
PIC: USLME-BASIC

Healthcare Knowledge Quiz
Test your medical knowledge with our comprehensive quiz designed for aspiring healthcare professionals! This quiz contains 31 questions that challenge your understanding of various conditions, diagnoses, and treatment options.
Whether you're preparing for an exam or just want to refresh your knowledge, this quiz is perfect for:
- Medical students
- Healthcare professionals
- Anyone interested in learning more about medicine
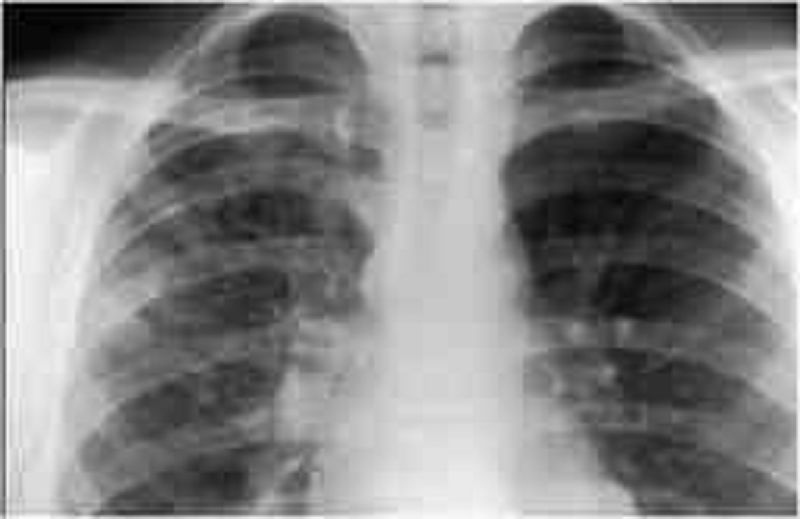
A 13-year-old develops fever, malaise, sore throat, and a dry, hacking cough over several days. He does not appear to be particularly sick, but his chest examination is significant for diffuse rales and rhonchi. The chest radio- graph is shown below. Which of the following is the most likely pathogen?
Staphylococcus aureu
Mycobacterium tuberculosis
Haemophilus influenzae
Streptococcus pneumoniae
Mycoplasma pneumoniae

A 13-year-old male is brought to the physician for evaluation of intermittent left knee pain that arose three months ago. He does not remember any trauma to his knee. The pain worsens after basketball games, but improves some with rest. He has been taking non-steroidal anti-inflammatory medications with some relief. On physical examination, he has edema and tenderness over the proximal tibia at the site of the patellar tendon insertion. Examination of the knee joint is normal and no effusion is present. His knee pain is reproducible by extending the knee against resistance. A lateral radiograph of his knee is shown below. Which of the following is the most likely cause of this patient's knee pain?
Prepatellar bursitis
Traction apophysitis
Patellar tendonitis
Tibial osteomyelitis
Patellofemoral stress syndrome

A 2-day-old boy in the newborn nursery was born at 39 weeks gestation to a 38-year-old woman by vaginal delivery. The mother received epidural fentanyl for severe painful contractions during labor, but the delivery was uncomplicated. Since birth, the boy has shown little interest in breast or bottle feeding. He spit up the last feed but has not vomited. He has not yet passed meconium. Physical examination shows a newborn with generalized hypotonia, a flat facial profile, low-set folded earlobes, and a single transverse crease on each palm. His abdomen is firm and distended. Digital rectal examination is notable for a tight anal canal and relieves an expulsion of gas and stool. Abdominal x-ray shows markedly distended loops of bowel with no gas in the rectum. What is the mostly likely mechanism for his findings?
Constipation from decreased levels of thyroxine
Failure of neural crest cell migration during fetal intestinal development
Intestinal ileus from exposure to maternal epidural analgesia
Intestinal obstruction from inspissated meconium
Invagination of a part of the intestine into itself
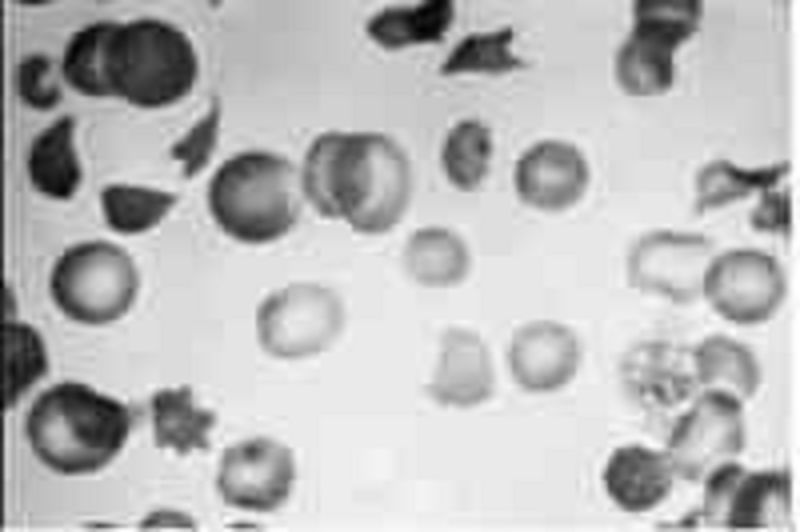
A 2-year-old child in shock has multiple nonblanching purple lesions of various sizes scattered about on the trunk and extremities; petechiae are noted, and oozing from the venipuncture site has been observed. The child’s peripheral blood smear is shown below. Clotting studies are likely to show which of the following?
Increased levels of factor V and VIII
A decreased prothrombin leve
An increased fibrinogen level
The presence of fibrin split products
Normal partial thromboplastin time (PTT)
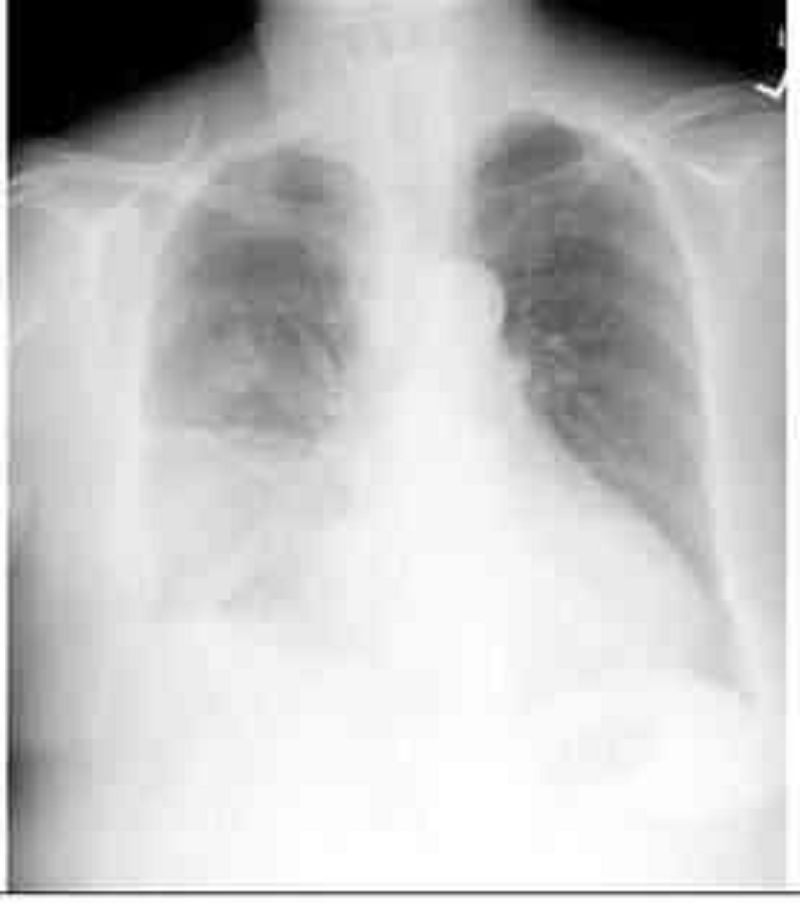
A 23-year-old, HIV-infected female presents with a five-day history of fever and productive cough. She is on antiretroviral therapy, and her CD4 count is 300/mm3. Her temperature is 39.0°C (102.5°F), pulse is 95/min, respirations are 22/min, and blood pressure is 115/76 mm Hg. Physical exam reveals dullness to percussion and bronchial breath sounds in the right lung base. Chest x-ray is shown below. What is the most likely cause of this patient's symptoms?
Streptococcus pneumonia
Mycobacterium tuberculosis
Disseminated coccidioidomycosis
Pneumocystis jiroveci (P. jiroveclj)
Pseudomonas aeruginosa

A 24-year-old woman comes to the physician complaining of a skin rash and pain in her wrists, ankles and elbows over the past 4 days. She has also had a fever and sweats, but denies headache, nausea or vomiting. She has no significant past medical history and does not take any medications. She recently took a vacation with her new boyfriend. She denies any previous sexually transmitted diseases but acknowledges having unprotected sex with her new boyfriend. She does not use tobacco, alcohol or illicit drugs. Her temperature is 38.5°C (101.3°F) and her pulse is 98/min. Her oropharynx is clear and there is no thrush or lymphadenopathy. Her abdomen is benign and the pelvic examination is within normal limits. She has pain along the tendon sheaths with active and passive hand movement. A photo of her skin rash is shown below. Which of the following is the most likely cause of her symptoms?
Lyme disease
Syphilis
Gonococcemia
Meningococcemia
Acute HIV infection

A 25-year-old man is recovering in the hospital from an open repair of his broken femur, which he suffered during an automobile accident. On postoperative day 3 he develops sudden onset shortness of breath and vague chest discomfort. His temperature is 37.6°C (99.6°F), heart rate is 108/min, blood pressure is 95/62 mm Hg, respiratory rate is 42/min, and oxygen saturation is 89% on room air. Physical examination is significant for jugular venous distention to 9 cm and an accentuated pulmonic component of S2. A pulmonary angiogram is shown in the image. Which of the following is most likely to be decreased?
Airway resistance
Alveolar dead space
Alveolar ventilation
Pulmonary compliance
Pulmonary vascular resistance

A 29-year-old construction worker fell 15 ft from a roof and broke his right humerus, as depicted in the accompanying radiograph. Given his injury, which of the following nerves is most at risk?
Median nerve
Radial nerve
Posterior interosseous nerve
Ulnar nerve
Ascending circumflex brachial nerve

A 3-year-old boy is brought to the pediatrician because his mother noticed a reddish-purple rash on his buttocks and thighs (see image). She notes that he has not seemed well since he had a mild cold 2 weeks earlier; he has been complaining of aches and pains in his legs and a stomach ache. Urinalysis shows 10–20 RBCs/ mm³ and 2+proteinuria. Which of the following is associated with this patient’s disease process?
Hemoptysis
High antistreptolysin O titer
Impaired glucose tolerance
Intussusception
Malar rash
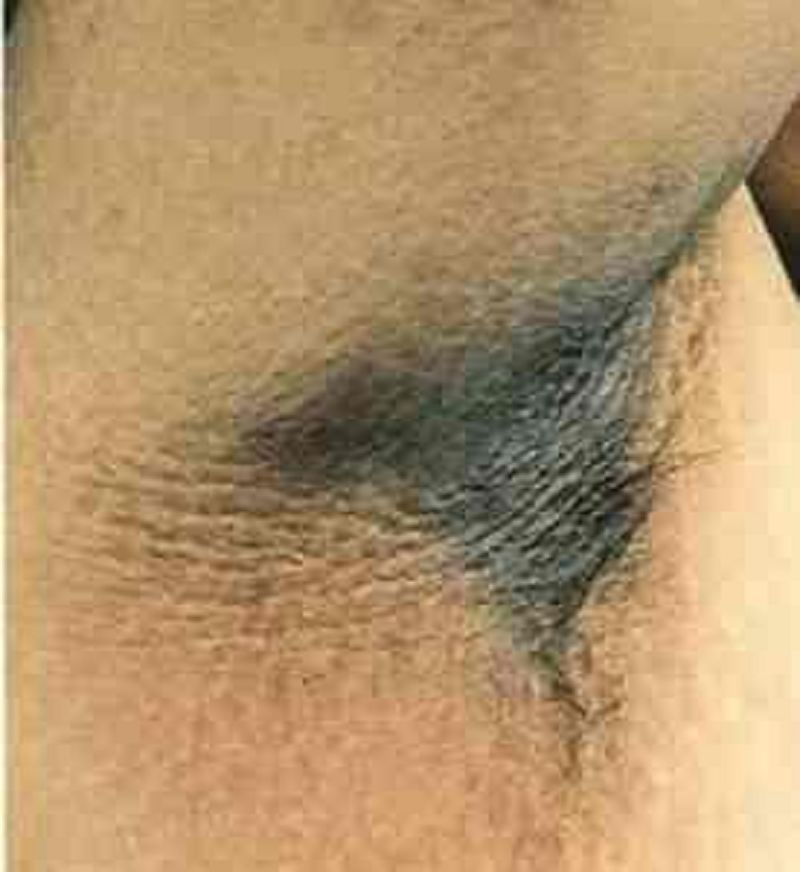
A 31-year-old male presents to your office with a velvety skin rash in his axilla as shown on the slide below. Which of the following is the most likely cause of this patient's condition?
Vitamin D resistance
Calcitonin hypersecretion
Testosterone unresponsiveness
Insulin resistance
Serotonin hypersecretion

A 32-year-old homosexual male with HIV infection presented to his physician with skin lesions. He first noted these lesions last month, and has since observed a change in color from pink to violet. There is no associated pain, itching, or burning. He was diagnosed with HIV infection three years ago and has been noncompliant with his medications. His pulse is 80/min, blood pressure is 115/70 mm Hg, respirations are 14/min, and temperature is 37.1° C (98.8°F). The appearance of his lesions is illustrated below. His CD4 count is 30/microl, and viral load is 300,000copies/ml. Which of the following is the most likely cause of his current condition?
Human herpesvirus 8 (HHV-8)
Human papillomavirus
Pneumocystis jiroveci
Poxvirus
Herpes simplex type 2 (HSV-2)
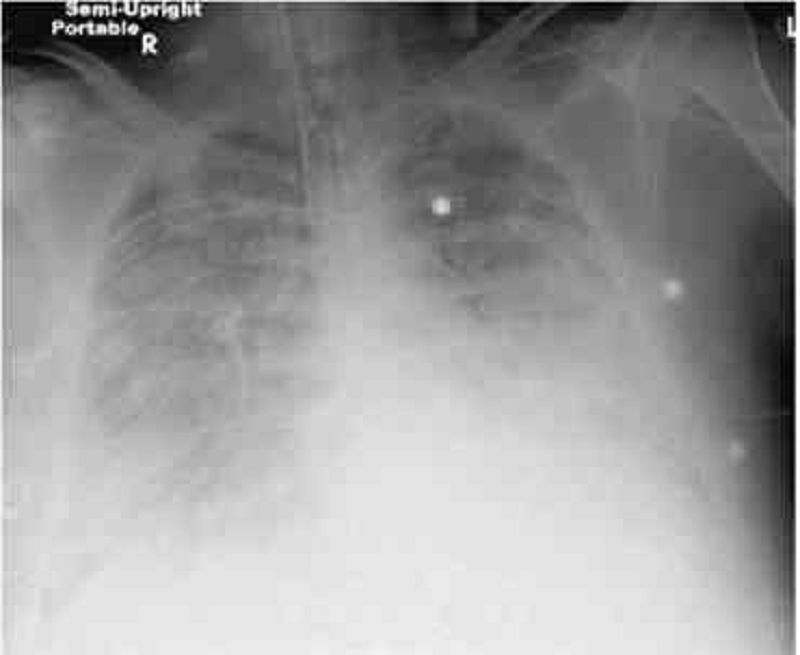
A 38-year -old male is brought to the emergency room with high-grade fever, shaking chills, productive cough and shortness of breath that started two days ago. His medical history is significant for two hospital admissions for alcohol withdrawal seizures. He continues to drink alcohol every day. He has no other medical problems and does not take any medications. On admission, his temperature is 39.7°C (103.5°F), pulse is 110/min, blood pressure is 100/70 mmHg, and respirations are 20/min. His skin and mucous membranes are dry. Physical examination reveals crackles and bronchial breath sounds in the right lower lobe. Chest x-ray demonstrates right lower lobe consolidation. He is started on ceftriaxone, azithromycin and intravenous normal saline at 200 ml/hr. Six hours later the nurse calls you because he is breathing at 38/min and requiring 100% oxygen. Emergent intubation is performed. A repeat chest x-ray is shown below. Which of the following is now most likely to be present in this patient?
Normal pulmonary capillary wedge pressure
Increased lung compliance
Increased left ventricular end diastolic pressure
Normal pulmonary arterial pressure
Normal alveolar-arterial oxygen gradient
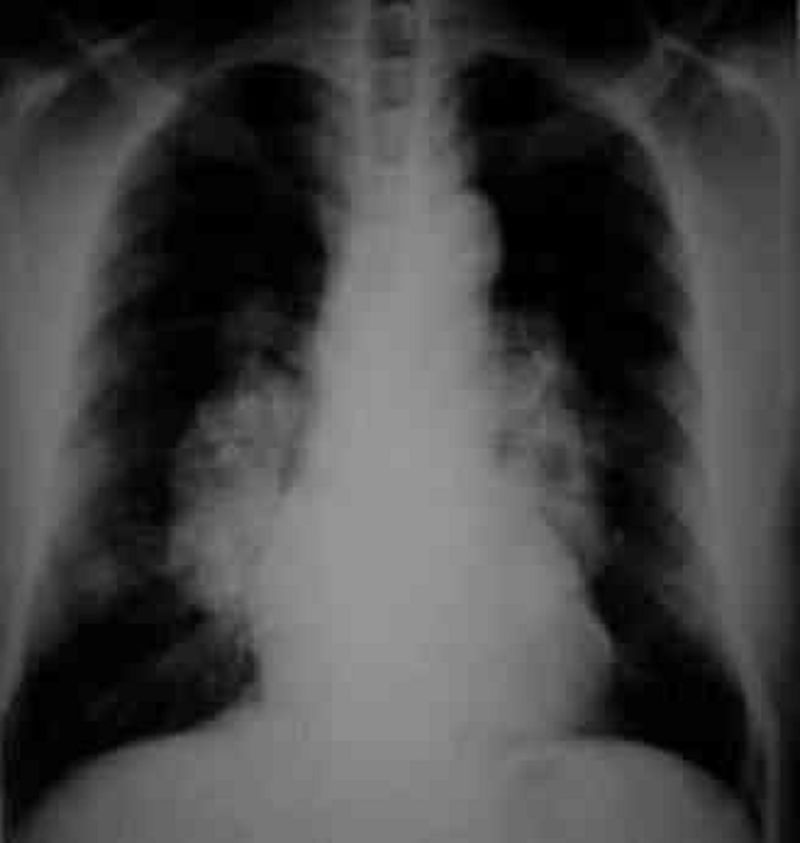
A 45-year-old black female presents to you because of a dry cough and has not been feeling well for the past month. She did have some pain in her shins a few weeks ago. She denies any allergies, smoking, or other medical problems. Her ECG shows normal sinus rhythm. The chest x-ray is shown below. What is the most likely pathophysiology in this patient?
Pulmonary venous congestion
Lupus pneumonitis
Inflammatory granulomas
Malignancy of the lung
Interstitial lung disease

A 45-year-old HIV-positive woman comes to her primary care physician complaining of a 2-day history of bloody diarrhea. She states that she has been feeling well until 2 days ago, when she developed abdominal pain. She denies fevers, chills, night sweats, nausea, or vomiting. She admits to feeling tired over the last couple of weeks and has had a 2.3-kg (5-lb) weight loss over the past 2 weeks. Her stool sample shows WBCs and RBCs. Her Gram stain is shown in the image. Her CD4+ cell count is 201/mm³. Which of the following is the most likely cause of this woman’s symptoms?
Escherichia coli
Kaposi’s sarcoma
Legionella
Mycobacterium avium complex
Mycobacterium tuberculosis

A 46-year-old construction worker is brought to the clinic by his wife because she has noticed an unusual growth on his left ear for the past 8 months (see photo below). The patient explains that, except for occasional itching, the lesion does not bother him. On physical examination, you notice an 8-mm pearly papule with central ulceration and a few small dilated blood vessels on the border. What is the natural course of this lesion if left untreated?
This is a benign lesion and will not change
Local invasion of surrounding tissue
Regression over time
Local invasion of surrounding tissue and metastasis via lymphatic spread
Disseminated infection resulting in septicemia

A 54-year-old female with a long history of hypertension and a recent hospitalization for atrial fibrillation with rapid ventricular response now returns to the hospital complaining of skin changes. Her medications include warfarin, hydrochlorothiazide and metoprolol. On physical examination, her temperature is 36.7°C (98°F), blood pressure is 130/80 mm Hg, pulse is 80/min and irregular, and respirations are 16/min. You observe the skin changes pictured below. Her exam is otherwise unremarkable. Which of the following is the primary cause of her condition?
Antithrombin III deficiency
Factor VII deficiency
Excessive platelet aggregation
Vitamin K deficiency
Protein C deficiency
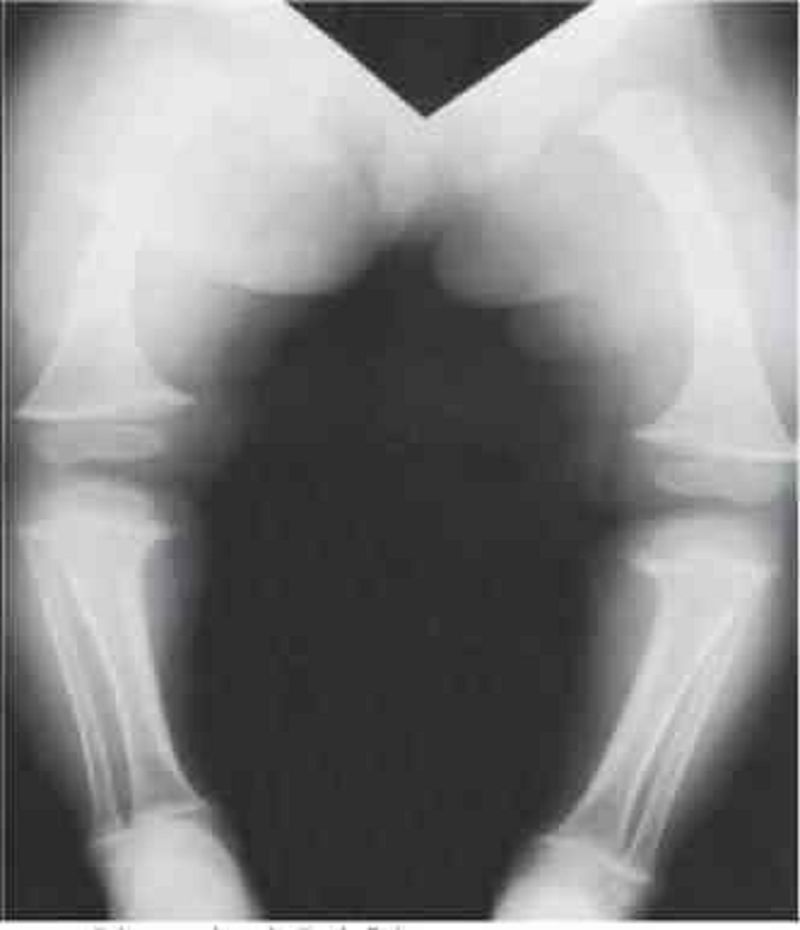
A 6-year-old boy is brought to his pediatrician for a routine check-up. He has not been seen by a physician for the past 3 years. Recently, he has developed some patchy areas of hair loss on his scalp. The mother also notes he has had many colds over the past year. She says he has developed normally, although he started walking later than her other two children. On physical examination his wrists appear enlarged, and he has bowing of the forearms and legs. X-ray of the boy’s legs is shown in the image. Laboratory tests show a calcium level of 7.1 mg/dL, phosphate of 1.8 mg/dL, and intact parathyroid hormone of 130 pg/mL (normal: 10–65 pg/mL). Vitamin D level is normal. Treatment with vitamin D does not correct the patient’s hypocalcemia. Which of the following disorders best explains this patient’s findings?
Dietary vitamin D deficiency
Hypoalbuminemia
Primary hyperparathyroidism
Pseudohypoparathyroidism
Vitamin D-resistant rickets

A 61-year-old man is being evaluated for progressive exertional dyspnea and decreased exercise tolerance. He has also noticed some ankle swelling. The patient has a 40 pack-year smoking history but denies illicit drug use or occupational exposures. His chest x-ray is shown below. The abnormal diaphragmatic contour seen here most likely results in which of the following?
Higher inspiratory flow
Reduced expiratory effort
Increased work of breathing
Increased thoracic wall recoil
Decreased lung compliance
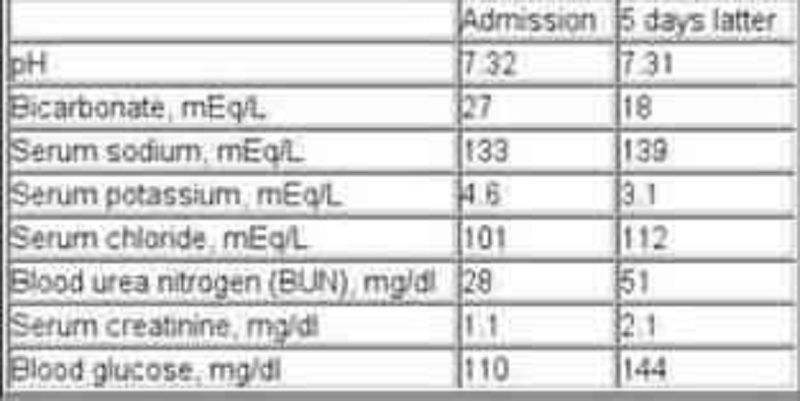
A 65-year-old chronic smoker presents to the hospital with increasing shortness of breath for the past few hours. He has been using albuterol occasionally, but it has not been helping him. He has been non-adherent to doctor's appointments and continues to smoke. He is afebrile. His oxygen saturation on room air is 86%. Examination shows elevated jugular venous pressure and lung auscultation reveals diffuse wheezing with no crackles. His heart sounds are muffled. Mild hepatomegaly and bilateral pitting pedal edema is present. Chest x-ray reveals hyperinflated lungs and a flattened diaphragm with no infiltrates. He is started on systemic steroids, bronchodilator nebulization and furosemide. His laboratory studies are shown below at the time of admission and five days later. Which of the following best explains the acid-base status change in this patient?
Acute renal failure
Development of ketoacidosis
Glucocorticoid treatment
Obstructive sleep apnea
Worsening respiratory failure

A 65-year-old female presents with 6 months of worsening dyspnea and dry cough. Whereas she had previously enjoyed an active lifestyle, she now becomes breathless after walking just a few steps. The patient denies fever or chest pain and does not use tobacco, alcohol or illicit drugs. Her only medicine is hydrochlorothiazide for hypertension. She is retired and lives with her husband. She has never travelled abroad and denies any history of exposure to pets. On physical examination, her temperature is 37.2°C (98.9°F), blood pressure is 140/86 mm Hg, pulse is 84/min and respirations are 18/min. Examination shows dry, late inspiratory crackles and finger clubbing. Her chest x-ray is shown below. Which of the following abnormalities is most likely to be present in this patient?
Increased diffusing capacity of carbon monoxide
Decreased FEV1/FVC ratio
Increased residual volume
Increased PaCO2
Increased A-a gradient
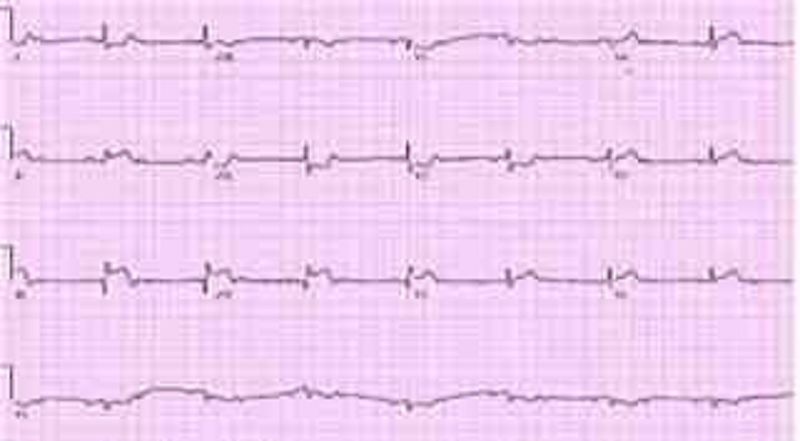
A 68-year-woman with hypertension and dyslipidemia presents with 30 minutes of retrosternal chest pain radiating to her neck. She is diaphoretic and in moderate distress. The ECG shows ST-segment elevation in the inferior leads. Which of the following mechanisms is the most likely cause of her condition?
Coronary plaque rupture
Aortic inflammation
Pericardial inflammation
Vasculitis
Myocarditis
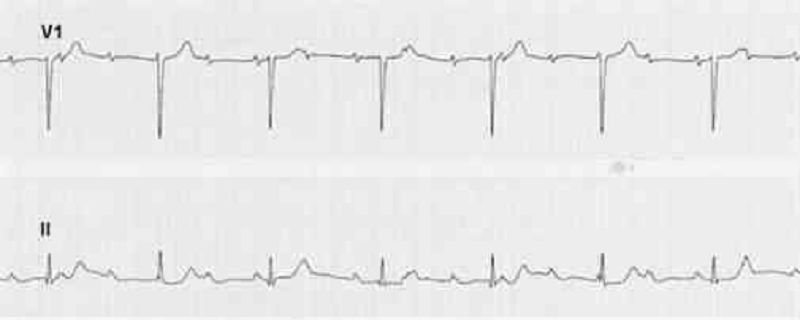
A 69-year-old woman complains of easy fatigue and one episode of presyncope. On examination of the jugular venous pressure (JVP), there are irregular large a waves. The ECG has fixed PP and RR intervals but varying PR intervals. Which of the following conditions is this most likely caused by?
Surgical removal of an atrium
Independent beating of atria and ventricles
A reentry phenomenon
A drug effect
A heart rate under 60 beats/min
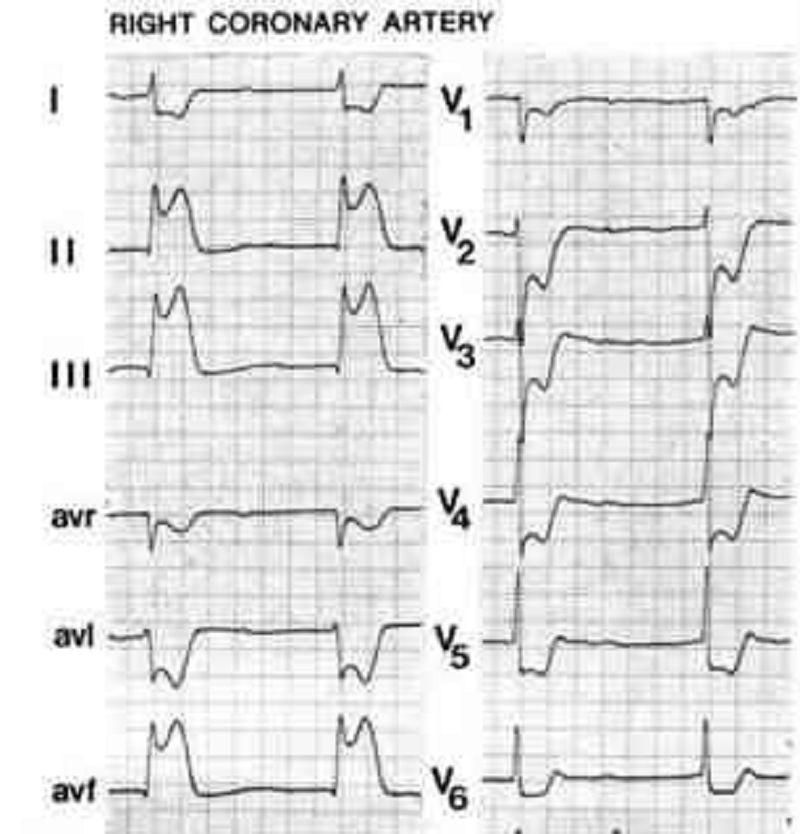
A 70-year-old Caucasian man comes to the emergency department because of the sudden onset of nausea, vomiting, diaphoresis, and chest pain. His other medical problems include hypertension, diabetes mellitus-type 2, and aortic stenosis. He has smoked one-and-a-half packs of cigarettes daily for 30 years and drinks 4 ounces of alcohol daily. His temperature is 37.2°C (99°F), blood pressure is 100/60 mmHg, pulse is 60/min, and respirations are 18/min. The patient's pulse oximetry showed 98% at room air. Examination shows normal first and second he sounds. Lungs are clear to auscultation. His EKG is shown below. Which of the following is the most likely mechanism of this patient's condition?
Occlusion of the right coronary artery
Occlusion of the left circumflex artery
Occlusion of the left anterior descending artery
Inflammation of the pericardium
Vasospasm of the left circumflex artery
A 72-year-old woman notices progressive dysphagia to solids and liquids. There is no history of alcohol or tobacco use, and the patient takes no medications. She denies heartburn, but occasionally notices the regurgitation of undigested food from meals eaten several hours before. Her barium swallow is shown. Which of the following is the cause of this condition?
Growth of malignant squamous cells into the muscularis mucosa
Scarring caused by silent gastroesophageal reflux
Spasm of the lower esophageal sphincter
Loss of intramural neurons in the esophagus
Psychiatric disease

A 74-year-old Caucasian woman is brought to the emergency department after a fall. Her husband is concerned since she is on "blood thinners." Her other medical problems include hypertension, hearing loss, congestive heart failure, coronary artery bypass graft, transient ischemic attack, and atrial fibrillation. She does not use tobacco, alcohol, or drugs. Her medications include aspirin, metoprolol, digoxin, furosemide, and warfarin. Her temperature is 37.2°C (99°F), blood pressure is 140/90 mmHg, pulse is 72/min, and respirations are 14/min. CT scan of the head without contrast is shown below. Which of the following is the most likely cause of her condition?
Tearing of middle meningeal artery
Tearing of bridging veins
Hypertensive hemorrhage
Rupture of an aneurysm
Tumor of the arachnoid granulation
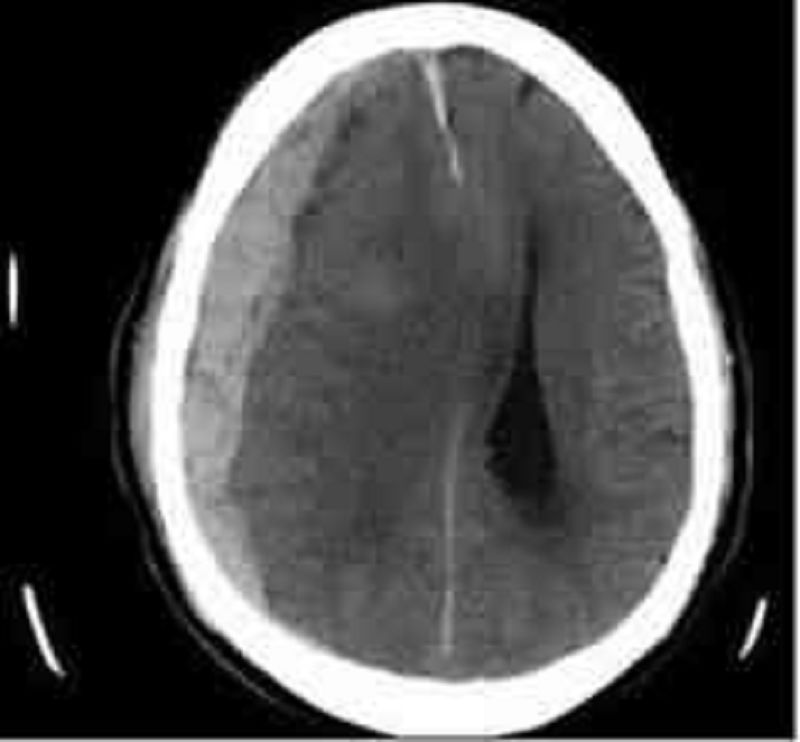
A 76-year-old man is brought to the emergency department by his son who found him confused in his apartment. The son also reports that his father has been limping for the past two days. The patient's past medical history is significant for hypertension, diabetes mellitus, and cataract surgery six months ago. His medications are metoprolol, enalapril, and glyburide. He has also been taking ibuprofen for recent headaches. A head CT scan is obtained and is shown below. Which of the following is the most likely cause of this patient's condition?
Carotid artery atherosclerosis
Small vessel hyalinosis
Blunt head trauma
Ruptured aneurysm
Recent eye surgery

A 80-year-old man with Type II diabetes and hypertension presents with increasing dyspnea. He appears short of breath, blood pressure is 170/95 mmHg, pulse 100/min and regular. The JVP is at 7 cm; there is a loud second heart sound and a systolic ejection murmur at the right sternal border, which does not radiate. The lungs have bibasilar crakles up to the scapula. The CXR has bilateral infiltrates and vascular redistribution. His echocardiogram reports aortic sclerosis, concentric left ventricular hypertrophy (LVH), and normal ejection fraction. Which of the following is the most likely mechanism for this condition?
Valvular heart disease
Diastolic dysfunction
Systolic dysfunction
Hibernating myocardium
Hypertrophic obstructive cardiomyopathy (HOCM)

A previously healthy 5-year-old boy has a 1-day history of low-grade fever, colicky abdominal pain, and a rash. He is well-appearing and alert. His vital signs, other than a temperature of 38°C (100.5°F) are completely normal. A diffuse, erythematous, maculopapular, and petechial rash is present on his buttocks and lower extremities, as shown in the photograph. He has no localized abdominal tenderness or rebound; bowel sounds are active. Laboratory data demonstrate Urinalysis: 30 red blood cells (RBCs) per high-powered field, 2+ protein. Stool: Guaiac positive Platelet count: 135,000/μL. These findings are most consistent with which of the following?
Anaphylactoid purpura
Meningococcemia
Child abuse
Leukemia
Hemophilia B
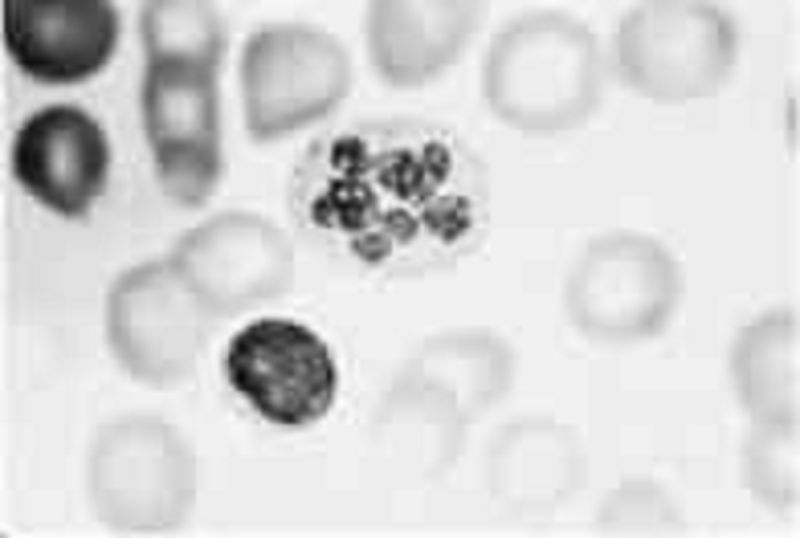
An otherwise healthy child has on his 1-year-old routine CBC the polymorphonuclear neutrophil shown below. This child likely has which of the following?
Malignancy
Iron deficiency
Folic acid deficiency
Döhle inclusion bodies
The Pelger-Huët nuclear anomaly
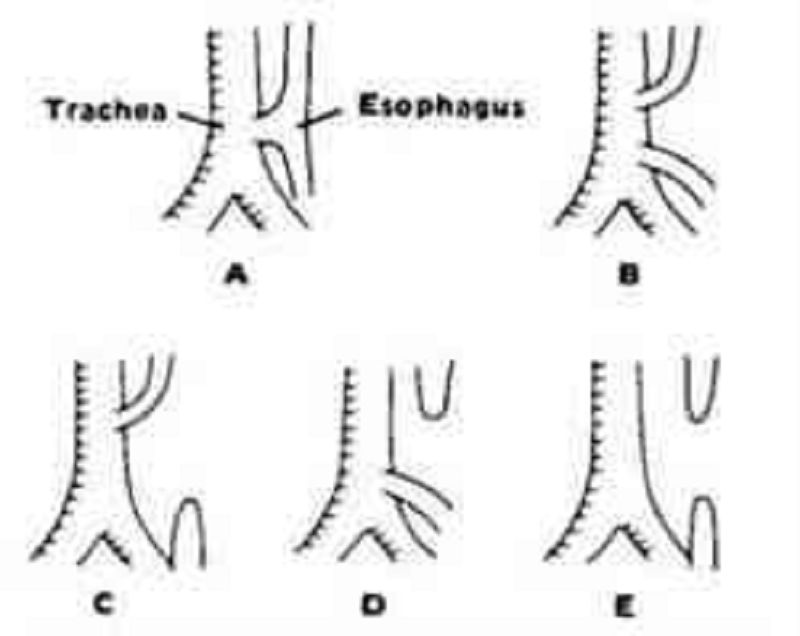
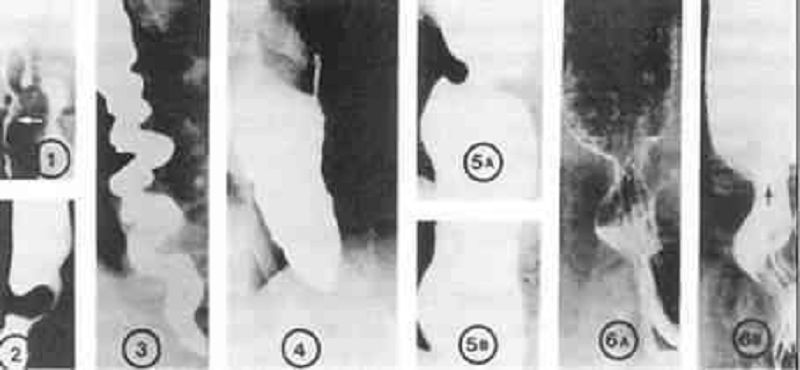
Shortly after birth, an infant develops abdominal distention and begins to drool. When she is given her first feeding, it runs out the side of her mouth, and she coughs and chokes. Physical examination reveals tachypnea, inter- costal retractions, and bilateral pulmonary rales. The esophageal anomaly that most commonly causes these signs and symptoms is illustrated by which of the following?
Figure A
Figure B
Figure C
Figure D
Figure E

You see the newborn baby shown below for the first time in the nursery. You consult plastic and reconstructive surgeon as well as the hospital’s speech therapist. Understandably, the parents have many questions. Which of the following statements is appropriate anticipatory guidance for this family?
Parenteral alimentation is recommended to prevent aspiration
Surgical closure of the palatal defect should be done before 3 months of age
Good anatomic closure will preclude the development of speech defects
Recurrent otitis media and hearing loss are likely complications
The chance that a sibling also would be affected is 1 in 1000
{"name":"PIC: USLME-BASIC", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"Test your medical knowledge with our comprehensive quiz designed for aspiring healthcare professionals! This quiz contains 31 questions that challenge your understanding of various conditions, diagnoses, and treatment options.Whether you're preparing for an exam or just want to refresh your knowledge, this quiz is perfect for:Medical studentsHealthcare professionalsAnyone interested in learning more about medicine","img":"https:/images/course8.png"}