JPOSNA May 2023: Trauma Quiz
Quiz Authors
Patrick Bosch, MD1; Philip McClure, MD2; Z. Deniz Olgun, MD3; Benjamin W. Sheffer, MD4; Trauma, Prevention, and Disaster Response Committee
1Alburquerque, NM; 2Rubin Institute for Advanced Orthopedics, International Center for Limb Lengthening at Sinai Hospital, Baltimore, MD; 3Pediatric Orthopaedic Division, UPMC Children’s Hospital of Pittsburgh, University of Pittsburgh, Pittsburgh, PA; 4Department of Orthopaedic Surgery and Biomedical Engineering, University of Tennessee-Campbell Clinic, Memphis, TN
Quiz Authors
Patrick Bosch, MD1; Philip McClure, MD2; Z. Deniz Olgun, MD3; Benjamin W. Sheffer, MD4; Trauma, Prevention, and Disaster Response Committee
1Alburquerque, NM; 2Rubin Institute for Advanced Orthopedics, International Center for Limb Lengthening at Sinai Hospital, Baltimore, MD; 3Pediatric Orthopaedic Division, UPMC Children’s Hospital of Pittsburgh, University of Pittsburgh, Pittsburgh, PA; 4Department of Orthopaedic Surgery and Biomedical Engineering, University of Tennessee-Campbell Clinic, Memphis, TN
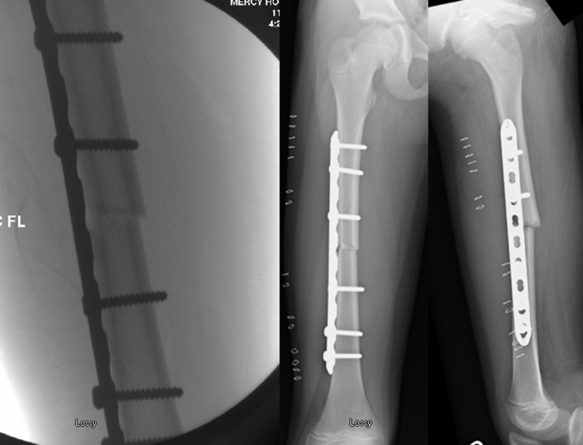
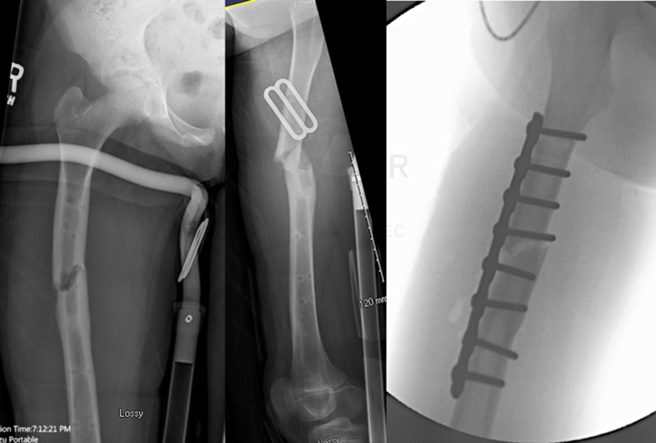
An 8-year-old female suffers a femur fracture (Figure A) that was treated with plate fixation (Figure B). At four months, she had her implant removed (Figure C); one week later she fell during gymnastics and had a recurrent fracture (Figure D) that was treated with repeat ORIF with a plate. Six months later, her refracture is healed, but she is unhappy with gait/fun

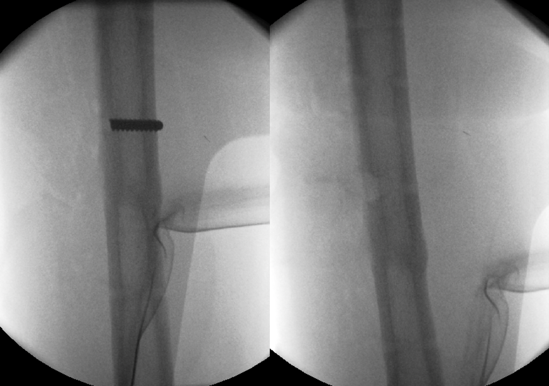

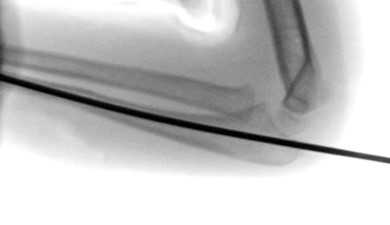
A 6-year-old female fell onto her outstretched arm off balance beam and sustained injury to right arm (Figure A). She was taken to the operating room for surgical treatment. After the ulna was anatomically open reduced, a long Steinmann pin was placed to hold the reduction (Figure B). Intra-operative fluoroscopic image in supination was assessed (Figure C and D). The next step in her care is:



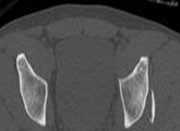
A 16-year-old male dislocated his left hip after a football game pile up. A closed reduction was achieved under conscious sedation and post reduction radiographs (Figure A) and CT scan was obtained (Figure B and C). The next step in management of this injury is:


A 15-year-old boy was involved in a high-speed motor vehicle crash. He sustained an open comminuted tibia fracture (Figure A). He was admitted to the Neuro ICU with a GCS score of 5 with elevated intracranial pressures (ICPs) and an extra-ventricular drain was placed. Finally stable on post injury day 6, he was taken to the operating room for debridement and a 2x7 cm segment of de-vascularized bone was removed while the skin was able to be closed.
What fixation method will be optimal for extended ICU cares while simultaneously minimizing intracranial pressure and risk of deep local infection?

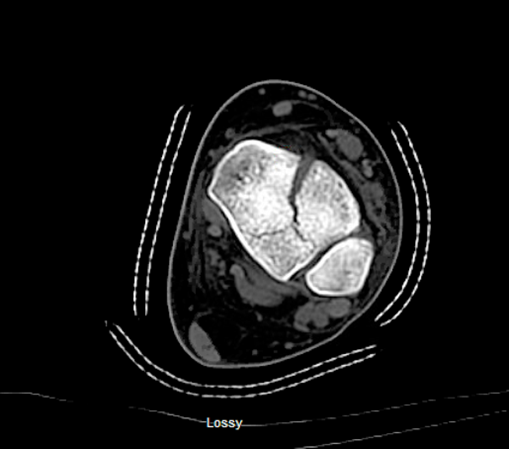
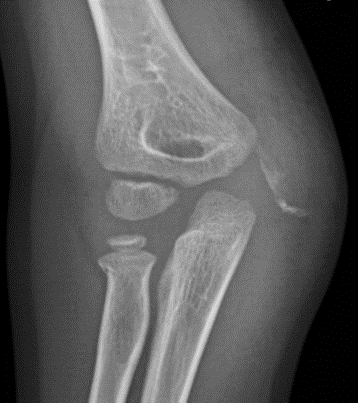
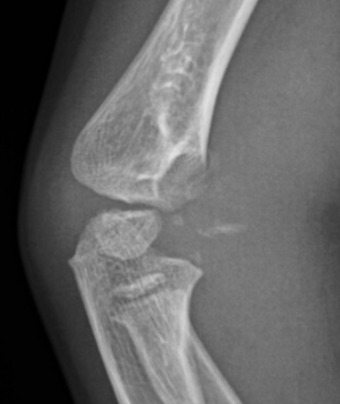
A 4-year-old male fell on the outstretched hand on the playground and sustained the injury seen in the below radiographs. Which of the following imaging modalities would add the most information to the diagnosis of this patient’s injury?
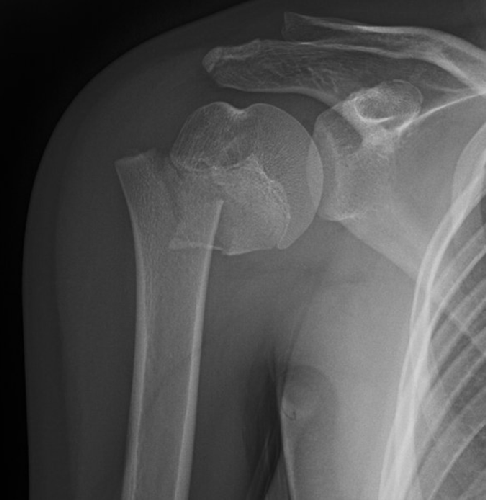
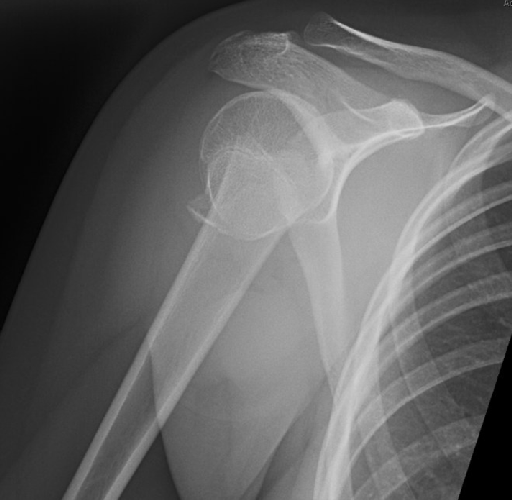
A 17-year-old healthy right-hand-dominant female sustains the below injury (Figure A and B) in the setting of polytrauma she elects to undergo operative fixation. Which of the following methods has been determined to have lower rates of reoperation due to fixation failure and/or implant irritation?