
Med management 3 a 100 qcm q1 to 100
1) A 46-year-old female is brought to the emergency department because of visual blurring and altered mental status. She was recently treated for gout. Physical examination shows moderate to severe splenomegaly and positive sternal tenderness. Laboratory studies reveal a WBC count of 120, 000/uL with left shifted myeloid series and basophilia. Bone marrow exam shows 3% blasts. Repeat CBC is ordered. The hematologist-on-call decides to start leukophereses emergently. What another drug should be given to this patient?
. Cladribine
. Hydroxyurea
. Cyclophosphamide
. Interferon alpha
. Imatinib mesylate
2) A 64-year-old male patient with deep vein thrombosis is being treated with unfractionated heparin. On the 4th day of treatment, his platelet count drops to 80,000/cmm. His previous platelet count on day 2 was within normal range. He denies any bleeding-related complications, and is completely asymptomatic. His complete examination does not reveal any signs of bleeding. His blood pressure is 128/80mm of Hg, pulse is 78/min, and respirations are 20/min. He is afebrile. What is the most appropriate next step in the management of this patient?
. Switch to low molecular weight heparin
. Stop heparin and start warfarin
. Stop heparin
. Start plasmapheresis
. Stop heparin and start platelet transfusion
3) A 19-year-old man comes to the office and says, "Doctor! I have been having a peculiar problem lately. My stool has a funny color. First, it was black and almost sticky. Yesterday, it became maroon. In fact, today I saw some bright red blood." He denies any associated pain or fever. He is adopted, and his family history is unknown. His vital signs are stable. Physical examination is normal, but his stool is positive for occult blood. Laboratory studies reveal a hematocrit of 29% and hemoglobin concentration of 9.6 g/dL. Colonoscopy reveals hundreds of colonic polyps, which are identified as adenomatous polyps with the biopsy. What is the appropriate recommendation for this patient at this point?
. Reassure the patient as the polyps are most probably benign and have no long-term complications
. Perform regular colonoscopy and biopsy every three years from now on to check for any malignant change
. Start regular colonoscopy and biopsy eight years from now
. The patient needs elective procto-colectomy
. The patient needs close surveillance with regular F OBT and CEA levels
4) A 6-year-old, African-American boy presents with fever and pain in his extremities for the last several hours. The pain is unrelated to movement or posture. His pulse is 102/min, blood pressure is 110/70 mm Hg, temperature is 38°C (100.4°F), and respirations are 18/min. Physical examination reveals pallor, jaundice, and splenomegaly. Both lower legs are tender to palpation. Lab tests show the following: Hematocrit 20%, WBC count 13,000/micro-L, Platelet count 180,000/miro-L, Bilirubin 5.0 mg/dL, Direct bilirubin 1.2 mg/dL, Reticulocyte count 11%. Peripheral blood smear shows sickle shaped cells. Hemoglobin electrophoresis confirms the diagnosis of sickle cell anemia. After treating the child with analgesia, hydration, and oxygen therapy, the painful episode subsides. Which of the following measures should be employed to prevent aplastic crisis in this child?
. Supplementation with folic acid
. Supplementation with iron
. Vaccination against parvovirus
. Vaccination against pneumococcus
. Treatment with hydroxyurea
5) A 22-year-old white male presented to the emergency room (ER) with the sudden onset of acute right upper quadrant pain. The ultrasound showed cholelithiasis. Initial evaluation revealed hemoglobin of 9 gm/dl with an MCV of 90 fl and a total reticulocyte count of 1000 cells per microliter. Peripheral smear revealed polychromatophilia and spherocytes. Liver function tests revealed an elevated indirect bilirubin and normal hepatic enzyme levels. Physical examination is consistent with pallor. The patient's parents were killed in an accident when he was 8-year-old, and the patient does not know anything about the family history. Which of the following is the most correct statement about this patient's condition?
. His condition is classically transmitted as autosomal recessive disorder
. He will probably depend on transfusions
. This patient should be placed on folic acid supplementation
. Vaccination against parvovirus has shown to decrease morbidity and mortality
. This patient's mean corpuscular hemoglobin concentration (MCHC) is likely to be very low
6) A 70-year-old man presents to the urgent care clinic complaining of extensive bruising and bleeding gums. His medical history is significant for atrial fibrillation for which he takes metoprolol and warfarin. He has been stable on his current dose of warfarin for several months. He denies any recent use of NSAIDs or other over-the-counter medications. The patient reports that he has been taking his warfarin as prescribed and has been trying to "live a healthier life" lately. On further questioning, he reports trying to exercise more often, taking numerous vitamin supplements daily, and eating more vegetables. His new diet consists mainly of vegetables like spinach, Brussels sprouts, and broccoli, as well as copious amounts of green tea. Which of the following lifestyle changes is most likely responsible for this patient's bleeding?
. Brussels sprouts
. Green tea
. Spinach
. Increased exercise
. Vitamin supplements
7) A 26-year-old man comes with his girlfriend to the emergency department due to a very high fever. He just finished his second cycle of BEP (bleomycin, etoposide, cisplatin) chemotherapy for metastatic seminoma 4 days ago. Other than his fever, he has no complaints. He denies any chest pain, cough, diarrhea or any rash. He stopped smoking ever since he was diagnosed with his "deadly disease," but drinks alcohol occasionally. His temperature is 38.9°C (102°F), blood pressure is 118/70 mm Hg, pulse is 102/min, and respirations are 19/min. Physical examination reveals a pale man without any eyebrows or eyelashes. Chest auscultation is clear. Blood tests reveal: WBC 690/mm3 with 9% neutrophils, Hemoglobin 8.6 g/dl, Hematocrit 25%, Platelets 74,000/mm3. What is the best next step in the management of this patient?
. Give acetaminophen and send him home
. Obtain blood cultures and give cefepime
. Obtain blood cultures and give vancomycin
. Order blood cultures and wait for the results
. Give blood, platelet, and G-CSF transfusion
8) A 34-year-old woman comes to the ER because of right lower leg swelling, redness, and pain. She has no significant past medical history and does not use any medications. Her mother has a history of pulmonary embolism. Her temperature is 36.7°C (98°F), pulse is 80/min, respirations are 16/min, and blood pressure is 120/76 mmHg. Examination shows tenderness to palpation in the right calf. Compressive ultrasonogram shows a deep vein thrombosis of the right leg. Further evaluation reveals an elevated plasma homocysteine level. She is started on heparin and warfarin therapy. What other additional therapy is indicated in this patient?
. Clopidogrel
. Streptokinase
. Vitamin E
. Pyridoxine
. Simvastatin
9) A 55-year-old male comes to the physician's office because of fatigue. He denies any other symptoms. His vital signs are stable. Examination shows pallor, massive splenomegaly, and mild hepatomegaly. CBC reveals pancytopenia with striking monocytopenia. His peripheral blood smear is shown below. Bone marrow biopsy shows a dry tap. What is the most appropriate treatment for this patient's condition? . Bone marrow transplantation . Cladribine . Cyclophosphamide . CHOP regimen . Chlorambucil and prednisone 10) A 36-year-old male comes to your office complaining of progressive fatigability. His past medical history is significant for infiltrative pulmonary tuberculosis diagnosed two months ago. His current treatment includes isoniazid, rifampin, ethambutol, and pyrazinamide. Laboratory values are: Hemoglobin 8 g/dl, MCV 77 fl, MCHC 30%, ESR 17 mm/hr, Serum iron 170 micro-g/dl (N 50- 150 micro-g/dl ), Total iron binding capacity (TIBC) 280 micro-g/dl (N 300-360 micro-g/dl). Microscopy reveals two populations of red blood cells (RBC)-hypochromic and normochromic. What is the next best step in the management of this patient? . Bone marrow biopsy . Iron preparations . Folic acid . Folic acid and vitamin B12 . Pyridoxine 11) A 56-year-old male is admitted to the ICU for the management of hepatic encephalopathy. He is a known alcoholic. He is started on oral neomycin, lactulose, and a low-protein, high-carbohydrate diet.
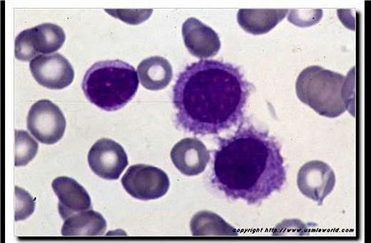
Image

. Bone marrow transplantation
. Cladribine
. Cyclophosphamide
. CHOP regimen
. Chlorambucil and prednisone
10) A 36-year-old male comes to your office complaining of progressive fatigability. His past medical history is significant for infiltrative pulmonary tuberculosis diagnosed two months ago. His current treatment includes isoniazid, rifampin, ethambutol, and pyrazinamide. Laboratory values are: Hemoglobin 8 g/dl, MCV 77 fl, MCHC 30%, ESR 17 mm/hr, Serum iron 170 micro-g/dl (N 50- 150 micro-g/dl ), Total iron binding capacity (TIBC) 280 micro-g/dl (N 300-360 micro-g/dl). Microscopy reveals two populations of red blood cells (RBC)-hypochromic and normochromic. What is the next best step in the management of this patient?
. Bone marrow biopsy
. Iron preparations
. Folic acid
. Folic acid and vitamin B12
. Pyridoxine
11) A 56-year-old male is admitted to the ICU for the management of hepatic encephalopathy. He is a known alcoholic. He is started on oral neomycin, lactulose, and a low-protein, high-carbohydrate diet. His blood pressure is 116/78 mm Hg, pulse is 78/min, temperature is 37.5°C (99.5°F), and respirations are 18/min. His labs reveal the following: Hb 10.2 g/dl, WBC 7,400/cmm, Hct 27%, Platelets 4 2,000/mm3, PT 18 sec, INR 2.02, PTT 31 sec. He has no evidence of active bleeding. Which of the following should be administered to this patient at this time?
. Fresh frozen plasma
. Cryoprecipitate
. Vitamin K
. Platelets
. Packed RBC
12) A 32-year-old Italian-American man presents to your office for a routine check-up. He works as a business executive and admits to being under a lot of stress recently. He drinks alcohol occasionally and smokes one pack of cigarettes per day. Laboratory analyses reveal: Hemoglobin 10.1 mg/dl, RBC count 4.0 x 10^12/L, MCV 70fl, WBC count 5,500/mm3, Platelets 170,000/mm3, Serum calcium 10.1 mg/dl, Serum potassium 4.5 meq/L, Serum sodium 135 meq/L. Serial fecal occult blood tests are negative. A peripheral blood smear reveals the following: Which of the following is the best treatment for this patient?
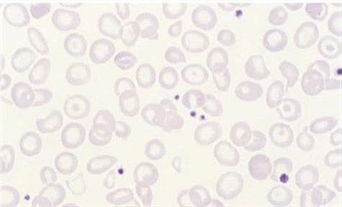
Image

. Iron
. Folic acid
. Cobalamin
. Reassurance
. Erythropoietin
13) A 47-year-old man comes to the office for the evaluation of a sore over his right ear. His sore bleeds and oozes, and has remained open for 3 weeks. He thinks that it has been growing slowly over the past year. He works for the postal service (USPS), and is usually out all day delivering mail. He admits to smoking approximately 2 packs of cigarettes daily for the last 13 years. Physical examination reveals a punched out 1.5 cm ulcer on his right auricle. There are no enlarged lymph nodes. Full thickness biopsy reveals proliferating malignant cells which arise from the epidermis and extend into the dermis in lobules or strands. What is the best next step in the management of this patient?
. Surgical excision with 1-2 mm of clear margins
. Wide excision with at least 5 em margins
. Scraping
. Observe for 3 weeks and then examine
. Local chemotherapy with anticancer creams
14) A 56-year-old man complains of fatigue and occasional palpitations. He has a 20-year history of diabetes mellitus and takes daily insulin therapy. He receives hemodialysis three times a week for end-stage renal disease. He was recently started on erythropoietin therapy for anemia (his pretreatment hemoglobin was 8.0 mg/dl). Physical examination at this visit reveals pale conjunctiva. Repeat laboratory studies show: Hemoglobin 9.2 mg/dl, MCV 77 fl, MCHC 30 g/dl, WBC count 7,000/mm3, Platelets 150,000/mm3, Hemoglobin A1c 7.5%, ESR 15 mm/hr. Which of the following is likely to be helpful in improving this patient's symptoms?
. Tighter blood glucose control
. Higher erythropoietin dose
. Iron supplementation
. Folic acid supplementation
. Splenectomy
15) A 48-year-old Caucasian female is undergoing a routine work-up 9 months after radical mastectomy due to right-sided breast cancer. She has no present complaints, and says that she is 'full of energy'. Chest radiograph reveals an isolated pulmonary nodule, 2.0 cm in diameter, in the middle lobe of the right lung. CT confirms that the lesion is solitary with poorly defined margins, but completely within lung parenchyma. Bone scan is negative. CT abdomen and pelvis is normal. Transthoracic biopsy demonstrates adenocarcinoma with positive estrogen receptors (ER) and no HER-2/neu overexpression. Which of the following is the best management strategy for this patient?
. Surgery
. Systemic chemotherapy
. Hormone therapy
. Pretreatment with monoclonal antibodies against HER-2/neu
. Combined chemotherapy and endocrine therapy
16) A 56-year-old white male is being evaluated for having isolated IgG elevation. The level of serum IgG is 2400 (Normal is 700 to 1500), while the levels of the other paraproteins are within normal limits. The patient was previously admitted with a diagnosis of pneumonia, which resolved completely with levofloxacin. His other laboratory test results are as follows: Hemoglobin 13.0 g/dl, Serum Ca 8.0 mg/dl, BUN 18 mg/dl, Creatinine 1.1 mg/dl. Bone marrow biopsy reveals 2% of plasma lesions. What is the most appropriate next step in the management of this patient?
. Reassurance and regular follow-up
. Melphalan and prednisolone
. Interferon
. Combination chemotherapy
. Autologus bone marrow transplantation
17) A 55-year-old Caucasian male is hospitalized after a massive hemorrhage from a duodenal ulcer. The hemorrhage was stopped with endoscopic manipulation. Two litters of Ringer lactate were infused and two units of packed red blood cells (RBC) ordered. Ten minutes after the transfusion of packed RBC had been started; the patient was complaining of tremor and feeling 'chilly.' His temperature is 39.4° C (103° F), blood pressure is 120/76 mmHg, pulse is 100/min, and respirations are 24/min. The transfusion was stopped, and acetaminophen was given. Direct antiglobulin test and plasma free hemoglobin level are negative. Urinalysis is normal. The reaction abated three hours after the transfusion had started. Which of the following actions could have prevented the reaction described?
. Warming the blood
. Using whole blood
. Careful cross matching of the blood
. Infusing calcium gluconate
. Washing cells
18) A 44-year-old white male comes to the office and says, "I have had this persistent, upper abdominal pain for the past 2 months. My wife has peptic ulcer, and I think I also have an ulcer down there, so I take some of her medicines. At first, the medicines made the pain go away, but soon after the pain proved to be too tough for the medicines. I hardly want to eat anything now. Do you think all this is due to some reaction to those medicines?" Physical examination reveals mild tenderness in the epigastric region. Esophagogastroduodenoscopy reveals a mass in the pylorus, which the biopsy identifies as an infiltrating, low-grade, gastric mucosa-associated lymphoid tissue (MALT) lymphoma. Further work-up concludes that there are no regional lymph nodes involved. What is the best next step in the management of this patient?
. Radical gastrectomy with en bloc resection of spleen and regional nodes
. Give a combination of omeprazole, clarithromycin, and amoxicillin
. Give combination chemotherapy
. Radiotherapy
. Observation and strict surveillance
19) A 42-year-old African-American woman presents to your office with bilateral knee pain that severely limits her mobility. She also complains of joint stiffness in the morning that takes several hours to improve. Her hand joints are symmetrically swollen. She has been taking over-the-counter ibuprofen and aspirin with little relief of symptoms. She has no other medical problems and does not use tobacco, alcohol, or illicit drugs. Her vital signs are within normal limits. Physical examination shows pain and swelling of both wrists and knees. Laboratory studies reveal: Hemoglobin 8.4 mg/dl, Serum iron 30 μg/dL (normal 50-150 μg/dL), Total iron binding capacity 230 μg/dL (normal 300-360 μg/dL), Ferritin 300 ng/dl. Which of the following is most likely to improve this patient's anemia?
. Iron supplementation
. Folic acid supplementation
. Cyanocobalamin supplementation
. Infliximab
. Splenectomy
20) A 25-year-old, G3P0 white female in her 8th week of gestation comes to the antenatal clinic. Her obstetric history is significant for two second trimester abortions. She is currently taking folic acid and iron supplementation. She does not smoke, but she drinks alcohol on social occasions. She is in a monogamous relationship with her husband. She has never been diagnosed with or treated for any STDs. Laboratory studies reveal the following: VDRL positive, FTA-ABS negative, Hct 33%, WBC 7,000/mico-L, Platelets 70,000/micro-L, PT 10 sec, APTT 40 sec. What is the most appropriate next step in the management of this patient?
. Give heparin and aspirin
. Repeat FTA-ABS
. Repeat VDRL
. Single dose of benzathine penicillin
. Three doses of benzathine penicillin
21) A 64-year-old male, who rarely sees the doctor and doesn't believe in screening procedures, comes to office with the complaint of severe back pain. He has not felt comfortable for the past 4 months and is having severe pain in the back. He has found it difficult to sleep. He has hypertension, for which he takes hydrochlorothiazides regularly. He thinks that he has lost some weight. On examination, his BP is 165/90mm of Hg, while rest of vitals are stable. On rectal examination you find a rock hard 2 cm nodule in prostate. Biopsy shows poorly differentiated adenocarcinoma. Bone scans shows wide spread metastasis all over his skeleton. What is the most appropriate treatment for his metastatic disease?
. Leuprolide
. Diethylstilbestrol (DES)
. Flutamide
. Radicle prostatectomy
. Complete androgen blockade with Leuprolide and Flutamide
22) A 65-year-old woman is very worried because she recently had a close family member and friend die, one after the other. First, her 85-year-old mother died of an ovarian cancer that was diagnosed 3 years ago. Last week, she lost her best friend to lung cancer that metastasized to the liver and brain. Today, her 58-year-old sister learned that she has breast cancer. She has regular pap smears and breast examinations. She has read in the paper that there are a few ways that have proved to be very successful in preventing breast cancer. Which of the following measures has the best evidence of preventing breast cancer in high-risk women?
. Prophylactic oophorectomy
. BRCA screening
. Low-fat diet
. Tamoxifen
. Having mammograms every month
23) A 16 year-old-girl with hereditary spherocytosis is scheduled for a splenectomy. She was previously managed with folate therapy and occasional blood transfusions, but her anemia became refractory to medical management alone. Before the operation, she is told that she will have an enhanced risk of developing pneumococcal sepsis. She then asks, "How long will these risks last?" What is the best response to her question?
. 2 weeks
. Up to 6 months
. Up to 2 years
. Up to 10 years
. More than 10 years
24) A 42-year-old mildly overweight Caucasian male is being worked-up for his second episode of deep venous thrombosis in two years. Both episodes seem to have been unprovoked. He denies any recent prolonged immobility, long-distance travel or lower extremity trauma. He has no past medical history of diabetes, cancer or liver disease. A thrombophilia work-up is ordered for this patient. Use of which of the following drugs is most likely to give a false-positive result for protein S deficiency?
. Heparin
. Warfarin
. Aspirin
. Clopidogrel
. Simvastatin
25) A 33-year-old computer programmer was diagnosed with ulcerative colitis last year. He had a colonoscopy and biopsy that showed pancolitis, after which no further work-up was done. This is his first visit to a physician in 6 months. He takes aminosalicylates and is in remission, without any symptoms. He is a member of the Ulcerative Colitis Support Group, which recently sent him a letter that said he should be screened for colon cancer. His vital signs are stable. Physical examination reveals mild tenderness on deep palpation of the lower abdomen. What is the best advice for him regarding his concerns?
. He has an increased risk of colon cancer and he should have prophylactic colectomy
. He has an increased risk of colon cancer and he should have colonoscopy every year
. He has an increased risk of colon cancer and he should have periodic colonoscopy eight years later
. Since he does not have any signs and symptoms, he has no increased risk and doesn't need any surveillance
. He has an increased risk of colon cancer, and he should have a biopsy
26) A 72-year-old Hispanic man comes to the clinic with complains of mild headache, and lethargy for the past several days. He complains of cough for the past 12 years, the cough has been bothering him more lately. The cough is mucoid, he has noticed blood in it once in a while. He has smoked 1 pack/day for 29 years. His vitals are, Temperature 37.0°C (98.6°F); BP 120/84 mm Hg; PR 78/min; RR 24/min. On examination of lungs, adventitious sounds are heard over all the lobes and scant crackles at the base. Laboratory studies show: WBC 7,600/mm3, Hemoglobin 13.6, Hematocrit 40%, Platelets 214,000mm3, Sodium 130 mEq/L, Potassium 3.6 mEq/L, Bicarbonate 18 mEq/L, Blood urea nitrogen 16 mg/dl, Creatinine 0.6 mg/dl, Glucose 95 mg/dl, Serum osmolality 260 mOsm/kg (normal 280), Urine osmolality 310 mOsm/kg. A chest x-ray shows a 2-centimeter left upper lobe mass and mediastinal adenopathy. What will be the next best step in management of this patient?
. Prescribe demeclocycline
. Restrict the patient water intake
. Start an infusion of hypertonic saline
. Start furosemide
. A CT of head
27) You are called by the hospice nurse to evaluate a 74-year-old man who refuses to eat. He has terminal colon cancer, which was diagnosed 8 months ago and has metastasized to his liver. He has already gone through chemotherapy with 5-Fiourouracil + oxaliplatin. During the past 4 months, his condition has gotten extremely worse. He has lost 501bs (27.6kg), and currently appears totally wasted. As you approach him, he says, "I don't feel like eating anything, and I don't want any more procedures, but I'll drink any pill that can make me feel better." His abdomen is distended with positive fluid thrills. His liver has several palpable nodules. What is the best pharmacological agent of choice for this patient's anorexia?
. Megestrol acetate
. Dexamethasone
. Dimenhydrinate
. Ondansetron
. Metoclopramide
28) A 67 -year-old man presents to your office with a one month history of progressive fatigue and exertional dyspnea. He has no significant past medical history. Physical examination reveals enlarged, non-tender axillary lymph nodes bilaterally. His abdomen is soft and non-tender and the liver span is 10 cm. Serial fecal occult blood tests are negative. Laboratory values are as follows: Hemoglobin 7.8 mg/dl, MCV 90 fl, MCHC 33 g/dl, Reticulocytes 7%, WBC count 22,000/mm3, Platelets 200,000/mm3. Which of the following is most likely to improve this patient's symptoms?
. Folic acid
. Iron
. Prednisone
. Pyridoxine
. Erythropoietin
29) A 22-year-old woman comes to the office for the evaluation of a breast mass which she discovered while taking a shower 2 months ago. She experiences severe pain in this mass during her menses. She looks very anxious because her 45-year-old friend was diagnosed with breast cancer last year, and who "now has all sorts of medicines that have made her lose her hair." She has no other problems. She has never been pregnant. She is an occasional smoker, and drinks 3-4 beers a week. There is no family history of breast cancer. Her vital signs are stable. Physical examination reveals a 4 x 5 x 6 cm firm, moveable, rubbery mass in her left breast. Ultrasound shows a cystic mass. Needle aspiration yields clear fluid, after which the mass disappears. What is the best approach in the management of this patient?
. Send the fluid for cytology
. Perform a core biopsy
. Observe for 4 weeks
. Order a mammogram to look for other lesions
. Breath CT scan
30) A 28-year-old male comes for complete physical examination for a new job he is starting next week. He is healthy and has no complaints. He smokes 1 pack/day cigarettes for the last 10 years. He drinks 4 oz of alcohol daily. His mother has hypertension and father has heart problems. Vitals signs are with in normal limits. Physical examination is within normal limits except for a painless, hard mass in left testicle. Ultrasound shows high likelihood of a testicular tumor. What is the next best step in management?
. Observe and recheck the mass after one month
. Platinum based chemotherapy
. Trans-scrotal biopsy
. Fine needle aspiration cytology
. Radical orchiectomy
31) A 41-year-old woman comes to the office for the evaluation of a lump on her left breast. She feels, "generally well," and denies having any medical problems. She takes a multivitamin and Tums daily. She stopped smoking after getting married 21 years ago. She drinks wine only on weekends. Her only surgery was a bilateral tubal ligation last year, after giving birth to her fourth child. Physical examination of the left breast reveals a 4 cm lump at the 11 O'clock position and two axillary nodes on the left side. Mammography shows irregular micro-calcifications. The result of the FNA is suggestive for infiltrating ductal carcinoma. Which of the following is the single most important prognostic factor in this patient?
. TNM staging
. Estrogen and progesterone receptor status
. Her-2/neu oncogene expression
. Histological grade of the tumor
. Irregular micro calcifications in mammogram
32) A 29-year-old woman comes to the office of a primary care physician complaining of pain in her right knee for the last 3 months. The pain is getting progressively worse and is not moving anywhere. She has tried ibuprofen but found little comfort. She is a housewife and unable to do household work because of this pain. She does not smoke nor drink and has hypertension well controlled by hydrocholorothiazide. Her vitals are stable and she is afebrile. On examination her right knee is a little swollen and tender with reduced range of motion. On x-ray, there is soap-bubble appearance in the epiphysis of distal femur. What is the next best step in the management of this patient?
. Refer to an orthopedic surgeon
. Perform biopsy in the office
. Order bone scan
. Start antibiotics
. Do rheumatoid factor and anti-nuclear antibody
33) A 55-year-old man has undergone renal transplantation due to end-stage renal failure. His postoperative course was uncomplicated. He is currently taking prednisone and cyclosporine. He is afebrile and his pulse is 80/min, respirations are 14/min, and blood pressure is 130/65 mm Hg. Physical examination is unremarkable. Which of the following should be added to his current medication regimen to prevent opportunistic infections?
. Trimethoprim-sulfamethoxazole
. Oseltamivir
. Itraconazole
. Azithromycin
. Penicillin
34) A 24-year-old man is found to be HIV positive. He is asymptomatic. Physical examination is unremarkable. Laboratory tests show: CD4 count 400/micro-L, HIV viral load 9,000 copies/mL, VDRL negative, Toxoplasma serology negative, PPD test 6mm induration. His chest x-ray is unremarkable. What is the most appropriate next step in the management of this patient?
. Reassurance and repeat testing in 2 months
. Isoniazid and pyridoxine for 9 months
. Rifampin for 9 months
. Rifampin, isoniazid, pyrazinamide, and ethambutol for 2 months, then isoniazid and rifampin for 4 months
. Rifampin, isoniazid, and pyrazinamide for 6 months
35) A very worried 25-year-old woman comes to the office, presents a positive pregnancy test, and says, "I'm six weeks pregnant. Two months ago, I received the rubella vaccine and my doctor told me to avoid getting pregnant for the next three months. I'm very concerned about the health of my unborn baby. I'd like to know all the available options to prevent any harm to my baby." What is the most appropriate next step in the management of this patient?
. Reassurance
. Explain the risks and benefits of abortion
. Advise abortion
. Serological testing for rubella
. Ultrasonography
36) A 30-year-old male has recently been diagnosed with HIV infection. He denies drug abuse. He is currently asymptomatic, and physical examination is unremarkable. He is in a stable heterosexual relationship. Laboratory studies show a CD4 count of 350/microL, HIV viral load of 15,000 copies/mL, negative VDRL, negative toxoplasma serology, tuberculin skin test of 7 mm induration, negative HBsAg, and positive anti-HBsAg antibodies. Hepatitis C antibodies are negative. Complete blood count, serum chemistries, and liver function tests are within normal limits. He has not received any vaccinations since being diagnosed with HIV. Which of the following vaccines is indicated in this patient?
. BCG vaccine
. Hepatitis A vaccine
. Hepatitis B vaccine
. Pneumococcal vaccine
. Meningococcal vaccine
37) A 42-year-old man with advanced HIV infection has a two-week history of pain and difficulty with swallowing. He was given fluconazole for these symptoms one week ago, but his pain has worsened. His current medications include tenofovir, emtricitabine, efavirenz, and trimethoprim-sulfamethoxazole. His CD4 count is 90/microl and viral load is 300,000copies/ml. Endoscopy reveals large, irregular, linear ulcers in the esophagus. A biopsy of the abnormal mucosa reveals tissue destruction and the presence of intranuclear and intracytoplasmic inclusions. Which of the following is the most appropriate pharmacotherapy for this patient?
. Prednisone
. Acyclovir
. Pentamidine
. Ganciclovir
. Itraconazole
38) A 26-year-old man presents to the physician's office with a two-day history of multiple symptoms, including rash on his trunk, headache, fatigue, malaise, myalgias, and high-grade fever. The rash is not associated with pain, itching, or burning. It has expanded over the last two days. He went on a camping trip in Vermont two weeks ago, and recalls a tick bite at that time. There is a single lesion on his trunk, which is erythematous with central clearing. The rest of the examination is unremarkable. What is the most appropriate next step in the management of this patient?
. Perform ELISA for confirmation of Lyme disease
. Perform western blot for confirmation of Lyme disease
. Give him oral doxycycline
. Give him oral amoxicillin
. Give him intravenous ceftriaxone
39) A 35-year-old HIV-positive male comes to the physician's office because of pain on swallowing and substernal burning for the last 3 days. Examination of the oral cavity is unremarkable. Lungs are clear to auscultation and percussion. His current medications include zidovudine, didanosine, indinavir, trimethoprim-sulfamethoxazole, and azithromycin. His last CD4 count is 40cells/microl. What is the most appropriate next step in the management of this patient?
. Esophagoscopy with biopsy, cytology and culture
. Oral Fluconazole
. Oral Famotidine
. Oral Acyclovir
. Oral Ganciclovir
40) A 25-year-old HIV-positive male comes to a physician with complaints of headache and left-sided weakness of recent onset. His temperature is 38°C (100.8°F), blood pressure is 115/70mm Hg, respirations are 14/min, and pulse is 73/min. Neurological examination reveals decreased power, hyperreflexia, and upgoing plantars in the left upper and lower limb. Neuroimaging by CT shows multiple ring-enhancing lesions. What is the most appropriate next step in management?
. Trimethoprim-sulfamethoxazole
. Sulfadiazine and pyrimethamine
. Brain irradiation
. Brain biopsy
. Anti-tuberculous therapy
41) An 18-year-old young man comes to your clinic with complaints of fatigue, malaise, fever, and sore throat for the past few days. His temperature is 38.8°C (101°F), pulse is 90/min, respirations are 18/min, and blood pressure is 135/70 mm Hg. Physical examination reveals cervical lymphadenopathy, pharyngeal hyperemia, and splenomegaly. Complete blood count shows leukocytosis with predominant atypical lymphocytes. The heterophile antibody test is positive. When you ask if he has any questions, he replies with, "Well, I'm a rugby player in school, so I need to know when I can start playing again." What is the most appropriate advice for this patient?
. He can start playing when he becomes afebrile
. He can start playing when he is no longer fatigued
. He can start playing when his labs normalize
. He can start playing when his physical examination is normal
. He can start playing whenever he wants
42) A 25-year-old man presents to the physician's office because of a clenched fist injury ("fight bite") incurred during a gang fight. The injury occurred two days ago and he has now started to develop pain, swelling, and redness around the wound. His immunizations are up to date. His wounds are cleaned in the clinic. Plain films of hand do not show evidence of foreign body or osteomyelitis. Which of the following is the most appropriate antibiotic for his current condition?
. Amoxicillin-clavulanate
. Clindamycin
. Ampicillin
. Erythromycin
. Ciprofloxacin
43) A 30-year-old white, HIV-infected male from Ohio presents with low-grade fever, anorexia and weight loss of 3.6kg (Bib) for the past 3 weeks. His baseline PPD test was negative. His pulse is 87/min, blood pressure is 126/76 mm Hg, temperature is 38.3°C (101°F), and respirations are 18/min. Examination shows oropharyngeal ulcers and hepatosplenomegaly. Lab testing shows: Hematocrit 36%, Platelet count 50,000/microL, WBC count 3,100/microL. Blood culture establishes the diagnosis of histoplasmosis. What is the most appropriate next step in the management of this patient?
. IV amphotericin B followed by lifelong treatment with itraconazole
. IV amphotericin B till the cultures become negative
. Itraconazole till the cultures become negative
. IV amphotericin B plus itraconazole till the cultures become negative
. Lifelong treatment with itraconazole
44) A 7-year-old boy is brought to the office by his mother due to anal pruritus for the past month. His symptoms are most severe at night. Physical examination is normal, except for mild perianal erythema. Stool examination is normal. "Scotch tape test" is positive. Which of the following is the most appropriate treatment for this child's condition?
. Pyrantel pamoate
. Albendazole
. Metronidazole
. Thiabendazole
. Ivermectin
45) A 37-year-old man comes to his primary care physician for the evaluation of slightly pruritic skin lesions around his anus. He denies fever, malaise, and anorexia. He is sexually active with multiple male partners and occasionally uses condoms. He has never been tested for HIV or other sexually transmitted diseases. He has no drug allergies. Examination shows skin-colored, verrucous, papilliform lesions around his anus. Which of the following is the most appropriate treatment for this patient? 1038
. Podophyllin
. Penicillin
. Erythromycin
. Doxycycline
. Tetracycline
46) A 28-year-old, HIV-infected female from Michigan is admitted with Pneumocystis jirovecii pneumonia (PCP) secondary to noncompliance with prophylaxis. She was diagnosed with HIV infection three years ago. Her C04 count on admission is 30/microl, and viral load is 300,000copies/ml. Her pneumonia is adequately treated with IV antibiotics, and she subsequently receives zidovudine, lamivudine, nelfinavir, and trimethoprim-sulfamethoxazole. What is the most appropriate drug to be added to her current regimen?
. Azithromycin
. Rifabutin
. Fluconazole
. Itraconazole
. Ganciclovir
47) A 65-year-old Connecticut resident calls your office after finding a 3 mm red-brown tick attached to his right leg. He just returned from a hiking trip and was about to a take a shower when he discovered the tick. Which of the following is the best advice to give this patient?

Image

. Crush the tick with your fingers
. Remove the tick with tweezers
. Apply petroleum jelly over the tick
. Come to the office tomorrow for tick removal
. Let the tick detach spontaneously
48) A 27-year-old man presents with fever, malaise, anorexia, and fatigue for the last three days. He denies cough, chest pain, arthralgias, and diarrhea. He has history of rheumatic heart disease and recently underwent a dental cleaning. His temperature is 38.5°C (101.3°F), pulse is 90/min, respirations are 18/min, and blood pressure is 135/76 mm Hg. Examination of his fingernail is shown below. Cardiovascular examination reveals an early diastolic murmur in the mitral area. The chest x-ray is negative. Urinalysis shows microscopic hematuria. What is the most appropriate next step in the management of this patient?
. Start antibiotics immediately and then obtain blood cultures
. Start antibiotics after drawing blood for culture
. Do transesophageal echocardiography
. Do transthoracic echocardiography
. Give aspirin and start his penicillin prophvlaxis
49) A 65-year-old African-American man is hospitalized after a car accident. He has a vertebral fracture at the level of the fifth thoracic vertebra and is unable to move his lower extremities. Since his injury, he has needed a catheter for micturition. Which of the following is the most effective measure for decreasing the risk of a urinary tract infection in patients requiring bladder catheterization?
. Antibacterial creams applied to the urethral meatus
. Prophylactic antibiotics
. Antibacterial washes of external genitalia
. Bladder irrigation with antibacterial solutions
. Intermittent catheterization
50) A 32-year-old man from Arkansas presents to physician with a two-day history of fever, headache, malaise, and myalgias. His family says that he seems slightly confused. He recalls having a tick bite two weeks ago after walking through the woods. His temperature is 39°C (102°F), pulse is 90/min, and blood pressure is 125/80 mm Hg. Neck is supple and there is no lymphadenopathy noted. Oropharynx is clear.
. Doxycycline
. Chloramphenicol
. Erythromycin
. Ceftriaxone
. Hepatitis serology
51) A 22-year-old woman presents to the emergency department after she is bitten on her right arm by her neighbor's dog. She provoked the dog while it was eating. The dog is not immunized against rabies, but does not show any signs of rabies. Her right forearm shows a deep bite wound. Her last tetanus booster was 3 years ago. Her wound is cleaned with soap, water, and povidone-iodine solution. What is the most appropriate next step in the management of this patient?
. Kill the dog and do brain biopsy
. Observe the dog for 10 days
. Active immunization for rabies
. Passive immunization for rabies
. Active and passive immunization for rabies
52) A 25-year-old male comes to the clinic because of a painless ulcer on his penis. He denies fever or urethral discharge, but admits to recent sexual activity with a prostitute. He describes severe rash and face swelling with penicillin. Physical examination reveals a shallow, non-tender ulcer. There is no lymphadenopathy. Darkfield microscopy reveals spirochetes. Which of the following is the most appropriate treatment for this patient?
. Intramuscular benzathine penicillin
. Ciprofloxacin
. IV aqueous crystalline penicillin
. Oral clindamycin
. Oral doxycycline
53) A 40-year -old man who underwent a renal transplant six months ago comes to the clinic with fever, chills, and a productive cough. His temperature is 39.4°C (103°F), pulse is 110/min, respirations are 22/min, and blood pressure is 110/65 mmHg. Chest x-ray shows a right lower lobe nodule with a cavity. Sputum gram stain is shown below. What is the most appropriate treatment of this patient's condition?
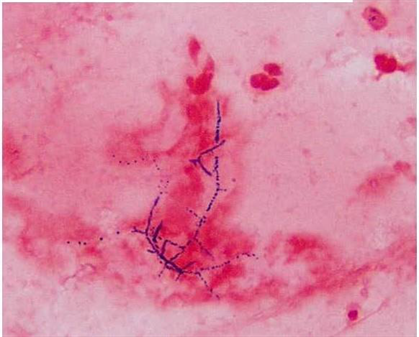
Image

. Penicillin
. Trimethoprim-sulfamethoxazole
. Vancomycin
. Gentamycin
. Metronidazole
54) A 36-year-old woman who lives in the suburbs of a large city comes to your office for a tuberculin skin test. She will be volunteering in her daughter's school cafeteria and the school district requires tuberculin testing. You inject a small amount of Mycobacterium tuberculosis purified protein derivative (PPD) in the skin and 2 days later she returns for a reading. You measure 12 mm of induration. She reports no history of tuberculosis exposure and no underlying medical conditions. She has never before been tested for tuberculosis. She was born in the United States, is not a healthcare worker, and has never spent time in prison. What is the best next step in her management?
. Chest X-ray
. Observation
. Isoniazid for 6 months
. Isoniazid with pyridoxine for 9 months
. Isoniazid, rifampin and pyrazinamide for 8 weeks
55) A 22-year-old female presents to the office with a three-day history of rash, fever, and malaise. There is no burning or itching associated with the rash. Two weeks ago, she had been camping in northern Massachusetts, and noted a tick bite after walking through the woods. She is twelve weeks pregnant. The rash is shown below. The examination is otherwise unremarkable. What is the most appropriate treatment for this patient?55) A 22-year-old female presents to the office with a three-day history of rash, fever, and malaise. There is no burning or itching associated with the rash. Two weeks ago, she had been camping in northern Massachusetts, and noted a tick bite after walking through the woods. She is twelve weeks pregnant. The rash is shown below. The examination is otherwise unremarkable. What is the most appropriate treatment for this patient?

Image

. Doxycycline
. Amoxicillin
. Azithromycin
. Ceftriaxone
. Penicillin G
56) A 5-year-old Hispanic girl is brought to the emergency department (ED) due to a cat bite on her right upper extremity. She was bitten after rambunctiously playing for several minutes with the cat, which had just been given to her as a birthday gift. Her most recent booster tetanus vaccine was one year ago. Her temperature is 36.7°C (98°F), blood pressure is 108/70 mm Hg, pulse is 107/min, and respirations are 21/min. Physical examination reveals a deep puncture wound on the volar aspect of her right forearm. Before going to the ED, her mother cleaned the wound with hydrogen peroxide. There is no visible debris in the wound, and little bleeding is evident. Neurovascular function is intact. Her wound is cleaned in the ED with Betadine and lavaged with saline solution. What is the best next step in managing this girl's care?
. Bandage with dry gauze and discharge home
. Prescribe amoxicillin
. Prescribe amoxicillin/clavulanate
. Prescribe erythromycin
. Prescribe levofloxacin
57) A 57-year-old male comes to your office in the middle of January. He complains of a 4-day history of a nonproductive cough and coryza. He also has vague muscle aches and a mild headache. He denies any shortness of breath or chest pain. His past medical history is significant for hyperlipidemia and impaired glucose tolerance. He takes aspirin and simvastatin 40 mg at bedtime. He has no known drug allergies. His medical records show that he did not show up for his scheduled annual influenza vaccine this year. His temperature is 38.5°C (101.3°F), blood pressure is 135/80 mm Hg, and pulse is 88/min. Physical examination shows conjunctival redness and an erythematous oropharynx. The tympanic membranes are clear. The heart sounds are audible with no added murmurs, rubs or gallops. His breath sounds are vesicular in quality and equal bilaterally. Which of the following is the most appropriate next step in management?
. Administer influenza vaccination now
. Write a prescription for amantidine
. Write a prescription for oseltamivir
. Advise bed rest and symptomatic treatment with acetaminophen
. Empiric trial of oral antibiotics
58) A 60-year-old Caucasian woman undergoes elective coronary artery bypass surgery and aortic valve replacement. Her postoperative course is complicated by acute renal failure, atrial fibrillation, and pulmonary edema. On the third postoperative day, extubation is attempted but not tolerated, thus warranting reintubation. On the fifth postoperative day, she develops a fever to 38.9°C (102°F). Her pulse is 110-120/min and irregular, respirations are 36/min, and blood pressure is 110/65 mmHg. Her chest x-ray shows right middle and lower lobe infiltrates. WBC count is elevated with bandemia. Gram stain of her sputum shows gram-negative rods. She is given intravenous ceftriaxone; however, she deteriorates over the next 24 hours. Which of the following is the most appropriate next step in the management of this patient?
. Stop ceftriaxone and start piperacillin-tazobactam
. Continue ceftriaxone and add vancomycin
. Stop ceftriaxone and start clindamycin
. Continue ceftriaxone and add ceftazidime
. Continue ceftriaxone and add amphotericin
59) A 34-year-old man is traveling in Southeast Asia on business. He is staying in Western-style hotels and eating food in large restaurants. He has not eaten from street vendors. One week after arrival, he develops symptoms of anorexia, nausea, and abdominal cramps followed by the sudden onset of watery diarrhea. He has no fever or chills and there is no blood or pus in the stools. Which of the following is the most appropriate therapy for his condition?
Amoxicillin
Symptomatic therapy with loperamide
Doxycycline
Oral rehydration only
Specific antitoxin
60) A 45-year-old woman is undergoing chemotherapy for breast cancer. She presents 10 days after her last chemotherapy with fever (temperature > 38.5°C), but no other symptoms except a sore throat and mouth. On examination, she looks well, there is oral mucositis, ears are normal, lungs are clear, and the central line site is clean. The CXR, urinalysis, and biochemistry are normal. Her WBC is 800/mL and the absolute neutrophil count is low ( < 500). Which of the following is the most appropriate next step in management?
Start empiric bacterial antibiotics
Start empiric antifungal and bacterial antibiotics
Acetaminophen alone until culture results are available
Start antiviral medications for HSV-1
Start antiviral and bacterial antibiotics
61) A 74-year-old man residing in a nursing home develops symptoms of high fever, diarrhea, chest pain, and nonproductive cough. His temperature is 40°C, blood pressure 120/80 mm Hg, respiration 24/min, and oxygen saturation 90%. He has bibasilar crackles, normal heart sounds, and a soft nontender abdomen. His CXR reveals bilateral lower lobe infiltrates. He is not able to provide any sputum, and the urine is positive for legionella antigen. Which of the following is the most appropriate antibiotic choice?
Trimethoprim-sulfamethoxazole
Azithromycin
Ceftriaxone
Cefuroxime
Gentamicin
62) A 28-year-old female presents to her internist with a 2-day history of low-grade fever and lower abdominal pain. She denies nausea, vomiting, or diarrhea. On physical examination, there is temperature of 38.3°C (100.9°F) and bilateral lower quadrant tenderness, without point or rebound tenderness. Bowel sounds are normal. On pelvic examination, an exudate is present and there is tenderness on motion of the cervix. Her white blood cell count is 15,000/μL and urinalysis shows no red or white blood cells. Serum β-hCG is undetectable. Which of the following is the best next step in management?
. Treatment with ceftriaxone and doxycycline
. Endometrial biopsy
. Surgical exploration
. Dilation and curettage
. Aztreonam
63) Two students from a university dormitory building have contracted meningitis due to Neisseria meningitides. Which of the following students in the dormitory are most likely to benefit from chemoprophylaxis?
Everybody in the dormitory, with oral amoxicillin
Close contacts only, with oral amoxicillin
Everybody in the dormitory, with oral rifampin
Close contacts only, with oral rifampin
Everybody in the dormitory, with meningococcal vaccine
64) You are a physician in charge of patients who reside in a nursing home. Several of the patients have developed influenza-like symptoms, and the community is in the midst of influenza A outbreak. None of the nursing home residents have received the influenza vaccine. Which course of action is most appropriate?
. Give the influenza vaccine to all residents who do not have a contraindication to the vaccine (ie, allergy to eggs)
. Give the influenza vaccine to all residents who do not have a contraindication to the vaccine; also give oseltamivir for 2 weeks to all residents
. Give amantadine alone to all residents
. Give azithromycin to all residents to prevent influenza-associated pneumonia
. Do not give any prophylactic regimen
65) A 22-year-old university student complains of fatigue and malaise for the past 2 weeks. She also reports feeling feverish, and recently had a sore throat. Physical examination reveals enlarged tonsils and palpable cervical lymph nodes. There is also tenderness in the right upper quadrant on deep palpation, and minimal splenomegaly. Laboratory data show hemoglobin 13 g/dL; hematocrit 40%; platelets 340,000/mL; WBC 9400/mL, with 35% segmented neutrophils, 1% eosinophils, and 64% lymphocytes, of which 36% were atypical. A heterophil antibody (sheep cell agglutination) test is positive. Which of the following is the most appropriate initial treatment for this condition?
Gamma-globulin
Adequate rest
Chlorambucil
Chloramphenicol
Radiation therapy
66) A 44-year-old renal transplant patient develops severe cough and shortness of breath on exertion. On examination, he appears dyspneic, respirations 24/min, pulse 110/min, and oxygen saturation 88%. His lungs are clear on auscultation and heart sounds are normal. CXR shows bilateral diffuse perihilar infiltrates. Bronchoscopy and bronchial brushings show clusters of cysts that stain with methenamine silver. Which of the following is the most appropriate next step in management?
Amphotericin B
Cephalosporins
Trimethoprim-sulfamethoxazole
Aminoglycosides
Penicillins
67) A businesswoman needs to make frequent trips to South America, but every time she is there, she develops traveler’s diarrhea, which requires her to change her business schedule. To prevent future episodes during business trips, she is inquiring about prophylaxis methods. Which of the following is the most helpful advice for her?
Take loperamide for symptoms
Take trimethoprim-sulfamethoxazole every day
Take azithromycin every day
Take doxycycline every day
Take ciprofloxacin only if moderate or severe symptoms develop
68) A 30-year-old male patient complains of fever and sore throat for several days. The patient presents to you today with additional complaints of hoarseness, difficulty breathing, and drooling. On examination, the patient is febrile and has inspiratory stridor. Which of the following is the best course of action?
. Begin outpatient treatment with ampicillin
. Culture throat for β-hemolytic streptococci
. Admit to intensive care unit and obtain otolaryngology consultation
. Schedule for chest x-ray
. Obtain Epstein-Barr serology
69) A 35-year-old previously healthy male develops cough with purulent sputum over several days. On presentation to the emergency room, he is lethargic. Temperature is 39°C, pulse 110, and blood pressure 100/70. He has rales and dullness to percussion at the left base. There is no rash. Flexion of the patient’s neck when supine results in spontaneous flexion of hip and knee. Neurologic examination is otherwise normal. There is no papilledema. A lumbar puncture is performed in the emergency room. The cerebrospinal fluid (CSF) shows 8000 leukocytes/μL, 90% of which are polys. Glucose is 30 mg/dL with a peripheral glucose of 80 mg/dL. CSF protein is elevated to 200 mg/dL. A CSF Gram stain shows gram-positive diplococci. Which of the following is the correct treatment option?
. Begin acyclovir for herpes simplex encephalitis
. Obtain emergency MRI scan before beginning treatment
. Begin ceftriaxone and vancomycin for pneumococcal meningitis
. Begin ceftriaxone, vancomycin, and ampicillin to cover both pneumococci and Listeria
. Begin high-dose penicillin for meningococcal meningitis
70) A young man has recently been bitten by a stray dog. He has a penetrating wound to the right forearm. The dog is nowhere to be found. In the emergency room, the wound is cleaned with water and povidone-iodine solution. Which of the following is the most appropriate next step in management?
Start postexposure prophylaxis
Contact the local public health professional for further advice
Treat with oral doxycycline
Treat with IV ceftriaxone
Start IV acyclovir
71) A 22-year-old male, recently incarcerated and now homeless, has received one week of clarithromycin for low-grade fever and left upper-lobe pneumonia. He has not improved on antibiotics, with persistent cough productive of purulent sputum and flecks of blood. Repeat chest x-ray suggests a small cavity in the left upper lobe. Which of the following statements is correct?
. The patient has anaerobic infection and needs outpatient clindamycin therapy
. The patient requires sputum smear and culture for acid fast bacilli
. The patient requires glove and gown contact precautions
. Isoniazid prophylaxis should be started if PPD is positive
. Drug resistant pneumococci may be causing this infection
72) A 23-year-old woman visits your office because of headache, malaise, anorexia, pain in both sides of her jaw, and discomfort in both lower abdominal quadrants. Physical examination reveals enlarged parotid glands; bilateral lower quadrant abdominal tenderness; a temperature of 38.7°C; and a pulse rate of 92/min. Serologic testing (IgM) confirms the diagnosis of mumps. Which of the following is the most appropriate treatment for this condition?
Symptomati
Immunization
Broad-spectrum antibiotics
Sulfonamides
Steroids
73) A 25-year-old woman complains of dysuria, frequency, and suprapubic pain. She has not had previous symptoms of dysuria and is not on antibiotics. She is sexually active and on birth control pills. She has no fever, vaginal discharge or history of herpes infection. She denies back pain, nausea, or vomiting. On physical examination she appears well and has no costovertebral angle tenderness. A urinalysis shows 20 white blood cells per high power field. Which of the following statements is correct?
. A 3-day regimen of trimethoprim-sulfamethoxazole is adequate therapy
. Quantitative urine culture with antimicrobial sensitivity testing is mandatory
. Obstruction resulting from renal stone should be ruled out by ultrasound
. Low-dose antibiotic therapy should be prescribed while the patient remains sexually active
. The etiologic agent is more likely to be sensitive to trimethoprim-sulfamethoxazole than to fluoroquinolones
74) A 40-year-old woman cut her finger while cooking in her kitchen. Two days later she became rapidly ill with fever and shaking chills. Her hand became painful and mildly erythematous. Later that evening her condition deteriorated as the erythema progressed and the hand became a dusky red. Bullae and decreased sensation to touch developed over the involved hand. What is the most important next step in the management of this patient?
. Surgical consultation and exploration of the wound
. Treatment with clindamycin for mixed aerobic-anaerobic infection
. Treatment with penicillin for clostridia infection
. Vancomycin to cover community-acquired methicillin-resistant Staphylococcus
. Evaluation for acute osteomyelitis
75) A 60-year-old man comes to the physician because of a 2-week history of worsening fatigue. He has chronic renal insufficiency, hypertension, diabetes mellitus, hypercholesterolemia, hypothyroidism polymyalgia rheumatica and depression. He was started on lisinopril for the prevention of proteinuria from diabetic nephropathy. Physical examination shows a few basal crackles. He is being considered for dialysis. Laboratory studies show hyperkalemia with serum K + of 6.0 mEq/L. EKG shows no abnormalities. Which of the following is the best treatment to remove K+ from his body?
. Sodium bicarbonate
. Beta agonists
. Calcium gluconate
. Kayexalate
. Insulin plus glucose
76) A 45-year-old man with advanced chronic renal failure comes to the physician because of edema of his feet. His temperature is 37°C (99°F), blood pressure is 150/100mm Hg, pulse is 78/min, and respirations are 15/min. Examination shows bilateral ankle edema. Laboratory studies show BUN of 62 mg/dl, serum creatinine of4.2 mg/dl, serum potassium of 5.6 meq/l, serum sodium of 146 meq/l, and total plasma cholesterol of 260 mg/dl. Which of the following is most likely to improve the prognosis of his disease?
. Captopril
. Simvastatin
. Protein restriction
. Salt restriction
. Potassium restriction
77) A 68-year-old male presents to the emergency room with cough. Chest x-ray is clear of infiltrates but reveals a right upper lobe lung lesion incidentally. A chest CT scan with IV contrast is performed in the emergency department and reveals a 1 cm x 2cm round lesion in the right upper lobe. The patient is admitted to the hospital, and by day 3 of his hospitalization, he has developed acute renal failure. The patient's past medical history is significant for hypertension, hyperlipidemia, diabetes and coronary artery disease. His medications include aspirin, hydrochlorothiazide, clopidogrel, metoprolol, atorvastatin and lisinopril, all of which he has been taking for several years. He has no known drug allergies. He is a former smoker and does not use alcohol or drugs. His baseline blood pressure is 140/90 mm Hg and has remained in the 140s/90s throughout this admission. Physical examination is otherwise unremarkable. The patient's laboratory values from the time of admission to present are given below. Over the course of the next week, the patient's renal function returns to normal. Which of the following would most likely have prevented his renal failure?

Image

. Prednisone
. Furosemide
. Stopping clopidogrel
. Intravenous hydration
. 100% oxygen mask
78) A 23-year-old male hospitalized for confusion and seizures is treated with intravenous high-dose acyclovir. On the third day of hospitalization, his serum creatinine level increases to 3.4 mg/dl from a baseline of 0.9 mg/dl at admission. The observed finding could have been potentially prevented by which of the following?
. Careful allergy history taking
. Monitoring the blood drug levels
. Pre-treatment with allopurinol
. Pre-treatment with prednisone
. Aggressive intravenous hydration
79) A 27-year-old man comes to the physician because of a 1-day history of fever and joint pains. He is being treated with cephalexin for a skin infection. His urine has turned darker. His temperature is 38.5°C (101.3°F), blood pressure is 125/70 mm Hg, pulse is 90/min, and respirations are 15/min. Examination shows a skin rash; examination otherwise shows no abnormalities. Urinalysis shows: 8 RBCs/HPF, 12 WBCs/HPF with white cell casts, eosinophiluria, and a mild degree of proteinuria. Laboratory studies show a BUN of 40 mg/dl and serum creatinine of 2.2 mg/dl. Which of the following is the most appropriate next step in management?
. Discontinue cephalexin
. Start ampicillin and gentamicin
. Start oral ciprofloxacin
. Start intravenous steroids
. Start oral steroids
80) A 30-year-old man is admitted to the hospital with a diagnosis of acute renal failure secondary to poststreptococcal glomerulonephritis. On his fifth hospital day, he develops retrosternal, non-radiating chest pain which is relieved by leaning forward. He denies the use of tobacco or drugs. He drinks alcohol occasionally. He has no past history of any serious illness. His temperature is 37.6°C (99.8°F), blood pressure is 145/95 mm Hg, pulse is 80/min, and respirations are 20/min. A pericardial friction rub is heard on chest auscultation. The rest of the examination shows no abnormalities. EKG shows ST segment elevation in all leads, with elevation of the PR segment in lead aVR. The chest x-ray is normal Urinalysis shows hematuria, red cell casts and mild proteinuria. Laboratory studies show a BUN level of 60 mg/dl and a serum creatinine level of 3 8 mg/dl. What is the most appropriate next step in management?
. Broad spectrum antibiotics
. Intravenous steroids
. Hemodialysis
. Thrombolytic therapy
. NSAIDs
81) A 47-year-old diabetic woman comes to the physician due to the recent onset of tremors. She has undergone combined pancreatic and kidney transplantation secondary to end stage renal disease and diabetes. She takes multiple medications, including immunosuppressants. Her temperature is 36.1° C (97°F), blood pressure is 152/90 mm Hg, pulse is 78/min, and respirations are 16/min. Examination shows gum hypertrophy. Laboratory studies show: Hb 13.0 g/dl, WBC 8,000/cmm, Serum Na 135 mEq/L, Serum K 5.3 mEq/L, BUN 26 mg/dl, Serum Creatinine 1.7 mg/dl. Which of the following immunosuppressants is most likely responsible for her presentation?
. Tacrolimus
. Cyclosporine
. Azathioprine
. Mycophenolate
. Diuretic
82) A 45-year-old male patient comes to the physician's office for a routine check-up. He denies any symptoms and says he feels "perfectly healthy." He was diagnosed with hypertension and mixed hypercholesterolemia a year ago. He is currently taking hydrochlorothiazide, amiloride and simvastatin daily. He does not use tobacco, alcohol or drugs. His blood pressure today is 135/85 mm Hg. Physical examination shows no abnormalities. Routine blood results reveal the following: CBC: Hb 14.2g/dL, Ht 42%, MCV 86 fl, Platelet count 260,000/cmm, Leukocyte count 8,500/cmm, Neutrophils 70%, Eosinophils 1%, Lymphocytes 24%, Monocytes 5%. Serum: Serum Na 140 mEq/L, Serum K 5.7 mEq/L, Chloride 100 mEq/L, Bicarbonate 24 mEq/L, BUN 10 mg/dL, Serum Creatinine 1.1 mg/dL, Calcium 9.0 mg/dL, Blood Glucose 118 mg/dL, Total cholesterol 220 mg/dL, LDL cholesterol 130 mg/dL. The blood sample is checked and is not hemolysed. The EKG shows normal sinus rhythm. What is the most appropriate next step in the management of this patient?
. Intravenous calcium gluconate
. Intravenous dextrose + insulin
. Stop amiloride and recheck lab results in 1 week
. Stop HCTZ and recheck lab results in 1 week
. Start patient on a low potassium diet
83) A 50-year-old man comes to the emergency department due to a sudden onset of severe, colicky pain in the right flank. He was admitted twice in the past for similar complaints; he was managed conservatively and sent home on both occasions. He has no other medical problems. He does not use tobacco, alcohol or drugs. His vital signs are stable. He is given IV fluids and narcotics. Laboratory studies show: Hb 14.5 g/dL, WBC 13,000/cmm; no bands, Platelets 300,000/cmm, BUN 16 mg/dl, Serum Creatinine 0.8 mg/dl. CT scan of the abdomen without contrast shows renal calculi. Which of the following is the best advice for the prevention of future stones in this patient?
. Decrease dietary calcium intake
. Mega doses of Vitamin C
. Decrease dietary protein and oxalate
. Restrict fluid intake
. Increase sodium intake
84) A 64-year-old male with a past medical history of hypertension, diabetes and chronic renal insufficiency presents with gross hematuria. His baseline serum creatinine is 1.6-1.7 mg/dl. The patient's medications include aspirin, hydrochlorothiazide, enalapril, and simvastatin. He has no known environmental, medication, or contrast allergies. On physical examination, the patient has a blood pressure of 130/80 mm Hg. The examination is otherwise unremarkable. Contrast CT scan of the abdomen is planned to evaluate his condition. Which of the following interventions would be most helpful in preventing contrast-induced kidney damage?
. Prednisone
. Non-ionic contrast agent
. Furosemide
. 100% oxygen mask
. Stopping simvastatin
85) A 26-year-old man comes to the emergency department because of a sudden onset of severe right-sided flank pain. The pain is colicky and radiates from the flank to the scrotum. He also has nausea, vomiting and dark-colored urine. He has never had these symptoms before. His temperature is 37°C (98.6°F), blood pressure is 126/70 mm Hg, pulse is 90/min, and respirations are 18/min. Examination shows no abnormalities. He is given adequate analgesia. Non-contrast helical CT shows a 4 mm radiopaque stone in the right upper ureter. Laboratory studies show serum calcium of 9.8 mg/dl, serum creatinine of 0.9 mg/dl, and BUN of 15mg/dl. Urinalysis shows hematuria but no casts. Which of the following is the most appropriate next step in management?
. 24 hr urine collection for metabolic evaluation
. Reassurance
. Fluid intake greater than 2L/day
. Intake of potassium citrate
. Restriction of dietary oxalate
86) A healthy 54-year-old man comes to the physician for a routine health maintenance examination. He has no complaints, but he is requesting for a CT scan of the abdomen. His father died at the age of 60 due to the sudden rupture of an undiagnosed abdominal aortic aneurysm. He has a history of hypertension and gouty arthritis. His social history is not significant. His vital signs are stable. Physical examination shows no abnormalities. ACT scan of the abdomen is shown below. Which of the following is the most appropriate next step in management?
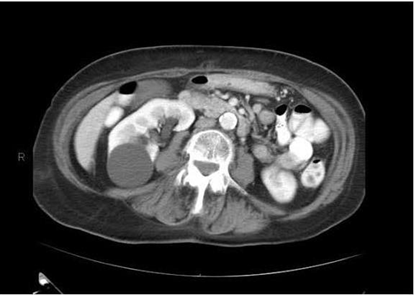
Image

. Reassurance
. Surgery
. CT guided biopsy
. Antibiotics
. Repeat CT scan in 3 months
87) A 72-year-old woman with poorly controlled type 2 diabetes mellitus presents to your clinic one week after being discharged from the hospital. She had been admitted with pyelonephritis secondary to a multi-drug resistant organism, and received several days of intravenous antibiotics. Her serum creatinine on admission had been 2.1 mg/dl. Today it is found to be 4.9 mg/dl. Urinalysis reveals rare epithelial casts and no white blood cells. FENa is greater than 2%. What antibiotic did she most likely receive during her hospitalization?
. Nafcillin
. Vancomycin
. Levofloxacin
. Amikacin
. Doxycycline
88) A 58-year-old man comes to the physician and complains of "problems with erection." He has recurrent and persistently painful erections. His other medical problems include ulcerative colitis, kidney stones, insomnia, depression, hypertension, drug-induced diabetes, obesity and hypercholesterolemia. He does not use tobacco, alcohol, or drugs. He takes prednisone, mesalamine, insulin, 6-mercaptopurine, simvastatin, glyburide, enalapril, trazodone, and fluoxetine. He has no known drug allergies. His vital signs are stable. The general physical examination is unremarkable. Avoidance of which of the following medications could have prevented his condition?
. Fluoxetine
. Trazodone
. Enalapril
. Glyburide
. Simvastatin
89) A 30-year-old woman comes to the physician due to the recent onset of occipital headaches. She has taken acetaminophen several times, but the pain returns. She has no fever or visual problems. She has not had similar episodes in the past. She has no history of serious illness. Her temperature is 36.1°C (98°F), blood pressure is 160/90 mm Hg, pulse is 88/min, and respirations are 16/min. Physical examination shows a rightsided renal bruit Which of the following is the most appropriate treatment for this patient's condition?
. ACE inhibitors
. Furosemide
. Angioplasty with stent placement
. Surgery
. Oral prednisone
90) A 45-year-old man with known cirrhosis due to hepatitis C is admitted to the hospital for abdominal discomfort and confusion. Physical examination reveals a distended abdomen, leg edema, and deep yellow discoloration of the skin and sclerae. Bibasilar crackles are heard on chest auscultation. His serum sodium level is 127 mEq/L, potassium level is 2.9 mEq/L, and creatinine level is 1.3 mg/dl. On day 3 of his hospitalization, the serum creatinine is 4.2mg/dl. A urinalysis reveals: Protein negative, Glucose negative, WBC 4-5/hpf, RBC 0-1/hpf. Renal ultrasound is normal and the post-void residual urinary volume is less than 50 ml. He is given 2 L of normal saline intravenously with no change in his serum creatinine concentration. This patient's kidney dysfunction can be best corrected by which of the following?
. High-dose spironolactone
. ACE inhibitors
. Liver transplantation
. Broad spectrum antibiotics
. Pegylated interferon
91) A 56-year-old man develops oliguria three days after having a kidney transplantation. His postoperative course was uncomplicated. His blood pressure is 160/100 mm Hg and heart rate is 90/min. Palpation of the transplant reveals mild tenderness. Laboratory studies show: Serum sodium 145 mEq/L, Serum potassium 5.5 mEq/L, Serum calcium 8.6 mg/dl, Serum creatinine 3.2 mg/dl, BUN 30 mg/dl. His serum cyclosporine level is normal. Renal ultrasonography does not detect dilatation of the calyces. Biopsy of the transplant shows heavy lymphocyte infiltration and vascular involvement with swelling of the intima. Which of the following is the most appropriate next step in management?
. Decrease the dose of cyclosporine
. Give IV steroids
. Order ureterography
. Administer IV diuretics
. Prepare for surgery
92) A 25-year-old woman comes to the physician because of a 3-day history of burning micturition and increased urinary frequency. She has suprapubic discomfort. She denies having unusual vaginal discharge. She has been sexually active and monogamous for the past 4 years with her husband. Her temperature is 37.1°C (98.9°F), blood pressure is 110/70 mm Hg, pulse is 68/min, and respirations are 15/min. Examination shows suprapubic tenderness without flank tenderness. The rest of the examination is normal. Urinalysis shows: Specific gravity 1.020, Blood Trace, Glucose Negative, Ketones Negative, Leukocyte esterase Positive, Nitrites Positive, WBC 40-50/hpf, RBC 6-10/hpf, Bacteria 50+. Which of the following is the most appropriate next step in management?
. Urine culture
. Oral trimethoprim-sulfamethoxazole
. Oral ciprofloxacin
. Oral nitrofurantoin
. Intravenous trimethoprim-sulfamethoxazole
93) A 34-year-old man is being evaluated for possible end-stage renal disease. He has a long history of diabetes, type 1. He previously developed chronic renal insufficiency despite being on enalapril and insulin. His renal function is getting worse day by day. A nephrologist is currently managing his renal condition. Which of the following long-term treatments would give the best survival rate for this patient?
. Hemodialysis
. Peritoneal dialysis
. Renal transplantation from a cadaver
. Renal transplantation from a living related donor
. Renal transplantation from a living unrelated donor
94) A 50-year-old diabetic woman presents for follow-up of her hypertension. Her blood pressure is 152/96 in the office today and she brings in readings from home that are consistently in the same range over the past month. Her current medications are amlodipine 5 mg daily and hydrochlorothiazide 25 mg daily. The diuretic was added when she developed peripheral edema on the amlodipine; now she has only trace peripheral edema. A spot urine specimen shows 280 μg of albumin per mg creatinine (microalbuminuria is present if this value is between 30 and 300 μg/mg). What would be the best next therapeutic step in this patient?
. Add clonidine
. Add a beta-blocker
. Increase the thiazide diuretic dose
. Add an alpha-blocker
. Add angiotensin-converting enzyme inhibitor or angiotensin receptor blocker
95) A 64-year-old woman develops severe diarrhea 2 weeks after finishing antibiotics for pneumonia. She has also noticed decreased urine output despite drinking lots of fluids. On examination, she has a postural drop in her blood pressure, the JVP is low, and the abdomen is soft but diffusely tender. Despite giving 4 L of normal saline, her urine output remains low. The urinalysis is positive for heme-granular casts and the urine sodium is 42mEq/L. Which of the following medications should be held during the recovery phase of this woman’s ARF?
Acetaminophen
Digoxin
Lorazepam
Enalapril
Simvastatin
96) A 67-year-old man with a history of gout presents with intense pain in his right great toe. He has a complex past medical history, including hypertension, coronary artery disease, congestive heart failure, myelodysplasia, and chronic kidney disease with a baseline creatinine of 3.2 mg/dL and a uric acid level of 10 mg/dL. His medications include aspirin, simvastatin, clopidogrel, furosemide, amlodipine, and metoprolol. What is the best therapy in this situation?
. Colchicine 1.2 mg po initially, followed by 0.6 mg 1 hour later
. Allopurinol 100 mg po daily and titrate to uric acid less than 6 mg/dL
. Prednisone 40 mg po daily
. Naproxen 750 mg po once followed by 250 mg po tid
. Probenecid 250 mg po bid
97) A 60-year-old diabetic woman develops angina and will need a coronary angiogram for evaluation of coronary artery disease. She has a creatinine of 2.2. Which of the following is the most effective in reducing the risk of contrast induced nephropathy?
. Administer mannitol immediately after the contrast is given
. Perform prophylactic hemodialysis after the procedure
. Give IV hydration with normal saline or sodium bicarbonate prior to and following the procedure
. Indomethacin 25 mg the morning of the procedure
. Dopamine infusion before and after the procedure
98) A 56-year-old man presents with hypertension and peripheral edema. He is otherwise healthy and takes no medications. Family history reveals that his father and a brother have kidney disease. His father was on hemo-dialysis before his death at age 68 of a stroke. Physical examination reveals BP 174/96 mm Hg and AV nicking on funduscopic examination. He has a soft S4 gallop. Bilateral flank masses measuring 16 cm in length are palpable. Urinalysis shows 15 to 20 RBC/hpf and trace protein but is otherwise normal; his serum creatinine is 2.4 mg/dL. Which is the most likely long-term complication of his condition?
. End-stage renal disease requiring dialysis or transplantation
. Malignancy
. Ruptured cerebral aneurysm
. Biliary obstruction owing to cystic disease of the pancreas
. Dementia
99) A 63-year-old woman has Type II diabetes mellitus, which is well-controlled. Her physical examination is positive for peripheral neuropathy in the feet and nonproliferative retinopathy. A urinalysis is positive for proteinuria. Which of the following treatments is most likely to attenuate the course of renal disease?
Calcium channel blockers
ACE inhibitors
Hepatic hydroxymethylglutaryl- coenzyme A (HMG-CoA) inhibitors
Dietary carbohydrate restriction
Weight reduction
100) A 60-year-old man is brought in by ambulance and is unable to speak. The EMS personnel tell you that a neighbor informed them he has had a stroke in the past. There are no family members present. His serum sodium is 118 mEq/L. Which of the following is the most helpful first step in the assessment of this patient’s hyponatremia?
. Order a chest x-ray
. Place a Foley catheter to measure 24-hour urine protein
. Clinical assessment of extracellular fluid volume status
. CT scan of head
. Serum AVP (arginine vasopressin) level
{"name":"Med management 3 a 100 qcm q1 to 100", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"1) A 46-year-old female is brought to the emergency department because of visual blurring and altered mental status. She was recently treated for gout. Physical examination shows moderate to severe splenomegaly and positive sternal tenderness. Laboratory studies reveal a WBC count of 120, 000\/uL with left shifted myeloid series and basophilia. Bone marrow exam shows 3% blasts. Repeat CBC is ordered. The hematologist-on-call decides to start leukophereses emergently. What another drug should be given to this patient?, 2) A 64-year-old male patient with deep vein thrombosis is being treated with unfractionated heparin. On the 4th day of treatment, his platelet count drops to 80,000\/cmm. His previous platelet count on day 2 was within normal range. He denies any bleeding-related complications, and is completely asymptomatic. His complete examination does not reveal any signs of bleeding. His blood pressure is 128\/80mm of Hg, pulse is 78\/min, and respirations are 20\/min. He is afebrile. What is the most appropriate next step in the management of this patient?, 3) A 19-year-old man comes to the office and says, \"Doctor! I have been having a peculiar problem lately. My stool has a funny color. First, it was black and almost sticky. Yesterday, it became maroon. In fact, today I saw some bright red blood.\" He denies any associated pain or fever. He is adopted, and his family history is unknown. His vital signs are stable. Physical examination is normal, but his stool is positive for occult blood. Laboratory studies reveal a hematocrit of 29% and hemoglobin concentration of 9.6 g\/dL. Colonoscopy reveals hundreds of colonic polyps, which are identified as adenomatous polyps with the biopsy. What is the appropriate recommendation for this patient at this point?","img":"https://www.quiz-maker.com/3012/images/ogquiz.png"}
More Quizzes
Bible Buzz Online: Quiz #3
22110
Just a trivia quiz
32160
KUP Post Test
20100
Discover Your Taste and Preferences!
9446
Find Your Perfect Fruits Basket Boyfriend: Take the!
201025278
Ace Your American Lit EOC Practice Test: Free Online
201040190
Think You're Smarter Than a 3rd Grader? Take the!
201088900
Can You Ace the Metric System in Biology? - Free Test
201038879
Individual Study for Seniors
15822710
Free Photosynthesis: Light & Energy
201024835
Free Personal Income Tax Practice
201021732
Ace the Aircraft Pneumatic System - Challenge Now!
201025278