
Part 25(158)
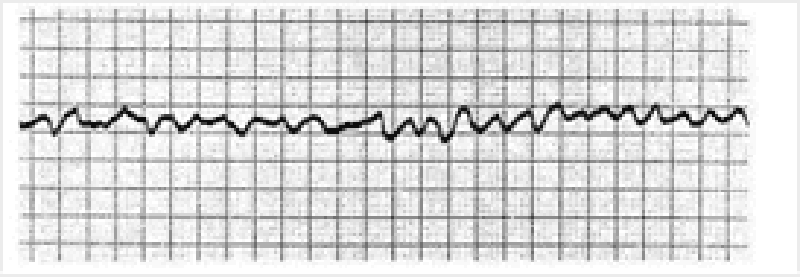
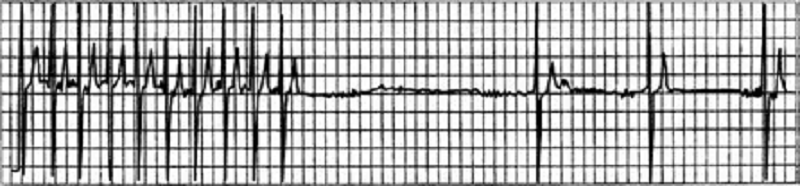
1) A 72-year-old female is admitted to the ICU with severe chest pain. The initial set of cardiac enzymes is positive and her EKG reveals an anterior wall myocardial infarction. She receives treatment with aspirin clopidogrel, metoprolol nitroglycerine drip, and morphine. Two hours later, her telemetry monitor displays the following rhythm. Which of the following is the best next step in managing this patient?
Lidocaine
Immediate echocardiogram
Defibrillation
Digoxin
Amiodarone

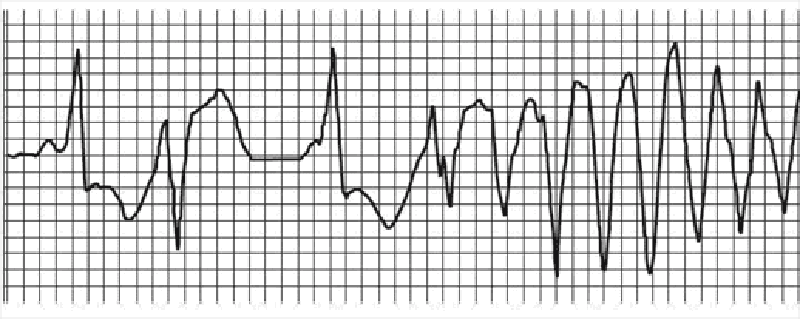
2) A 46-year-old man collapsed while getting out of his bed. He has been feeling weak over the last several days and has complained of vague chest discomfort. He ascribed the symptoms to a recent respiratory infection and did not visit a doctor. His mother died of a stroke and his father suffered from recurrent myocardial infarctions. He eats a balanced diet and takes a multivitamin daily. His most recent blood cholesterol level was 200 mg/dl. An ECG strip taken by EMS is shown below. Which of the following is the best initial management of this patient?
Procainamide
Beta-blockers and aspirin
Synchronized DC cardioversion
Pericardiocentesis
3) A 67-year-old Caucasian male is hospitalized in the intensive care unit (ICU) with an episode of prolonged hypotension and shortness of breath. His skin is cold and clammy. Intra-arterial blood pressure monitoring is established, and pulmonary artery catheterization is performed to control basic hemodynamic parameters. His blood pressure is 70/40 mmHg, and heart rate is 100/min. Cardiac output (CO) measured by thermodilution method is 2.3 L/min. Pulmonary capillary wedge pressure (PCWP) is estimated to be 22 mmHg. Systemic vascular resistance (SVR) calculated using data on mean arterial pressure, right atrial pressure and cardiac output is 2000 dynes*s/cm5 (N= 700 -1200 dynes*s/cm5). Which of the following is the most likely underlying problem in this patient?
Cardiogenic shock
Right ventricular infarction
Volume depletion
Septic shock
Volume overload
4) A 59-year-old man comes to visit his friend in the hospital and collapses in the parking lot. He had been feeling unwell all day due to vague chest discomfort. A bystander witnesses his collapse, finds no pulse, and immediately calls for help. Which of the following is the most important factor for survival in this patient?
Time to chest compressions
Time to cardiac catheterization lab
Time to defibrillation
Time to endotracheal intubation
Time to epinephrine injection
5) A 59-year-old male presents to the ER with sudden onset severe chest pain associated with vomiting and diaphoresis. The pain radiates to the left shoulder and is not relieved by sublingual nitroglycerine. His past medical history is significant for diabetes mellitus for seven years and hypercholesterolemia for six years. His medications include metformin, glipizide and simvastatin. On physical examination, his blood pressure is 150/98 mmHg and pulse is 86/min. An EKG obtained in the ER shows ST segment elevations in leads aVL and I. Cardiac troponin and CK-MB are elevated. Which of the following medications should be avoided in this patient at this time?
Heparin
Heparin
Nifedipine
Metoprolol
Aspirin

6) A 69-year-old male undergoes coronary artery bypass and aortic valve replacement surgery. The procedure goes well, and he is extubated and discharged to the step-down unit on postoperative day 2. That night, he complains of weakness, chest tightness and shortness of breath. His blood pressure is 70/30 mmHg, respiratory rate is 26/min, and heart rate is 148 beats per minute. Lung auscultation reveals bibasilar crackles. An EKG rhythm strip is obtained. Which of the following is the best next step in the management of this patient?
Amiodarone
Digoxin
Transcutaneous pacing
DC cardioversion
Lidocaine

7) A 66-year-old male is rushed to the emergency department because he feels dizzy and light-headed. He denies chest pain or palpitations. He has a history of hypertension and diabetes. His blood pressure is 116/62 mmHg and his pulse is 35-40/min. He is alert, awake, and fully oriented. He is breathing comfortably and does not appear to be in any distress. His extremities are slightly cold and capillary refill is 3 seconds. His EKG is shown below. Which of the following is the most appropriate next step in management?
Intravenous adenosine push
Transcutaneous pacing
Intravenous atropine
Intravenous epinephrine
Intravenous amiodarone
8) A 68-year-old male was intubated in the emergency room because of pulmonary edema. Stat echocardiogram reveals an ejection fraction of 45% and severe mitral regurgitation. In spite of aggressive diuresis with furosemide, the patient continues to require mechanical ventilation secondary to pulmonary edema. What is the best next step in treating this patient?
Arrange for mitral valve replacement surgery
Place an intra-aortic balloon pump
Begin metoprolol
Begin a second loop diuretic
Begin intravenous enalapril
9) A 45-year-old male is brought to the ER with sudden onset palpitations and chest tightness. His past medical history is significant for hypertension, gout and diabetes mellitus. Cardiac monitoring shows atrial fibrillation at a rate of 120-140/min. As the nurse is attempting to establish IV access, the patient becomes unresponsive. There is no palpable pulse over the carotids or femoral arteries. The cardiac monitor still shows atrial fibrillation at the same rate. What is the best next step in management?
Synchronized cardioversion
Arterial blood gas analysis
Defibrillation
IV lidocaine
Chest compressions
10) A 64-year-old male presents to the emergency department with chest pain. An ECG reveals ST elevations in leads II, III, and aVF. Thrombolytic therapy and heparin are administered, and the pain resolves. Eight hours after admission, the patient develops hypotension. He denies recurrence of chest pain. His temperature is 37.5°C (99.6°F), blood pressure is 84/55 mm Hg, pulse is 90/min, and respirations are 15/min. His medications include a nitroglycerin drip, beta-blocker, aspirin, heparin, and simvastatin. Examination reveals an elevated jugular venous pressure of 14 cm, cold clammy extremities, and clear lung fields. Based on this information, what is the next best step in this patient's management?
Start dopamine
Administer intravenous furosemide
Administer normal saline bolus and stop nitroglycerin
Administer intravenous furosemide
Stop nitroglycerin and start dobutamine drip
11) Neighbors find a 65-year-old male unconscious in his garden and immediately call EMS. The man is intubated at the scene. In the ER, he develops sustained ventricular tachycardia and requires cardioversion. He is started on an antiarrhythmic agent and, once recovered, is discharged to home. Three months later he returns to his physician complaining of dyspnea on exertion. Chest x-ray reveals bilateral lung fibrosis. All cultures are negative and lung biopsy reveals lipoid pneumonitis. Which of the following medications is most likely responsible for his current condition?
Procainamide
Digoxin
Amiodarone
Lidocaine
Quinidine
12) A 36-year-old female presents to the emergency room complaining of chest pain that started suddenly while she was shopping at the mall. She also reports shortness of breath, palpitations and diaphoresis. The pain is retrosternal and radiates to the left arm. There are no aggravating or relieving factors. On review of systems, the patient reports having had a runny nose, sore throat and dry cough for the past 3 days. Her past medical history is significant for panic attacks, for which she takes paroxetine, and dysfunctional uterine bleeding, for which she takes estrogen. Her family history is significant for the sudden death of her father at age 44 from a heart attack. Social history reveals that she has smoked one pack of cigarettes per day for the past 15 years. Which of the following is the most appropriate initial therapy for this patient?
Lorazepam
Acetaminophen
Heparin
Aspirin
Ibuprofen
13) A 21-year-old man comes to the ER with palpitations and dizziness that began suddenly one hour ago. He notes having similar past episodes provoked by fatigue or strong emotions. He says he can usually stop the episodes by putting his head into cold water or squatting and taking a deep breath. However, these techniques are not working this time. Presently, his blood pressure is 60/30 mmHg and his heart rate is 240/min. He is diaphoretic with cold extremities. An EKG rhythm strip shows a regular, narrow complex tachycardia. Which of the following is the best next step in managing his condition?
Adenosine
DC cardioversion
Procainamide
Verapamil
Digoxin
14) A 64-year-old Caucasian male presents to the Emergency Room with a sharp, left-sided chest pain. He says that the pain is worse when he takes deep breaths, but he gets relief with leaning forward. He had an acute non-ST elevation myocardial infarction six months ago and had undergone angioplasty for the right coronary artery. His other medical problems include: diabetes, hypertension, hyperlipidemia, peripheral neuropathy, diabetic retinopathy, paroxysmal atrial fibrillation, hypothyroidism, and chronic renal insufficiency. His vital signs are BP 142/86 mmHg, PR 78/min, RR 16/min, and T 36.1°C (97°F). On examination, you find a pericardial rub. EKG shows diffuse ST elevation. Lab results are: Hb 9.0 g/dl, WBC 8,000/cmm, Platelets 210,000/cmm, Blood Glucose 248 mg/dl, Serum Na 135 mEq/L, Serum K 5.8 mEq/L, Bicarbonate 17 mEq/L, BUN 86 mg/dl, Serum Creatinine 4.4 mg/dl. Which of the following is the most appropriate management of this patient?
NSAIDs
Hemodialysis
Corticosteroids
Pericardiocentesis
Hemodialysis
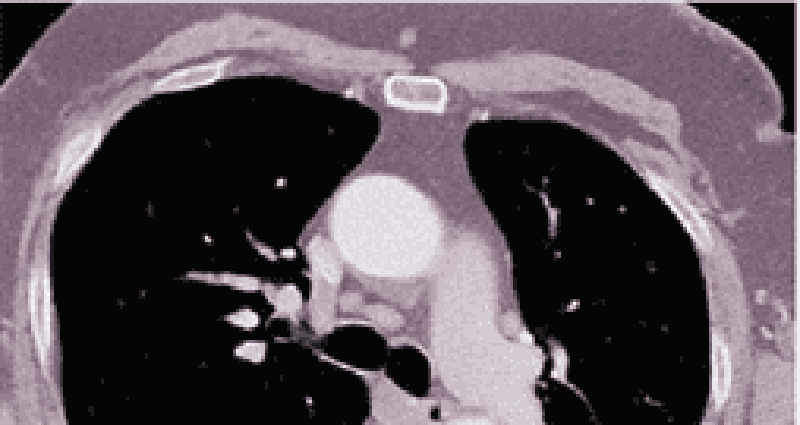
15) A 48-year-old African American man presents to the emergency room with severe retrosternal chest pain. His temperature is 36.7°C (98°F), blood pressure is 190/ 100 mmHg, pulse is 100/min, and respirations are 16/min. On physical examination, his lungs are clear to auscultation and his heart sounds are normal. EKG shows evidence of left ventricular hypertrophy. A CT image of his chest is shown below. Which of the following is the most appropriate immediate pharmacotherapy for this patient?
Labetalol
Hydralazine
Nifedipine
Heparin
Hydrochlorothiazide

16) A 64-year-old male is admitted in ICU for acute myocardial infarction. He is on metoprolol, lisinopril, aspirin, furosemide, and potassium supplements. All of a sudden, the nurse mentions that the patient has a change in his tele monitoring. His blood pressure is 120/60 mmHg. His potassium level is 4.2. He is alert, awake and oriented time, place and person. Examination shows scattered bilateral crackles, peripheral pedal edema and elevated JVI. Which of the following is the next best step in the management of this patient?
IV amiodarone
Carotid massage
IV digoxin
Cardioversion
IV diltiazem
17) A 56-year-old man presents to the emergency department with dyspnea. He describes waking up during the night with difficulty breathing and chest pain that kept him from falling back to sleep. He has never had these symptoms before. His past medical history is significant for long-standing hypertension and non-compliance with his antihypertensive therapy. He has smoked a pack of cigarettes per day for the past 30 years. On physical examination, his blood pressure is 170/100 mmHg and his heart rate is 120/min and regular. Lung auscultation reveals bibasilar rales and scattered wheezes. Which of the following is most likely to relieve this patient's dyspnea?
Metoprolol
Hydralazine
Nitroglycerin
Dopamine
Amiodarone
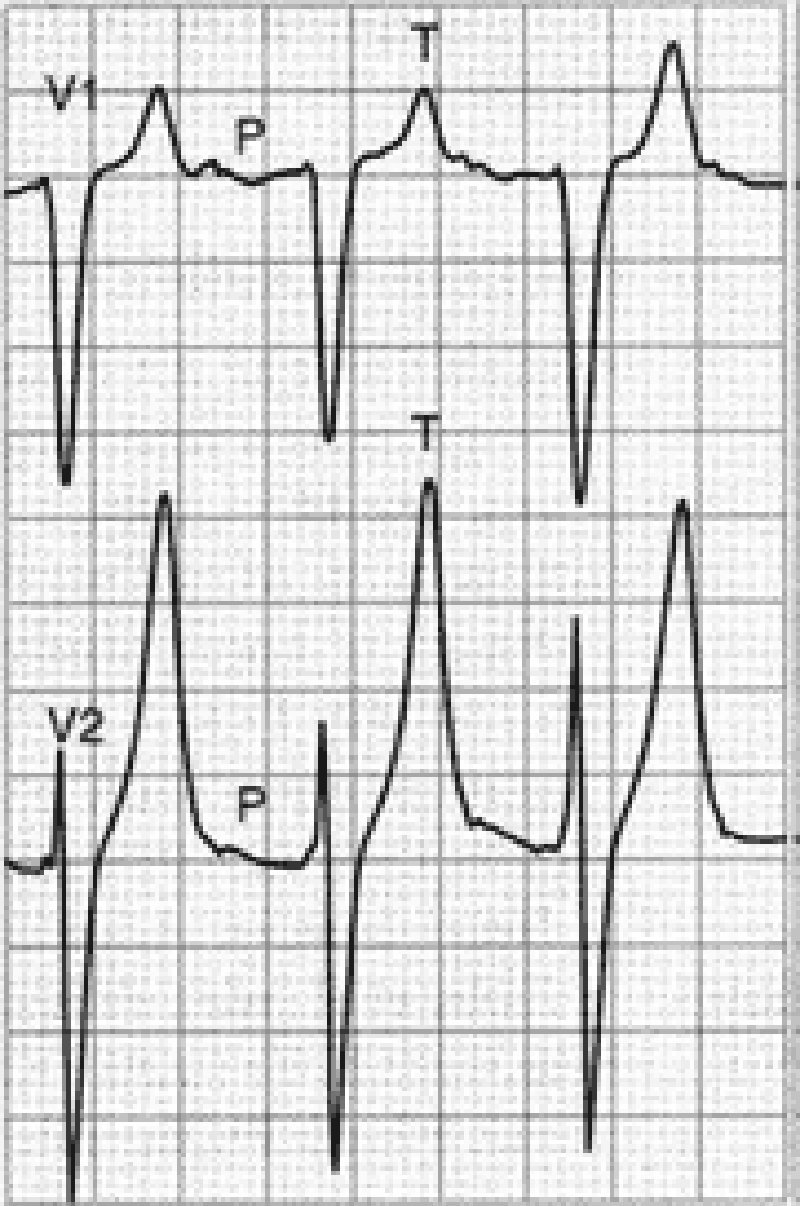
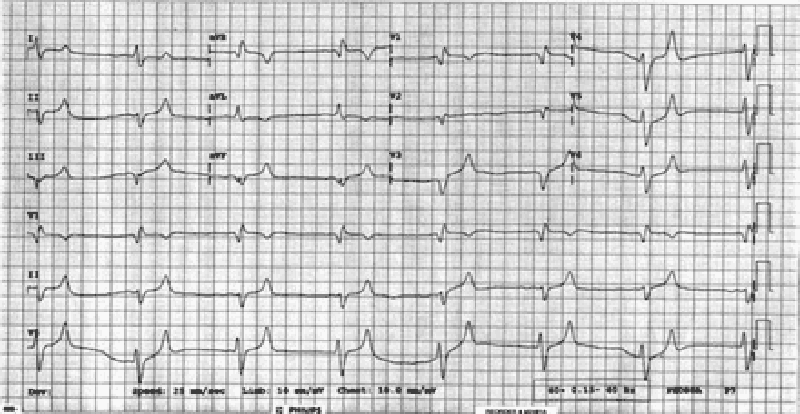
18) A 70-year-old male with a history of mild chronic kidney disease, diabetes mellitus, and CHF is admitted to your inpatient service with decreased urine output, weakness, and shortness of breath. He takes several medications but cannot remember their names. Labs are pending; his ECG is shown below. Based on the information available, what is the best initial step in management?
Administration of intravenous insulin
Administration of oral sodium polystyrene sulfonate
Administration of intravenous sodium bicarbonate
Administration of intravenous 3% hypertonic saline
Administration of intravenous calcium gluconate
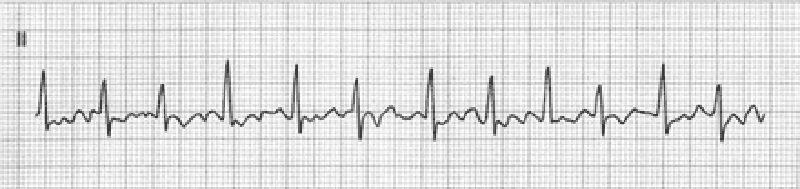
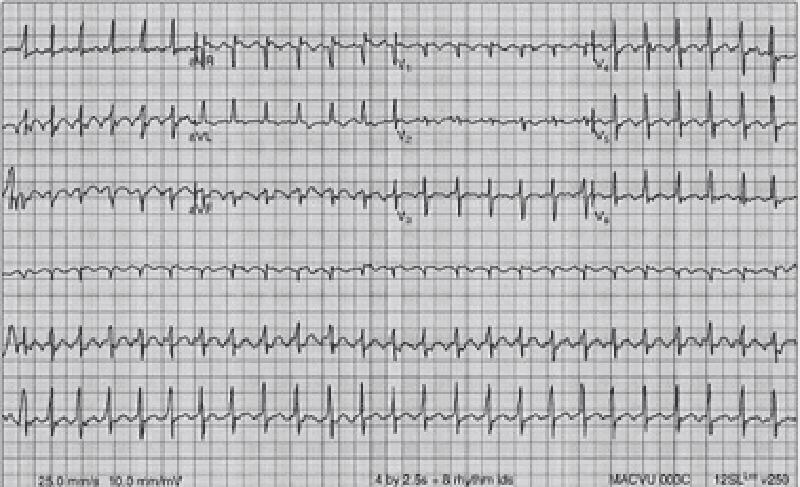
19) A 51-year-old man with a long history of hypertension presents to the ED complaining of intermittent chest palpitations lasting for a week. He denies chest pain, shortness of breath, nausea, and vomiting. He recalls feeling similar episodes of palpitations a few months ago but they resolved. His blood pressure (BP) is 130/75 mmHg, heart rate (HR) is 130 beats per minute, respiratory rate (RR) is 16 breaths per minute, and oxygen saturation is 99% on room air. An ECG is seen below. Which of the following is the most appropriate next step in management?
Sedate patient for immediate synchronized cardioversion with 100 J
Administer warfarin
Prepare patient for the cardiac catheterization laboratory
Administer amiodarone
Administer diltiazem
20) An 82-year-old white female is admitted to the hospital for observation after presenting to the emergency department with dizziness. After being placed on a cardiac monitor in the ER, the rhythm strip below was recorded. There is no past history of cardiac disease, diabetes, or hypertension. With prompting, the patient discloses several prior episodes of transient dizziness and one episode of brief syncope in the past. Physical examination is unremarkable. Which of the following is the best plan of care?
Reassurance. This is a benign condition, and no direct therapy is needed
Nuclear cardiac stress testing; treatment depending on results
. Reassurance. The patient may not drive until she is symptom free, but otherwise no direct therapy is needed
Begin therapy with aspirin
Arrange placement of a permanent pacemaker
21) A 48-year-old man presents to the emergency department complaining of crushing substernal chest pain. He is diaphoretic, anxious, and dyspneic. His pulse is 110/min, blood pressure is 175/112 mmHg, respiratory rate is 30/min, and oxygen saturation is 94%. Aspirin, oxygen, sublingual nitroglycerin, and morphine are given, but they do not relieve his pain. ECG shows ST-segment elevation in leads V2 to V4. The duration of symptoms is now approximately 30 minutes. What is the most appropriate treatment for this patient at this time?
Calcium channel blocker
Tissue plasminogen activator
Intravenous angiotensin-converting enzyme inhibitor
Intravenous β-blocker
Magnesium sulfate
22) A 70-year-old woman presents to the emergency department complaining of dizziness. She is disoriented to the date and her location and it is difficult to gather an accurate history. Her pulse is 48/min, blood pressure is 84/60 mmHg, and respiratory rate is 12/min. On examination her extremities are cool and clammy. Her capillary refill time is 5 seconds. What is the most appropriate therapy?
Adenosine
Metoprolol
Amiodarone
Atropine
Isoproterenol
23) A 64-year-old man in the surgical intensive care unit goes into rapid atrial fibrillation on postoperative day one after a decortication for a loculated pulmonary empyema. He is given an appropriate loading dose of digoxin, but 4 hours after his second dose, the patient complains of increased palpitations and dizziness. The patient is conscious and hemodynamically stable. STAT serum blood tests show a potassium level of 5.0 mEq/L; all other electrolytes, including divalents, are in the normal range. The digitalis level is above the therapeutic range at 4 ng/mL (therapeutic range 0.5-2 ng/mL). Results of cardiac telemetry are shown in the image. Which of the following should be administered immediately?
Calcium
Sodium polystyrene sulfonate
Furosemide
Magnesium
Potassium
24) A 49-year-old man presents to the clinic for a health maintenance visit. He has no complaints, but he requests a prescription for his “pressure pills,” as he lost his original prescription. On physical examination his blood pressure is 220/130 mmHg. Physical examination is otherwise within normal limits. Laboratory tests show: Na+: 142 mEq/L, K+: 3.8 mEq/L, Cl−: 105 mEq/L, Carbon dioxide: 25 mEq/L, Blood urea nitrogen: 20 mg/dL, Creatinine: 1.0 mg/dL, Glucose: 133 mg/dL. Urinalysis is within normal limits, and his ECG is normal. Which of the following is the most effective management?
24) A 49-year-old man presents to the clinic for a health maintenance visit. He has no complaints, but he requests a prescription for his “pressure pills,” as he lost his original prescription. On physical examination his blood pressure is 220/130 mmHg. Physical examination is otherwise within normal limits. Laboratory tests show: Na+: 142 mEq/L, K+: 3.8 mEq/L, Cl−: 105 mEq/L, Carbon dioxide: 25 mEq/L, Blood urea nitrogen: 20 mg/dL, Creatinine: 1.0 mg/dL, Glucose: 133 mg/dL. Urinalysis is within normal limits, and his ECG is normal. Which of the following is the most effective management?
Administer oral furosemide for management of hypertensive emergency
Administer intravenous nitroprusside for management of hypertensive urgency
Administer oral metoprolol for management of hypertensive urgency
Administer sublingual nifedipine for management of hypertensive emergency
25) A 65-year-old man presents to the emergency department following the acute onset of palpitations. His wife states that he was eating dinner when he noticed the palpitations, lightheadedness, and shortness of breath. The patient has a history of treated hypertension, but no other medical history. The patient is not able to relate any meaningful history. Blood pressure is 80/40 mmHg, heart rate is 126/ min, respiratory rate is 20/min, and oxygen saturation is 99% on room air; he is afebrile. His heart rate is irregularly irregular with no murmurs, clicks, or rubs. Respiratory examination is unremarkable. X-ray of the chest shows no acute disease. ECG shows no discernible P waves and an irregularly spaced QRS response. Which of the following is the best first step in management?
Administration of adenosine
Placement of dual lead pacemaker
Cardiac catheterization and stent placement
Cardioversion to sinus rhythm
Carotid massage
26) A 65-year-old man develops palpitations and dizziness. His blood pressure is 80/50 mm Hg and his pulse is regular at 150/min. His ECG shows a “saw-toothed” pattern of P waves. Which of the following procedures is most appropriate in converting him back to sinus rhythm?
Carotid sinus pressure
Valsalva maneuver
Gagging procedures
Eyeball compression
Electrical cardioversion
27) A 55-year-old man presents to the ED with worsening weakness, muscle cramps, and paresthesias. His past medical history is significant for hypertension and diabetes. He smokes one pack of cigarettes per day. On examination, the patient is alert and oriented and diffusely weak. An ECG is seen below. Which of the following is the most important next step in management?
Administer calcium gluconate
Order an emergent head CT scan and get a neurology consult
Administer insulin and dextrose
Administer aspirin and call the catheterization laboratory
Collect a sample of his urine to test for ketones
28) A 57-year-old man complains of chest palpitations and light-headedness for the past hour. Five years ago he underwent a cardiac catheterization with coronary artery stent placement. He smokes half a pack of cigarettes daily and drinks a glass of wine at dinner. His HR is 140 beats per minute, BP is 115/70 mmHg, and oxygen saturation is 99% on room air. An ECG reveals a wide complex tachycardia at a rate of 140 that is regular in rhythm. An ECG from 6 months ago shows a sinus rhythm at a rate of 80. Which of the following is the most appropriate medication to treat this dysrhythmia?
Digoxin
Bretylium
Diltiazem
Amiodarone
Adenosine

29) As you are examining the patient described in the previous question, he starts to complain of chest discomfort and shortness of breath and has another syncopal episode. His ECG is shown below. Which of the following is the most appropriate next step in management?
Call cardiology consult
Apply transcutaneous pacemaker
Cardiovert the patient
Administer metoprolol
Administer amiodarone
30) A 19-year-old woman was attacked while coming home from a party and is brought to the emergency department. She recalls being punched in the side of the head and stabbed in the left flank. Her speech is slow and she complains of a bad headache. Her pulse is 110/min, blood pressure is 90/50 mmHg, and respiratory rate is 25/min. On examination she has a stab wound at the left costal margin in the midaxillary line. Two large-bore intravenous lines are inserted, and after infusion of 2 L of lactated Ringer’s solution her blood pressure rises to 95/55 mmHg. What is the most appropriate next step in management?
Abdominal ultrasound
Peritoneal laparoscopy
Diagnostic peritoneal lavage
Exploratory laparotomy
Noncontrast CT of the head
31) A 20-year-old woman arrives at the emergency department actively seizing with QRS prolongation on ECG per paramedics. The patient’s roommate called emergency medical services after the patient collapsed, was not responsive to questioning, and began having clonic jerks bilaterally in her upper extremities. The patient’s roommate denies any knowledge of the patient consuming alcohol or illicit drugs. She does not believe the patient had any plan of harming herself, but does acknowledge that the patient has seemed “down” lately and was recently prescribed medication for generalized anhedonia. Which of the following is the most appropriate first-line treatment?
Activated charcoal
Sodium bicarbonate and diazepam
Diazepam
Flumazenil
Physostigmine
32) A 67-year-old woman is brought to the ED by paramedics complaining of dyspnea, fatigue, and palpitations. Her BP is 80/50 mmHg, HR is 139 beats per minute, and RR is 20 breaths per minute. Her skin is cool and she is diaphoretic. Her lung examination reveals bilateral crackles and she is beginning to have chest pain. Her ECG shows a narrow complex irregular rhythm with a rate in the 140s. Which of the following is the most appropriate immediate treatment for this patient?
Diltiazem
Synchronized cardioversion
Metoprolol
Digoxin
Coumadin
33) A 61-year-old woman with a history of congestive heart failure (CHF) is at a family picnic when she starts complaining of shortness of breath. Her daughter brings her to the ED where she is found to have an oxygen saturation of 85% on room air with rales halfway up both of her lung fields. Her BP is 185/90 mmHg and pulse rate is 101 beats per minute. On examination, her jugular venous pressure (JVP) is 6 cm above the sternal angle. There is lower extremity pitting edema. Which of the following is the most appropriate first-line medication to lower cardiac preload?
Metoprolol
Oxygen
Morphine sulfate
Nitroprusside
Nitroglycerin
34) A 59-year-old man presents to the ED with left-sided chest pain and shortness of breath that began 1 hour ago. Initial vital signs are BP 85/45 mmHg, HR 105 beats per minute, RR 20 breaths per minute, and oxygen saturation 94% on room air. An ECG is seen below. Which of the following is the most appropriate definitive treatment?
Administer metoprolol or diltiazem
Percutaneous angioplasty
Electrical cardioversion
Administer calcium gluconate
Thrombolytic therapy
35) A 32-year-old man is stabbed in the left chest and presents to the emergency department in distress. His pulse is 130/min, blood pressure is 70/50 mmHg, and respiratory rate is 39/min. The stab wound is in the left fifth intercostal space in the midaxillary line. On examination his trachea is deviated to the right, jugular veins are distended bilaterally, and he has absent breath sounds and hyperresonance to percussion on the left side. Subcutaneous emphysema is palpated on the left thoracic wall. What is the best next step in management?
Chest tube thoracotomy
Diagnostic peritoneal lavage
Needle thoracostomy
Pericardiocentesis
Surgical exploration
36) In the ICU, a patient suddenly becomes pulseless and unresponsive, with cardiac monitor indicating ventricular tachycardia. The crash cart is immediately available. What is the best first therapy?
Amiodarone 150-mg IV push
Defibrillation at 200 J
Lidocaine 1.5-mg/kg IV push
Epinephrine 1-mg IV push
Defibrillation at 360 J
37) A 55-year-old African American female presents to the ER with lethargy and blood pressure of 250/150 mmHg. Her family members indicate that she was complaining of severe headache and visual disturbance earlier in the day. They report a past history of asthma but no known kidney disease. On physical examination, retinal hemorrhages are present. Which of the following is the best approach?
Intravenous labetalol therapy
Clonidine by mouth to lower blood pressure
Continuous-infusion nitroprusside
Intravenous loop diuretic
Nifedipine sublingually to lower blood pressure
38) A 36-year-old male presents with the sensation of a racing heart. His blood pressure is 110/70 mmHg, respiratory rate 14/minute, and O2 saturation 98%. His ECG shows a narrow QRS complex tachycardia with rate 180, which you correctly diagnose as paroxysmal atrial tachycardia. Carotid massage and Valsalva maneuver do not improve the heart rate. Which of the following is the initial therapy of choice
Adenosine 6-mg rapid IV bolus
Electrical cardioversion at 50 J
Verapamil 2.5 to 5 mg IV over 1 to 2 min
Diltiazem 0.25-mg/kg IV over 2 min
Digoxin 0.5 mg IV slowly
39) A 56-year-old woman with a history of chronic renal disease presents to the emergency department because of severe, sharp, retrosternal chest pain that radiates to her jaw. The pain worsens when the patient lies down, and she is most comfortable leaning forward and hugging her knees. She takes erythropoietin, furosemide, calcitriol, and sodium polystyrene sulfonate. She is scheduled for dialysis three times per week, but she admits to sometimes missing sessions. She stopped drinking and smoking 20 years ago, and she has no family history of heart or renal problems. Auscultation of the heart reveals a friction rub. Laboratory tests show: WBC count: 12,000/mm3, Hemoglobin: 10.0 g/dL, Hematocrit: 30.0%, Platelet count: 150,000/mm3, Na+: 141 mEq/L, K+: 4.8 mEq/L, Cl: 101 mEq/L, HCO3 : 22 mEq/L, Blood urea nitrogen: 63 mg/dL, Creatinine: 3.2 mg/dL, Glucose: 111 mg/dL. The emergency medicine physician urges the patient to be more compliant with her dialysis, but the patient complains that she is too tired to go to dialysis all of the time and that it is ruining her life. Which of the following is the most likely complication if the patient’s condition remains untreated?
Cardiac tamponade
Restrictive cardiomyopathy
Decreased jugular venous pressure
Mitral regurgitation
Septic shock
40) A 39-year-old white man with essential hypertension presents for a routine health maintenance visit. He has no complaints and reports compliance with his hydrochlorothiazide. His pulse is 70/min, blood pressure is 145/92 mmHg, and respiratory rate is 16/min. His body mass index is 24 kg/m2. His physical examination is within normal limits. For which condition is the patient at increased risk?
End-stage renal disease
Type 2 diabetes mellitus
Hypercholesterolemia
Hypertrophic cardiomyopathy
Second-degree Mobitz I atrioventricular block
41) A 40-year-old man is brought to the emergency room after his wife found him alone in a confused state. He admits to overdosing in a suicide attempt, but does not specify the drug taken. En route to the hospital, he is drowsy and ataxic with blurred vision. His past medical history is significant for asthma, insomnia, depression, and substance abuse. His temperature is 38.3°C (100°F), blood pressure is 130/80mmHg, pulse is 100/min, and respirations are 22/min. Examination shows dry mucus membranes and skin; pupils are 8mm bilaterally. There is no neck stiffness. Lungs are clear to auscultation. Heart sounds are within normal limits. Abdominal examination shows reduced bowel sounds with no tenderness. A Foley catheter is placed in the ER and 600 ml of urine is collected over one hour. Which of the following is the most likely diagnosis?
Salicylate intoxication
Phencyclidine poisoning
Serotonin syndrome
Cocaine intoxication
Diphenhydramine poisoning
42) A 46-year-old male is admitted to the hospital because of right hand cellulitis. He has a history of intravenous drug use, hepatitis C infection and septic arthritis of the knee. He smokes one pack of cigarettes and drinks one pint of vodka daily. He is started on vancomycin. On the following day, the swelling and redness of his arm decreases. However, he complains of bugs crawling on his skin. His temperature is 38.3°C (100.9°F), blood pressure is 160/90 mmHg, pulse is 110/min, and respirations are 18/min. Examination shows mild hand tremors and diaphoresis. Which of the following is the most appropriate next step in management
Start chlordiazepoxide
Start methadone
Give haloperidol
Start propranolol
Stop vancomycin
43) A 35-year-old woman is brought to the emergency room after an apparent suicide attempt. Her current prescription of imipramine was found at her bedside along with a suicide note. En route to the hospital, she suffered a seizure. She has been treated with many different anti-depressants over the past several years without improvement. Her temperature is 38.3°C (101°F), blood pressure is 90/50 mmHg, pulse is 120/min and respirations are 24/min. EKG shows QRS widening (0.18sec). She is given sodium bicarbonate along with supportive treatment. Which of the following is the most likely mechanism that explains the beneficial effects of sodium bicarbonate?
Alkalinization of urine will promote diuresis of the antidepressants
Sodium load of sodium bicarbonate will alleviate depressant action on sodium channels
Acidification of urine will promote diuresis of the antidepressants
Sodium load of sodium bicarbonate will alleviate depressant action on potassium channels
Sodium load of sodium bicarbonate will alleviate depressant action on calcium channels
44) A 32-year-old male is admitted to the hospital because of confusion. He was recently diagnosed with schizophrenia His temperature is 38.6°C (101.6°F), blood pressure is 160/100 mmHg, pulse is 116/min, and respirations are 22/min. He is not oriented to time, place or person. Mucus membranes are dry. Profuse diaphoresis is present. Lungs are clear to auscultation. Abdominal, neck and extremity muscles are rigid. Muscle tone is increased. Deep tendon reflexes are 2+. Laboratory studies show a serum CK of 50,000 IU/L. CSF fluid analysis shows a total white blood cell count of 5/microL. Which of the following is the most appropriate next step in management?
Risperidone
Antibiotics
Dantrolene
L-Dopa
Prednisone
45) A 38-year-old homeless man is brought to the emergency room. He is obtunded and unable to speak. No previous medical history is known. His temperature is 34.0°C (93.2°F), blood pressure is 90/60 mmHg, pulse is 60/min and respirations are 6/min. Oxygen saturation is 86% on room air. Pupils are 5 mm in size, bilaterally. Oropharynx is dry. Lungs are clear to auscultation. Abdomen is soft; bowel sounds are decreased; there is no organomegaly. Extremities reveal several needle marks. Babinski sign is negative. Deep tendon reflexes are 2+ throughout. Which of the following is the most appropriate next step in management?
CT scan of the head
Flumazenil
Glucagon
Methadone
Naloxone
46) A mother brings her 16-year-old daughter to the ER after she had two episodes of coffee ground emesis. The mother reports that for the past two weeks, the teen has not been acting like herself; she has been especially isolated and has had a poor appetite and poor sleep. Her medical history is significant for anemia, for which she takes iron sulfate and folic acid. She also takes acetaminophen for occasional back pain. Presently, the patient's blood pressure is 110/70 mmHg and heart rate is 120/min. Which of the following is most likely to establish the diagnosis?
Liver function tests
Upper GI endoscopy
Serum iron level
CT scan of the head
Serum acetaminophen level
47) A 47-year-old man is brought to the ED by EMS after being found wandering in the street mumbling. His BP is 150/75 mmHg, HR is 110 beats per minute, temperature is 100.5°F, RR is 16 breaths per minute, oxygen saturation is 99% on room air, and fingerstick glucose is 98 mg/dL. On examination, the patient is confused with mumbling speech. His pupils are dilated and face is flushed. His mucous membranes and skin are dry. Which of the following toxic syndromes is this patient exhibiting?
Sympathomimetic syndrome
Ethanol syndrome
Anticholinergic syndrome
Cholinergic syndrome
Opioid syndrome
48) A 25-year-old man is carried into the ED by two of his friends who state that he is not breathing. The patient has a history of heroin abuse. His vital signs are BP 115/70 mmHg, HR 99 beats per minute, temperature 98.9°F, RR 3 breaths per minute, and oxygen saturation 87% on room air. You notice fresh needle marks and miotic pupils. You begin bag-valvemask ventilation and his oxygen saturation increases to 99%. Which of the following is the most appropriate next step in management?
Continue bag-valve-mask ventilation until he breathes on his own
Evaluate response to administration of naloxone
Perform endotracheal intubation of the patient
Put the patient on supplemental oxygen
Place a nasogastric tube and administer activated charcoal
49) A 42-year-old man who is actively seizing is brought to the ED by EMS after a massive ingestion of an unknown substance. The man is known to have a history of acquired immunodeficiency syndrome (AIDS). An intravenous (IV) line is established and anticonvulsant therapy is administered. After high doses of diazepam, phenobarbital, and phenytoin, it is determined that the seizures are refractory to standard anticonvulsant therapy. Which of the following substances did this patient most likely ingest?
Cocaine
Isoniazid (INH)
Diphenhydramine
Tricyclic antidepressant (TCA)
Haloperidol
50) A 26-year-old man is brought to the emergency room by police with depressed mental status. Out of fear of arrest, he swallowed a handful of pills as the police officers approached him. On examination, he responds to painful stimuli but is somnolent. His respiratory rate is 8/min and after naloxone bolus infusion increases to 12/min. Lungs are clear to auscultation. Which of the following additional findings is most likely to be present in this patient?
Miosis, bradycardia, hypertension
Mydriasis, tachycardia, hypertension
Miosis, tachycardia, hypotension
Miosis, bradycardia, hypotension
Miosis, tachycardia, hypertension
51) A 29-year-old male is brought to the emergency room because of sudden onset confusion and fever. He was recently admitted to the hospital for hallucinations and was discharged instable condition. His temperature is 38.6°C (101.6°F), blood pressure is 150/100 mmHg, pulse is 112/min, and respirations are 24/min. Mucus membranes are dry. Profuse diaphoresis is present. Lungs are clear to auscultation. Abdominal muscles are rigid. Muscle tone is increased; "lead pipe rigidity" is noted in all four extremities. Deep tendon reflexes are 2+. Tremor is noted. Which of the following is the most likely diagnosis?
Tetanus
Cocaine intoxication
Meningitis
Drug induced idiosyncratic reaction
Cocaine intoxication
52) A 26-year-old man is brought to the emergency room after an attempted suicide by medication overdose. For the past hour, he has suffered two seizures. His temperature is 38.8°C (102°F), blood pressure is 110/85 mmHg, pulse is 90/min, and respirations are 22/min. He is not oriented to time, place, and person. Pupils are dilated, but reactive to light and accommodation; skin is flushed and dry. Abdominal examination shows reduced bowel sounds. EKG shows prolonged QRS complexes (0.19 sec). Toxicology studies are pending. Which of the following is the most appropriate indicator of severity of intoxication?
Serum drug levels
Bowel sounds
Urine drug levels
Duration of QRS complex
Pupillary size

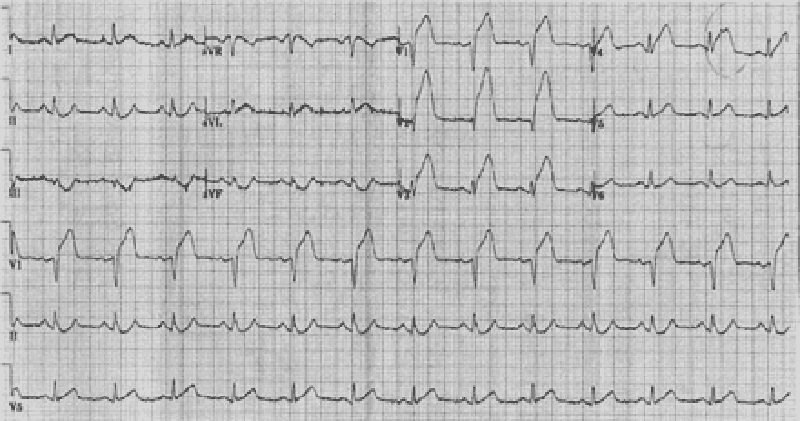
53) A 42-year-old male is admitted to the hospital with fever and shortness of breath. He has HIV infection, hepatitis C infection, and alcohol induced cardiomyopathy. His temperature is 38.6°C (101.5°F). Thrush is noted in the oropharynx. Chest x-ray reveals right lower lobe consolidation. He is started on fluconazole and moxifloxacin. His pneumonia and thrush improve over the next 2 days. However, on the third day, he develops palpitations. His EKG strip is shown below. Which of the following is the most appropriate next step in management?
Calcium gluconate
Magnesium sulphate
Sotalol
Amiodarone
Adenosine
54) A 34-year-old homeless man is brought to the emergency room in a confused state. He complains of epigastric pain, vomiting and blurred vision. His temperature is 36.8°C (98.2°F), blood pressure is 110/60 mmHg, pulse is 110/min and respirations are 22/min. Physical examination shows poor oral hygiene and dry mucous membranes. Lungs are clear to auscultation. Abdominal exam shows mild epigastric discomfort. Funduscopic examination reveals optic disc hyperemia. Laboratory studies show: Serum sodium 136 mEq/L, Serum potassium 3.0 mEq/L, Chloride 93 mEq/L, Bicarbonate 6 mEq/L, Blood urea nitrogen (BUN) 30 mg/dL, Serum creatinine 0.8 mg/dL, Blood glucose 80 mg/dL, Serum ketones negative, Plasma lactate 2.2 mEq/L. Which of the following is the most likely cause of his symptoms?
Ethylene glycol poisoning
Mesenteric ischemia
Septic shock
Diabetic ketoacidosis
Methanol poisoning
55) You receive notification from EMS that they are bringing in a 17-yearold adolescent boy who was found unconscious by a police officer. The police officer at the scene states that he snuck up on a group of kids that he thought were using drugs. Two of them got away and one just fell to the ground seconds after standing up. Lying on the ground next to the adolescent were plastic bags. The emergency medical technician (EMT) states that the patient was in ventricular fibrillation. He was shocked in the field and is now in a sinus rhythm. The EMT also administered IV dextrose, thiamine, and naloxone without any change in mental status. Which of the following substances was the patient most likely abusing?
Butane
PCP
Ethanol
Heroin
Cocaine
56) A 61-year-old man with a history of depression and hypertension is brought to the ED by EMS for altered mental status. The patient’s wife states that he stopped taking his fluoxetine 1 month ago and now only takes metoprolol for his hypertension. The patient’s BP is 75/40 mmHg, HR is 39 beats per minute, RR is 14 breaths per minute, oxygen saturation is 99% on 100% oxygen, and fingerstick glucose is 61 mg/dL. The patient is awake and moaning, responding only to deep stimuli. His extremities are cool to the touch. You suspect an overdose of metoprolol. You endotracheally intubate the patient for airway control. Which of the following is the most appropriate next step in management?
Normal saline bolus, administer atropine, administer 1-g calcium gluconate bolus, then insert a transvenous cardiac pacer
Cardioversion with 200 J, then administer atropine
Put the patient on pacer pads, then administer norepinephrine drip
Normal saline bolus, atropine, norepinephrine
Normal saline bolus, atropine, glucagon
57) A 22-year-old woman presents to the ED by ambulance from a dance club. The paramedics report that the patient was agitated in the club and had a generalized seizure. Her BP is 165/100 mmHg, HR is 119 beats per minute, temperature is 101.9°F, RR is 17 breaths per minute, oxygen saturation is 98% on room air, and fingerstick glucose is 92 mg/dL. On examination, the patient is hyperactive and appears to be hallucinating. Her pupils are dilated to 6 mm bilaterally and reactive. Her neck is supple. Examination of the heart is unremarkable except for tachycardia. Her lungs are clear and abdomen is soft and nontender. The patient moves all four extremities. Laboratory results are as follows: Sodium 109 mEq/L, WBC 12,000/mm3, Potassium 3.5 mEq/L, Hct 49%, Chloride 83 mEq/L, Platelets 350/μL, Bicarbonate 20 mEq/L, BUN 10 mg/dL, Creatinine 1 mg/dL, Glucose 103 mg/dL. Which of the following substances did this patient most likely consume?
Cocaine
Ketamine (special K)
Heroin
3,4-Methylenedioxymethamphetamine (MDMA
PCP
58) A 32-year-old woman is brought to the emergency department by her husband because of slurred speech and difficulty walking. She has also been very drowsy for the past several hours, a non-typical behavior for a very active woman. She has a history of bipolar disorder, insomnia, migraine headaches, seizures and hypothyroidism. Her temperature is 37°C (98.6°F), blood pressure is 110/70 mmHg, pulse is 76/min, and respirations are 16/min. She is lethargic and falls asleep during the interview and physical examination. Pupils are 5 mm in size and reactive to light. Neck is supple. Oropharynx is clear. Chest auscultation is unremarkable. Abdomen is soft and non-tender; bowel sounds are normal. Limited neurologic examination shows 1+ deep tendon reflexes in all four extremities; there is no Babinski sign; strength is 5/5 throughout. There is no nystagmus or hand tremor. Blood sugar is 130 mg/dL. Which of the following is the most likely cause of her symptoms?
Cerebrovascular accident
Lithium toxicity
Phenytoin toxicity
Benzodiazepine overdose
Ethanol intoxication
59) A 31-year-old woman with a known psychiatric history presents to the ED after ingesting an unknown quantity of pills from her medication vial. In the ED, she complains of nausea, abdominal cramping, and feels unsteady on her feet. On physical examination, you observe that she is tachycardic and ataxic. Which of the following substances will best be treated by activated charcoal that could present like this
Phenobarbital
Lye (sodium hydroxide
Carbamazepine
Lithium
Acetaminophen
60) A 27-year-old man presents to the ED extremely agitated complaining of mild chest pain and dyspnea. He states that he was snorting cocaine all afternoon. You place him on a monitor and get his vital signs. His BP is 215/130 mmHg, HR is 112 beats per minute, temperature is 100.1°F, RR is 17 breaths per minute, and oxygen saturation is 98% on room air. An ECG reveals sinus tachycardia at a rate of 116. Which of the following is the most appropriate medication to administer?
Haloperidol
Diazepam
Labetalol
Esmolol
Diltiazem
61) A 30-year-old man is brought to the ED by police officers. The patient is agitated, vomiting, and complaining of body aches. He states that he is withdrawing from his medication. His vital signs are BP 160/85 mmHg, RR 20 breaths per minute, HR 107 beats per minute, and temperature 99.7°F. On examination he is diaphoretic, has rhinorrhea, piloerection, and hyperactive bowel sounds. Which of the following substances is this patient most likely withdrawing from?
Ethanol
Clonidine
Cocaine
Nicotine
Methadone
62) A 25-year-old man is brought into the ED by two police officers because of suspected drug use. The patient is extremely agitated and is fighting the police officers. It takes three hospital staff members and the two police officers to keep him on the stretcher. His vital signs are BP 150/80 mmHg, HR 107 beats per minute, temperature 99.7°F, RR 18 breaths per minute, and oxygen saturation 99% on room air. Physical examination is unremarkable except for cool, diaphoretic skin, persistent vertical and horizontal nystagmus, and occasional myoclonic jerks. Which of the following is the most likely diagnosis?
Cocaine intoxication
Opiate withdrawal
Cocaine withdrawal
Anticholinergic toxidrome
PCP intoxication
63) A 20-year-old female is brought to the emergency room after getting struck by a motor vehicle. She appears confused. According to her parents, she has no other medical problems and does not take any prescription medications. However, they have noticed her increase in appetite recently. She occasionally drinks alcohol and smokes half a pack of cigarettes daily. Her temperature is 37.2°C (99°F), blood pressure is 150/90mmHg, pulse is 110/min, and respirations are 22/min. Examination reveals dry mouth and conjunctival injection. Pupils are equal, reactive to light and accommodation. She has impaired time orientation and shortterm memory. Which of the following is the most likely explanation for this patient's symptoms?
Benzodiazepine overdose
Marijuana overdose
Opioid overdose
Cocaine intoxication
Alcohol intoxication
64) A 34-year-old male is brought to the emergency department by his neighbor. The neighbor found the man lying on the floor beside an empty bottle of unknown substance. At the hospital, the patient is conscious and alert, but in severe pain. His temperature is 36.8°C (98.2°F), blood pressure is 130/70 mmHg, pulse is 90/min and respirations are 20/min. Abdomen is benign, with normal bowel sounds. Pupils are 5 mm, bilaterally. His tongue is white, heavy drooling of saliva is noted and he is unable to swallow. Which of the following is the most likely explanation for this patient's symptoms?
Anticholinergic poisoning
Alcohol intoxication
Caustic poisoning
Tricyclic antidepressant poisoning
Cyanide poisoning
65) A 35-year-old woman calls her family physician after her 7-year old son accidentally splashed an unknown liquid containing acid on his face. Some liquid likely entered his eye, as the child is complaining of severe pain in his right eye. She knows a doctor living in her immediate neighborhood but is hesitant about what to do next. Which of the following is the most appropriate initial course of action that the mother should take
Call 911 immediately
Wash the eye with copious amount of water
Go to local emergency room immediately
Go to the doctor in the neighborhood immediately
Do not try to wash the eye as it can enhance the damage
66) A worried and anxious pregnant mother brings her 3-year-old son to the emergency room after he experienced several episodes of vomiting and abdominal pain for the past two hours. His vomit is coffee ground in appearance. He is irritable and lethargic. His blood pressure is 80/50mmHg and pulse rate is 120/min. Examination shows a normal oropharynx; chest auscultation is within normal limits. Abdomen is soft and mildly tender at the epigastrium; there is no hepatosplenomegaly. Extremities are cold to touch. Initial laboratory studies show: Hemoglobin 10.3 g/L, Leukocyte count 14,500/mm3, Bicarbonate 18 mEq/L. Chest x-ray is within normal limits. Abdominal imaging shows radio opaque tablets in the stomach. Intravenous normal saline is started. Which of the following is the most appropriate next step in management?
Sodium bicarbonate
Hemodialysis
Deferoxamine
Magnesium sulphate
Hemodialysis
67) A 32-year-old male comes to the hospital complaining of pain, swelling and redness of his right arm. His past medical history is significant for substance abuse. His temperature is 38.9°C (102.0°F), blood pressure is 110/60 mmHg, pulse is 110/min and respirations are 14/min. He is started on intravenous clindamycin. The next day the swelling and pain improve, but he develops nausea, vomiting, abdominal cramps and diarrhea. He is restless and asks for pain medication to treat his aching muscles and joints. His temperature now is 37.3°C (99.1°F), blood pressure is 120/70 mmHg, pulse is 80/min and respirations are 16/min. His laboratory studies at the time of admission and the following day show: Hemoglobin 13.0 g/L (12.8 g/L), Leukocyte count 17,500/mm3 (8,500/mm3), NeutrophiIs 86% (64%), Lymphocytes 14% (26%). Which of the following is the most appropriate next step in management?
Stool for Clostridium difficile toxin
Start intravenous morphine
Discontinue clindamycin
Start chlordiazepoxide
Start methadone
68) A 34-year-old homeless male is brought to the ER in a confused state. He complains of flank pain. His past medical history is unknown. His temperature is 36.8°C (98.2F), blood pressure is 110/60 mmHg, pulse is 110/min and respirations are 22/min. His appearance is disheveled. Pupils are equal, 4 mm in size and reactive to light. Funduscopic examination is within normal limits. Lungs have crackles at both bases. Mild costovertebral angle tenderness is present. Foley catheter is placed and urine appears red. Laboratory studies show: Serum sodium 136 mEq/L, Serum potassium 3.5 mEq/L, Chloride 93 mEq/L, Bicarbonate 6 mEq/L, Blood urea nitrogen (BUN) 34 mg/dl, Serum creatinine 2.8 mg/dl, Blood glucose 80 mg/dl, Calcium 6.5 mg/dl, Serum ketones negative, Plasma lactate 2.4 mEq/L. Which of the following is the most appropriate next step in management?
Fomepizole
N-acetylcysteine
Broad spectrum antibiotics
Regular insulin
Glucagon
69) A 26-year-old bar employee is brought to the emergency room because of agitated, combative behavior in which three people had to restrain her. She has also been hallucinating during this entire period. Her temperature is 37.7°C (100°F), blood pressure is 160/90 mmHg, pulse is 126/min, and respirations are 18/min. She is confused and agitated during the examination. Pupils are 6 mm in diameter and respond to light; prominent nystagmus is present. The remainder of her examination is unremarkable. Which of the following is the most likely diagnosis?
Barbiturate intoxication
Opioid intoxication
Phencyclidine intoxication
Cocaine intoxication
Marijuana Intoxication
70) A 38-year-old man is brought to the emergency room by EMS after an apparent suicide attempt. En route to the hospital, he appeared confused and suffered a seizure. He has a history of hypertension and major depression. His temperature is 37.7°C (100°F), blood pressure is 70/40 mmHg, pulse is 40/min, and respirations are 12/min. Examination shows normal heart sounds and diffuse wheezing. Extremities are cold and clammy. EKG shows AV block. The patient is given intravenous fluids and atropine; however, his bradycardia and hypotension do not improve. Which of the following is the most appropriate next step in management?
Epinephrine
Pacemaker
Aminophylline
Digoxin specific antibody
Glucagon
71) A 24-year-old woman is brought to the emergency room after ingesting 14 acetaminophen tablets, 500 mg each, two hours ago. She does not smoke but drinks alcohol on the weekends. She is alert and oriented. Her temperature is 37.2°C (99°F), blood pressure is 110/60mmHg, pulse is 90/min and respirations are 18/min. Examination shows no abnormalities. Laboratory studies show: Hct 40%, WBC 6,000/mm3, Platelet 390,000/mm3. Which of the following is the most appropriate next step in management?
Administer the loading dose of N-acetylcysteine
Obtain serum acetaminophen levels now
Obtain serum acetaminophen levels in two hours
Transfer to liver transplantation facility
Discharge her home without further work up
72) A group of teenagers attend an indoor barbecue on a cold winter night. They all ate servings of potato salad and barbecue chicken. A few hours later, they present to the local emergency room with headache, nausea, vomiting, vague abdominal discomfort and confusion. One of the teenagers mentions a pet dog that was in the room with them had similar symptoms. A quick physical examination of one patient reveals tachycardia, tachypnea and a pinkish-skin hue. Which of the following is the most likely diagnosis?
Viral illness
Methemoglobinemia
Carbon monoxide poisoning
Acute gastroenteritis
Cyanide poisoning
73) A 40-year-old man is brought to the emergency room for retrosternal and epigastric pain after ingesting an unknown amount of "lye" (drain cleaner) 45 minutes ago. His past medical history is significant for major depression and suicide attempt. He is unable to swallow his saliva and is drooling. His temperature is 36.8°C (98.2°F), blood pressure is 120/70 mmHg, pulse is 110/min, and respirations are 20/min. Examination shows oropharyngeal erythema and edema. Lungs are clear to auscultation. Abdominal examination reveals tenderness at the epigastrium without rebound or guarding. Chest x-ray shows no abnormalities. Intravenous hydration is started. Which of the following is the most appropriate next step in treatment?
Gastric decontamination with ipecac
Administer high dose systemic steroids
Administer activated charcoal in water
Neutralization and dilution of the alkali
Upper gastrointestinal contrast studies and endoscopy
74) A 34-year-old farmer is brought to the hospital after attempting suicide. His body and clothes are soiled with vomitus. He is short of breath and appears agitated. His family reports no previous medical history or regular use of prescription medications. His temperature is 36.6°C (98°F), blood pressure is 110/60 mmHg, pulse is 50/min, and respirations are 22/min. His oxygen saturation is 86% on room air. Examination shows watering of the eyes and 1 mm pupils, bilaterally. Lung examination shows widespread rhonchi with prolonged expiration. Abdominal examination shows increased bowel sounds. Neurologic examination shows muscle fasciculations. What would be the most appropriate next step in management of this patient?
Obtain EKG for QRS duration
Obtain a head CT scan
Remove all the clothing and wash the body
Obtain a chest x-ray
Give physostigmine
75) A 60-year-old male is found lying down on the street by police one winter morning. He has been taking ibuprofen for headaches, fluphenazine for his schizophrenia and amitriptyline for chronic painful neuropathy secondary to post-herpetic neuralgia. He is also receiving cephalexin for cellulitis of the right lower leg. His temperature is 34°C (90°F), blood pressure is 80/50 mmHg, pulse is 88/min, and respirations are 12/min. Which of the following medications most likely have contributed to the development of hypothermia in this patient?
Ibuprofen
Glucagon
Amitriptyline
Cephalexin
Fluphenazine
76) A 45-year-old woman is brought to the ER by ambulance after a neighbor found her to be in a somewhat obtunded state with an empty bottle of medication next to her. While en route to the ER she suffered a tonic clonic seizure. Her past medical history is significant for major depression. Her temperature is 38.3°C (100.9°F), blood pressure is 90/70 mmHg, pulse is 120/min, and respirations are 16/min. She is able to respond to painful stimuli. Pupils are 8 mm in size bilaterally. Skin is warm and flushed. Lungs are clear to auscultation. Abdomen is soft and non-tender. Bowel sounds are decreased. There is no neck stiffness. EKG shows QRS duration of 130 msec, a change from her previous EKG a month ago. Which of the following is the most appropriate next step in management?
Lumbar puncture
Echocardiogram
Thyroid function tests
Calcium gluconate
Sodium bicarbonate
77) After being fired from his job, a 35-year-old man attempts suicide by drinking from a bottle labeled “insecticide.” Three hours later, emergency medical services (EMS) brings him into the emergency department (ED) and you notice that he is extremely diaphoretic, drooling, and vomiting. He is awake but confused. His vital signs include a blood pressure (BP) of 170/90 mmHg, heart rate (HR) of 55 beats per minute, respiratory rate (RR) of 22 breaths per minute, temperature of 98.6°F, and oxygen saturation of 95% on room air. Physical examination demonstrates pinpoint pupils and crackles and wheezing on lung examination. What is the treatment to reverse this patient’s poisoning?
Naloxone
Physostigmine
N-acetylcysteine (NAC)
Atropine and pralidoxime (2-PAM)
Flumazenil
78) A 19-year-old man is brought to the ED by EMS after he was found lying on the floor at a dance club. EMS states that the patient seemed unconscious at the dance club, but as soon as they transferred him onto the gurney, he became combative. Upon arrival in the ED, his BP is 120/65 mmHg, HR is 75 beats per minute, temperature is 98.9°F, RR is 12 breaths per minute, and oxygen saturation is 98% on room air. On physical examination, his pupils are midsized, equal, and reactive to light. His skin is warm and dry. Lung, cardiac, and abdominal examinations are unremarkable. As you walk away from the bedside, you hear the monitor alarm signaling zero respirations and the oxygen saturation starts to drop. You perform a sternal rub and the patient sits up in bed and starts yelling at you. As you leave him for the second time, you hear the monitor alarm again signal zero respirations. You administer naloxone, but there is no change in his condition. Which of the following is most likely the substance ingested by this patient?
γ-Hydroxybutyrate (GHB)
Phencyclidine (PCP)
Diazepam
Cocaine
Heroin
79) A 43-year-old woman presents to the ED with a 3-week history of intermittent headache, nausea, and fatigue. She was seen at her private doctor’s office 1 week ago along with her husband and children, who also have similar symptoms. They were diagnosed with a viral syndrome and told to increase their fluid intake. She states that the symptoms began approximately when it started to get cold outside. The symptoms are worse in the morning and improve while she is at work. Her BP is 123/75 mmHg, HR is 83 beats per minute, temperature is 98.9°F, and oxygen saturation is 98% on room air. Physical examination is unremarkable. You suspect her first diagnosis was incorrect. Which of the following is the most appropriate next step to confirm your suspicion?
Order a mono spot test
Order a lead level
Perform a nasal pharyngeal swab to test for influenza
Consult psychiatry to evaluate for malingering
Order a carboxyhemoglobin (COHb) level
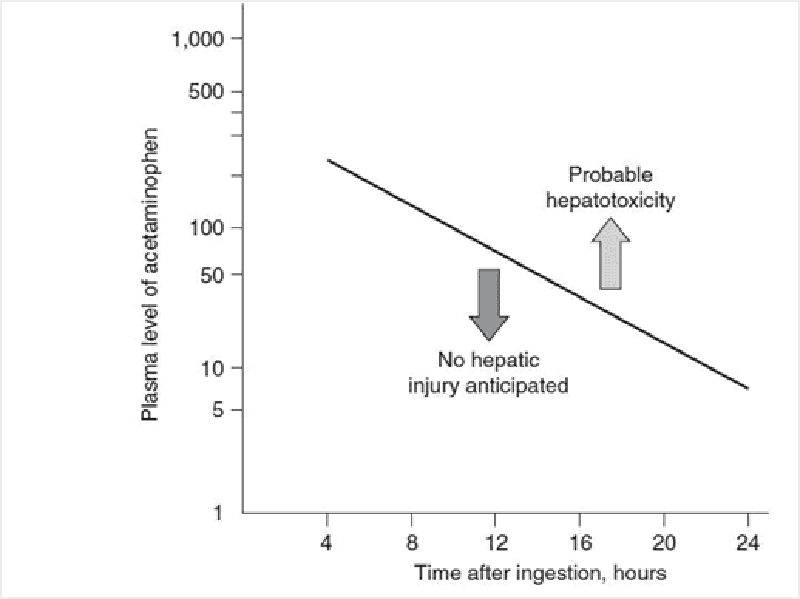
80) An 18-year-old woman is brought to the ED by her mother. The patient is diaphoretic and vomiting. Her mom states that she thinks her daughter tried to commit suicide. The patient admits to ingesting a few handfuls of acetaminophen (Tylenol) approximately 3 hours ago. Her temperature is 99.1°F, BP is 105/70 mmHg, HR is 92 beats per minute,RR is 17 breaths per minute, and oxygen saturation is 99% on room air. On examination, her head and neck are unremarkable. Cardiovascular and pulmonary examinations are within normal limits. She is mildly tender in her right upper quadrant, but there is no rebound or guarding. Bowel sounds are normoactive. She is alert and oriented and has no focal deficits on neurologic examination. You administer 50 g of activated charcoal. At this point, she appears well and has no complaints. Her serum acetaminophen (APAP) concentration 4 hours after the reported time of ingestion returns at 350 μg/mL. You plot the level on the nomogram seen below. Which of the following is the most appropriate next step in management?
Begin NAC and admit to the hospital
Repeat the acetaminophen level 4 hours after the patient arrived in the ED. Treat only if this level is above the line
Discharge home with instructions to return if symptoms return
Observe for 6 hours and, if the patient still has no complaints, discharge her home
Admit to the psychiatry unit and keep on suicide watch while performing serial abdominal examinations.
81) A 60-year-old woman with a history of diabetes is brought into the ED by EMS workers who state that the patient was found on a bus in a lethargic and diaphoretic condition. Her fingerstick glucose level at the scene was 35 mg/dL. EMS workers quickly administered dextrose through an IV line. The patient became alert and responsive, stating that she just took her normal medication. Her blood sugar went up to 110 mg/dL and she remained this way throughout her trip to the ED. However, in the ED you notice that the patient is again diaphoretic and is mumbling her speech. Her fingerstick glucose is now 47 mg/dL. You administer dextrose and she perks right up. Which of the following diabetes medications commonly causes hypoglycemia for which the patient is likely to require hospital admission
Regular insulin
Acarbose
Metformin
Glyburide
Sitagliptin
82) A 23-year-old woman presents to the ED complaining of abdominal pain, nausea, and vomiting. She has a history of depression but is not currently taking any antidepressant medications. Upon further questioning, the patient states that she ingested a bottle of pills in her medicine cabinet approximately 3 hours ago. Her BP is 115/65 mmHg, HR is 101 beats per minute, temperature is 100.1°F, RR is 29 breaths per minute, and oxygen saturation is 100% on room air. Physical examination is unremarkable except for mild diffuse abdominal tenderness. Laboratory results reveal a white blood cell (WBC) count of 10,300/μL, hematocrit 46%, platelets 275/μL, aspartate transaminase (AST) 70 U/L, alanine transaminase (ALT) 85 U/L, alkaline phosphatase 75 U/L, sodium 143 mEq/L, potassium 3.7 mEq/L, chloride 98 mEq/L, bicarbonate 8 mEq/L, blood urea nitrogen (BUN) 22 mg/dL, creatinine 0.9 mg/dL, and glucose 85 mg/dL. Arterial blood gas values on room air are pH 7.51, PCO2 11 mm Hg, and PO2 134 mm Hg. Which of the following substances did this patient most likely ingest
Diphenhydramine
Aspirin
Ibuprofen
Acetaminophen
Pseudoephedrine
83) A 35-year-old agitated man presents to the ED in police custody. He denies any past medical history and takes no medication. He admits to using some drugs today. His BP is 195/90 mmHg, HR is 121 beats per minute, temperature is 100.1°F, RR is 18 breaths per minute, and oxygen saturation is 99% on room air. On examination, he is diaphoretic, and has pupils that are 8 mm in diameter, along with 3+ patella reflexes bilaterally. Electrocardiogram (ECG) reveals sinus tachycardia with a rate of 123. Which of the following toxic syndromes is this patient exhibiting?
Anticholinergic
Sedative hypnotic
Cholinergic
Sympathomimetic
Opioid
84) An undomiciled 49-year-old man presents to the ED with altered mental status. His BP is 149/75 mmHg, HR is 93 beats per minute, temperature is 97.5°F, RR is 18 breaths per minute, and O2 saturation is 99% on room air. Physical examination reveals an unkempt man with the odor of “alcohol” on his breath. His head is atraumatic and pupils are 4 mm, equal, and reactive. The neck is supple. Cardiovascular, pulmonary, and abdominal examinations are unremarkable. There is no extremity edema and his pulses are 2+ and symmetric. Neurologically, he withdraws all four extremities to deep stimuli. ECG is sinus rhythm. Laboratory results reveal: Sodium 141 mEq/L, Potassium 3.5 mEq/L, Chloride 101 mEq/L, Bicarbonate 14 mEq/L, BUN 15 mg/dL, Creatinine 0.7 mg/dL, Glucose 89 mg/dL, Arterial blood pH 7.26, Lactate 1.7 mEq/L, Ethanol level undetectable, Measured serum osmolarity 352 mOsm/L, Calculated serum osmolarity 292 mOsm/kg. Urinalysis: no blood, ketones, or protein. Which of the following statements best describes the laboratory findings?
Anion gap metabolic acidosis and osmol gap
Nonanion gap metabolic acidosis without osmol gap
Anion gap metabolic acidosis without osmol gap
Nonanion gap metabolic acidosis and osmol gap
Metabolic alkalosis with secondary acidosis
85) A 26-year-old woman with a history of depression is brought into the ED. She was found lying on the floor of her apartment next to an unlabeled empty pill bottle. Her HR is 117 beats per minute, BP is 95/65 mmHg, RR is 14 breaths per minute, and oxygen saturation is 97% on 2-L nasal cannula. On examination, the patient appears obtunded, and her pupils are 3 mm and reactive. Her oropharynx is dry and there is no gag reflex to pharyngeal stimulation. Her neck is supple. The heart is tachycardic without murmurs, the lungs are clear to auscultation, and the abdomen is soft. There is normal rectal tone and brown stool that is heme negative. Her skin is cool and moist with no signs of needle tracks. Neurologically, she is unresponsive but withdraws all extremities to deep palpation. Fingerstick blood glucose is 85 mg/dL. Her ECG reveals sinus tachycardia at 119 with a QRS complex of 140 milliseconds and a terminal R wave in lead aVR. Which of the following is the most appropriate next step in management?
Orotracheal intubation, administer activated charcoal through orogastric tube, and IV naloxone
Orotracheal intubation, administer activated charcoal through orogastric tube, and IV NAC
Orotracheal intubation, administer activated charcoal through orogastric tube, and IV sodium bicarbonate
Orotracheal intubation, administer syrup of ipecac through orogastric tube, and IV sodium bicarbonate
Induce vomiting prior to intubation to lower the risk of aspiration then administer IV sodium bicarbonate
86) A 37-year-old woman is brought into the ED by her friend who states that the patient swallowed approximately 50 capsules of 325-mg acetaminophen (APAP) 6 hours ago in an attempted suicide. The patient states she feels nauseated and vomits while you take her history. Her BP is 100/75 mmHg, HR is 97 beats per minute, temperature is 98.9°F, RR is 18 breaths per minute, and oxygen saturation is 99% on room air. Examination is unremarkable except for mild epigastric tenderness. Which of the following is the correct antidote for APAP overdose?
NAC
Digibind
Physostigmine
Flumazenil
Naloxone
87) A 31-year-old man is brought to the ED by EMS who state that the man was found lying on the floor of his garage. He is rousable in the ED, speaks with slurred speech, and vomits. His BP is 140/85 mmHg, HR is 94 beats per minute, temperature is 98.8°F, RR is 17 breaths per minute, and oxygen saturation is 99% on room air. You place an IV line, draw blood, and start a liter of normal saline running through the line. Laboratory results reveal serum sodium 139 mEq/L, potassium 3.5 mEq/L, chloride 101 mEq/L, bicarbonate 14 mEq/L, BUN 15 mg/dL, creatinine 1 mg/dL, glucose 105 mg/dL, arterial blood pH 7.27, COHb 4%, and lactate 2.8 mEq/L. Urinalysis shows 1+ protein, trace ketones, WBC 4/hpf (high-power field), red blood cell (RBC) 2 to 3/hpf, and multiple envelope-shaped and needle shaped crystals. Which of the following conditions would best explain his metabolic acidosis?
Ibuprofen toxicity
Ethylene glycol poisoning
Diabetic ketoacidosis (DKA)
Lactic acidosis
Isopropyl alcohol poisoning
88) A 35-year-old man who is employed as a forklift operator was found sitting outside a warehouse. He came stumbling out complaining of dizziness and headaches. Co-workers in an adjoining warehouse also complained of headache and nausea. After collapsing outside, he regained consciousness immediately but appeared confused. In the ED, his BP is 100/54 mmHg, HR is 103 beats per minute, temperature is 100°F, pulse ox is 91% on room air, and RR is 23 breaths per minute. Physical examination is unremarkable. Laboratory results reveal WBC 10,500/μL, hematocrit 45%, platelets 110/μL, sodium 137 mEq/L, potassium 4 mEq/L, chloride 103 mEq/L, bicarbonate 21 mEq/L, BUN 8 mg/dL, creatinine 0.5 mg/dL, and glucose 89 mg/dL. Arterial blood gas results are pH 7.32, PCO2 32 mm Hg, and PO2 124 mm Hg. Which of the following is the most likely diagnosis?
Methemoglobinemia
CO poisoning
Hypoglycemic syncope
Hydrocarbon poisoning
Opioid overdose
89) A 51-year-old man presents to the ED complaining of nausea and abdominal pain after drinking some “bitter stuff.” He is considered one of the “regulars” who is usually at triage with ethanol intoxication. His temperature is 97.9°F, BP is 130/65 mmHg, HR is 90 beats per minute, RR is 16 breaths per minute, and oxygen saturation is 97% on room air. Physical examination is unremarkable, except for slurred speech and the smell of acetone on the patient’s breath. Laboratory results reveal serum sodium 138 mEq/L, potassium 3.5 mEq/L, chloride 105 mEq/L, bicarbonate 23 mEq/L, BUN 10 mg/dL, creatinine 2.1 mg/dL, glucose 85 mg/dL, arterial blood pH 7.37, and lactate 1.4 mEq/L. Urinalysis shows moderate ketones. Which of the following is the most likely diagnosis?
DKA
Ethylene glycol intoxication
Ethanol intoxication
Methanol intoxication
Isopropyl alcohol intoxication
90) A 55-year-old man presents to the ED 6 hours after ingesting two bottles of his baby aspirin. He complains of nausea, vomiting, dizziness, and tinnitus. His temperature is 100.3°F, BP is 140/80 mmHg, HR is 105 beats per minute, RR is 31 breaths per minute, and oxygen saturation is 99% on room air. Arterial blood gas on room air reveals a pH of 7.52, PCO2 10 mmHg, and PO2 129 mmHg. The blood salicylate level returns at 45 mg/dL. Which of the following is the most appropriate next step in management?
Administer activated charcoal, begin IV hydration, and administer sodium bicarbonate
Administer activated charcoal, begin IV hydration, and administer NAC
Administer activated charcoal, begin IV hydration, and intubate the patient for respiratory failure
Arrange for immediate hemodialysis
Gastric lavage, IV hydration, and repeat levels before beginning therapy
91) A 40-year-old man with a known history of ethanol abuse states that 2 hours ago he ingested two bottles of extra strength Tylenol. The patient has no medical complaints except for some nausea. At 4 hours post ingestion, you send blood to the laboratory to measure the serum acetaminophen concentration. The level returns and falls above the treatment line when you plot it on the APAP nomogram. You administer activated charcoal and decide to start IV NAC. Which of the following is a known adverse effect of IV NAC administration?
Hepatic failure
Confusion
Anaphylactoid reaction
Hypertensive crisis
Change in urine color
92) A 19-year-old woman presents to the ED with abdominal pain, nausea, vomiting, diarrhea, and hematemesis after ingesting an unknown substance in a suicide attempt. Which of the following antidotes are correctly paired?
Organophosphate—Physostigmine
Acetaminophen overdose—Naloxone
Iron overdose—Deferoxamine
Aspirin overdose—NAC
Acetaminophen overdose—Naloxone
93) A 34-year-old woman presents to the ED after ingesting an unknown quantity of her antidepressant pills. EMS workers found an empty bottle of amitriptyline on her apartment floor. She is awake but appears delirious. Her BP is 130/65 mmHg, HR is 101 beats per minute, temperature is 99.1°F, RR is 16 breaths per minute, and oxygen saturation is 100% on room air. On examination, her pupils are 7 mm and reactive. Her face is flushed and mucous membranes are dry. Her lungs are clear and heart is without murmurs. The abdomen is soft, nontender, and with decreased bowel sounds. She is moving all four extremities. ECG reveals sinus rhythm at a rate of 99 and QRS just under 100 milliseconds. In a TCA overdose, which of the following is responsible for her mydriasis, dry mucous membranes, and delirium?
Sodium channel blockade
α-Receptor blockade
Muscarinic receptor blockade
Inhibition of serotonin and norepinephrine reuptake
Histamine receptor blockade
94) An asymptomatic young adult was brought to the ED by a police officer after his home was raided. The patient swallowed five small packets of an unknown substance before being arrested. His BP is 125/75 mmHg, HR is 85 beats per minute, temperature is 98.7°F, and RR is 16 breaths per minute. Physical examination is unremarkable. An abdominal radiograph confirms intraluminal small bowel densities. Which of the following is the most appropriate treatment?
Magnesium citrate
NAC
Gastric lavage
Activated charcoal and polyethylene glycol
Syrup of ipecac
95) A 33-year-old woman presents to the ED with a painful sprained ankle. She has a past medical history of depression for which she is taking phenelzine, a monoamine oxidase inhibitor. After you place an elastic wrap on her ankle, she asks you to prescribe her some pain medication. Which of the following medications is contraindicated in patients taking a monoamine oxidase inhibitor?
Ibuprofen
Hydrocodone
Acetaminophen
Meperidine
Oxycodone
96) A 27-year-old woman presents to the ED 6 hours after the onset of body aches, abdominal cramping, and diarrhea. She is currently visiting relatives and normally lives in another state. She regularly takes six to eight tablets daily of hydrocodone for chronic low-back pain, sumatriptan for migraines, and amitriptyline and paroxetine for bulimia nervosa. Her BP is 130/80 mmHg, HR is 100 beats per minute, temperature is 98.6°F, RR is 16 breaths per minute, and oxygen saturation is 99% on room air. Examination shows diaphoresis, dilated pupils, and piloerection. Neurologically she is moving all four extremities and you do not note tremors. She is alert and cooperative but seems restless. She denies hallucinations or suicidal ideations. She becomes very angry when you ask her for the phone numbers of her regular physicians. Which of the following is the most likely explanation of her symptoms?
Anticholinergic overdose
Opiate withdrawal
TCA intoxication
Ethanol withdrawal
Serotonin syndrome
97) A 58-year-old woman is brought to the emergency department (ED) by emergency medical service (EMS) after slipping on a patch of ice while walking to work and hitting her head on the cement pavement. Bystanders acknowledged that the patient was unconscious for approximately 1 minute. On arrival, her vital signs are blood pressure (BP) 155/75 mmHg, heart rate (HR) 89 beats per minute, respiratory rate (RR) 18 breaths per minute, and pulse oxygenation 98% on room air. She has a 5-cm laceration to the back of her head that is actively bleeding. You ask the patient what happened but she cannot remember. You inform her that she is in the hospital as a result of a fall. Over the next 10 minutes she asks you repeatedly what happened and where she is. You do not find any focal neurologic deficits. As you bring the patient to the CT scanner, she vomits once. CT results show a normal brain scan. Which of the following is the most likely diagnosis?
Cerebral concussion
Trauma-induced Alzheimer disease
Diffuse axonal injury
Cerebral contusion
Posttraumatic epilepsy
98) A 41-year-old man, the restrained driver in a high-speed motor vehicle collision, is brought to the ED by EMS. The patient is breathing without difficulty with bilateral and equal breaths sounds. He has strong pulses peripherally indicating a BP of at least 90 mmHg. The HR is 121 beats per minute. His Glasgow coma scale (GCS) is 14. A secondary survey reveals chest wall bruising. You suspect a cardiac injury. Which of the following locations most commonly involve cardiac contusions?
Right atrium
Septum
Right ventricle
Left atrium
Left ventricle
99) A 25-year-old man is brought into the trauma resuscitation room after his motorcycle is struck by another vehicle. EMS reports that the patient was found 20 ft away from his motorcycle, which was badly damaged. His vital signs include a BP of 90/60 mmHg, HR 115 beats per minute, RR 22 breaths per minute, and pulse oxygenation of 100% on facemask. Which of the following is the smallest amount of blood loss that produces a decrease in the systolic BP in adults?
Loss of 5% of blood volume
Loss of greater than 40% of blood volume
Loss of 10% of blood volume
Loss of 15% to 30% of blood volume
Loss of 30% to 40% of blood volume
100) You are notified by the EMS dispatcher that there is a multiple-car collision on the local highway with many injuries. He states that there are two people dead at the scene, one person is critically injured and hypotensive, and three people have significant injuries but with stable vital signs. Which of the following is the leading cause of death and disability in trauma victims?
Abdominal injury
Head injury
Thoracic injury
Back injury
Cervical injury
101) Paramedics bring a 17-year-old high school football player to the ED on a backboard and with a cervical collar. During a football game, the patient “speared” another player with his helmet and subsequently experienced severe neck pain. He denies paresthesias and is able to move all of his extremities. A cervical spine CT scan reveals multiple fractures of the first cervical vertebra. Which of the following best describes this fracture?
Odontoid fracture
Jefferson fracture
Hangman’s fracture
Clay shoveler’s fracture
Teardrop fracture
102) A 20-year-old man presents to the ED with multiple stab wounds to his chest. His BP is 85/50 mmHg and HR is 123 beats per minute. Two large-bore IVs (intravenous) are established and running wide open. On examination, the patient is mumbling incomprehensibly, has good air entry on lung examination, and you notice jugular venous distension (JVD). As you are listening to his heart, the nurse calls out that the patient has lost his pulse and that she cannot get a BP reading. Which of the following is the most appropriate next step in management?
Atropine
Pericardiocentesis
Epinephrine
ED thoracotomy
Bilateral chest tubes
103) A 22-year-old man calls the ED from a local bar stating that he was punched in the face 10 minutes ago and is holding his front incisor tooth in his hand. He wants to know what the best way is to preserve the tooth. Which of the following is the most appropriate advice to give the caller?
Place the tooth in a napkin and bring it to the ED
Place the tooth in a glass of water and bring it to the ED
Place the tooth in a glass of beer and bring it to the ED
Pour some water over the tooth and place it immediately back into the socket
Place the tooth in a glass of milk and bring it to the ED
104) A 19-year-old man is brought into the trauma room by EMS after a head-on cycling accident. The patient was not wearing a helmet. Upon presentation his BP is 125/75 mmHg, HR is 105 beats per minute, RR is 19 breaths per minute, and oxygen saturation is 100% on mask. His eyes are closed but open to command. He can move his arms and legs on command. When you ask him questions, he is disoriented but able to converse. What is this patient’s GCS score?
11
15
12
13
14
105) An 18-year-old man presents to the ED after getting stabbed in his abdomen. His HR is 140 beats per minute and BP is 90/40 mmHg. He is yelling that he is in pain. Two large-bore IVs are inserted into his antecubital fossa and fluids are running wide open. After 2 L of fluids, his BP does not improve. Which of the following is the most common organ injured in stab wounds?
Liver
Spleen
Small bowel
Stomach
Colon
106) A 61-year-old man presents to the ED with chest wall pain after a motor vehicle collision. He is speaking full sentences, breath sounds are equal bilaterally, and his extremities are well-perfused. His BP is 150/75 mmHg, HR is 92 beats per minute, and oxygen saturation is 97% on room air. Chest radiography reveals fractures of the seventh and eighth ribs of the right anterolateral chest. He has no other identifiable injuries. Which of the following is the most appropriate treatment for this patient’s rib fractures?
Insert a chest tube into the right thorax
Apply adhesive tape on the chest wall perpendicular to the rib fractures
Bring the patient to the OR for surgical fixation
Analgesia and incentive spirometry
Observation
107) A 27-year-old man brought to the ED by paramedics after a motor vehicle collision. His RR is 45 breaths per minute, oxygen saturation is 89%, HR is 112 beats per minute, and BP is 115/75 mmHg. You auscultate his chest and hear decreased breath sounds on the left. Which of the following is the most appropriate next step in management?
Order a stat chest radiograph
Perform a tube thoracostomy
Perform a pericardiocentesis
Perform a diagnostic peritoneal lavage (DPL)
Perform an ED thoracotomy
108) A 29-year-old man is brought to the ED by EMS after being stabbed in the left side of his back. His BP is 120/80 mmHg, HR is 105 beats per minute, RR is 16 breaths per minute, and oxygen saturation is 98% on room air. On the secondary survey, you note motor weakness of his left lower extremity and the loss of pain sensation in the right lower extremity. Which of the following is the most likely diagnosis?
Spinal shock
Brown-Sequard syndrome
Central cord syndrome
Anterior cord syndrome
Cauda equina syndrome
109) A 33-year-old man, who was drinking heavily at a bar, presents to the ED after getting into a fight. A bystander tells paramedics that the patient was punched and kicked multiple times and sustained multiple blows to his head with a stool. In the ED, his BP is 150/75 mmHg, HR is 90 beats per minute, RR is 13 breaths per minute, and oxygen saturation is 100% on non-rebreather. On examination, he opens his eyes to pain and his pupils are equal and reactive. There is a laceration on the right side of his head. He withdraws his arm to pain but otherwise does not move. You ask him questions, but he just moans. Which of the following is the most appropriate next step in management?
Prepare for intubation
Neurosurgical intervention
Suture repair of head laceration
Administer mannitol
Bilateral burr holes
110) A 74-year-old man presents to the ED after being involved in a motor vehicle collision. He states he was wearing his seat belt in the driver’s seat when a car hit him from behind. He thinks his chest hit the steering wheel and now complains of pain with breathing. His RR is 20 breaths per minute, oxygen saturation is 98% on room air, BP is 145/75 mmHg, and HR is 90 beats per minute. On examination, you notice paradoxical respirations. Which of the following best describes a flail chest?
One rib with three fracture sites
Three adjacent ribs, each with two fracture sites
Two adjacent ribs, each with two fracture sites
Two fractured right-sided ribs and two fractured left-sided ribs
One fractured right-sided rib and one fractured left-sided rib
111) A 29-year-old man presents to the ED after being stabbed in his neck. The patient is speaking in full sentences. His breath sounds are equal bilaterally. His BP is 130/75 mmHg, HR is 95 beats per minute, RR is 16 breaths per minute, and oxygen saturation is 99% on room air. The stab wound is located between the angle of the mandible and the cricoid cartilage and violates the platysma. There is blood oozing from the site although there is no expanding hematoma. Which of the following is the most appropriate next step in management?
Explore the wound and blind clamp any bleeding site
Apply direct pressure and bring the patient immediately to the OR to explore the zone I injury
Probe the wound looking for injured vessels
Apply direct pressure and bring the patient immediately to the OR to explore the zone II injury
Apply direct pressure and bring the patient immediately to the OR to explore the zone III injury
112) A 45-year-old man is brought to the ED after a head-on motor vehicle collision. Paramedics at the scene tell you that the front end of the car is smashed. The patient’s BP is 130/80 mmHg, HR is 100 beats per minute, RR is 15 breaths per minute, and oxygen saturation is 98% on room air. Radiographs of the cervical spine reveal bilateral fractures of the C2 vertebra. The patient’s neurologic examination is unremarkable. Which of the following best describes this fracture?
Colles fracture
Jefferson fracture
Boxer’s fracture
Hangman’s fracture
Clay shoveler’s fracture
113) A 71-year-old man is found lying on the ground one story below the balcony of his apartment. Paramedics bring the patient into the ED. He is cool to touch with a core body temperature of 96°F. His HR is 119 beats per minute and BP is 90/70 mmHg. His eyes are closed, but they open when you call his name. His limbs move to stimuli, and he answers your questions but is confused. On examination, you note clear fluid dripping from his left ear canal and an area of ecchymosis around the mastoid bone. Which of the following is the most likely diagnosis?
Le Fort fracture
Otitis interna
Otitis externa
Tripod fracture
Basilar skull fracture
114) A 34-year-old construction worker is brought to the ED by EMS after falling 30 ft from a scaffold. His vital signs are HR 124 beats per minute, BP 80/40 mmHg, and oxygen saturation 93% on 100% oxygen. He has obvious head trauma with a scalp laceration overlying a skull fracture on his occiput. He does not speak when asked his name, his respirations are poor, and you hear gurgling with each attempted breath. Auscultation of the chest reveals diminished breath sounds on the right. There is no JVD or anterior chest wall crepitus. His pelvis is unstable with movement laterally to medially and you note blood at the urethral meatus. His right leg is grossly deformed at the knee and there is an obvious fracture of his left arm. Which of the following is the most appropriate next step in management?
Insert a 32F chest tube into the right thoracic cavity
Create two Burr holes into the cranial vault to treat a potential epidural hematoma
Perform a DPL to rule out intra-abdominal hemorrhage
Immediately reduce the extremity injuries and place in a splint until the patient is stabilized
Plan for endotracheal intubation of the airway with in-line stabilization of the cervical spine

115) A 20-year-old man was found on the ground next to his car after it hit a tree on the side of the road. Bystanders state that the man got out of his car after the collision but collapsed within a few minutes. Paramedics subsequently found the man unconscious on the side of the road. In the ED, his BP is 175/90 mmHg, HR is 65 beats per minute, temperature is 99.2°F, RR is 12 breaths per minute, and oxygen saturation is 97% on room air. Physical examination reveals a right-sided fixed and dilated pupil. A head CT is shown below. Which of the following is the most likely diagnosis?
Epidural hematoma
Cerebral contusion
Subdural hematoma
Subarachnoid hemorrhage (SAH)
Intracerebral hematoma
116) An 81-year-old woman presents to the ED after tripping over the sidewalk curb and landing on her chin causing a hyperextension of her neck. She was placed in a cervical collar by paramedics. On examination, she has no sensorimotor function of her upper extremities. She cannot wiggle her toes, has 1/5 motor function of her quadriceps, and only patchy lower extremity sensation. Rectal examination reveals decreased rectal tone. Which of the following is the most likely diagnosis?
Central cord syndrome
Exacerbation of Parkinson disease
Anterior cord syndrome
Brown-Sequard syndrome
Transverse myelitis
117) A 22-year-old man presents to the ED after being ejected from his vehicle following a high-speed motor vehicle collision. Upon arrival, his BP is 85/55 mmHg and HR is 141 beats per minute. Two large-bore IVs are placed in the antecubital veins and lactated Ringer solution is being administered. After 3 L of crystalloid fluid, the patient’s BP is 83/57 mmHg. Which of the following statements is most appropriate regarding management of a hypotensive trauma patient who fails to respond to initial volume resuscitation?
It is important to wait for fully cross-matched blood prior to transfusion
Blood transfusion should begin after 4 L of crystalloid infusion
Whole blood should be used rather than packed red blood cells (RBCs)
Type O blood that is Rh-negative should be transfused
Type O blood that is Rh-positive should be transfused
118) A 24-year-old man is brought into the ED by paramedics after being run over by a car. His systolic BP is 90 mmHg by palpation, HR is 121 beats per minute, RR is 28 breaths per minute, and oxygen saturation is 100% on non-rebreather. The airway is patent and breath sounds are equal bilaterally. You establish large-bore access and fluids are running wide open. Secondary survey reveals an unstable pelvis upon movement with lateral to medial force. Bedside focused abdominal sonography for trauma (FAST) is negative for intraperitoneal fluid. Which of the following is the most appropriate immediate next step in management?
Bilateral chest tubes
Angiographic embolization
Application of external fixator
Application of pelvic binding apparatus
Venographic embolization
119) A 32-year-old man is brought to the ED by paramedics after a diving accident. The lifeguard on duty accompanies the patient and states that he dove head first into the shallow end of the pool and did not resurface. On examination, the patient is speaking but cannot move his arms or legs and cannot feel pain below his clavicle. He is able to feel light touch and position of his four extremities. A cervical spine radiograph does not reveal a fracture. Which of the following is the most likely diagnosis?
Spinal cord injury without radiographic abnormality (SCIWORA)
Anterior cord syndrome
Central cord syndrome
Cauda equina syndrome
Brown-Sequard syndrome
120) A 22-year-old man is brought to the ED 20 minutes after a head-on motor vehicle collision in which he was the unrestrained driver. On arrival, he is alert and coherent but appears short of breath. His HR is 117 beats per minute, BP is 80/60 mmHg, and oxygen saturation is 97% on a nonrebreather. Examination reveals bruising over the central portion of his chest. His neck veins are not distended. Breath sounds are present on the left but absent on the right. Following administration of 2 L of lactated Ringer solution, his systolic BP remains at 80 mmHg. Which of the following is the most appropriate next step in management?
Sedate, paralyze, and intubate
Perform a needle thoracostomy
Perform a pericardiocentesis
Perform a DPL
Perform a FAST examination
121) An 87-year-old man is brought to the ED on a long board and in a cervical collar after falling down a flight of steps. He denies losing consciousness. On arrival, his vital signs include an HR of 99 beats per minute, BP of 160/90 mmHg, and RR of 16 breaths per minute. He is alert and speaking in full sentences. Breath sounds are equal bilaterally. Despite an obvious right arm fracture, his radial pulses are 2+ and symmetric. When examining his cervical spine, he denies tenderness to palpation and you do not feel any bony deformities. Which of the following is a true statement?
Epidural hematomas are very common in the elderly age population
Increased elasticity of their lungs allows elderly patients to recover from thoracic trauma more quickly than younger patients
Cerebral atrophy in the elderly population provides protection against subdural hematomas
The most common cervical spine fracture in this age group is a wedge fracture of the sixth cervical vertebra.
Despite lack of cervical spine tenderness, imaging of his cervical spine is warranted
122) A 45-year-old man is brought into the ED after a head-on motor vehicle collision. His BP is 85/45 mmHg and HR is 130 beats per minute. He is speaking coherently. His breath sounds are equal bilaterally. After 2 L of fluid resuscitation, his BP is 80/40 mmHg. A FAST examination reveals fluid in Morison pouch. Which of the following organs is most likely to be injured in blunt abdominal trauma?
Liver
Bladder
Spleen
Kidney
Small bowel
123) A 47-year-old man is brought into the ED after falling 20 ft from a ladder. His HR is 110 beats per minute, BP is 110/80 mmHg, RR is 20 breaths per minute, and oxygen saturation is 100% on face mask. He is able to answer your questions without difficulty. His chest is clear with bilateral breath sounds, abdomen is nontender, pelvis is stable, and the FAST examination is negative. You note a large scrotal hematoma and blood at the urethral meatus. Which of the following is the most appropriate next step in management?
Scrotal ultrasound
Retrograde urethrogram
Kidney-ureter-bladder (KUB) radiograph
IV pyelogram
Retrograde cystogram
124) A 17-year-old man presents to the ED after getting hit in the right eye with a tennis ball during a tennis match. On arrival to the ED, you note periorbital swelling and ecchymosis. The patient’s visual acuity is 20/20. When you are testing his extraocular muscles, you note that his right eye cannot look superiorly but his left eye can. He also describes pain in his right eye when attempting to look upward. Which of the following is the most likely diagnosis?
Zygomatic arch fracture
Ruptured globe
Orbital floor fracture
Retrobulbar hematoma
Mandible fracture with entrapment of the pterygoid
125) A 24-year-old man is brought to the ED after being shot once in the abdomen. On arrival, his BP is 100/60 mmHg, HR is 115 beats per minute, and RR is 22 breaths per minute. His airway is patent and you hear breath sounds bilaterally. On abdominal examination, you note a single bullet entry wound approximately 1 cm to the right of the umbilicus. During the log roll, you see a single bullet exit wound approximately 3 cm to the right of the lumbar spine. His GCS score is 15. The patient’s BP is now 85/65 mmHg and HR is 125 beats per minute after 2L of fluid. Which of the following is the most appropriate next step in management?
Probe the entry wound to see if it violates the peritoneum
Perform a DPL
Perform a FAST examination
Take the patient directly to the CT scanner
Take the patient directly to the OR
126) A 43-year-old man, who currently uses drugs intravenously (IV), presents to the emergency department (ED) with 2 weeks of fever, back pain, and progressive weakness in his legs bilaterally. He denies any history of trauma or prior surgery. His blood pressure (BP) is 130/75 mmHg, heart rate (HR) is 106 beats per minute, temperature is 103°F, and respiratory rate (RR) is 16 breaths per minute. On physical examination, he has tenderness to palpation in the mid-lumbar spine, increased patellar reflexes, and decreased strength in the lower extremities bilaterally, with normal range of motion. Laboratory results reveal a white blood cell (WBC) count of 15,500/μL, hematocrit 40%, and platelets 225/μL. Urinalysis and spinal x-rays are unremarkable. Which of the following is the most likely diagnosis?
Fibromyalgia
Spinal metastatic lesion
Ankylosing spondylitis
Spinal epidural abscess
Vertebral compression fracture
127) An 81-year-old woman is brought to the ED by her children who state that the patient is acting more tired than usual, has had fever for the last 2 days, and is more confused. Ordinarily, the patient is high functioning: she is ambulatory, cooks for herself, and walks on a treadmill 30 minutes a day. Her vital signs are BP 85/60 mmHg, HR 125, RR 20, temperature 101.3°F, and pulse oxygenation 97% on room air. On examination, the patient has dry mucous membranes but is otherwise unremarkable. She is oriented to person and place but states that the year is 1925. Her laboratory results show a WBC 14,300/μL, hematocrit 31%, and platelets 350/μL. Her electrolytes are within normal limits. Blood glucose is 92 mg/dL. A chest radiograph does not show any infiltrates. Urinalysis reveals 2+ protein, trace ketones, WBC > 100/hpf, red blood cell (RBC) 5 to 10/hpf, nitrite positive, and leukocyte esterase positive. After administering a 500-cc normal saline fluid bolus and broad-spectrum antibiotics through her peripheral IV line, the patient’s BP is 82/60 mmHg. You suspect that the patient is in septic shock due to an acute urinary tract infection. Which of the following is the next most appropriate course of action to manage this patient with earlygoal-directed therapy (EGDT)?
Immediately start a norepinephrine infusion to increase the blood pressure given the low systolic blood pressure
Prepare to transfuse uncrossed matched packed RBC to increase oxygen-carrying capacity given the low hematocrit
. Place a central venous line into the right internal jugular vein to measure central venous pressure (CVP)
Transport the patient to radiology for a stat CT scan of her head given the acute change in mental status
Place a central venous line into the right internal jugular vein to measure mixed venous oxygen saturation (SVO2)
128) A 23-year-old man presents to the ED with left lower abdominal pain and left testicular pain that started 1 to 2 weeks ago and has gradually worsened. He has some nausea and vomiting. His HR is 98 beats per minute, BP is 125/65 mmHg, temperature is 100.9°F, and RR is 18 breaths per minute. Physical examination reveals a tender left testicle with a firm nodularity on the posterolateral aspect of the testicle. Pain is relieved slightly with elevation of the testicle and the cremasteric reflex in normal. You make the presumptive diagnosis of epididymitis. Which of the following is the next best step?
Prescribe pain medications and penicillin for coverage of syphilis, the most likely causative organism
Give ceftriaxone 125 mg intramuscularly (IM), plus a one-time dose of azithromycin 1g orally
Recommend bed rest, ice, and scrotal elevation with prompt urology follow-up
Give ceftriaxone 250 mg intramuscularly (IM), plus a 10-day course of oral doxycycline
Confirm the diagnosis with transillumination of the testicle, and then consult urology for surgical drainage
129) A 40-year-old man with insulin-dependent diabetes presents to the ED with complaints of 2 days of increasingly severe perineal pain and subjective fevers. His HR is 118 beats per minute, BP is 95/55 mmHg, temperature is 103.4°F, and RR is 22 breaths per minute. The bedside sugar reading is “high.” Physical examination demonstrates crepitus over the medial thigh and widespread erythema and purple discoloration with sharp demarcation over the scrotum. The scrotum is markedly tender, warm, and edematous. Which of the following is the most likely diagnosis?
Cutaneous candidiasis
Testicular torsion
Fournier syndrome
Phimosis
Paraphimosis
130) A 55-year-old man with a history of diabetes presents with complaints of developed left knee pain several days following a fall from standing height. The patient was brought to the ED by ambulance after being found on a park bench stating he was unable to walk because of the pain. On physical examination, there are no rashes or external signs of trauma. His left knee is warm, diffusely tender, and swollen with a large effusion. He has pain on passive range of motion and is refusing to walk. His BP is 150/85 mmHg, HR is 105 beats per minute, temperature is 102.7°F, RR is 16 breaths per minute, and fingerstick glucose is 89 mg/dL. Which of the following is the most appropriate diagnostic test?Knee radiographs
Knee radiographs
Arthrocentesis
Magnetic resonance imaging (MRI)
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
Bone scan
131) A 35-year-old woman with systemic lupus erythematosus (SLE) is brought to the ED by her brother after he found her febrile and confused. Physical examination reveals fever, tachycardia, a waxing and waning mental status, petechiae over her oral mucosa, pallor, and mildly heme-positive stool. Her urinalysis is positive for blood, red cell casts, and proteinuria. Laboratory results reveal blood urea nitrogen (BUN) of 40 mg/dL and creatinine of 2 mg/dL. Her bilirubin is elevated (unconjugated > conjugated) and her international normalized ratio (INR) is 0.98. Her complete blood count reveals WBC 12,000/μL, hematocrit 29%, and platelet count 17,000/μL with schistocytes on the peripheral smear. Which of the following is the most appropriate next step in management?
Admit to the intensive care unit (ICU) for plasmapheresis and close monitoring for acute bleeds
. Admit to the ICU for corticosteroid infusion, transfusion of platelets, and prompt surgical consultation for emergent splenectomy
Admit to the ICU for platelet transfusion and monitoring for acute bleeds
Admit to the ICU for dialysis and close monitoring for acute bleeds
Perform a noncontrast head computed tomography (CT) to screen for intracranial bleeding and mass effect followed by a lumbar puncture (LP) for analysis of cerebrospinal fluid (CSF). If negative, admit to telemetry for hemodynamic monitoring
132) A 30-year-old woman presents to the ED with fever, headache, a “sunburn-like” rash, and confusion. A friend states that the patient has complained of nausea, vomiting, diarrhea, and a sore throat over the past few days. Her last menstrual period began 4 days ago. Vital signs are HR 110 beats per minute, BP 80/45 mmHg, RR of 18 breaths per minute, and temperature of 103°F. On physical examination, you note an ill-appearing woman with a diffuse blanching erythroderma. Her neck is supple without signs of meningeal irritation. On pelvic examination, you remove a tampon. You note a fine desquamation of her skin, especially over the hands and feet, and hyperemia of her oropharyngeal, conjunctival, and vaginal mucous membranes. Laboratory results reveal a creatine phosphokinase (CPK) of 5000, WBC 15,000/μL, platelets of 90,000/μL, BUN 40 mg/dL, creatinine 2 mg/dL, and elevated liver enzymes. You suspect thediagnosis of toxic shock syndrome and initiate IV fluids. You target antibiotics at which of the following causative organism?
Staphylococcus aureus
Neisseria gonorrhoeae
Rickettsia rickettsii
Streptococcus pyogenes
Neisseria meningitidis
133) A 32-year-old diabetic man presents to the ED with a fever and 1 week of increasing right foot pain. He states he stepped on a nail while running barefoot 2 weeks ago but didn’t think much of it at that time. On physical examination, his heel is mildly erythematous and diffusely tender to palpation, with overlying warmth and edema. There is a small amount of purulent drainage through the puncture hole in his heel. A plain radiograph of his foot demonstrates a slight lucency of the calcaneus. He has decreased range of motion, but you are able to passively dorsiflex and plantarflex his ankle without difficulty. His vital signs include a temperature of 101.4°F, HR of 98 beats per minute, BP of 130/75 mmHg, and RR of 16 breaths per minute. Which of the following is the most common causative organism of this condition?
Salmonella sp
Pasteurella multocida
Pseudomonas aeruginosa
Staphylococcus aureus
Group B streptococci
134) A 75-year-old woman is transferred to your ED from the local nursing home for fever, cough, and increasing lethargy. Over the past 3 days, the nursing home staff noticed increasing yellow sputum and decreasing urine output from the patient. Her BP is 118/75 mmHg, RR is 20 breaths per minute, HR is 105 beats per minute, temperature is 100.9°F, and pulse oxygenation is 94% on room air. On examination, auscultation of the lungs reveals bibasilar crackles. Laboratory results reveal WBC 14,500/μL, hematocrit 39%, platelets 250/μL, sodium 132 mEq/L, potassium 3.5 mEq/L, chloride 100 mEq/L, bicarbonate 18 mEq/L, BUN 27 mg/dL, creatinine 1.5 mg/dL, and glucose 85 mg/dL. Serum lactate is 4.7 mmol/dL. Chest radiography reveals bilateral lower lobe infiltrates. Based on this patient’s presentation, which of the following is the most likely diagnosis?
Hospital-acquired pneumonia (HAP)
Health care–associated pneumonia (HCAP)
Community-acquired pneumonia (CAP)
Ventilator-associated pneumonia (VAP)
Atypical pneumonia
135) A 55-year-old man presents to the ED with fever, drooling, trismus, and a swollen neck. He reports a foul taste in his mouth caused by a tooth extraction 2 days ago. On physical examination, the patient appears anxious. He has bilateral submandibular swelling and elevation and protrusion of the tongue. He appears “bull-necked” with tense and markedly tender edema and brawny induration of the upper neck, and he is tender over the lower second and third molars. There is no cervical lymphadenopathy. These lungs are clear to auscultation with good air movement. His vital signs are HR 105 beats per minute, BP 140/85 mmHg, RR 26 breaths per minute, and temperature 102°F. Which of the following is the most appropriate next step in management?
Obtain a sample for culture, administer a dose of IV antibiotics, and obtain a soft tissue radiograph of the neck
Administer a dose of IV antibiotics and obtain a CT scan of the soft tissues of the neck
Obtain a sample for culture, perform a broad incision and drainage at bedside, and administer a dose of IV antibiotics
Administer a dose of IV antibiotics, obtain a CT scan of the soft tissues of the neck, and obtain an emergent ENT consult
Secure his airway, administer a dose of IV antibiotics, and obtain an emergent ENT (ear, nose, and throat) consult
136) A 67-year-old woman with a history of steroid-dependent COPD, non–insulin-dependent diabetes, and hypertension presents to the ED with complaints of a painful, red, swollen left lower leg. She states she noted a “bug bite” in that area 1 week ago and since then has had gradually increasing symptoms. On examination, you note a 12 cm × 10 cm sharply demarcated area of blanching erythema, warmth, and tenderness on the medial thigh with ascending erythema to the groin. You also note tender adenopathy in the left inguinal region. Her BP is 90/55 mmHg, RR is 24 breaths per minute, HR is 105 beats per minute, temperature is 102.4°F, and pulse oxygenation is 98% on room air. Laboratory results reveal WBC 19,500/μL, hematocrit 39%, platelets 175/μL, sodium 132 mEq/L, potassium 3.5 mEq/L, chloride 100 mEq/L, bicarbonate 14 mEq/L, BUN 32 mg/dL, creatinine 1.7 mg/dL, and glucose 455 mg/dL. Serum lactate is 4.7 mmol/dL. Which of the following best describes her clinical state?
She has systemic inflammatory response syndrome (SIRS)
She has severe sepsis
She has sepsis
She is in septic shock
She has multiple organ dysfunction syndrome
137) An 84-year-old man presents to the ED with his family due to concerns that his condition is worsening despite being placed on levofloxacin for a urinary tract infection 5 days ago by his primary care physician. His is obtunded and unable to give any additional history. Physical examination does not reveal the source of infection. His BP is 84/45 mmHg, HR is 135 beats per minute, temperature is 102.8°F, and his RR is 28 breaths per minute. Laboratory results reveal WBC 24,500/μL, hematocrit 19%, platelets 90/μL, sodium 132 mEq/L, potassium 7.5 mEq/L, chloride 100 mEq/L, bicarbonate 12 mEq/L, BUN 37 mg/dL, creatinine 6.5 mg/dL, and glucose 255 mg/dL. Serum lactate is 11.3 mmol/dL. Cardiac enzymes and troponin are mildly elevated, and he has hyperacute T-waves on electrocardiogram (ECG). His chest radiograph shows cardiomegaly with bilateral patchy opacities and pulmonary vascular congestion. Rapid urinalysis reveals 3+ WBCs and blood and nitrates. You secure his airway with intubation, initiate broad-spectrum antibiotics, IV fluids, and other supportive therapies, and emergently consult nephrology, cardiology, and pulmonology. Which of the following best describes his clinical state
He has SIRS
He has MODS
He has sepsis
He has severe sepsis
He is in septic shock
138) A 37-year-old man presents to the ED with complaints of 2 days of a sore throat and subjective fever at home. He denies cough or vomiting. His BP is 130/75 mmHg, HR is 85 beats per minute, temperature is 101°F, and his RR is 14 breaths per minute. He has diffuse tonsillar swelling and bilateral exudates with bilaterally enlarged and tender lymph nodes of the neck. Which of the following is the next best step in management
Administer penicillin and discharge the patient without further testing
Discharge the patient without treatment or further testing
Perform a rapid antigen test. If it is negative, confirm with a throat culture, and administer penicillin if the results are positive
Perform a rapid antigen test. If it is negative, administer penicillin and discharge the patient
Perform a rapid antigen test. If it is positive, administer penicillin and discharge the patient
139) A 37-year-old man who just finished a full course of penicillin for pharyngitis presents to the ED requesting to be checked out again. He states he took the antibiotics exactly as prescribed and initially felt somewhat improved, but over the last 2 to 3 days has had increased pain and progressive difficulty swallowing. His BP is 130/65 mmHg, HR is 95 beats per minute, temperature is 100.1°F, RR is 16 breaths per minute, and oxygen saturation is 99%. On examination, the patient is in no acute distress but has a fluctuant mass on the right side of his neck. You visualize a normal soft palate with swelling of the right tonsillar arch and deviation of the uvula to the left, but additional examination is limited because he is unable to open his mouth fully. Review of his records reveals a throat culture that was positive for Streptococcus. Which of the following is the most appropriate next step in management?
Attempt needle aspiration, treat him with a new course of antibiotics (either penicillin or clindamycin), and have him return in 24 hours
Give him morphine for pain control, give him a dose of IV antibiotics, and observe him in the ED for 6 hours
Admit him for incision and drainage in the OR under general anesthesia
Switch his antibiotic to clindamycin and have him return in 24 hours
Order a CT scan to visualize his neck, continue the penicillin, and have him return in 24 hours
Order a CT scan to visualize his neck, continue the penicillin, and have him return in 24 hours
Identification of viral particles on Gram stain with an elevated CSF-to-serum glucose level
A markedly elevated lymphocyte count, often exceeding 100,000 cells/mm 3 with a mildly elevated total protein level
A mildly elevated total protein level with a decreased glucose level
A mildly elevated total protein level with a WBC count of fewer than 500 cells/mm 3
Increased turbidity with marked xanthochromia
141) A 32-year-old woman presents to the ED with 7 days of vaginal discharge and pelvic pain. She is sexually active and admits to several recent “one night stands.” She denies trauma/injury and does not have any urinary or other abdominal complaints. Her HR is 85 beats per minute, BP is 135/90 mmHg, RR is 18 breaths per minute, and temperature is 101.4°F. On bimanual examination, you note a copious, thin, white discharge with mild diffuse adnexal tenderness with significant cervical motion tenderness. There are no rashes, skin lesions, or adenopathy. Laboratory results are notable for a WBC of 18,000/μL. A urinalysis shows WBCs but is otherwise within normal limits. Which of the following is the most appropriate next step in management?
Prescribe her a 14-day course of levofloxacin (500 mg PO once per day) and urgent gynecology follow-up within 1 week
Give her a dose of metronidazole (2 g PO) and prescribe her a 14-day course of cephalexin (500 mg) with urgent gynecology follow-up within 1 week
Give her a one-time dose of oral metronidazole (2 g PO), azithromycin (1 g PO), and ceftriaxone (250 mg IM) with gynecology follow-up if she is not feeling better
Give her a one-time dose azithromycin (1 g PO), and ceftriaxone (250 mg IM) with urgent gynecology follow-up within 1 week
Give her a dose of ceftriaxone (250 mg IM), and prescribe her a 10-day course of doxycycline (100 mg PO BID) with urgent gynecology follow-up within 1 week
142) A 45-year-old woman presents to the ED complaining of 3 days of fever and worsening throat pain and painful odynophagia without cough or coryza. She sits on a chair, leaning forward with her mouth slightly open. She is refusing to swallow and has a cup of saliva and a box of facial tissues at her side. Vitals are HR of 120 beats per minute, BP of 110/70 mmHg, RR of 22 breaths per minute, oxygen saturation of 99% on room air, and temperature of 102.8°F. You note a slight wheezing noise coming from her anterior neck. Her voice is hoarse and she is able to open her mouth fully, making her examination quite difficult. From what you can visualize, her posterior oropharynx is moderately hyperemic, without exudates or tonsillar enlargement. A soft tissue lateral cervical radiograph shows marked edema of the prevertebral soft tissues and absence of the vallecular space. Which of the following is the most likely diagnosis?
Retropharyngeal abscess
Laryngotracheitis
Peritonsillar abscess
Epiglottitis
Pharyngitis
143) A 19-year-old woman presents with 4 days of bilateral lower abdominal pain right greater than left. She also complains of a fever, nausea, vomiting, and general malaise. Her last menstrual period was 5 days ago. Vitals are HR 98 beats per minute, BP 110/65 mmHg, RR 18 breaths per minute, and temperature of 102.7°F. Pelvic examination demonstrates exquisite cervical motion tenderness and right adnexal tenderness. Laboratory reports are notable for a WBC 15,000/μL, an ESR of 95 mm/h, and a negative urine β-human chorionic gonadotropin (β-hCG). Transvaginal ultrasound demonstrates a right complex mass with cystic and solid components. Which of the following is the most appropriate next step in management?
. Prescribe her a 14-day course of levofloxacin (500 mg PO once per day) and urgent gynecology follow-up within 1 week
. Give her a dose of metronidazole (2 g PO) and prescribe her a 14-day course of cephalexin (500 mg) with urgent gynecology follow-up within 1 week
. Give her a one-time dose of oral metronidazole (2 g PO), azithromycin (1 g PO), and ceftriaxone (250 mg IM) with gynecology follow-up if she is not feeling better
. Given her a one-time dose with emergent gynecology consultation for possible laparoscopic drainage
. Give her a dose of ceftriaxone (250 mg IM), and prescribe her a 10-day course of doxycycline (100 mg PO BID) with urgent gynecology follow-up within 1 week
144) A 42-year-old IV drug user presents to the ED with fever, chills, pleuritic chest pain, myalgias, and general malaise. The patient’s vitals include an HR of 110 beats per minute, BP of 110/65 mmHg, RR of 18 breaths per minute, and temperature of 103.4°F. Physical examination is notable for retinal hemorrhages, petechiae on the conjunctivae and mucous membranes, a faint systolic ejection murmur, and splenomegaly. Which of the following is the most likely diagnosis?
Disseminated gonorrhea
Endocarditis
Myocarditis
Pericarditis
Infectious mononucleosis
145) A 51-year-old diabetic man complains of intense right-ear pain and discharge. On physical examination, his BP is 145/65 mmHg, HR 91 beats per minute, and temperature 101°F. He withdraws when you retract the pinna of his ear. The external auditory canal is erythematous, edematous, and contains what looks like friable granulation tissue in the external auditory canal. The tympanic membrane is partially obstructed but appears to be erythematous, as well. You make the presumptive diagnosis of necrotizing (malignant) otitis externa. Which of the following statements regarding this condition is true
146) A 26-year-old woman presents to the ED with fever, malaise, and an evolving rash in the right axilla that she initially thought was from an insect bite that she received while hiking 1 week earlier. She complains of generalized fatigue, nausea, headache, and joint pain over the past several days. Her vitals are BP of 120/75 mmHg, HR of 75 beats per minute, RR of 16 breaths per minute, and temperature of 101°F. On physical examination, she is awake and alert, with a nonfocal neurologic examination. Her neck is supple, but she is diffusely tender over the shoulder, knee, and hip joints bilaterally without any distinct effusions. Her abdomen is soft and nontender. She has a 9-cm erythematous annular plaque with partial central clearing and a bright red outer border and a target center under her right axilla. Which of the following is the next best step?
Treat empirically with broad-spectrum antibiotics and consult dermatology emergently for a biopsy of the rash
Treat empirically for a cellulitis with cephalexin for 10 days and arrange follow-up with her primary care doctor
Treat empirically for Lyme disease with doxycycline for 21 days and arrange follow-up with her primary-care doctor
Treat empirically for an allergic dermatitis with prednisone, diphenhydramine, and famotidine for 3 days, and arrange follow-up with her primary care doctor
Perform serologic testing for Borrelia burgdorferi to confirm the diagnosis of Lyme disease and arrange follow-up with her primary care doctor
147) A 22-year-old man without medical complaints presents to the ED with a 3-day history of fever, malaise, and myalgias. He denies chest pain, shortness of breath, nausea or vomiting, abdominal pain, cough, sore throat, genitourinary symptoms, or respiratory tract complaints. On examination, the patient’s BP is 100/60 mmHg, HR is 110 beats per minute, RR is 20 breaths per minute, and temperature is 102°F. He appears awake, alert, and comfortable. His physical examination is normal. Which of the following is the most appropriate next step in management?
Discharge him with antipyretics and follow up with his primary care doctor in 1 or 2 days for a repeat examination
Order a CBC, urinalysis, chest x-ray, two sets of blood cultures, and perform an LP. Start empiric IV antibiotics and admit him for observation
Order a CBC, urinalysis, and chest x-ray. If normal, discharge him with antipyretics and follow up with his primary care doctor in 1 or 2 days for a repeat examination
Order a CBC, urinalysis, chest x-ray, and two sets of blood cultures. If normal, discharge him with antipyretics and follow up with his primary care doctor in 1 or 2 days for a repeat examination
Order a CBC, urinalysis, chest x-ray, two sets of blood cultures, and perform an LP. If normal, discharge him with antipyretics and follow up with his primary care doctor in 1 or 2 days for a repeat examination
148) A 54-year-old man with a history of hepatitis C, alcohol abuse, and cirrhotic ascites presents with increasing abdominal girth and abdominal pain. He complains of increasing difficulty breathing, especially when lying down, caused by worsening ascites. On physical examination, the patient is cachectic and appears older than his stated age. He has a diffusely tender abdomen and tense ascites. The liver is palpable 4 cm below the costal margin. Vitals include a BP of 110/65 mmHg, HR of 110 beats per minute, RR of 22 breaths per minute, and temperature of 102°F. Which of the following is the most common organism seen in spontaneous bacterial peritonitis?
Pseudomonas aeruginosa
Streptococcus viridans
Enterococcus
Streptococcus pneumoniae
Enterobacteriaceae
149) A 30-year-old man with type 1 diabetes presents to the emergency department (ED). His blood pressure (BP) is 100/70 mmHg and heart rate (HR) is 140 beats per minute. His blood glucose is 750 mg/dL, potassium level is 5.9 mEq/L, bicarbonate is 5 mEq/L, and arterial pH 7.1. His urine is positive for ketones. Which of the following is the best initial therapy for this patient?
Give normal saline as a 2-L bolus; then administer 20 units of regular insulin subcutaneously
Give normal saline in 2 L bolus and then administer 10 units of insulin intravenously followed by an insulin drip and continued hydration
Bolus 2 ampules of bicarbonate and administer 10 units of insulin intravenously
Give him 5 mg of metoprolol to slow down his heart, start intravenous (IV) hydration, and then give 10 units of regular insulin intravenously
Give normal saline in 2 L bolus with 20 mEq/L potassium chloride (KCl) in each bag
150) A 39-year-old woman, brought into the ED by her family, states that she has had 4 days of diarrhea and has now started acting “crazy” with mood swings and confusion. The family states that she usually takes a medication for a problem with her neck. Her BP is 130/45 mmHg, HR is 140 beats per minute, temperature is 101.5°F, and her respiratory rate (RR) is 22 breaths per minute. An electrocardiogram (ECG) reveals atrial fibrillation with a normal QRS complex. After you address the airway, breathing, and circulation (ABCs), which of the following is the most appropriate next step in management?
Administer 2 ampules of bicarbonate to treat for tricyclic antidepressant overdose
Administer ceftriaxone and prepare for a lumbar puncture
Administer chlordiazepoxide, thiamine, and folate
Administer propranolol and propylthiouracil (PTU); then wait an hour to give Lugol iodine solution
Administer ciprofloxacin and give a 2-L bolus of normal saline for treatment of dehydration secondary to infectious diarrhea
151) A 65-year-old woman brought into the ED by her family, states that she has been weak, lethargic, and saying “crazy things” over the last 2 days. Her family also states that her medical history is significant only for a disease of her thyroid. Her BP is 120/90 mmHg, HR is 51 beats per minute, temperature is 94°F rectally, and RR is 12 breaths per minute. On examination, the patient is overweight, her skin is dry, and you notice periorbital nonpitting edema. On neurologic examination, the patient does not respond to stimulation. Which of the following is the most likely diagnosis?
Apathetic thyrotoxicosis
Schizophrenia
Myxedema coma
Graves disease
Acute stroke
152) A 74-year-old woman who is a known diabetic is brought to the ED by emergency medical service (EMS) with altered mental status. The home health aide states that the patient ran out of her medications 4 days ago. Her BP is 130/85 mmHg, HR is 110 beats per minute, temperature is 99.8°F, and RR is 18 breaths per minute. On examination, she cannot follow commands but responds to stimuli. Laboratory results reveal white blood cell (WBC) count of 14,000/L, hematocrit 49%, platelets 325/L, sodium 128 mEq/L, potassium 3.0 mEq/L, chloride 95 mEq/L, bicarbonate 22 mEq/L, blood urea nitrogen (BUN) 40 mg/dL, creatinine 1.8 mg/dL, and glucose 850 mg/dL. Urinalysis shows 3+ glucose, 1+ protein, and no blood or ketones. After addressing the ABCs, which of the following is the most appropriate next step in management?
Begin fluid resuscitation with a 2- to 3-L bolus of normal saline; then administer 10 units of regular insulin intravenously
Arrange for urgent hemodialysis
Begin fluid resuscitation with a 2- to 3-L bolus of normal saline; then administer 10 units of regular insulin intravenously and begin phenytoin for seizure prophylaxis
Administer 10 units of regular insulin intravenously; then begin fluid resuscitation with a 2- to 3-L bolus of normal saline
Order a computed tomographic (CT) scan of the brain; if negative for acute stroke, begin fluid resuscitation with a 2- to 3-L bolus of normal saline
153) A 21-year-old man presents to the ED. He has a known history of type 1 diabetes. He is hypotensive with BP of 95/65 mmHg, tachycardic at 120 beats per minute, and tachypneic at 30 breaths per minute. Laboratory results reveal a WBC 20,000/μL, hematocrit 45%, platelets 225/μL, sodium 131 mEq/L, potassium 5.3 mEq/L, chloride 95 mEq/L, bicarbonate 5 mEq/L, BUN 20 mg/dL, creatinine 0.9 mg/dL, and glucose 425 mg/dL. Arterial blood gas reveals a pH of 7.2. Urinalysis reveals glucosuria and ketosis. There is a fruity odor to his breath. Which of the following provides the strongest evidence for the diagnosis?
Hypotension, tachycardia, and tachypnea
Glucosuria, hypotension, and leukocytosis
Glucose of 425 mg/dL, ketosis, and leukocytosis
Glucose of 425 mg/dL, ketosis, pH 7.2, and bicarbonate of 5 mEq/L
Glucose of 425 mg/dL, hypotension, and fruity odor to breath
154) A 32-year-old man is brought to the ED by EMS for confusion. EMS reports that the patient was at a local pharmacy filing his prescriptions when the pharmacist noticed the patient sweating and having difficulty answering questions. In the ED, the patient’s BP is 130/68 mmHg, HR is 120 beats per minute, temperature is 98.9°F, and RR is 12 breaths per minute. The patient is unable to explain what happened. His fingerstick glucose is 410 mg/dL and his urine is positive for ketones. An electrolyte panel reveals Na + 131 mEq/L, K + 4 mEq/L, Cl − 91 mEq/L, and Ca 2+ 11 mEq/L. Which of the following electrolytes are most important to supplement during the management of his medical condition?
Sodium, potassium, and calcium
Sodium and calcium
Sodium
Potassium
Calcium
155) A 36-year-old immigrant woman is brought to the ED from her workplace. She was found to be agitated and behaving bizarrely. The patient’s past medical history and medications are unknown. Her BP is 162/92 mmHg, HR is 140 beats per minute, temperature is 101.8°F, and RR is 18 breaths per minute. On examination, the patient is delirious, tremulous, and has a large goiter. Which of the following is the most appropriate management of this patient?
Administer dantrolene
Protect airway; administer acetaminophen, propranolol, and PTU
Administer dantrolene
Protect airway; administer iodine
Administer diazepam
156) A 75-year-old woman is brought to the ED by EMS after she had a witnessed seizure on the street. A bystander reports that the patient fell to the ground, had tonic-clonic activity, and was drooling. Her BP is 162/85mmHg, HR is 95 beats per minute, temperature is 99.4°F, and RR is 16 breaths per minute. On examination, the patient is unresponsive and has a bleeding superficial scalp laceration. Which of the following electrolyte disturbances is least likely to cause a seizure?
Hypoglycemia
Hypokalemia
Hyperglycemia
Hyponatremia
Hypernatremia
157) A 53-year-old woman is brought to the ED by her husband. He states that his wife is feeling very weak over the last 2 days, is nauseated, and vomiting at least three times. The husband states that she was taking a high-dose medication for her joint pain but ran out of her pills last week. Her vital signs are BP of 90/50 mmHg, HR 87 beats per minute, RR 16 breaths per minute, and temperature 98.1°F. You place her on the monitor, begin IV fluids, and send her blood to the laboratory. Thirty minutes later the metabolic panel results are back and reveal the following: Na+ 126 mEq/L, K+ 5 mEq/L, Cl− 99 mEq/L, HCO3 21 mEq/L, BUN 24 mg/dL, Creatinine 1.6 mg/dL, Glucose 69 mg/dL, Ca+ 11 mEq/L. What is the most likely diagnosis
Myxedema coma
Hyperaldosteronism
Thyroid storm
Adrenal insufficiency
Diabetic ketoacidosis (DKA)
158) A 44-year-old agitated woman is brought to the ED by her husband. He states that she has had fevers to 101°F and a productive cough at home for the last 3 days. Today she became labile, agitated, and complained of abdominal pain. She was recently diagnosed with Graves disease and started on PTU. Her BP is 156/87 mmHg, HR is 145 beats per minute, temperature is 102.4°F, and RR is 20 breaths per minute. On examination, the patient is agitated, confused, and has rales on auscultation bilaterally. Which of the following is the most likely diagnosis?
Pheochromocytoma
Neuroleptic malignant syndrome
Cocaine ingestion
Thyroid storm
Heat stroke
{"name":"Part 25(158)", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"1) A 72-year-old female is admitted to the ICU with severe chest pain. The initial set of cardiac enzymes is positive and her EKG reveals an anterior wall myocardial infarction. She receives treatment with aspirin clopidogrel, metoprolol nitroglycerine drip, and morphine. Two hours later, her telemetry monitor displays the following rhythm. Which of the following is the best next step in managing this patient?, 2) A 46-year-old man collapsed while getting out of his bed. He has been feeling weak over the last several days and has complained of vague chest discomfort. He ascribed the symptoms to a recent respiratory infection and did not visit a doctor. His mother died of a stroke and his father suffered from recurrent myocardial infarctions. He eats a balanced diet and takes a multivitamin daily. His most recent blood cholesterol level was 200 mg\/dl. An ECG strip taken by EMS is shown below. Which of the following is the best initial management of this patient?, 3) A 67-year-old Caucasian male is hospitalized in the intensive care unit (ICU) with an episode of prolonged hypotension and shortness of breath. His skin is cold and clammy. Intra-arterial blood pressure monitoring is established, and pulmonary artery catheterization is performed to control basic hemodynamic parameters. His blood pressure is 70\/40 mmHg, and heart rate is 100\/min. Cardiac output (CO) measured by thermodilution method is 2.3 L\/min. Pulmonary capillary wedge pressure (PCWP) is estimated to be 22 mmHg. Systemic vascular resistance (SVR) calculated using data on mean arterial pressure, right atrial pressure and cardiac output is 2000 dynes*s\/cm5 (N= 700 -1200 dynes*s\/cm5). Which of the following is the most likely underlying problem in this patient?","img":"https://cdn.poll-maker.com/10-475751/untitled-png1.png?sz=1200"}