusception
Meckel’s diverticulum
84) A 23-year-old woman presents to the ED with RLQ pain for the last 1 to 2 days. The pain is associated with nausea, vomiting, diarrhea, anorexia, and a fever of 100.9°F. She also reports dysuria. The patient returned 1 month ago from a trip to Mexico. She is sexually active with one partner but does not use contraception. She denies vaginal bleeding or discharge. Her last menstrual period was approximately 1 month ago. She has a history of pyelonephritis. Based on the principles of emergency medicine, what are the three priority considerations in the diagnosis of this patient?
Perihepatitis, gastroenteritis, cystitis
Ectopic pregnancy, appendicitis, pyelonephritis
Pelvic inflammatory disease (PID), gastroenteritis, cystitis
Ectopic pregnancy, PID, menstrual cramps
Gastroenteritis, amebic dysentery, menstrual cramps
85) A 28-year-old man presents with symptoms of frequent bowel movements, crampy abdominal pain, and the passage of mucus. There is no history of any bloody diarrhea, but recently, he developed joint discomfort in his hands, knees, and back. On examination he is thin, and his abdomen is soft with voluntary guarding in the left lower quadrant. His joints are not actively inflamed and there is an asymmetric distribution. Which of the following is the most likely diagnosis?
lymphoma of the bowel
amyloid infiltration
chronic pancreatitis
ulcerative colitis
tropical sprue
86) A 64-year-old white woman presents to her primary care physician complaining of difficulty and pain with swallowing, as well as occasional chest pain. She has a history of breast cancer treated with lumpectomy and radiation, hyper- tension, high cholesterol, and ovarian polyps. She indicates that her current problem started with liquids, but has progressed to solids, and that the food “just gets stuck in my throat.” The chest pain was once so bad that she took one of her husband’s nitroglycerin pills and the pain subsided, but it has since occurred many times. The physician orders an x-ray of the chest, but it is not diagnostic. Manometry is conducted, and it shows uncoordinated contractions. Which of the following is the most likely diagnosis?
Breast cancer relapse
Diffuse esophageal spasm
Esophageal cancer
Myocardial infarction
Nutcracker esophagus
87) A 22-year-old woman presents with chronic diarrhea. She has no abdominal discomfort, feels well, and reports no weight loss or systemic symptoms. Physical examination reveals a healthy young woman who is 5’7” tall and weighs 150 lb. The complete physical examination is normal. Which of the following is the most likely cause of a secretory diarrhea in this young woman?
surreptitious use of stimulant laxatives
carcinoid tumor
ulcerative colitis
lactose deficiency
celiac disease
88) A full-term 5-day-old African-American girl is taken to the pediatrician because her “eyes look yellow.” She is being exclusively formula- fed with an iron-rich formula. She has six wet diapers a day and stools twice a day. The pregnancy was uncomplicated and she was delivered by spontaneous vaginal delivery. Her Apgar scores were 9 and 10 at 1 and 5 minutes, respectively. Her temperature is 37°C (98.6°F), her head circumference is in the 50th percentile, and her weight is 3420 g (3 g below her birth weight). Her sclerae are icteric. There is no hepatomegaly or splenomegaly. Her total bilirubin is 9 mg/dL and her conjugated bilirubin is 0.2 mg/dL. Hemoglobin is 15 g/dL. Which of the following is the most likely diagnosis?
α1-Antitrypsin deficiency
Biliary atresia
Dubin-Johnson syndrome
Physiologic jaundice
Rotor syndrome
89) A 20-year-old man presents to the ED with fever and severe right lower quadrant (RLQ) pain for 1 day. Prior to this episode, he reports 2 months of crampy abdominal pain, generalized malaise, a 10-lb weight loss, and occasional bloody diarrhea. On examination, his HR is 115 beats per minute, BP is 125/70 mm Hg, RR is 18 breaths per minute, and temperature is 100.8°F. His only significant past medical history is recurrent perirectal abscesses. On physical examination, the patient appears uncomfortable and has a tender mass in the RLQ, without guarding or rebound. Rectal examination is positive for trace heme-positive stool. An abdominal computed tomographic (CT) scan reveals no periappendiceal fat stranding. There is inflammation of the distal ileum and several areas of the colon. There are no rectal inflammatory changes. Which of the following is the most likely diagnosis?
Crohn disease (CD)
Ulcerative colitis (UC)
Appendicitis
Pseudomembranous enterocolitis
Diverticulitis
90) A 55-year-old white woman with a history of iron deficiency anemia has had intermittent trouble swallowing solids for the past few years. She denies alcohol or tobacco use. Her vital signs are stable. Her iron level is 40μg/dL and total iron binding capacity is 500 μg/dL. Other laboratory tests are within normal limits. Which of the following is the most likely diagnosis?
Achalasia
Barrett’s esophagus
Esophageal carcinoma
Mallory-Weiss syndrome
Plummer-Vinson syndrome
91) A 64-year-old woman develops sudden-onset abdominal discomfort after eating a large meal. The pain is constant, localizes to the epigastric area with radiation to her right scapula. She also has nausea and vomiting. It eventual subsides 1 hour later. An ultrasound of the abdomen reveals a dilated common bile duct secondary to stones. Which of the following statements regarding common bile duct stones is most likely true?
all originate in the gallbladder
always produce jaundice
produce constant level of jaundice
can be painless
indicate anomalies of the bile duct
92) A 30-year-old man complains of chronic diarrhea for the past 6 months. There is no weight loss, fever, or abdominal pain. He takes no medications and feels fine. His physical examination is completely normal. Further history reveals that this man does not take laxatives; however, in an effort to stay slim he eats a lot of sugar-free gum and sugarless candy. Which of the following explanations is the most likely cause of his diarrhea?
direct stimulant effect of chemicals in the candies
lack of fiber in his diet
pancreatic insufficiency secondary to chronic protein-calorie malnutrition
secondary intestinal mucosal atrophy
nonabsorbed carbohydrates
93) A 16-year-old girl is referred to the office because of chronic diarrhea and weight loss. She is experiencing large-volume watery diarrhea that is painless. The symptoms persist even when she is fasting, and there is no relationship to foods or liquids. She is not on any medications, and there is no travel history or other constitutional symptoms. Her physical examination is normal. Which of the following is the most likely diagnosis?
partial small bowel obstruction
partial large bowel obstruction
osmotic diarrhea
secretory diarrhea
inflammatory bowel disease
94) A 52-year-old man has suffered with chronic diarrhea for several years, but has refused to see a doctor. He finally comes because he is having trouble driving at night, because of difficulty seeing. Physical examination reveals a slender, pale, unwell-looking man. He has a microcytic anemia, low calcium, and albumin levels. Which of the following is the most likely cause for his diarrhea?
malabsorption
osmotic diarrhea
secretory diarrhea
inflammatory bowel disease
colonic tumor
95) The physician on call is paged to the well-baby nursery because a full-term, 3-hour-old boy has had green emesis twice, once after each of his feedings. He is being breast-fed. He was born by spontaneous vaginal delivery following a pregnancy complicated by polyhydramnios. His Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. His temperature is 37°C (98.6°F), blood pressure is 70/50 mm Hg, pulse is 150/min, and respiratory rate is 24/ min. His upper abdomen is distended, soft, and without palpable masses. Air is visualized in the duodenum and the stomach on x-ray. Which of the following is the most likely diagnosis?
Duodenal atresia
Hirschsprung’s disease
Intussusception
Malrotation with volvulus
Pyloric stenosis
96) A 55-year-old man presents to the ED complaining of mild diffuse abdominal pain. He states that he underwent a routine colonoscopy yesterday and was told “everything is fine.” The pain began upon waking up and is associated with some nausea. He denies fever, vomiting, diarrhea, and rectal bleeding. His BP is 143/71 mm Hg, HR is 87 beats per minute, temperature is 98.9°F, and RR is 16 breaths per minute. His abdomen is tense but only mildly tender. You order baseline laboratory tests. His chest radiograph is seen below. Which of the following is the most likely diagnosis?

Ascending cholangitis
Acute pulmonary edema
Acute liver failure
Pancreatitis
Pneumoperitoneum
97) A 35-year-old White man has a long past history of diarrhea, rectal bleeding, crampy abdominal pain, and the passage of mucus. He now presents with a worsening of his symptoms despite taking his medications. A barium enema is performed and is shown in Fig. Which of the following is the most likely diagnosis of this new complication?

toxic megacolon
amoebic colitis
appendicitis
ischemic colitis
annular carcinoma
98) A 45-year-old man with a long history of alcohol intake comes into the emergency room with upper gastrointestinal (UGI) bleeding. Urgent endoscopy reveals the following findings. Which of the following is the most likely diagnosis?

esophageal varices
esophageal carcinoma
foreign body
tertiary waves
Barrett’s esophagus
99) A 50-year-old woman undergoes screening colonoscopy at her primary care physician’s recommendation. She has no family history of colorectal cancer. A single lesion is removed during the procedure and sent for pathologic examination. Which of the following findings carries the greatest risk of malignancy?
Lymphoid polyp
Peutz-Jeghers polyp
Tubular adenoma
Tubulovillous adenoma
Villous adenoma
100) A 24-year-old woman presents to her primary care provider because of bloody diarrhea for several months and uveitis. Complete blood cell count shows mild anemia but a normal WBC count. The erythrocyte sedimentation rate and the C-reactive protein level are not elevated. Which of the following is the most likely diagnosis?
Bacterial enterocolitis
Bowel ischemia
Colon carcinoma
Mallory-Weiss tear
Ulcerative colitis
101) A 66-year-old woman presents to her physician because of recurrent painless bleeding on defecation over the past month. She has regular, soft bowel movements and no history of constipation or diarrhea. A recent diagnosis of aortic stenosis was an incidental finding on echocardiogram. She takes calcium and vitamin D supplements daily. Her last colonoscopy (at age 60) was normal. Heart rate is 82/min, blood pressure is 133/72 mm Hg, respiratory rate is 12/min, and temperature is 36.6°C (97.8°F). Physical examination reveals her conjunctivae are pink and mucosa is moist. She has no abdominal tenderness or palpable masses and no hemorrhoids or fissures. Stool is hemoccult positive. Colonoscopy shows a spider-like lesion in the ascending colon. Which of the following is the most likely diagnosis?
Angiodysplasia
Crohn’s disease
Diverticulosis
Ischemic colitis
Peptic ulcer disease
102) A 61-year-old woman is brought to the emergency department drowsy and disoriented, able only to follow simple commands. On examination her abdomen is distended and nontender, her skin has a yellow hue, and there are multiple spider nevi on her chest. In her purse, the physician finds prescriptions for peginterferon and ribavirin. When asked to raise her hands, the physician notices a coarse tremor. Laboratory tests show: Blood urea nitrogen: 17 mg/dL Creatinine kinase: 1.1 mg/dL Aspartate aminotransferase: 89 U/L Alanine aminotransferase: 93 U/L Total bilirubin: 3.1 mg/dL Ammonia: 124 μg/dL Which of the following is the most likely diagnosis?
Bleeding esophageal varices
Hepatic encephalopathy
Hepatocellular carcinoma
Hepatorenal syndrome
Spontaneous bacterial peritonitis
103) A 74-year-old man presents to the emergency department with abdominal pain. The pain is deep and aching and is localized to the left lower quadrant. The man reports multiple episodes of diarrhea over the preceding week. He also reports having multiple similar episodes of abdominal pain in the past. On physical examination he is febrile and has tenderness to palpation of the left lower quadrant. His WBC count is 23,000/mm³. Results of CT are shown in the image. Which of the following is the most likely diagnosis?

Angiodysplasia
Carcinoid syndrome
Carcinoma of the colon
Diverticulitis
Infectious colitis
104) A 51-year-old man describes 1 week of gradually worsening scrotal pain and dysuria. He is sexually active with his wife. His temperature is 100.1°F, HR 81 beats per minute, BP 140/75 mm Hg, and oxygen saturation is 99% on room air. On physical examination, his scrotal skin is warm and erythematous. A cremasteric reflex is present. The posterior left testicle is swollen and tender to touch. Color Doppler ultrasonography demonstrates increased testicular blood flow. Urinalysis is positive for leukocyte esterase. What is the most likely diagnosis?
Epididymitis
Testicular torsion
UTI
Testicular tumor
Varicocele
105) A 40-year-old woman presents to the ED complaining of fever and 1 day of increasingly severe pain in her RUQ. She denies nausea or vomiting and has no history of fatty food intolerance. The patient returned from a trip to Mexico 6 months ago. About 2 weeks ago she experienced intermittent diarrhea with blood-streaked mucus. Her BP is 130/80 mm Hg, HR is 107 beats per minute, temperature is 102°F, and RR is 17 breaths per minute. Physical examination reveals decreased breath sounds over the right lung base. Abdominal examination shows tenderness to percussion over the RUQ and normal active bowel sounds. There is no Murphy sign. Her WBC is 20,500/μL. Chest radiograph reveals a small right-pleural effusion. Which of the following is the most likely diagnosis?
Amebic abscess
Cholecystitis
Cryptosporidium
Enterobiasis
Pyogenic abscess
106) A 20-year-old man presents with several weeks of painful rectal bleeding. He denies fever, nausea, or vomiting. He is sexually active with women only and usually uses condoms. He denies any history of CD, UC, or malignancy. He states that the pain is most severe during and immediately after defecating. Bleeding is bright red and only enough to stain the toilet paper. Which of the following is the most common etiology of painful rectal bleeding?
External hemorrhoid
Anal fissure
Anorectal tumor
Internal hemorrhoid
Venereal proctitis
107) A premature newborn is being treated in the neonatal intensive care unit. On the sixth day of life he is noted to be lethargic and in mild respiratory distress. His heart rate is 162/min, blood pressure is 55/38 mm Hg, and respiratory rate is 56/min. In addition to a distended abdomen, he has guaiac-positive stools. X-ray of the abdomen shows gas bubbles within the bowel wall. From what potentially life-threatening condition is this patient most likely suffering?
Bowel obstruction
Intussusception
Meconium ileus
Meningitis
Necrotizing enterocolitis
108) A 65-year-old man comes to the emergency department complaining of left lower abdominal pain that began the prior morning. He became concerned when he developed bloody diarrhea overnight. He has experienced similar pain, although to a lesser degree, over the past 2 months, especially after eating. The pain usually resolved within 1–2 hours, and he never had bloody diarrhea. His past medical history is significant for coronary artery disease and hypertension. He has smoked one pack of cigarettes per day for the past 30 years. On physical examination he is afebrile, heart rate is 90/min, and blood pressure is 135/85 mm Hg. He is visibly uncomfortable but in no apparent distress. His abdominal examination is significant for left lower quadrant tenderness but no guarding or rebound. Which of the following is the most likely diagnosis?
Acute mesenteric ischemia
Colon cancer
Diverticulitis
Infectious colitis
Inflammatory bowel disease
109) A 25-year-old previously healthy man experiences fatigue and malaise. One week ago he had a “viral” type illness consisting of a sore throat, fever, and myalgias. He now appears jaundiced, but the rest of the physical examination is normal. His investigations reveal a total bilirubin of 4 mg/dL (0.1–1.0 mg/dL) and a direct bilirubin of 0.3 mg/dL (0.0–0.3 mg/dL). Which of the following is the most likely diagnosis?
hemolysis
gallstones
alcoholic liver disease
pancreatic carcinoma
Dubin-Johnson syndrome
110) A 49-year-old man is brought to the ED by EMS stating that he vomited approximately three cups of blood over the last 2 hours. He also complains of epigastric pain. While examining the patient, he has another episode of hematemesis. You decide to place an NG tube. You insert the tube, confirm its placement, and attach it to suction. You retrieve 200 mL of coffee-ground blood. What is the most common etiology of an upper GI bleed?
Varices
Peptic ulcer
Gastric erosions
Mallory-Weiss tear
Esophagitis
111) A 63-year-old woman with cirrhosis caused by chronic hepatitis C is hospitalized because of confusion. She has guaiac-positive stools and a low-grade fever. She has received lorazepam for sleep disturbance. On physical examination, the patient is confused. She has no meningeal signs and no focal neurologic findings. There is hyperreflexia and a nonrhythmic flapping tremor of the wrists. Which of the following is the most likely explanation for this patient’s mental status change?
Tuberculous meningitis
Subdural hematoma
Alcohol withdrawal seizure
Hepatic encephalopathy
Central nervous system vasculitis from cryoglobulinemia
112) A 40-year-old white male complains of weakness, weight loss, and abdominal pain. On examination, the patient has diffuse hyperpigmentation and a palpable liver edge. Polyarthritis of the wrists and hips is also noted. Fasting blood sugar is 185 mg/dL. Which of the following is the most likely diagnosis?
Insulin-dependent diabetes mellitus
Pancreatic carcinoma
Addison disease
Hemochromatosis
Metabolic syndrome
113) A 55-year-old white woman has had recurrent episodes of alcoholinduced pancreatitis. Despite abstinence, the patient develops postprandial abdominal pain, bloating, weight loss despite good appetite, and bulky, foul-smelling stools. KUB shows pancreatic calcifications. In this patient, you should expect to find which of the following?
Diabetes mellitus
Malabsorption of fat-soluble vitamins D and K
Guaiac-positive stool
Courvoisier sign
Markedly elevated amylase
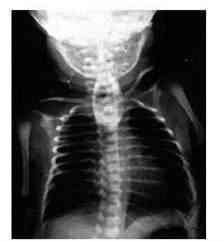
114) A male infant is delivered at 37 weeks’ gestation via cesarean section for breech presentation. The pregnancy was complicated by polyhydramnios. The 34-year-old mother is rubella immune and has blood type B. She is negative for Rh antibody, Group B streptococci, rapid plasma reagin, hepatitis B surface antigen, gonorrhea, and Chlamydia. At delivery there is no meconium. He has a birth weight of 2.7 kg (6 lb). The baby has a weak cry and is pale and frothing at the nose and mouth. He has nasal flaring and retractions, with a respiratory rate of 56/min. Heart rate is 140/min and he has a regular rhythm and a harsh 2/6 holosystolic murmur that is best heard at the left sternal border. On auscultation he has fine diffuse crackles in his lungs bilaterally. The infant is missing both thumbs and has fusion of the remaining digits of his upper extremities bilaterally. The pediatric resident is able to suction secretions from the patient’s nasopharynx and oropharynx; however, she is unable to pass a nasogastric or orogastric tube more than 10 cm down. X-ray of the chest is shown in the image. Which of the following is the most likely diagnosis?
Congenital diaphragmatic hernia
Pyloric stenosis
Respiratory distress syndrome
Tracheoesophageal fistula
Transient tachypnea of the new-born
115) A 55-year-old male comes to you with complaint of fatigue for the past month. He also complains of occasional heartburn. His past medical history is significant for hepatomegaly, secondary to fatty liver. He has been drinking 3-4 shots of alcohol per day for the past 30 years. He denies smoking. His physical examination reveals pallor of skin and mucous membranes, and mild hepatomegaly. His laboratory report shows: Hb 8.5 g/dl, WBC 8,000/cmm, MCV 110 fl, Platelets 150,000/cmm, Blood glucose 118 mg/dl, BUN 16 mg/dl, Serum creatinine 1.0 mg/dl. What is the most likely cause of anemia in this patient?
Vitamin B- 12 deficiency
Folate deficiency
Chronic blood loss from peptic ulcer
Anemia of chronic disease
Thiamine deficiency
116) A 62-year-old Caucasian man presents to your office with occasional ear pain and a lump in his neck. His past medical history is significant for hypertension treated with hydrochlorothiazide and diabetes mellitus treated with metformin. He smokes two packs of cigarettes per day and consumes alcohol occasionally. He is not sexually active. Physical examination reveals a hard, non-tender submandibular mass that is 3 cm in diameter. Chest examination is unremarkable. Abdomen is soft and non-tender. The liver span is 8 cm and the spleen is not palpable. His extremities have no cyanosis, clubbing, or edema. Complete blood count is within normal limits. Which of the following is the most likely cause of this patient's complaint?
Bacterial infection
Squamous cell carcinoma
Herpes simplex infection
Connective tissue disease
Hodgkin's lymphoma
117) A 67-year-old woman comes to her physician because she is feeling tired, all the time. She thinks that it is due to multiple surgeries she had over the past several years. She had two caesarian sections at the age of 22 and 26. She also had a thyroid surgery for Graves’s disease, 30 years ago. 12 years ago she was diagnosed with colon cancer and had undergone left hemicolectomy. She denies smoking or alcohol use. Her vitals are Temperature 36.7°C (98.2°F); BP 138/86 mm Hg; PR 77/min; RR 12/min. She looks markedly pale and has weakness in all four extremities. There is some sensory loss in lower limbs. The test for occult blood was negative. Labs came back as: Sodium 144 mEq/L, Potassium 4.2 mEq/L, Bicarbonate 24mEq/L, Blood urea nitrogen 18mg/dl, Creatinine 1.0 mg/dl, Glucose 82 mg/dl, WBC 8,600/cmm, Hemoglobin 7.9, Hematocrit 25%, Platelets 176,000/cmm. The physician decides to further investigate anemia and order RBC indices and peripheral blood smear. The results are: MCV 120 fl, MCH 36 pg, MCHC 28%, Reticulocyte count 04%. Peripheral smear showed anisocytosis, poikilocytosis, 4+ macrocytes, polychromatophilia and basophilic stippling. A whole new bunch of tests are ordered and the following report is seen on the computer. Vitamin B12 106 pg/ml (N=210-911 pg/ml), Serum Folate 16.4 ng/ml (N=2.8-17.8 ng/ml), Serum Bilirubin 1.8 mg/dl, Serum LDH 2500 U/L. Gastric analysis demonstrated an absence of hydrochloric acid. What is the most probable cause of her anemia?
Folate deficiency
Dietary B12 deficiency
Pernicious anemia
Hemicolectomy
Malabsorption syndrome
118) A 34-year-old Caucasian man presents to your office with easy fatigability, difficulty concentrating, insomnia, and occasional muscle pain. He also complains of right hand clumsiness and some memory loss. He does not smoke and drinks one to two cans of beer on the weekends. Physical examination reveals extensor weakness of the right hand. Ankle reflexes are symmetric and there is no Babinski reflex. Laboratory studies show: Hemoglobin 8.5 g/dl, MCV 81 fl, AST 18 U/L, ALT 16 U/L, Bilirubin 0.8 mg/dl, Creatinine 2.1 mg/dl. Which of the following is most important in revealing the cause of this patient's condition?
Vaccination history
Family history
Occupational history
Nutrition
Childhood infections
119) A 26-year-old woman presents to your office complaining of fatigue. Her past medical history is insignificant. She was adopted in Greece and came to the United States when she was three years old. Her menstrual periods are regular and bleeding lasts three days. She does not use tobacco, alcohol, or illicit drugs. She takes no medication. Laboratory studies show: Complete blood count: Hemoglobin 10.1 g/L, MCHC 28%, MCV 70 fL, Platelets 200,000/mm3, Leukocyte count 7,500/mm3, Neutrophils 56%, Eosinophils 1%, Lymphocytes 33%, Monocytes 10%. Fecal occult blood test is negative. Iron therapy is initiated. When the patient returns four weeks later, her lab findings are essentially the same. This patient most likely suffers from:
Iron deficiency
Folic acid deficiency
Cobalamin deficiency
Erythropoietin deficiency
Hemoglobinopathy
120) An 8-month-old pale child is referred by a nurse practitioner due to "pale mucous membranes, irritability, and listlessness." The stool examination is negative for occult blood, ova and parasites. Laboratory studies reveal: Hemoglobin 6.0 g/L, MCHC 25%, MCH 16.5 pg, MCV 68 fl, Reticulocytes 0.6%, Platelets 230,000/mm3, Leukocyte count 5,500/mm3, Neutrophils 56%, Eosinophils 1%, Lymphocytes 33%, Monocytes 10%, Serum Iron 40 mg/dL, TIBC 460 mg/dL (normal 300-350 mg/dL), Percent saturation of transferrin 8.7%, Total serum bilirubin 0.9 mg/dL. The peripheral blood smear shows marked anisocytosis, microcytosis, hypochromia, and poikilocytosis. Which of the following is the most likely diagnosis?
Iron deficiency anemia
Sideroblastic anemia
Dimorphic anemia
Megaloblastic anemia
Anemia of chronic disease
121) A 54-year-old Caucasian man presents to his family physician's office complaining of several months of increased fatigability. He eats meat occasionally and drinks two to three cans of beer on weekends. Physical examination reveals pale conjunctivae and hyperdynamic carotid pulses. His blood hemoglobin level is 7.7 mg/dl, WBC count is 4,500/mm3, and platelet count is 170,000/mm3 Folic acid therapy is initiated. Four weeks later the patient's hemoglobin level is 9.1 mg/dl, but he complains of new tingling in his toes. Which of the following is a likely cause of this patient's current symptoms?
Drug toxicity
Iron deficiency
Vitamin deficiency
Glucose intolerance
Extramedullary hematopoiesis
122) A 46-year-old bank executive is referred to the clinic by her dentist. For the past 6 weeks, she has had swollen, bleeding gums. She appears pale and feels weak. She smokes half a pack of cigarettes daily and drinks alcohol socially. Her family history is not significant. Her vital signs are stable. She is afebrile. WBC 44,100 mm3, Hemoglobin 9.0 g/dL, Hematocrit 27%, Platelets 16,000/mm3. Leukocyte distribution: Blast forms 79%, Promonocytes 12%, Monocytes 8%, Lymphocytes 1%. Cytochemical analysis:Sudan black: slightly positive, Alpha-naphthyl esterase: positive, PAS reaction: negative. Which of the following is the most likely diagnosis?
AML with maturation
Acute promyelocytic leukemia
Acute lymphoblastic leukemia
Acute erythroleukemia
Acute monocytic leukemia
123) A 65-year-old woman is being evaluated for "generalized depression." She has felt weak and fatigued ever since her husband died 4 months ago. She does not have any suicidal thoughts, but is losing interest in her daily activities. She quit smoking 24 years ago, and drinks 1-2 beers weekly. Physical examination reveals pallor and cervical lymphadenopathy. Blood work reveals: Hemoglobin 12.0 g/L, MCV 85 fl, Platelets 224,000/mm3, Leukocyte count 54,500/mm3, Neutrophils 16%, Lymphocytes 75%, Monocytes 9%. Some variants of lymphocytes and smudge cells are present. Which of the following is the most likely diagnosis?
Lymphoblastic leukemia
Hodgkin's disease
Chronic lymphocytic leukemia
Chronic myeloid leukemia
Hairy cell leukemia
124) A 54-year-old male is brought to the emergency department because of severe abdominal pain and diarrhea for the past 24 hours. He is confused and crying out in pain. His temperature is 38.6°C (101.6°F), blood pressure is 82/58 mm Hg, pulse is 118/min, and respirations are 24/min. Physical examination reveals extensive abdominal distention. There is fresh blood in his stools. Intravenous administration of normal saline is started after drawing blood for the necessary laboratory tests. The results of these tests are: Sodium 136 mEq/L, Potassium 3.6 mEq/L, Bicarbonate 18 mEq/L, Blood urea nitrogen 32 mg/dL, Creatinine 1.3 mg/dL, Glucose 86 mg/dL, WBC 35,000/mm3, Hemoglobin 13.0 g/dL, Hematocrit 36%, Platelets 460,000/mm3. Leukocyte distribution:Promyelocyte 2%, Myelocytes 7%, Metamyelocytes 18%, Bands 32%, Segmented neutrophils 24%, Lymphocytes 15%. The patient's temperature continues to remain elevated during the night of admission. A broad-spectrum antibiotic is added to the IV infusion. Repeat CBC on the following morning shows a WBC count of 118,000/mm3 with essentially the same differential distribution of leukocytes. His leukocyte alkaline phosphatase score is elevated. What is the most probable diagnosis of this patient?
CML with blast crisis
Chronic lymphocytic leukemia
Leukemoid reaction
Secondary polycythemia
Myelodysplastic syndrome
125) A 25-year-old African American man presents to your office complaining of nocturia over the past several months. He reports having to wake to urinate 2 to 3 times per night despite restricting his fluid intake. He denies any back pain, fever, dysuria, or urinary urgency. His past medical history is significant for recurrent otitis media in childhood and hepatitis A infection two years ago. He is sexually active with one partner and does not use condoms. His brother died of a "blood disease" at age 10. The man's hematocrit is 49%. Urinalysis reveals no proteinuria or sediment abnormalities. His nocturia is most likely related to:
Childhood infections
Nephrolithiasis
Sexual history
Family history
Glomerular pathology
126) A 25-year-old African American male comes to the office with sudden-onset back pain, dark urine and an one day history of fatigue. Two days ago, he was started on trimethoprim-sulfamethoxazole for his sinusitis. Otherwise, his past medical history is unremarkable. Physical examination reveals significant pallor. His laboratory report shows: Hb 7.5 g/dl, Total bilirubin 3.5 mg/dl, Direct bilirubin 0.8 mg/dl, Haptoglobin decreased, LDH increased. The peripheral smear shows bite cells. His G6PD level is normal. Which of the following is the most likely cause of his hemolysis?
G6PD deficiency
Pyruvate kinase deficiency
Galactokinase deficiency
Sickle cell disease
Mechanic trauma
127) A 75-year-old Caucasian male comes to the office for his routine medical check-up. He complains of fatigue for the past month. His previous medical history is significant for calcified aortic valves and hypertension. His vital signs are stable; except for a blood pressure of 150/90 mm Hg. Physical examination reveals pallor and a 4+ ejection systolic murmur in the aortic area. Lab reports show: Hb 9 g/dl, MCV 75 fl, Reticulocyte count increased, Serum LDH increased, Haptoglobin decreased, Peripheral smear fragmented RBC. Which of the following is the most likely cause of this patient's anemia?
Bleeding peptic ulcer
Diverticulosis
Macrovascular traumatic hemolysis
Warm antibody hemolysis
G6PD deficiency anemia
128) A 68-year-old unconscious man is brought to the emergency department by a hospice nurse. He had seizures 2 hours ago, after which he lost consciousness. The hospice staff responded by securing his airway and giving him 2L of oxygen. He is in hospice for terminal care for stage IV esophageal carcinoma. He also had a part of his finger removed 1.5 years ago due to a skin cancer. His pulse oximetry reading is 91%. His temperature is 37.9°C (100.2°F), respirations are 23/min, pulse is 96/min, and blood pressure is 140/85 mmHg. He does not respond to painful stimuli. Rectal examination reveals a hard, irregular surface of an enlarged prostate. His recent prostate specific antigen level is 40. MRI shows an intracranial lesion with bleeding inside, and these findings are consistent with metastasis. What is the most likely diagnosis?
Metastatic prostatic carcinoma
Glioblastoma multiforme
Metastatic melanoma
Metastatic squamous cell carcinoma of the skin
Metastatic esophageal carcinoma
129) A 44-year-old woman comes to the office with complaints of weight loss and blood in her stools for the last year. Her mother is on chemotherapy for colon carcinoma. Her maternal uncle also had colon cancer, as did her first cousin who died of colon cancer at the age of 46. She is very worried that she might have the same cancer. Based on her history, she falls within the criteria for Lynch syndrome (also known as HNPCC/ Hereditary Nonpolyposis Colorectal Cancer). Apart from the complete work-up for colon cancer, this patient should be evaluated for which of the following condition?
Pancreatic carcinoma
Hepatic carcinoma
Pseudomembranous colitis
Diverticulitis
Endometrial carcinoma
130) A 72-year-old Hispanic man comes to the clinic with complaints of mild headache and lethargy for the past several days. He complains of cough for the past 12 years but, has been bothering him more lately. The cough is mucoid in nature. He has noticed blood in it once in a while. He has been smoking 1 pack/day for 29 years. His Temperature 37C (98.6F); BP 120/84 mmHg; PR 78/min; RR 24/min. On examination of the lungs, adventitious sounds are heard in all the lobes and scant basilar crackles. Laboratory studies show: WBC 7,600/mm3, Hemoglobin 13.6, Hematocrit 40%, Platelets 214,000/mm3, Sodium 131 mEq/L, Potassium 3.6 mEq/L, Bicarbonate 18 mEq/L, Blood urea nitrogen 16 mg/dL, Creatinine 0.6 mg/dL, Glucose 95 mg/dL, Serum osmolality 260 mOsm/kg (275-295 mosm/kg H2O), Urine osmolality 310 mOsm/kg (38-1400 mosm/kg H2O). A chest x-ray shows a 2-centimeter left upper lobe nodule and mediastinal adenopathy your diagnosis is?
Chronic obstructive pulmonary disease
Squamous cell carcinoma
Large cell carcinoma
Small cell carcinoma
Adenocarcinoma
131) A 63-year-old Caucasian man reports occasional palpitations when exercising. He denies chest pain. Past medical history includes coronary artery disease status post coronary artery stenting, mitral valve replacement with mechanical valve, and diabetes mellitus. He consumes a well-balanced diet and takes one multivitamin tablet daily. His medications include warfarin, simvastatin, metoprolol, lisinopril, and metformin. Physical examination reveals conjunctival pallor and heart sounds consistent with the presence of a mechanical mitral valve. His hematocrit is 30%. The peripheral blood smear shows occasional schistocytes and his serum LDH level is elevated. His stool is negative for occult blood. Which of the following is the most likely cause of this patient's anemia?
Iron deficiency
Folate deficiency
Traumatic hemolysis
Glucose-6-phosphate dehydrogenase deficiency
Autoimmune hemolysis
132) An 80-year-old female is brought to your office, by her son, because of severe fatigue. She lives alone and is suffering from severe degenerative joint disease, which puts her in a house arrest-type state. Her son usually helps with getting grocery. Her only other medical problem is hypertension. She takes hydrochlorothiazide and acetaminophen. Her vitals are stable. On examination, she has pallor, and evidence of severe degenerative joint disease. Which of the following is the most likely cause of pallor in this patient?
Vitamin D deficiency
Vitamin C deficiency
Iron deficiency
Folate deficiency
Chronic hemolysis
133) A 56-year-old white male comes to the office for a health maintenance visit. He feels healthy, and is "enjoying life as much as possible in a stressed environment." He smokes 2-3 packs of cigarettes daily and drinks socially. His temperature is 37°C (98.6°F), blood pressure is 160/94 mm Hg, pulse is 78/min, and respirations are 14/min. Physical examination reveals plethora of the face and moderate splenomegaly. Blood tests show the following: WBC 15,600/mm3, Hemoglobin 17 gm/dl, Hematocrit 52%, Platelets 550,000mm3, RBC count 7.5 million, Sodium 141 mEq/L, Potassium 3.6 mEq/L, Bicarbonate 22 mEq/L, Blood urea nitrogen 16 mg/dl, Creatinine 0.6 mg/dl, Glucose 95 mg/dl. The erythrocyte indices are all within normal range. What is the most probable diagnosis?
Idiopathic hypertension
Cushing syndrome
Polycythemia vera
Congestive heart failure
Primary hyperaldosteronism
134) A 49-year-old woman comes to the office and complains of a "strange, itchy rash" on her left areola which has been present for the last month. She tried applying various lotions and creams, but the lesion did not resolve. She denies having other skin conditions, except for a poison ivy rash 2 months ago. She does not take any medications and feels "goofy" when she takes penicillin. Physical examination reveals an eczemoid lesion on the left nipple. No abnormality is visible on the mammogram. Biopsy demonstrates large cells surrounded by halo-like areas which invade the epidermis. What is the most likely diagnosis?
Adenoma of nipple
Scirrhous carcinoma
Paget's disease
Phyllodes tumor
Lymphocytic carcinoma of breast
135) A 41-year-old fire-fighter comes to your office and requests for prostate cancer screening. He is concerned because his elder brother was recently diagnosed with prostate cancer, and he read in the paper that "cancers run in families." He requests to be screened urgently, as he "cannot even think of life with such a deadly disease." He has no medical complaints. He has been your patient for the past 6 years, and has no other medical history. He is on a very balanced diet, and adds that he eats a lot of garlic "so that cholesterol remains in check." He takes a low-dose aspirin daily. He does not smoke, and is only a social drinker. He admits using marijuana "once in a while” What is the best next step to address this patient's concerns?
Transurethral ultrasonogram
Bone scan
T ransrectal ultrasonogram
Perform digital rectal examination
Needle biopsy
136) A 27-year-old male presents with dyspnea and fatigue. He has no family history of asthma, heart disease or any blood disorder. His vital signs are stable, and he is afebrile. The only significant findings on examination are pallor and splenomegaly. Lab studies show: Hematocrit 20%, WBC count 4,000/micro-L, Platelet count 85,000/miro-L, Bilirubin 7 mg/dl, Direct bilirubin 1.2 mg/dl, Serum LDH 500 U/L (normal value is 80-280 U/L), Serum haptoglobin 20mg/dl (normal value is 30-220 mg/dl). Peripheral blood smear shows microcytic hypochromic cells. Serum ferritin is low while total iron binding capacity (TIBC) is elevated. Reticulocyte count is 5 %. Urine dipstick testing is positive for hematuria and microscopy of urine shows 1 RBC/HPF. Repeated G6PD assays are normal. Coomb's and micro-Coomb's tests are negative. Bone marrow examination shows hypocellular marrow. Based on these findings, what is the most likely diagnosis?
Aplastic anemia
G6PD deficiency
Hereditary spherocytosis
Autoimmune hemolytic anemia
Paroxysmal nocturnal hemoglobinuria
137) A 44-year-old man who comes to the office because he has had several episodes of hemoptysis for the past two months. He admits to smoking 2-3 packs of cigarettes daily for the last 24 years. Physical examination and chest x-ray are very suggestive of a lung malignancy. Chest CT and bronchoscopy with biopsy are done, and the patient goes on vacation in Aruba. The patient returns to the office after one week, and you are now holding the biopsy result in your hands. It reads, "The tumor has spread to the hilar and mediastinal lymph nodes with bony extension." Which of the following is the most appropriate opening statement?
"How much would you like to know about your condition?"
"I am sorry to tell you that you have lung cancer and it is fairly advanced."
. "What do you think of your symptoms?"
"Unfortunately, the situation is more serious than what I earlier thought."
"Would you like to have someone else with you as I don't have good news for you?"
138) A 25-year-old male presents to his physician with dyspnea and fatigue for the last few weeks. He is a non-smoker. He denies any family history of asthma or blood disorders. He does not take any medications. Examination shows pallor, scleral icterus and splenomegaly. Lab tests show the following: Hematocrit 20%, WBC count 10,000/micro-L, Platelet count 180,000/miro-L, Total Bilirubin 7 mg/dl, Direct bilirubin 1 A mg/dl, BUN 10 mg/dl, Serum creatinine 0.7 mg/dl, Serum LDH 400 U/L (normal value is 80-280 U/L), Serum haptoglobin 160mg/dl (normal value is 30-220 mg/dl ), Reticulocyte count 8 %. Peripheral blood smear shows spherocytes with central pallor. Osmotic fragility and direct Coombs' tests are positive Based on these findings, what is the most likely diagnosis?
Hereditary spherocytosis
Autoimmune hemolytic anemia
Paroxysmal nocturnal hemoglobinuria
Sickle cell anemia
G6PD deficiency
139) A 10-year-old white boy is brought to the office by his foster parents for the evaluation of severe pain in his left knee for the last few days. His left knee has been hurting so bad that he is now unable to play with his peers. The pain is continuous and non-radiating. His knee appears swollen, but he denies any history of trauma. His family history is unknown. His vital signs are stable. Physical examination reveals a pale young boy. The left knee is tender, erythematous and swollen. Blood tests reveal: WBC 12,600/mm3, Hemoglobin 9.3 g/dl, Hematocrit 29%, Platelets 201,000/mm3, ESR 40. X-ray of the knee reveals that the lower end of the femur has a central lytic lesion, onion skinning and a moth-eaten appearance with some extension into the soft tissue. What is the most likely diagnosis?
Osteomylitis
Ewings sarcoma
Chondrosarcoma
Glomus tumor
Fibrosarcoma
140) A 56-year-old woman is complaining of cough for the past 4 months. The cough was dry initially, but only yesterday she was scared-to-death to see phlegm with blood. She is not feeling well and thinks that she has lost "a lot of weight" recently, despite no apparent change in her diet. She swears that she has never smoked a cigarette in her life. There is no history of night sweats nor contact with any person with similar complaints. She is a housewife who rarely drinks, and can't think of using recreational drugs. She is completely faithful to her husband. Her husband is also a "religious non-smoker". Her vitals are stable and lung examination reveals no significant findings. Her chest x-ray shows 1.5cm lesion in the right peripheral lung field and no evidence of any hilar or mediastinal lymph node enlargement. What is the most probable diagnosis?
Tuberculosis
Sarcoidosis
Small cell carcinoma of lung
Squamous cell carcinoma of lung
Adenocarcinoma of lung
141) A 74-year-old immigrant from Colombia comes to the office and complains of having "all sorts of problems of old age." He has pain all over his body. He often has headaches and feels dizzy. He has visual problems, and finds it difficult to walk. For the last several weeks, he has been feeling weak and numb in his feet. He lives with his son, and is not happy with the way his son treats him; however, he denies receiving any form of physical abuse. His past medical history is unremarkable. His mother had "some blood disease." His vital signs are stable. Physical examination reveals multiple bruises on his body, and sensory deficits in his feet. Other significant findings include lymphadenopathy and hepatosplenomegaly. Ophthalmoscopy shows dilated, segmented, and tortuous retinal veins. Laboratory studies show: WBC 10,200 /mm3, Hemoglobin 9.6 g/dl, Hematocrit 29%, Platelets 94,000 /mm3, Sodium 141 mEq/L, Potassium 3.6 mEq/L, Blood urea nitrogen 18 mg/dl, Creatinine 0.8 mg/dl, Glucose 115 mg/dl. Serum protein electrophoresis reveals an lgM spike. Which of the following is the most likely diagnosis in this patient?
Multiple myeloma
Waldenstrom's macroglobulinemia
Monoclonal gammopathy of undetermined significance
Elderly abuse
Heavy chain disease
142) A 25-year-old white female presents to the clinic with persisting pain in her wrists and ankles for the last 3 months. The pain is 3/10 in intensity, and partially relieved by ibuprofen. She also has a rash on her face. She denies smoking, and drinks alcohol occasionally. Her temperature is 37.3°C (99.2°F), blood pressure is 120/80 mm Hg, pulse is 79/min, and respirations are 18/min. Physical examination reveals swollen joints of the hands and ankle, as well as erythema over the bridge of the nose and the upper cheeks. There is no muscle weakness. Labs show: Hemoglobin 11.0 g/dL, Hematocrit 33%, Platelets 240,000/mm3, WBC 13,600/mm3. Leukocyte distribution:Segmented neutrophils 76%, Lymphocytes 20%, Bands 2%, Monocytes 2%. RF, ANA, and antibodies to double stranded-DNA are positive in high titers. What is the most likely diagnosis?
Scleroderma
Systemic lupus erythematosus
Dermatomyositis
Polymyositis
Mixed connective tissue disease
{"name":"Part 3 \"510-764\" Na IV (638-678)", "url":"https://www.quiz-maker.com/QDR31G9","txt":"44) A 65-year-old man comes to the physician's office with a 2-month history of dysphagia. He initially had difficulty swallowing solids, but now this includes liquids. He has occasional heartburn, which usually responds well to antacids. He has lost 20 lbs of weight in the past 2 months. He has a 40 pack- year history of smoking. He has been a chronic alcoholic for 20 years. His temperature is 36.7°C (98°F), blood pressure is 110\/80 mmHg, pulse is 66\/min, and respirations are 14\/min. Physical examination shows no abnormalities. Barium studies show a minimally dilated esophagus with beak-shaped narrowing. Manometry shows increased lower esophageal sphincter tone. Which of the following is the most likely diagnosis?, 45) Ms. Lee, a 62-year-old Chinese woman, comes with yellowness in her eyes for the past 6 weeks. She is generally feeling tired, has lost some weight, and occasionally had some nausea. She denies any altered bowel habits. She is a non-smoker but drinks 2-3 beers each night. Her dad is suffering from high cholesterol and also has had stroke. She had a dilatation and curettage for an abnormal pap smear 15 years ago. Her vitals are stable and she is afebrile. She has marked scleral icterus. An abdominal examination reveals normal bowel sounds and no organomegaly. Her stools were occult blood negative. Her liver function tests and enzymes were ordered and the results are: Total protein 6.1 g\/dl, Albumin 39 g\/dl, AST 67U\/L, ALT 52U\/L, Alkaline phosphatase 290 U\/L, Total bilirubin 96 mg\/dl, Direct bilirubin 89 mg\/dl, Serum lipase is 46 U\/L, Anti-mitochondrial antibodies negative. Which of the following is the most likely cause of these findings?, 46) A 64-year-old white male with a history of severe stable angina and peripheral vascular disease undergoes coronary artery bypass surgery. His post-operative course is complicated by hypotension, which is treated successfully; however, a few hours later, he experiences abdominal pain followed by bloody diarrhea. His temperature is 37.8°C (100°F), blood pressure is 110\/60 mmHg, pulse is 110\/min, and respirations are 20\/min. Abdominal examination is benign. Laboratory studies show a WBC count of 15,000\/cmm with 7% bands. The lactic acid level is elevated. A CT scan is ordered. Which of the following areas of the colon will most likely show abnormal findings?","img":"https://www.quiz-maker.com/3012/images/ogquiz.png"}