
QCU/DES/USMLE/NEPHROLOGY&ELECTROLYTE
Nephrology and Electrolyte Quiz
Test your knowledge in nephrology and electrolyte management with this comprehensive quiz. Designed for medical professionals, students, and those interested in enhancing their understanding of renal disorders, this quiz presents a series of clinically relevant questions.
Whether you're preparing for the USMLE, studying for a nephrology course, or simply looking to challenge yourself, this quiz covers:
- Clinical presentations
- Diagnostic approaches
- Treatment modalities
- Renal physiology
1. A 51-year-old man is admitted to the hospital because of renal failure. His past medical history is significant for recurrent episodes of bilateral flank pain over the past several years as well as nocturia 2 to 3 times per night for the past 10 years. He has no weight loss. On physical examination, his blood pressure is 160/100 mm Hg. His mucous membranes are pale. There is a palpable mass located at the right flank. Which of the following is the most likely diagnosis?
A. Horseshoe kidney
B. Nephrolithiasis
C. Papillary necrosis
D. Polycystic kidney disease
E. Renal cell carcinoma
2. A 60-year-old man comes to the physician because of a 2-week history of worsening fatigue. He has chronic renal insufficiency, hypertension, diabetes mellitus, hypercholesterolemia, hypothyroidism, polymyalgia rheumatica and depression. He was started on lisinopril for the prevention of proteinuria from diabetic nephropathy. Physical examination shows a few basal crackles. He is being considered for dialysis. Laboratory studies show hyperkalemia with serum K + of 6.0 mEq/L. EKG shows no abnormalities. Which of the following is the best treatment to remove K + from his body?
A. Sodium bicarbonate
B. Beta agonists
C. Calcium gluconate
D. Kayexalate
E. Insulin plus glucose
3. A 45-year-old man with advanced chronic renal failure comes to the physician because of edema of his feet. His temperature is 37C(99F), blood pressure is 150/100mm Hg, pulse is 78/min, and respirations are 15/min. Examination shows bilateral ankle edema. Laboratory studies show BUN of 62 mg/dl, serum creatinine of4.2 mg/dl, serum potassium of 5.6 meq/l, serum sodium of 146 meq/l, and total plasma cholesterol of 260 mg/dl. Which of the following is most likely to improve the prognosis of his disease?
A Captopril
B. Simvastatin
C. Protein restriction
D. Salt restriction
E. Potassium restriction
4. A 30-year-old African American man comes to the physician because of a two-week history of fatigue and ankle edema. He is HIV-positive. He takes no medications. He does not use tobacco, alcohol, or drugs. His temperature is 36.7C (98F), blood pressure is 140/86 mm Hg and respirations are 16/min. Physical examination shows mild ankle edema. Laboratory studies show:Hb 12.5 g/dl WBC 6,000/cmm Platelets 140,000/cmm Serum Na 135 mEq/L Serum K 5.0 mEq/L BUN 28 mg/dl Serum creatinine 2.4 mg/dl Urinalysis revealed 2+ proteinuria but otherwise shows no abnormalities. CD4 count taken three weeks ago was 550. Which of the following is the most probable form of kidney disease in this patient?
A. Membranous glomerulonephritis
B. Mesangioproliferative glomerulonephritis
C. Collapsing focal and segmental glomerulosclerosis
D. Diffuse proliferative glomerulonephritis
E. Acute interstitial nephritis
5. A 24-year-old woman comes to the physician because of a 24-hour history of right flank pain, burning micturition and high-grade fever with chills. Her temperature is 102 F (38.9C), blood pressure is 90/60 mm Hg, pulse is 130/min, and respirations are 20/min. Physical examination shows costovertebral angle tenderness Which of the following is the most likely urine dipstick finding in this patient?
A. Positive for nitrites and esterase
B. Positive for nitrites only
C. Positive for esterase only
D. Negative for both esterase and nitrites
E. Negative for esterase and positive nitrites
6. A 60-year-old woman comes to the physician because of a 3-month history of worsening fatigue and back pain. She has had diabetes mellitus for the past three years, and hypertension for the past ten years. Laboratory studies show:Hb 9.0 mg/dL Serum calcium 11.2 mg/dL Serum phosphorus 3.5 mg/dL BUN 38 mg/dL Serum creatinine 2.0 mg/dL Which of the following is the most likely cause of this patient's renal failure?
A. Hypertension
B. Diabetes mellitus
C. Paraprotein
D. Primary hyperparathyroidism
E. Renal artery stenosis
7. A 43-year-old man complains of occasional red urine. He denies fever, edema, flank pain or weight loss. Specifically, he says that each urine stream starts out transparent, but turns red by the end of the stream. At times he has noticed small clots in his urine. Physical examination is within normal limits. What is the most likely cause of his complaints?
A. Glomerular disease
B. Nephrolithiasis
C. Urinary tract infection
D. Urethral injury
E. Bladder disease
8. A 70-year-old man comes to the physician due to a 4-6-month history of "almost continuous urinary dribbling." This symptom is present both day and night, and is progressively getting worse. He denies dysuria and hematuria. He has a 20-year history of diabetes mellitus-type 2, hypertension, alcoholic hepatitis and coronary artery disease. He had a gastric emptying study done a few weeks ago because of continuous nausea and early satiety. He had laser photocoagulation of both eyes for diabetic retinopathy. He has smoked one pack of cigarettes daily for 50 years, and drinks 4 to 6 beers daily. He takes NPH insulin, regular insulin, metformin, aspirin, metoprolol, lisinopril and metoclopramide. His vital signs are stable. Physical examination shows a well-appearing man. Pertinent physical findings are a normal sized prostate, decreased sensation in both legs below the knees, and absent Achilles tendon and knee reflexes bilaterally. Fecal occult blood test is negative. Postvoid residual volume is 550 mi. Urinalysis shows: Specific gravity 1.020 Blood trace Glucose positive Ketones negative Protein moderate Leukocyte esterase negative Nitrites negative WBC 1-2/hpf RBC 3-4/hpf Which of the following is the most likely cause of this patient's incontinence?
A. Multiinfarct dementia
B. Overflow incontinence due to detrusor weakness
C. Overflow incontinence from bladder outlet obstruction
D. Urinary tract infection
E. Overflow incontinence due to medication
9. A 74-year-old man comes to the physician because of a one-year history of increased urinary frequency and urgency. He feels that his bladder is "not emptying properly", and has a constant sensation of incomplete voiding. His only other medical problem is hypertension, for which he takes hydrochlorothiazide. He never had any surgeries. Urine culture shows no abnormality. Which of the following is true regarding this patient's disorder?
A. It is best treated with oral antibiotics.
B. It usually starts in the central part of the prostate.
C. It can be treated with continuous suprapubic catheter irrigation.
D. It responds well to beta blockers.
E. It usually starts in the peripheral part of the prostate.
10. A 65-year-old male presents to the emergency department complaining of fever, chills, and a productive cough for the past 3 days. He also complains of right-sided chest pain and shortness of breath. He says that his chest pain worsens with deep breathing. The patient's past medical history is significant for diabetes and hyperlipidemia. He takes aspirin, simvastatin, metformin, glipizide and rosiglitazone. He does not use tobacco, alcohol or drugs. On physical exam, he has a temperature of 39.2°C (102.5.F), a blood pressure of 110/70 mm Hg, a pulse of 112/min, and respirations of 24/min. His mucus membranes are dry. Chest x-ray reveals a right lower lobe pneumonia. Laboratory studies show: Hemoglobin 17.0 g/L Platelets 250,000/mm3 Leukocyte count 16,500/mm3 Serum sodium 140 mEq/L Serum potassium 4.5 mEq/L Blood urea nitrogen (BUN) 48 mg/dL Serum creatinine 2.0 mg/dL Serum calcium 10.3 mg/dL Blood glucose 128 mg/dL Blood cultures are obtained and antibiotics are administered. What is the appropriate next step in the management of this patient?
A. Add lisinopril
B. Discontinue rosiglitazone
C. Discontinue metformin
D. Discontinue glipizide
E. Begin bisphosphonate therapy
11. A 27-year-old woman complains of fatigue, low-grade fevers, anorexia, headaches and skin rash over the past several weeks. She also notes new exertional dyspnea and an unintentional 5-pound weight gain over the past two weeks. On physical examination, her blood pressure is 190/110 mmHg and her heart rate is 90/min. Which of the following is the most likely finding on this patient's urinary tests?
A High VMA excretion
B. High daily cortisol excretion
C. Red blood cells
D. Glucosuria
E. Uric acid crystals
12. A 70-year-old man comes to the physician because of nocturia. He states that over the past two years his urinary frequency has increased and he has to strain while passing urine. He also notes dribbling of a few drops of urine at the end of voiding. Sometimes he has to void again within two hours. He has no other symptoms. He has no history of diabetes mellitus, stroke or trauma. He does not take any medication. His father had surgery of the prostate for benign prostatic hyperplasia. He has a 15-pack-years history of cigarette smoking. Rectal examination shows smooth, firm enlargement of the prostate with no induration. Neurological examination shows no abnormalities. Laboratory study shows a serum creatinine of 0.7 mg/dl. Which of the following studies is indicated at this time?
A. Blood urea nitrogen
B. Ultrasound of kidney, bladder and ureter
C. Urinalysis
D. Serum prostate specific antigen
E. Cystoscopy
13. A 70-year-old woman is brought to the emergency department by her daughter because of altered mental status. She lives alone and is able to perform all daily activities. She experienced a minor febrile illness with decreased appetite several days ago, but has otherwise been in good health. She takes no medications. Her temperature is 37.2C (99F), blood pressure is 92/50 mm Hg, pulse is 100/min, and respirations are 18/min. Physical examination shows dry oral mucosa. Laboratory studies show: Hematocrit 45% Serum sodium 147 mEq/L Serum potassium 5.2 mEq/L BUN 70 mg/dl Serum creatinine 1.8 mg/dl Which of the following is the most appropriate next step in management?
A. Intravenous colloids
B. Intravenous crystalloids
C. Order packed red blood cells
D. Intravenous antibiotics
E. Diuretics
14. A 46-year-old man complains of right flank discomfort. He describes decreased urination over the last week with occasional episodes of high urine output and weakness. He is otherwise healthy. There is no family history of renal disease. On physical examination, his blood pressure is 140/90 mmHg and his heart rate is 80/min. The serum creatinine level is 2.1 mg/dl. Urinalysis shows few red blood cells, white blood cells, trace protein, and no casts. Which of the following is the most likely cause of his complaints?
A. Hematologic malignancy
B. Renal artery stenosis
C. Inherited renal disease
D. Interstitial nephritis
E. Urinary outflow obstruction
15. A 65-year-old man comes to the physician because of increased urinary frequency and urgency, as well as suprapubic discomfort His temperature is 37C(98.6F), blood pressure is 130/75 mm Hg, pulse is 76/min, and respirations are 14/min. Rectal examination shows prostatic induration; physical examination otherwise shows no abnormalities. Urinalysis shows no abnormalities. Expressed prostatic secretions show a leukocyte count of 20 WBCs/HPF (normal is less than 10 WBCs/HPF). They are sent for culture and sensitivity, and fail to grow any bacteria. Serum prostatic specific antigen is 2 ng/ml (normal value is less than 4ng/ml). A diagnosis of nonbacterial prostatitis is suggested. Which of the following is the most appropriate next step in management?
A Perform urinary cytology and cystoscopy
B. Repeat urinalysis
C. Repeat culture of prostatic secretions
D. Treatment with oral erythromycin
E. Treatment with oral trimethoprim-sulphamethoxazole
16. A 45-year-old woman presents to the emergency department (ED) with vomiting and severe right flank pain that radiates to her groin. She has been to the ED twice in the past due to similar episodes of renal colic, and was subsequently discharged on both occasions. She admits to not seeking further medical care because she has no insurance. KUB shows a renal stone. 24-hour urine collection shows a urinary calcium excretion of 350 mg (normal is less than 250 mg in women). Laboratory studies show a serum calcium concentration of 8.9 mg/dL; serum PTH is normal. An x-ray film of the chest shows no abnormalities. Further investigations fail to reveal the cause of her hypercalciuria. Apart from advising her to increase her fluid intake, which of the following interventions will benefit this patient?
A. Restriction of calcium in her diet
B. Thiazide diuretics
C. Low dose furosemide
D. High sodium intake
E. Potassium citrate
17. A 17-year-old man comes to the emergency department and complains of intensive left flank pain that radiates to the groin. He refers to his symptom as "stone passage," which he has experienced "for so many times since childhood." His uncle has the same problem. Urinalysis shows hexagonal crystals. The urinary cyanide nitroprusside test is positive. Which of the following is the most likely cause of this patient's condition?
A. Amino acid transport abnormality
B. Parathyroid adenoma
C. Abnormality of uric acid metabolism
D. Excessive intestinal reabsorption of oxalate
E. Infection
18. A 12-year-old girl comes to the physician because of a 2-day history of periorbital edema and abdominal distention. She has no other complaints. She has never been diagnosed with hypertension. Her father died at the age of 40, with renal failure. Her temperature is 37.1 C(98.9F), blood pressure is 125/75 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows facial puffiness, shifting dullness, and 1+ bilateral pitting pedal edema. Urinalysis shows 3 + proteinuria and lipid laden casts. 24-hour urinary protein excretion is 5 g/day, total serum protein is 4.5 g/dl and serum albumin is 2.3 g/dl. Which of the following is this patient at increased risk of developing?
A. Macrocytic normochromic anemia
B. Accelerated atherogenesis
C. Hypergammaglobulinemia
D. Hypercalcemia
E. Hypoparathyroidism
19. A 26-year-old man comes to the emergency department because of a sudden onset of severe, colicky, left sided flank pain that radiates to the scrotum. He also has nausea, vomiting and dark-colored urine. He has never had these symptoms before. Examination shows no abnormalities. Non-contrast helical CT shows a 5 mm radiopaque stone in the left upper ureter. His laboratory studies are as follows: Serum calcium 9.8 mg/dl Serum creatinine 0.9 mg/dl BUN 15 mg/dl Urinalysis shows hematuria but no casts. Which of the following is the most likely cause of this patient's symptoms?
A. Calcium oxalate stones
B. Calcium phosphate stones
C. Uric acid stones
D. Cysteine stones
E. Struvite stones
20. A 20-year-old man is brought to the emergency department by his mother because of a one-day history of fever, headache, and altered mental status. He has no history of medical illness. Herpes simplex encephalitis is suspected after cerebral spinal fluid analysis shows lymphocytic pleocytosis, elevated protein level, and normal glucose level; in addition, CT scan shows contrast enhancement in the temporoparietal area. High-dose intravenous acyclovir therapy is started. Two days after the beginning of the therapy, the neurologic status improves, but the patient develops oliguria. Laboratory studies show: Serum sodium 140 mEq/L Serum potassium 4.5 mEq/L Serum creatinine 2.8 mg/dl BUN 25 mg/dl Which of the following is the most likely cause of renal damage in this patient?
A. Prerenal azotemia
B. Renal tubular obstruction
C. Glomerular injury
D. Interstitial nephritis
E. Bladder neck obstruction
21. A 33-year-old woman comes to the emergency department due to a 4-day history of left-sided flank pain, nausea, vomiting, fevers and chills. Her temperature is 39C (102F) and blood pressure is 100/60 mm Hg. Examination shows significant left costovertebral angle tenderness. Urinalysis shows positive nitrites, many WBC and bacteria. Laboratory studies show a WBC count of 17,000/cmm with 8% bands. Which of the following is the most appropriate next step in management?
A. Intravenous pyelogram
B. Intravenous antibiotics
C. Blood cultures
D. CT scan of the abdomen
E. Ultrasound of the abdomen
22. A 36-year-old man comes to the physician because of fatigue and generalized edema. He was recently diagnosed with Hodgkin's lymphoma. Laboratory studies show: Serum sodium 145 mEq/L Serum potassium 3.8 mEq/L Serum albumin 2.0 g/dl Serum globulin 7.0 g/dl Total serum bilirubin 0.9 mg/dl Serum creatinine 1.2 mg/dl Urinalysis shows proteinuria 4+. Which of the following glomerulopathies is more likely to be present in this patient?
A. Focal segmental glomerulosclerosis
B. Membranous glomerulonephritis
C. Diffuse proliferative glomerulonephritis
D. Minimal change disease
E. Crescentic glomerulonephritis
23. A 65-year-old male has been having a non-productive, hacking cough for over a week. He takes an over-the-counter medication containing guaifenesin and diphenhydramine in an effort to improve his symptoms. The next day, he complains of lower abdominal discomfort and difficulty voiding. Which of the following most likely accounts for this patient's new complaint?
A. Detrusor inactivity
B. Urethral obstruction
C. Detrusor-sphincter dyssynergia
D. Overactive bladder
E. Abdominal muscle weakness
24. A 30-year-old woman comes to the physician because of a 2-day history of periorbital edema and abdominal distention. She has no other complaints. Her temperature is 37.1C (98.9F), blood pressure is 125/75 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows ascites. Urinalysis shows proteinuria; 24-hour urinary protein excretion is 4 g/day, total serum protein is 5 g/dl and serum albumin is 2.5g/dl. A diagnosis of nephrotic syndrome is made. Renal biopsy is performed. She is started on diuretics and her salt and protein intake is restricted. Her edema begins to improve. However, the patient suddenly develops severe abdominal pain, fever, and gross hematuria. Which of the following is the most likely diagnosis that will be revealed by renal biopsy?
A. Minimal change disease
B. Systemic amyloidosis
C. Focal segmental glomerulosclerosis
D. Membranous glomerulonephritis
E. Diabetic nephropathy
25. A 68-year-old male presents to the emergency room with cough. Chest x-ray is clear of infiltrates but reveals a right upper lobe lung lesion incidentally. A chest CT scan with IV contrast is performed in the emergency department and reveals a 1 cm x 2cm round lesion in the right upper lobe. The patient is admitted to the hospital, and by day 3 of his hospitalization, he has developed acute renal failure. The patient's past medical history is significant for hypertension, hyperlipidemia, diabetes and coronary artery disease. His medications include aspirin, hydrochlorothiazide, clopidogrel, metoprolol, atorvastatin and lisinopril, all of which he has been taking for several years. He has no known drug allergies. He is a former smoker and does not use alcohol or drugs. His baseline blood pressure is 140/90 mm Hg and has remained in the 140s/90s throughout this admission. Physical examination is otherwise unremarkable. The patient's laboratory values from the time of admission to present are given below:Over the course of the next week, the patient's renal function returns to normal. Which of the following would most likely have prevented his renal failure?
A. Prednisone
B. Furosemide
C. Stopping clopidogrel
D. Intravenous hydration
E. 100% oxygen mask
26. A 30-year-old African American man comes to the physician because of a 2-day history of periorbital edema and abdominal distention. His temperature is 37.1C (98.7), blood pressure is 125/75mm Hg, pulse is 80/min, and respirations are 14/min. His height is 170cm (5'7") and weight is 104kg (2301bs). He has been in a drug rehabilitation program for the past 2-months, for a long history of IV drug abuse. Examination shows significant ascites. Urinalysis shows proteinuria; 24-hr urinary protein excretion is 4g/day. Which of the following is the most likely diagnosis?
A Minimal change disease
B. Systemic amyloidosis
C. Focal segmental glomerulosclerosis
D. Membranous glomerulonephritis
E. lgA nephropathy
27. A 12-year-old girl is brought to the clinic due to a 2-month history of headaches. Her headaches last 1-2 hours and have no fixed time of occurrence. She denies nausea, vomiting, chills or fevers. She has no other medical problems and takes no medication. Her family history is significant for hypertension and diabetes. Her blood pressure is 156/90 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows an alert child in no distress. There is a soft to-and-fro bruit heard at the right costovertebral angle. Which of the following is the most likely cause of her hypertension?
A. Coarctation of aorta
B. Renal artery atherosclerosis
C. Pheochromocytoma
D. Fibromuscular dysplasia
E. Conn's syndrome
28. A 65-year-old man is brought to the emergency department due to the sudden onset of weakness. He was lying on the floor for several hours before he was brought in. His other medical problems include hypertension, diabetes mellitus, coronary artery disease, transient ischemic attacks and osteoarthritis. CT scan of the head shows evidence of a right middle cerebral artery territory stroke. Laboratory studies show:  Serum Na 137 mEq/L Serum K 64 mEq/L Chloride 104 mEq/L Bicarbonate 18 mEq/L BUN 36 mg/dl Serum creatinine 3.0 mg/dl Calcium 8.3 mg/dl Blood glucose 178 mg/dl His serum creatinine level one month ago was 1.4 mg/dl. EKG shows tall 'T' waves. CK level is pending. Which of the following is the most appropriate next step in management?
A. Insulin with dextrose
B. Kayexalate
C. Sodium bicarbonate
D. Calcium gluconate
E. Regular insulin
29. A 50-year-old man comes to the physician for a routine check-up. He has no present complaints. He has diabetes mellitus, type 2, stable angina, and gout. He takes glyburide and atenolol. He smokes two packs a day and, occasionally, consumes alcohol. His father had an early myocardial infarction; his brother has diabetes mellitus. His blood pressure is 140/90 mm Hg and heart rate is 65/min. Physical examination shows no abnormalities. There is concern about end organ damage in this patient due to diabetes mellitus. Which of the following is the earliest renal abnormality that could be seen in this patient?
A. Nodular sclerosis
B. Glomerular basement membrane (GBM) thickening
C. Mesangial expansion
D. Immune deposits
E. Glomerular hyperfiltration
30. A 59-year-old man comes to the physician because of dysuria, urinary urgency, and frequency. He also complains of hematuria, nocturia, decreased force of stream, and a feeling of incomplete voiding. These symptoms have been present for more than a month. For the past few days he has been experiencing dull, non-radiating suprapubic pain. He has also been having low-grade fever and malaise for the past couple of days. He has been taking analgesics for osteoarthritis of his right knee for more than 10 years. He has a 40-pack-years history of cigarette smoking and does not use alcohol or drugs. Rectal examination shows a smooth, firm enlargement of the prostate without induration or asymmetry. Neurological examination shows no abnormalities. Urinalysis shows hematuria with isomorphic red blood cells. Laboratory studies show a serum creatinine of 1.5 mg/dl, and a PSA of 2 ng/ml. Which of the following is the most likely explanation for this patient's symptoms?
A. Benign prostatic hyperplasia
B. Carcinoma of bladder
C. Carcinoma of prostate
E. Urinary fistula
D. Multiple sclerosis
31. A 70-year-old man presents to the emergency department with a 12-hour history of inability to void. He also complains of nocturia and problems with initiating micturition for the past few weeks. He denies fever, weakness, numbness, dysuria or hematuria. He does not use tobacco, alcohol, or drugs. Neurological examination shows no abnormalities, except absent Achilles tendon reflexes bilaterally. Straight catheterization of the bladder produces 600 ml of urine. Further evaluation will most likely show which of the following?
A. Urinary tract infection
B. Enlarged prostate
C. Carcinoma of the bladder
D. Multiple sclerosis
E. Urinary fistula
32. A 14-year-old boy comes to the physician because of a 2-day history of fever and nasal discharge. He has also had malaise, fatigue and myalgia. His temperature is 38.8C (101.9F), blood pressure is 130/70mm Hg, pulse is 90/min, and respirations are 15/min. Examination shows no abnormalities. Urine dipstick testing shows proteinuria but there is no hematuria or pyuria; urinalysis otherwise shows no abnormalities. Which of the following is the most appropriate next step in management?
A. Repeat dipstick testing
B. BUN and serum creatinine
C. 24-hour urinary collection for protein
D. Renal ultrasound
E. Reassurance
33. A 23-year-old male hospitalized for confusion and seizures is treated with intravenous high-dose acyclovir. On the third day of hospitalization, his serum creatinine level increases to 3.4 mg/dl from a baseline of 0.9 mg/dl at admission. The observed finding could have been potentially prevented by which of the following?
A. Careful allergy history taking
B. Monitoring the blood drug levels
C. Pre-treatment with allopurinol
D. Pre-treatment with prednisone
E. Aggressive intravenous hydration
34. A 27-year-old man comes to the physician because of a 1-day history of fever and joint pains. He is being treated with cephalexin for a skin infection. His urine has turned darker. His temperature is 38.5C (101.3F), blood pressure is 125/70 mm Hg, pulse is 90/min, and respirations are 15/min. Examination shows a skin rash; examination otherwise shows no abnormalities. Urinalysis shows: 8 RBCs/HPF, 12 WBCs/HPF with white cell casts, eosinophiluria, and a mild degree of proteinuria. Laboratory studies show a BUN of 40 mg/dl and serum creatinine of 2.2 mg/dl. Which of the following is the most appropriate next step in management?
A. Discontinue cephalexin
B. Start ampicillin and gentamicin
C. Start oral ciprofloxacin
D. Start intravenous steroids
E. Start oral steroids
35. A 36-year-old man comes to the emergency department because of excruciating flank pain. The pain radiates to the groin. His temperature is 36.9C(98.5F), blood pressure is 115/75 mm Hg, pulse is 85/min, and respirations are 14/min. Urinalysis shows six RBCs/HPF. Laboratory studies show BUN of 12mg/dl and serum creatinine of 0.9mg/dl. X-ray film of the abdomen shows nephrocalcinosis and IVP shows multiple contrast filled cysts. Ultrasonogram of the kidneys is unremarkable. Which of the following is the most likely diagnosis?
A. Medullary cystic kidney
B. Hydronephrosis
D. Autosomal recessive polycystic kidney disease
C. Autosomal dominant polycystic kidney disease
E. Acquired cystic kidney disease
36. An 80-year-old female is brought from a nursing home with a two-day history of poor oral intake and lethargy. Her past medical history is significant for hypertension, diabetes mellitus, coronary artery disease with coronary stenting two years ago and Alzheimer's disease. She was hospitalized six months ago with pneumonia. Her current medications are aspirin, lisinopril, metoprolol, hydrochlorothia zide, metformin and memantine. Her blood pressure is 95/60 mmHg and heart rate is 90/min. Physical examination reveals fine crackles at the right lung base. Her mucous membranes are dry. Her laboratory findings are significant for WBC of 15,000/mm3, creatinine of 2.1 and BUN of 61 mg/dl. Her creatinine was 0.9 mg/dl during the last admission. Which of the following is the best explanation for the abnormal laboratory findings in this patient?
A. Age-related renal function decline
B. Renal inflammatory infiltration
C. Renal tubular dysfunction
D. Renal vasoconstriction
E. Obstructive uropathy
37. A 30-year-old man is admitted to the hospital with a diagnosis of acute renal failure secondary to poststreptococcal glomerulonephritis. On his fifth hospital day, he develops retrosternal, non-radiating chest pain which is relieved by leaning forward. He denies the use of tobacco or drugs. He drinks alcohol occasionally. He has no past history of any serious illness. His temperature is 37.6C (99.8F), blood pressure is 145/95 mm Hg, pulse is 80/min, and respirations are 20/min. A pericardial friction rub is heard on chest auscultation. The rest of the examination shows no abnormalities. EKG shows ST segment elevation in all leads, with elevation of the PR segment in lead aVR. The chest x-ray is normal. Urinalysis shows hematuria, red cell casts and mild proteinuria. Laboratory studies show a BUN level of 60 mg/dl and a serum creatinine level of 3 8 mg/dl. What is the most appropriate next step in management?
A. Broad spectrum antibiotics
B. Intravenous steroids
C. Hemodialysis
D. Thrombolytic therapy
E. NSAIDs
38. A 22-year -old man comes to the physician because of a 2-day history of dark urine. He has had an upper respiratory tract infection for 3 days. His temperature is 37.1 C (98.9F), blood pressure is 145/90mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows no abnormalities. Laboratory studies show: Urinalysis: Glucose Negative Protein 1+ Ketones Negative Leukocyte esterase Negative Nitrites Negative WBC 3-6/hpf RBC 30-50/hpf Casts RBC Serum chemistry: Serum Na 138 mEq/L Serum K 4.5 mEq/L Bicarbonate 22 mEq/L BUN 30 mg/dL Serum creatinine 1.8 mg/dL Serum complement level is within normal limits. Which of the following is the most likely diagnosis?
A. IgA nephropathy
B. Acute interstitial nephritis
C. Acute post-infectious glomerulonephritis
D. Anti-glomerular basement membrane disease
E. Benign recurrent hematuria
39. A 3-year-old girl is brought to the emergency department because of fever, chills, vomiting, and abdominal pain. Her temperature is 39.5C (103.1F), blood pressure is 70/40 mm Hg, pulse is 110/min, and respirations are 20/min. She is restless and diaphoretic. The abdominal examination shows right costovertebral tenderness. Laboratory studies show: Hemoglobin 15.0 g/L Platelets 260,000/mm3 Leukocyte count 16,500/mm3 BUN 20 mg/dL Serum creatinine 1.1 mg/dL Urinalysis: Blood Negative Glucose Negative Ketones Negative Leukocyte esterase Positive Nitrites Positive WBC 40-50/hpf RBC 5-9/hpf Blood and urine cultures are taken. Which of the following is the most appropriate next step in management?
A. Empiric therapy with oral antibiotics
B. Empiric therapy with intravenous antibiotics
C. Renal ultrasound
D. Voiding cystoureterogram
E. Plain abdominal x-ray
40. A 27-year-old man comes to the physician because of red urine. He has had no pain or burning on urination. He has infiltrative pulmonary tuberculosis (diagnosed recently). He takes isoniazid, rifampin, and pyrazinamide. He smokes two packs a day and consumes alcohol occasionally. Vital signs are stable Physical examination shows no abnormalities. Which of the following is the most likely diagnosis?
A Acute cystitis
B. Renal tuberculosis
C. Drug reaction
D. Nephrolithiasis
E. Glomerulopathy
41. An 18-year-old girl comes to the emergency department with a rash and arthralgias. She is sexually active and has had the same sexual partner for the past 4-months. Recent medical history is significant for an episode of dysuria and increased urinary frequency, both of which started 5-days ago. Her primary care physician prescribed TMP+SMX (Bactrim) for this. She developed her present symptoms 3-days after starting the medication. Her aunt has Lupus. Her temperature is 38.5C(101.3F), pulse is 86/min, and respirations are 16/min. Physical examination shows a disseminated maculopapular rash; there is no costovertebral tenderness or flank pain; serum creatinine is 2 mg/dL. Urinalysis shows 2-5 RBC/hpf, numerous white blood cell casts made mostly of eosinophils, and mild proteinuria. Which of the following is the most likely diagnosis?
A. Disseminated gonococcemia
B. Post-infectious acute glomerulonephritis
C. Drug induced interstitial nephritis
D. Lupus nephritis
E. Pyelonephritis
42. A 47-year-old diabetic woman comes to the physician due to the recent onset of tremors. She has undergone combined pancreatic and kidney transplantation secondary to end stage renal disease and diabetes. She takes multiple medications, including immunosuppressants. Her temperature is 36.1 C (97F), blood pressure is 152/90 mm Hg, pulse is 78/min, and respirations are 16/min. Examination shows gum hypertrophy. Laboratory studies show: Hb 13.0 g/dl WBC 8,000/cmm Serum Na 135 mEq/L Serum K 5.3 mEq/L BUN 26 mg/dl Serum Creatinine 1.7 mg/dl Which of the following immunosuppressants is most likely responsible for her presentation?
A. Tacrolimus
B. Cyclosporine
C. Azathioprine
D. Mycophenolate
E. Diuretic
43. A 45-year-old male patient comes to the physician's office for a routine check-up. He denies any symptoms and says he feels "perfectly healthy." He was diagnosed with hypertension and mixed hypercholesterolemia a year ago. He is currently taking hydrochlorothiazide, amiloride and simvastatin daily. He does not use tobacco, alcohol or drugs. His blood pressure today is 135/85 mm Hg. Physical examination shows no abnormalities. Routine blood results reveal the following: CBC: Hb 14.2g/dL Ht 42% MCV 86 fl Platelet count 260,000/cmm Leukocyte count 8,500/cmm Neutrophils 70% Eosinophils 1% Lymphocytes 24% Monocytes 5% Serum: Serum Na 140 mEq/L Serum K 5.7 mEq/L Chloride 100 mEq/L Bicarbonate 24 mEq/L BUN 10 mg/dL Serum Creatinine 1.1 mg/dL Calcium 9.0 mg/dL Blood Glucose 118 mg/dL Total cholesterol 220 mg/dL LDL cholesterol 130 mg/dL The blood sample is checked and is not hemolysed. The EKG shows normal sinus rhythm. What is the most appropriate next step in the management of this patient?
A. Intravenous calcium gluconate
B. Intravenous dextrose + insulin
C. Stop amiloride and recheck lab results in 1 week
D. Stop HCTZ and recheck lab results in 1 week
E. Start patient on a low potassium diet
44. A 26-year-old woman presents with a one-week history of dysuria and increased urinary frequency. She admits to having multiple sexual partners in the past. Her temperature is 37.1C (98.9F), blood pressure is 110/70 mm Hg, pulse is 68/min, and respirations are 15/min. Examination shows suprapubic tenderness. Mucopurulent discharge is observed at the urethral os. Urinalysis shows: Blood Negative Glucose Negative Ketones Negative Leukocyte esterase Positive Nitrites Negative WBC 40-50/hpf RBC 1-2/hpf Bacteria None Urine culture after 24hours < 100colonies/ml. Which of the following is the most likely diagnosis?
A. Acute pyelonephritis
B. Acute bacterial cystitis
C. Chlamydial urethritis
D. Gonococcal urethritis
E. Trichomonal vaginitis
45. A 60-year-old man comes to the physician because of worsening fatigue and nausea. He had a carotid angiogram for the evaluation of symptomatic carotid artery stenosis 15 days ago, and was discharged home three days after the procedure. His medical problems are hypercholesterolemia, coronary artery disease, intermittent claudication, hypertension for 18 years, and diabetes mellitus for 15 years. Physical examination shows painless, reddish-blue mottling of the skin of the extremities. Laboratory studies show: Hb 10.5 g/dl WBC 10,000/cmm with 12% eosinophils BUN 46 mg/dl Serum creatinine 3.0 mg/dl Serum C 3 level Decreased Urinalysis: pH Normal Esterase Negative Nitrite Negative Protein 1+ WBC Many eosinophils RBC 1-2/HPF Which of the following is the most likely cause of this patient's findings?
A. Contrast nephropathy
B. Cholesterol embolism
C. Diabetic nephropathy
D. Post streptococcal glomerulonephritis
E. Acute allergic interstitial nephropathy
46. A 50-year-old man comes to the emergency department due to a sudden onset of severe, colicky pain in the right flank. He was admitted twice in the past for similar complaints; he was managed conservatively and sent home on both occasions. He has no other medical problems. He does not use tobacco, alcohol or drugs. His vital signs are stable. He is given IV fluids and narcotics. Laboratory studies show: Hb 14.5 g/dL WBC 13,000/cmm; no bands Platelets 300,000/cmm BUN 16 mg/dl Serum Creatinine 0.8 mg/dl CT scan of the abdomen without contrast shows renal calculi. Which of the following is the best advice for the prevention of future stones in this patient?
A. Decrease dietary calcium intake
B. Mega doses of Vitamin C
C. Decrease dietary protein and oxalate
D. Restrict fluid intake
E. Increase sodium intake
47. A 45-year-old man comes to the emergency department (ED) with severe right flank pain. He is tossing in bed due to the pain. KUB done in the ED shows no abnormalities; however, abdominal ultrasound shows a 5 mm stone in the right ureter. Urinalysis shows: Urine pH 4.5 (normal is 5-6) WBC Absent RBC 2-3/HPF Bacteria Absent Nitrites Negative Esterase Negative Which of the following is the most beneficial next step in management?
A. Oral sodium bicarbonate
B. Hydrochlorothiazide
C. Furosemide
D. High-protein diet
E. Calcium-restricted diet
48. A 57-year-old man comes to the physician because of 2 episodes of hematuria. He also complains of cough fatigue and fever for several days. He has smoked two packs of cigarettes daily for 25 years. He does not use alcohol or drugs. Vital signs are stable. Examination shows a left-sided varicocele which fails to empty when the patient is recumbent; examination otherwise shows no abnormalities. Laboratory studies show Hb of 16.2 g/dl and platelets of 480,000/cmm. Which of the following is the most appropriate diagnostic step in management?
A. Chest x-ray
B. Abdominal CT scan
C. Urinalysis
D. Serum alfa-fetoprotien levels
E. Ultrasonogram of the testicles
49. A 64-year-old male with a past medical history of hypertension, diabetes and chronic renal insufficiency presents with gross hematuria. His baseline serum creatinine is 1.6-1.7 mg/dl. The patient's medications include aspirin, hydrochlorothiazide, enalapril, and simvastatin. He has no known environmental, medication, or contrast allergies. On physical examination, the patient has a blood pressure of 130/80 mm Hg. The examination is otherwise unremarkable. Contrast CT scan of the abdomen is planned to evaluate his condition. Which of the following interventions would be most helpful in preventing contrast-induced kidney damage?
A. Prednisone
B. Non-ionic contrast agent
C. Furosemide
D. 100% oxygen mask
E. Stopping simvastatin
50. A patient with benign prostatic hyperplasia has moderately severe symptoms and is started on finasteride. After six months of treatment with finasteride, his symptoms improve remarkably and his prostate has regressed in size. Which of the following histological patterns was most likely present at the time of initiation of treatment?
A. Hyperplasia of prostate with predominance of epithelial components
B. Hyperplasia of prostate with predominance of muscular element
C. Hyperplasia of prostate with predominance of collagen
D. Hyperplasia of prostate with predominance of both collagen and smooth muscles
E. Hyperplasia of prostate with predominance of glandular tissue
51. A 60-year-old man comes to the physician's office because of fatigue and hematuria. His past medical history is significant for fatty liver, gout, and anemia. He has smoked two packs of cigarettes daily for 40 years. He is a heavy alcohol drinker. His last visit to his physician was 1 month agoforthe 'flu'. His temperature is 37.1C (98.9F), blood pressure is 145/90mm Hg, pulse is 78/min, and respirations are 14/min. Examination shows no abnormalities. Dipstick testing is positive for hematuria. Laboratory studies show: Urinalysis: Glucose Negative Ketones Negative Leukocyte esterase Negative Nitrites Negative WBC 1-2/hpf RBC 1-2/hpf Casts Epithelial cell Serum chemistry: Serum Na 140 mEq/L Serum K 5.0 mEq/L Bicarbonate 20 mEq/L BUN 36 mg/dL Serum creatinine 34 mg/dL Which of the following is the most likely diagnosis?
A. Post infectious glomerulonephritis
B. Hepatorenal syndrome
C. Rhabdomyolysis
D. Renal cell cancer
E. Bladder cancer
52. A 50-year-old man comes to the physician because of a skin rash, joint pains, malaise and fatigue. He has a history of intravenous drug abuse. His temperature is 37.1 C (98.9F), blood pressure is 140/90 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows palpable purpura and hepatosplenomegaly. Urinalysis shows hematuria, red blood cell casts and proteinuria. The results of the laboratory studies are as follows: BUN 30 mg/dl Creatinine 2.0 mg/dl Serum complement Low Anti-HCV Positive Which of the following is the most likely diagnosis?
A. Alpert's syndrome
B. Acute interstitial nephritis
C. Acute post infectious glomerulonephritis
D. Mixed essential cryoglobulinemia
E. Benign recurrent hematuria
53. A 40-year-old man comes to the physician because of a two-week history of fatigue, lower extremity edema and dark urine. He has no history of serious illnesses. He takes no medications. He does not use tobacco, alcohol, or drugs. His blood pressure is 130/80 mm Hg and pulse is 80/min. Physical examination shows symmetric pitting edema of lower extremities. Laboratory studies show a serum creatinine level of 1.1 mg/dl. Urinalysis shows 4+ proteinuria and microhematuria. Light microscopy of the specimen obtained from kidney biopsy shows dense deposits within glomerular basement membrane that stain for C3, not immunoglobulins. Which of the following is the most likely pathophysiologic mechanism that explains this patient's condition?
A. Anti-GBM antibodies
B. Circulating immune complexes
C. Persistent activation of the alternative complement pathway
D. Cell-mediated injury
E. Non-immunologic damage
54. A 35-year-old man comes to the physician due to a one-month history of weight gain and facial edema. The facial edema resolves at the end of the day, but ankle edema develops. His temperature is 37.2C (99F), blood pressure is 142/80 mm Hg, pulse is 80/min, and respirations are 16/min. Examination shows 2+ ankle edema. Laboratory studies show: Hb 11.0 g/dl WBC 8,000/cmm Platelets 200,000/cmm Serum Na 135 mEq/L Serum albumin 2.2 g/dl BUN 16 mg/dl Serum creatinine 1.0 mg/dl Urinalysis: Glucose Absent Protein 4+ WBC 1-2/HPF RBC Absent Casts Fatty casts This patient is most likely at risk for developing which of the following?
A. Rupture of brain aneurysm
B. Abdominal aortic aneurysm
D. Pulmonary hemorrhage
C. Hypercoagulability
E. Gall stone pancreatitis
55. A 65-year-old woman comes to the physician because of a two-month history of fatigue and weight gain. She has rheumatoid arthritis and hypertension. She takes hydrochlorothiazide and naproxen. She does not use tobacco, alcohol, or drugs. Her blood pressure is 120/70 mm Hg, pulse is 80/min, and respirations are 14/min. Physical examination shows generalized edema; liver is palpated 2 cm below the costal margin. Urinalysis shows 4+ proteinuria. Ultrasound of the kidneys shows slight enlargement. Renal biopsy was performed. Which of the following is the most likely finding on renal specimen analysis?
A. Crescent formation on light microscopy
B. Deposits revealed under polarized light
C. Linear immunoglobulin deposits revealed on immunofluorescence microscopy
D. Granular immunoglobulin deposits revealed on immunofluorescence microscopy
E. Normal light microscopy findings
56. A 65-year-old male comes to the physician's office after noticing blood in his urine. He denies any abdominal pain or dysuria. He denies any recent illness. The review of systems is otherwise unremarkable. His past medical history is significant for hypertension and a transient ischemic attack. He takes a baby aspirin and hydrochlorothiazide daily. His temperature is 36.7C (98F), blood pressure is 130/86 mm Hg, pulse is 80/min and respirations are 16/min. A complete physical examination is unremarkable. Which of the following is the most likely cause of his symptoms?
A. Polycystic kidney disease
B. Renal cell carcinoma
C. Bladder mass
D. Acute glomerulonephritis
E. Schistosoma infection
57. A 73-year-old man comes to the physician because of a one-year history of progressively worsening urinary urgency, hesitancy, nocturia, and weak urinary stream. He has no fever, abdominal pain, hematuria, malaise or weight loss. He takes atenolol for essential hypertension. He has no history of diabetes mellitus or ischemic heart disease. He does not use tobacco, alcohol, or drugs. Rectal examination shows a smooth, firm enlargement of the prostate with no induration or asymmetry. Neurological examination shows no abnormalities. Urinalysis shows no abnormalities. Laboratory studies show serum creatinine of 2.1 mg/dl. Which of the following is the most appropriate next step in management?
A. Ultrasound of kidneys, ureters, and bladder
B. Watchful waiting
C. Transurethral resection of prostate
D. Treatment with finasteride
E. Treatment with prazosin
58. A 26-year-old man comes to the emergency department because of a sudden onset of severe right-sided flank pain. The pain is colicky and radiates from the flank to the scrotum. He also has nausea, vomiting and dark-colored urine. He has never had these symptoms before. His temperature is 37C (98.6F), blood pressure is 126/70 mm Hg, pulse is 90/min, and respirations are 18/min. Examination shows no abnormalities. He is given adequate analgesia. Non- contrast helical CT shows a 4 mm radiopaque stone in the right upper ureter. Laboratory studies show serum calcium of 9.8 mg/dl, serum creatinine of 0.9 mg/dl, and BUN of 15mg/dl. Urinalysis shows hematuria but no casts. Which of the following is the most appropriate next step in management?
A. 24 hr urine collection for metabolic evaluation
B. Reassurance
C. Fluid intake greater than 2 Uday
D. Intake of potassium citrate
E. Restriction of dietary oxalate
59. A 27-year-old man comes to the physician because of a 2-day history of periorbital swelling. He was treated with oral dicloxacillin for a skin infection 3-weeks ago. His urine has turned darker. His temperature is 37.4C (99.4F), blood pressure is 150/90 mm Hg, pulse is 80/min, and respirations are 15/min. Examination shows periorbital swelling. Urinalysis shows 8 RBCs/HPF with RBC casts and a mild proteinuria. Laboratory studies show low serum C3 levels; BUN is 40 mg/dl and serum creatinine is 2 mg/dl. Which of the following is the most likely diagnosis?
A. Drug-induced acute interstitial nephritis
B. Acute pyelonephritis
D. Membranoproliferative glomerulonephritis
C. Post streptococcal glomerulonephritis
E. lgA nephropathy
60. A 27 -year-old man comes into the emergency department because of a 2-week history of hemoptysis, breathing difficulty, ankle edema, and dark urine. His past medical history is insignificant. He is not taking any medication. He does not use tobacco, alcohol, or drugs. Laboratory studies show: Hb 10.5 g/dl Serum Na 135 mEq/L Serum K 4.8 mEq/L BUN 36 mg/dl Serum creatinine 2.8 mg/dl Urinalysis shows numerous dysmorphic red blood cells/HPF, moderate proteinuria, and red cell casts. Chest x-ray reveals bilateral alveolar infiltrates. Diagnosis of which of the following pulmonary-renal syndromes require emergency plasmapheresis?
A. Goodpasture's syndrome
B. Wegener's granulomatosis
C. SLE-associated nephritis
D. Polyarteritis nodosa
E. Idiopathic rapidly progressive glomerulonephritis (RPGN)
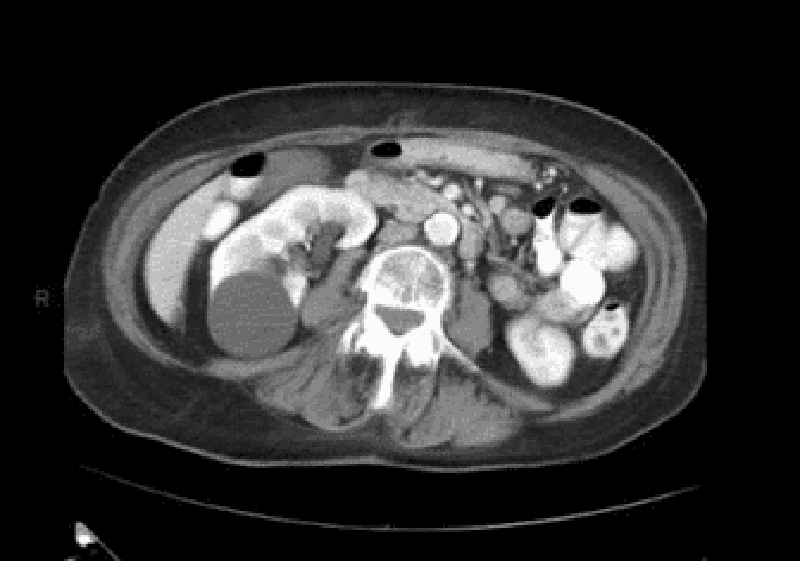
61. A healthy 54-year-old man comes to the physician for a routine health maintenance examination. He has no complaints, but he is requesting for a CT scan of the abdomen. His father died at the age of 60 due to the sudden rupture of an undiagnosed abdominal aortic aneurysm. He has a history of hypertension and gouty arthritis. His social history is not significant. His vital signs are stable. Physical examination shows no abnormalities. ACT scan of the abdomen is shown below.Which of the following is the most appropriate next step in management?
A. Reassurance
B. Surgery
C. CT guided biopsy
D. Antibiotics
E. Repeat CT scan in 3 months
62. A 30-year-old woman comes to the office due to the recent onset of fever, chills, and dysuria. Her temperature is 38.3C (101.0F), blood pressure is 110/70mm Hg, pulse is 68/min, and respirations are 15/min. Examination shows tenderness at the right costovertebral angle. Laboratory studies show WBC count of 16,000/microl with left shift. Urinalysis shows bacteriuria and pyuria. Her urine and blood is collected for culture and sensitivity. She is prescribed oral ciprofloxacin and sent home. After three days, she returns for a follow-up visit. She is still febrile, and the physical examination is unchanged. The blood cultures have no growth after 72 hours of incubation. Results of the urine culture show:Which of the following is the most appropriate next step in management?
A. Start intravenous ampicillin and gentamicin
B. Start intravenous ciprofloxacin
C. Continue oral ciprofloxacin for another 10 days
D. Perform renal ultrasound
E. Renal CT scan
63. A 62-year-old woman presents to your office complaining of urinary frequency and burning during urination. She denies fever, chills, nausea, back pain or abdominal pain. Her past medical history is significant for a long history of diabetes mellitus and hypertension. She does not use tobacco or consume alcohol. Her blood pressure is 160/100 mmHg and her heart rate is 70/min. Her hematocrit is 43% and her WBC count is 8,500/mm3 Urinalysis reveals the following:Glucose negative Ketones negative Nitrates positive Protein 2+ WBC 20-25/hpf RBC 3-5/hpf She is given a three-day course of levofloxacin. Urinalysis two weeks later reveals 2+ protein but no nitrates, WBCs, or RBCs. Which of the following is most likely responsible for her persistent urinalysis abnormality?
A. Atherosclerotic narrowing of the renal arteries
B. Glomerular basement membrane changes
C. Cystic transformation of the renal parenchyma
D. Parenchymal atrophy due to calyceal dilation
E. Insoluble crystal precipitation in the tubular lumen
64. A 72-year-old woman with poorly controlled type 2 diabetes mellitus presents to your clinic one week after being discharged from the hospital. She had been admitted with pyelonephritis secondary to a multi-drug resistant organism, and received several days of intravenous antibiotics. Her serum creatinine on admission had been 2.1 mg/dl. Today it is found to be 4.9 mg/dl. Urinalysis reveals rare epithelial casts and no white blood cells. FENa is greater than 2%. What antibiotic did she most likely receive during her hospitalization?
A Nafcillin
B. Vancomycin
C. Levofloxacin
D. Amikacin
E. Doxycycline
65. A 58-year-old man comes to the physician and complains of "problems with erection." He has recurrent and persistently painful erections. His other medical problems include ulcerative colitis, kidney stones, insomnia, depression, hypertension, drug-induced diabetes, obesity and hypercholesterolemia. He does not use tobacco, alcohol, or drugs. He takes prednisone, mesalamine, insulin, 6-mercaptopurine, simvastatin, glyburide, enalapril, trazodone, and fluoxetine. He has no known drug allergies. His vital signs are stable. The general physical examination is unremarkable. Avoidance of which of the following medications could have prevented his condition?
A. Fluoxetine
B. Trazodone
C. Enalapril
D. Glyburide
E. Simvastatin
6. A 60-year-old man comes to the physician because of a 2-day history of fever and left-sided scrotal pain. The pain has progressed in severity and it radiates to the flank. His has also had increased urinary frequency and urgency along with dysuria. His temperature is 38.1C (100.8F), blood pressure is 130/75mm Hg, pulse is 86/min, and respirations are 15/min. Physical examination shows left scrotal swelling and a tender scrotal mass; there is no urethral discharge. Rectal examination shows a tender prostate. Laboratory studies show a WBC count of 14,000/microl with a left shift. Urinalysis shows bacteriuria and pyuria. Which of the following is the most likely organism responsible for this patient's findings?
A. Escherichia coli
B. Pseudomonas
C. Chlamydia trachomatis
D. Gonococcus
E. Staphylococcus aureus
67. A 40-year-old man comes to the physician because of increasing urinary frequency and urgency. He has had these symptoms in the past, but they are more troublesome now. He has also had urinary hesitancy and interruption of flow. His temperature is 37C(98.6F), blood pressure is 130/75mm Hg, pulse is 76/min, and respirations are 15/min. Physical examination shows no abnormalities except increased tone of the anal sphincter and mild periprostatic tenderness. Urinalysis and urine culture shows no abnormalities and expressed prostatic secretions show a leukocyte count of four WBCs/HPF (normal is less than 10 WBCs/HPF). Serum prostate-specific antigen is 2 ng/ml (normal value is less than 4ng/ml). Which of the following is the most likely diagnosis?
A. Chronic bacterial prostatitis
B. Inflammatory chronic prostatitis
C. Non-inflammatory chronic prostatitis
D. Prostatic cancer
E. Acute bacterial prostatitis
68. A 16-year-old girl presents with a 2-day history of lower abdominal discomfort, burning micturition and increased frequency of urination. She had her first sexual intercourse last week. Her vital signs are stable. Examination shows suprapubic tenderness. Urinalysis shows positive nitrites, positive esterase, 50+ WBC, and many bacteria. Which of the following is the most likely mechanism responsible for her clinical condition?
A. Sexual transmission
B. Hematogenous spread of infection
C. Lymphatic spread of infection
D. Poor genital hygiene
E. Ascending infection
69. A 68-year-old Caucasian man is admitted with a diagnosis of left lower lobe pneumonia, and is started on gatifloxacin. He has a long history of diabetes, hypothyroidism, hypercholesterolemia, and hypertension. He also has diabetic retinopathy, peripheral neuropathy, and nephropathy. He has an arterio-venous fistula placed for a possible dialysis. His medications are insulin, furosemide, atorvastatin, metoprolol and levothyroxine. After having his blood drawn for some laboratory studies today, he bleeds persistently. Laboratory studies show: Hb 11.5 g/dl Platelets 160,000/cmm Blood glucose 178 mg/dl BUN 56 mg/dl Serum creatinine 3.5 mg/dl His baseline creatinine level is between 3.2-3.5 mg/dl. Which of the following is the most likely cause of his bleeding?
A. Disseminated intravascular coagulation
B. Platelet dysfunction
C. Factor VIII deficiency
D. Consumptive coagulopathy
E. Thrombocytopenia
70. A 64-year-old man is scheduled for hemodialysis due to end stage renal disease. He has a several year history of hypertension, diabetes, coronary artery disease, hypercholesterolemia, peripheral vascular disease, gout, and diverticulosis. Six months ago, he was admitted for urosepsis. Recently, his haemoglobin has ranged between 8.5 to 9.5 g/dl. He has already been on iron therapy, and now you are considering erythropoietin injections twice weekly. Which of the following is most likely to be seen following erythropoietin therapy?
A. Worsening of his hypertension
B. Increase in insulin requirement
D. Deterioration in renal function
C. Increased susceptibility to infections
E. Flare-up of gout
71. A 70-year-old man is brought to the hospital by his son because of worsening fatigue. His son states that his father does not like seeing doctors and has not seen a physician in the past 20 years. He has no medical problems. Physical examination of the prostate shows no abnormalities. Laboratory studies show: Hb 10.5 g/dl WBC 7,400/cmm Platelets 160,000/cmm Serum Na 135 mEq/L Serum K 5.0 mEq/L BUN 50 mg/dl Serum creatinine 3.0 mg/dl Ultrasonogram of the abdomen shows bilateral small kidneys and no evidence of hydronephrosis. Kidney biopsy shows intimal thickening and luminal narrowing of renal arterioles with evidence of sclerosis. Which of the following is the most likely cause of this patient's findings?
A. Hypertension
B. Diabetes mellitus
C. Multiple myeloma
D. Analgesic abuse
E. Renal lithiasis
72. A 30-year-old woman comes to the physician due to the recent onset of occipital headaches. She has taken acetaminophen several times, but the pain returns. She has no fever or visual problems. She has not had similar episodes in the past. She has no history of serious illness. Her temperature is 36.1C (98F), blood pressure is 160/90 mm Hg, pulse is 88/min, and respirations are 16/min. Physical examination shows a rightsided renal bruit Which of the following is the most appropriate treatment for this patient's condition?
A. ACE inhibitors
B. Furosemide
C. Angioplasty with stent placement
D. Surgery
E. Oral prednisone
73. A 45-year-old man with known cirrhosis due to hepatitis C is admitted to the hospital for abdominal discomfort and confusion. Physical examination reveals a distended abdomen, leg edema, and deep yellow discoloration of the skin and sclerae. Bibasilar crackles are heard on chest auscultation. His serum sodium level is 127 mEq/L, potassium level is 2.9 mEq/L, and creatinine level is 1.3 mg/dl. On day 3 of his hospitalization, the serum creatinine is 4.2mg/dl. A urinalysis reveals: Protein negative Glucose negative WBC 4-5/hpf RBC 0-1/hpf Renal ultrasound is normal and the post-void residual urinary volume is less than 50 ml. He is given 2 L of normal saline intravenously with no change in his serum creatinine concentration. This patient's kidney dysfunction can be best corrected by which of the following?
A. High-dose spironolactone
B. ACE inhibitors
C. Liver transplantation
D. Broad spectrum antibiotics
E. Pegylated interferon
74. A 35-year-old woman who recently emigrated from Russia comes to the physician because of hematuria. She has a history of frequent headaches. Extensive evaluation did not reveal the cause of her headaches. They occur almost every day, and she tried various analgesics to relieve them. Her family history is significant for hypertension and diabetes mellitus. She does not use tobacco, alcohol, or drugs. Her blood pressure is 120/70 mm Hg and heart rate is 80/min. Physical examination shows no abnormalities. Urinalysis shows numerous unchanged red blood cells/hpf. Which of the following is the most likely cause of this patient's condition?
A Malignancy
B. Glomerular injury
D. Infection
C. Papillary necrosis
E. Nephrolithiasis
75. A 73-year-old man presents to the emergency department complaining of lower abdominal pain and nausea. He denies any vomiting or diarrhea, and his last bowel movement was two days ago. The patient also notes that several days ago he began taking amitriptyline for chronic neck pain. He does not smoke or consume alcohol. On physical examination, his blood pressure is 160/70 mmHg and his heart rate is 100/min. His lung fields are clear to auscultation. Palpation of the abdomen reveals fullness and tenderness along the midline below the umbilicus. Which of the following is the best initial management for this patient?
A. Abdominal CT scan
B. Upright abdominal x-ray
C. Barium enema
D. Broad spectrum antibiotics
E. Urinary catheterization
76. A 55-year-old woman comes to the physician for an annual physical examination. She has no new complaints, except fatigue. She has an 8-year history of chronic low back pain; severe degenerative joint disease has been documented on MRI. She had an anterior wall myocardial infarction four years ago. Her current medications include naproxen, acetaminophen, oxycodone, aspirin, atenolol, and simvastatin. Her blood pressure is 130/80 mm Hg and pulse is 72/min. Laboratory studies show: Hb 10 g/dl WBC 6,000/cmm Blood sugar 82 mg/dl BUN 36 mg/dl Serum creatinine 2.0 mg/dl Urinalysis : Protein 2+ Glucose Absent RBC Absent WBC 10-15/HPF Nitrite Negative Esterase Negative Sediment WBC casts Serum protein electrophoresis is negative for monoclonal gammopathy. Two years ago, her BUN level was 22 mg/dl, and creatinine level was 1.6 mg/dl. Which of the following is the most likely pathology involved in this patient's renal failure?
A. Acute tubular necrosis
B. Chronic glomerulonephritis
C. Tubulointerstitial nephritis
D. Recurrent pyelonephritis
E. Renal tuberculosis
77. A 56-year-old man develops oliguria three days after having a kidney transplantation. His postoperative course was uncomplicated. His blood pressure is 160/100 mm Hg and heart rate is 90/min. Palpation of the transplant reveals mild tenderness. Laboratory studies show: Serum sodium 145 mEq/L Serum potassium 5.5 mEq/L Serum calcium 8.6 mg/dl Serum creatinine 3.2 mg/dl BUN 30 mg/dl His serum cyclosporine level is normal. Renal ultrasonography does not detect dilatation of the calyces. Biopsy of the transplant shows heavy lymphocyte infiltration and vascular involvement with swelling of the intima. Which of the following is the most appropriate next step in management?
A. Decrease the dose of cyclosporine
B. Give IV steroids
C. Order ureterography
D. Administer IV diuretics
E. Prepare for surgery
78. A 50-year-old man comes to the physician for a routine follow-up visit. He has hypertension, diabetes mellitus, secondary hyperparathyroidism, and end-stage renal disease. He has been on hemodialysis for the past three years. He was admitted three months ago for line sepsis, which was treated with antibiotics. He had a right below-the-knee amputation two years ago following a non-healing foot ulcer. Physical examination shows a right carotid bruit. If this patient dies within the next five years, what would be the most likely cause of his death?
A. Cardiovascular disease
B. Stroke
C. Infection
D. Cancer
E. Withdrawal from dialysis
79. A 15-year-old boy comes to the physician because of hematuria and lower abdominal pain. This is his third episode of hematuria in the past 2 years. He has a family history of renal disease. His temperature is 37.1 C (98.9F), blood pressure is 140/90 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows mild sensorineural deafness bilaterally. Urinalysis shows hematuria and proteinuria. Laboratory studies show BUN of 50 mg/dl and serum creatinine of 3.1 mg/dL; serum complement levels are normal. Renal biopsy shows foam cells, and immunofluorescence shows no immunoglobulins or complement. Electron microscopy shows alternating areas of thinned and thickened capillary loops with splitting of GBM. Which of the following is the most likely diagnosis?
A. Alport's syndrome
B. Acute interstitial nephritis
C. Acute post infectious glomerulonephritis
D. Anti-glomerular basement membrane disease
E. Benign recurrent hematuria
80. A 25-year-old woman comes to the physician because of a 3-day history of burning micturition and increased urinary frequency. She has suprapubic discomfort. She denies having unusual vaginal discharge. She has been sexually active and monogamous for the past 4 years with her husband. Her temperature is 37.1 C (98.9F), blood pressure is 110/70 mm Hg, pulse is 68/min, and respirations are 15/min. Examination shows suprapubic tenderness without flank tenderness. The rest of the examination is normal. Urinalysis shows: Specific gravity 1.020 Blood Trace Glucose Negative Ketones Negative Leukocyte esterase Positive Nitrites Positive WBC 40-50/hpf RBC 6-10/hpf Bacteria 50+ Which of the following is the most appropriate next step in management?
A. Urine culture
B. Oral trimethoprim-sulfamethoxazole
D. Oral nitrofurantoin
C. Oral ciprofloxacin
E. Intravenous trimethoprim-sulfamethoxazole
81. A 57 -year-old woman is admitted to the ICU after being involved in a highway motor vehicle accident. She was hypotensive at the scene and received 7 litters of fluids, which included crystalloids, blood, and fresh frozen plasma. She apparently had significant external blood loss from multiple fractures and skin loss. She undergoes surgery, after which she is transferred to the ICU and receives continuous IV fluids and vasopressors. Her laboratory studies 24 hours after the accident show the following: Hb 9.5 g/dl WBC 15,000/cmm Platelets 130,000/cmm BUN 34 mg/dl Serum Creatinine 2.2 mg/dl Which of the following is the most likely microscopic finding on urinalysis?
A. Broad cast
B. Muddy brown cast
C. RBC casts
D. WBC casts
E. Fatty casts
82. A 56-year-old male with a long history of diabetes mellitus complains of nocturnal urinary frequency, occasional dribbling and difficulty completing his stream. His past medical history is significant for a myocardial infarction two years ago and moderately decreased visual acuity. On physical examination, his blood pressure is 160/100 mmHg and his heart rate is 70/min. There is a carotid bruit auscultated on the left side as well as trace ankle edema. Post-void bladder catheterization yields 60 ml of urine. Dipstick urinalysis reveals 2+ protein and 3-4 WBC/hpf. The patient's serum creatinine level is 2.4 mg/dl. Which of the following is the most likely cause of his renal dysfunction?
A. Ascending infection
B. Obstructive uropathy
D. Renal hypoperfusion
C. Microangiopathy
E. Cystic kidney disease
83. A 34-year-old man is being evaluated for possible end-stage renal disease. He has a long history of diabetes, type 1. He previously developed chronic renal insufficiency despite being on enalapril and insulin. His renal function is getting worse day by day. A nephrologist is currently managing his renal condition. Which of the following long-term treatments would give the best survival rate for this patient?
A. Hemodialysis
B. Peritoneal dialysis
D. Renal transplantation from a living related donor
C. Renal transplantation from a cadaver
E. Renal transplantation from a living unrelated donor
84. A 17-year-old African American man comes to the physician after an episode of gross hematuria that resolved spontaneously. He has no other complaints. His past medical history is insignificant. He takes no medications. He smokes occasionally. He does not use drugs or alcohol. His temperature is 36.7C (98F), blood pressure is 120/70 mm Hg, pulse is 70/min, and respirations are 14/min. Physical examination shows no abnormalities. Urinalysis shows many unchanged red blood cells/HPF, but is otherwise normal. Laboratory studies show a creatinine level of 0.9 mg/dl. Which of the following is the most likely diagnosis?
A. Acute glomerulonephritis
B. Acute interstitial nephritis
C. Sickle cell trait
D. Coagulopathy
E. Acute cystitis
85. A 34-year-old woman comes to the physician's office because of occasional headaches and palpitations. She has no other medical problems. She takes no medications. She smokes one and a half packs of cigarettes daily. Her blood pressure is 170/100 mm Hg in both arms, and heart rate is 80/min. Physical examination shows bilateral flank masses. Laboratory studies show: Serum sodium 140 mEq/L Serum potassium 4.4 mEq/L BUN 26 mg/dL Serum creatinine 1.3 mg/dL Urinalysis shows 10-12 red blood cells/hpf, but otherwise shows no abnormalities. The most likely complication that can occur in this patient is which of the following?
A. Liver necrosis
B. Intracranial aneurysms
D. Pancreatic cancer
C. Restrictive cardiomyopathy
E. Aortic dissection
86. A 30-year-old woman comes to the physician due to several weeks history of generalized edema, fatigue, and decreased appetite. She has no other medical problems. She takes no medications. She does not use tobacco, alcohol, or drugs. Her temperature is 36.7C (98F), blood pressure is 110/70 mm Hg, pulse is 80/min, and respirations are 18/min. Physical examination shows generalized edema. Laboratory studies show a low serum albumin level. HBsAg is positive, and liver function tests are abnormal. Urinalysis shows +4 proteinuria and microhematuria. Which of the following is the most likely diagnosis?
A. Membranoproliferative glomerulonephritis
B. Minimal change disease
D. Diffuse proliferative glomerulonephritis
C. Focal segmental glomerulosclerosis
E. Membranous glomerulonephritis
87. A 62-year-old man presents to the emergency department with severe back pain that began suddenly after he attempted to lift a heavy box. He says the pain radiates down his right thigh and leg and that coughing and moving make the pain “unbearable” The patient also complains of an inability to urinate since the pain started. On physical examination, he has no focal lower extremity weakness or numbness, and pinprick testing in the perianal area elicits a quick spasm of the anal sphincter. Rectal exam reveals an enlarged, smooth, nontender prostate. Which of the following best explains this patient's urinary retention?
A. Severe pain
B. Nerve root injury
C. Detrusor instability
D. Hypertonic bladder
E. Urethral injury
88. A 46-year-old man comes to the physician because of a 2-day history of fever and chills. His fever was gradual in onset. He also complains of perineal and back pain, which is worse towards the sacral area. He has repeated urges to urinate, along with pain on micturition. Rectal examination shows a boggy, exquisitely tender prostate. Laboratory studies show: Hb 13 gldl Hct 40% WBC 12,000/cmm Platelets 329,000/cmm Dipstick urinalysis: Esterase +++ PH 5.0 Nitrite +++ WBC 50+ Protein + Blood ++ Which of the following is the most appropriate next step in management?
A. Send culture of post-prostatic massage sample
B. Send culture of mid-stream urine sample
C. Administer alpha blocking agents
D. Start empirical treatment on an outpatient basis
E. Urethral catheterization
89. A 25-year-old woman presents with nausea and vomiting of 2 days duration. She is not on any medications and was previously well until now. Her physical examination is normal except for a postural drop in her blood pressure from 110/80 mm Hg supine to 90/80 mm Hg standing. Her serum electrolytes are sodium 130 mEq/L, potassium 3 mEq/L, chloride 90 mEq/L, bicarbonate 30 mEq/L, urea 50 mg/dL, and creatinine 0.8 mg/dL. Which of the following electrolytes is most likely to be filtered through the glomerulus but unaffected by tubular secretion?
(A) potassium
(B) sodium
(D) urea
(C) bicarbonate
(E) creatinine
90. A 19-year-old man presents with malaise, nausea, and decreased urine output. He was previously well, and his physical examination is normal except for an elevated jugular venous pressure (JVP) and a pericardial rub. His electrolytes reveal acute renal failure (ARF). Which of the following findings on the urinalysis is most likely in keeping with acute glomerulonephritis (GN)?
(A) proteinuria
(B) white blood cell casts
(D) erythrocyte casts
(C) granular casts
(E) hyaline casts
91. A 50-year-old diabetic woman presents for follow-up of her hypertension. Her blood pressure is 152/96 in the office today and she brings in readings from home that are consistently in the same range over the past month. Her current medications are amlodipine 5 mg daily and hydrochlorothiazide 25 mg daily. The diuretic was added when she developed peripheral edema on the amlodipine; now she has only trace peripheral edema. A spot urine specimen shows 280 μg of albumin per mg creatinine (microalbuminuria is present if this value is between 30 and 300 μg/mg). What would be the best next therapeutic step in this patient?
A. Add clonidine.
B. Add a beta-blocker.
C. Increase the thiazide diuretic dose.
D. Add an alpha-blocker.
E. Add angiotensin-converting enzyme inhibitor or angiotensin receptor blocker.
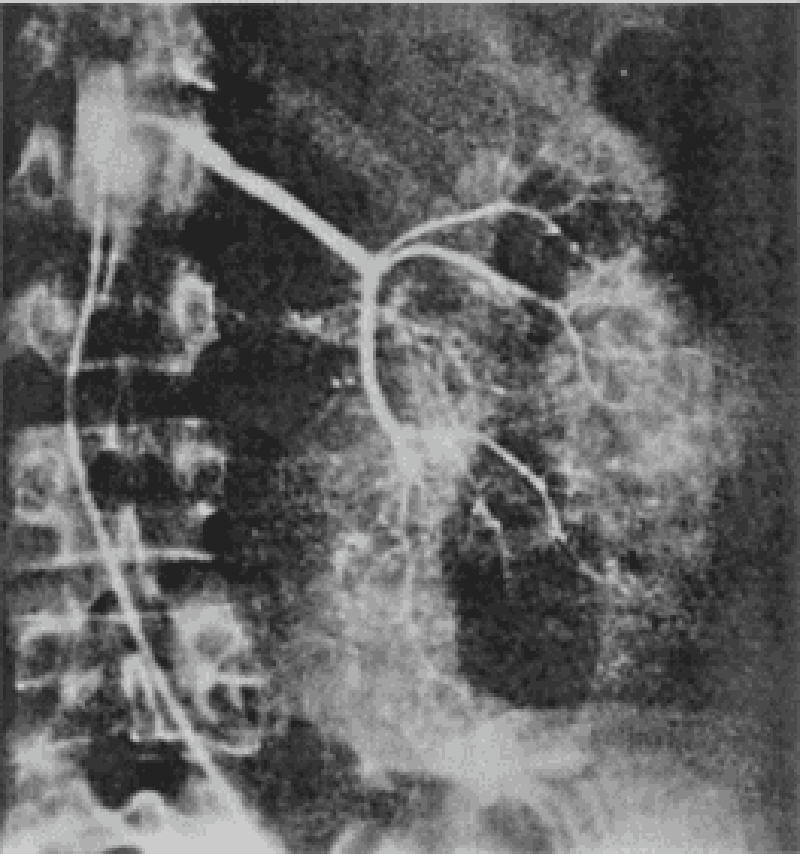
92. A 64-year-old man is admitted for hematuria after slipping on an icy pavement. His physical examination is normal. A selective angiogram of the left kidney is shown in Fig. Which of the following is the most likely diagnosis?
(A) renal cell carcinoma
(B) kidney contusion and laceration
(D) renal hamartoma
(C) transitional cell carcinoma
(E) renal hemangioma
93. A 29-year-old man with HIV, on a highly active antiretroviral therapy (HAART) regimen including the protease inhibitor indinavir, presents with severe edema and a serum creatinine of 2.0 mg/dL. He has had bone pain for 5 years and takes large amounts of acetaminophen with codeine, aspirin, and ibuprofen. He is on prophylactic trimethoprim-sulfamethoxazole. Blood pressure is 170/110; urinalysis shows 4+ protein, 5 to 10 RBC, 0 WBC; 24-hour urine protein is 6.2 g. The serum albumin is 1.9 g/L the following is the most likely cause of his renal disease?
A. Indinavir toxicity
B. Analgesic nephropathy
C. Trimethoprim-sulfamethoxazole–induced I n t e r s t I t I a l nephritis
D. Focal glomerulosclerosis
E. Renal artery stenosis
94. A 24-year-old woman presents with nausea, vomiting, anorexia, and gross hematuria. She had a sore throat 2 weeks ago that resolved on its own. On examination, her blood pressure is 160/90 mm Hg, pulse 90/min, JVP is 7 cm, heart sounds are normal, there is 1+ pedal edema, and the lungs are clear. She has a renal biopsy. Which of the following electron microscopy findings on the renal biopsy is most likely in keeping with poststreptococcal GN?
(A) diffuse mesangial deposits
(B) no deposits
(C) electron-dense endothelial deposits
(D) closed capillary lumen
(E) subepithelial humps
95. A 74-year-old man is brought to hospital because of urinary retention. He has a Foley catheter inserted to relieve the obstruction, and 1500 cc of urine is emptied from his bladder. Over the next few hours, he has 200cc/h of urine output. Which of the following urine electrolyte values is most likely in keeping with his diagnosis?
(A) high sodium
(B) low potassium
(C) high specific gravity
(D) low pH
(E) osmolality >500 mOsm/kg
96. A 64-year-old woman develops severe diarrhea 2 weeks after finishing antibiotics for pneumonia. She has also noticed decreased urine output despite drinking lots of fluids. On examination, she has a postural drop in her blood pressure, the JVP is low, and the abdomen is soft but diffusely tender. Despite giving 4 L of normal saline, her urine output remains low. The urinalysis is positive for heme-granular casts and the urine sodium is 42mEq/L. Which of the following medications should be held during the recovery phase of this woman’s ARF?
(A) acetaminophen
(B) digoxin
(C) lorazepam
(D) enalapril
(E) simvastatin
97. A 64-year-old man presents with weight gain, shortness of breath, easy bruising, and leg swelling. On examination, his blood pressure is 140/80 mm Hg, pulse 100/min, JVP 4 cm, heart sounds normal, and lungs are clear. There is a 3+ pedal and some periorbital edema. Investigations include a normal chest x-ray (CXR), electrocardiogram (ECG) with low voltages, anemia, high urea and creatinine, and 4 g/day of protein in the urine. A renal biopsy, which shows nodular deposits that have an apple-green birefringence under polarized light when stained with Congo red. Which of the following is the most likely diagnosis?
(A) amyloidosis
(B) multiple myeloma
(C) diabetic nephropathy
(D) minimal change disease
(E) immunoglobulin A (IgA) nephropathy
98. A 67-year-old man with a history of gout presents with intense pain in his right great toe. He has a complex past medical history, including hypertension, coronary artery disease, congestive heart failure, myelodysplasia, and chronic kidney disease with a baseline creatinine of 3.2 mg/dL and a uric acid level of 10 mg/dL. His medications include aspirin, simvastatin, clopidogrel, furosemide, amlodipine, and metoprolol. What is the best therapy in this situation?
A. Colchicine 1.2 mg po initially, followed by 0.6 mg 1 hour later
B. Allopurinol 100 mg po daily and titrate to uric acid less than 6 mg/dL
C. Prednisone 40 mg po daily
D. Naproxen 750 mg po once followed by 250 mg po tid
E. Probenecid 250 mg po bid
99. A 60-year-old diabetic woman develops angina and will need a coronary angiogram for evaluation of coronary artery disease. She has a creatinine of 2.2. Which of the following is the most effective in reducing the risk of contrast induced nephropathy?
A. Administer mannitol immediately after the contrast is given.
B. Perform prophylactic hemodialysis after the procedure.
C. Give IV hydration with normal saline or sodium bicarbonate prior to and following the procedure.
D. Indomethacin 25 mg the morning of the procedure.
E. Dopamine infusion before and after the procedure.
100. A 47-year-old HIV-positive man is brought to the emergency room because of weakness. The patient has HIV nephropathy and adrenal insufficiency. He takes trimethoprim-sulfamethoxazole for PCP prophylaxis and is on triple-agent antiretroviral treatment. He was recently started on spironolactone for ascites due to alcoholic liver disease. Physical examination reveals normal vital signs, but his muscles are diffusely weak. Frequent extrasystoles are noted. He has mild ascites and 1+ peripheral edema. Laboratory studies show a serum creatinine of 2.5 with a potassium value of 7.3 mEq/L. An EKG shows peaking of the T waves and QRS duration of 0.14. What is the most important immediate treatment?
A. Sodium polystyrene sulfonate (Kayexalate)
B. Acute hemodialysis
C. IV normal saline
D. IV calcium gluconate
E. IV furosemide 80 mg stat
101. An 85-year-old man who resides in a nursing home presents with a 3-day history of lower abdominal pain and increasing fatigue and lethargy. He is afebrile, his BP is 160/92, and RR 16. His lungs are clear and his heart examination normal. There is diffuse abdominal tenderness on palpation and a large area of fullness and dullness to percussion starting just below the umbilicus and extending to the suprapubic area. His serum sodium is 130 mEq/L, potassium 4.9 mEq/L, BUN 75 mg/dL, and creatinine is 3.5 mg/dL. His baseline BUN and creatinine were 25 and 1.3 respectively as recently as 1 month ago. A Foley catheter is placed and 1200 cc of urine is obtained. What will be the likely clinical course for this patient with regard to his renal function?
A. His creatinine will continue to rise slowly for 2 to 3 more days.
B. His creatinine will return to 1.3 over the next week.
C. He will require dialysis within 24 hours.
D. He will produce minimal urinary output for at least 3 days.
E. His renal function is unlikely to show any improvement in the future and 3.5 will be his new baseline.
102. A 74-year-old man presents with fatigue, shortness of breath on exertion, and back and rib pain, which is made worse with movement. Investigations reveal he is anemic, calcium, urea, and creatinine are elevated. X-rays reveal multiple lytic lesions in the long bones and ribs, and protein electrophoresis is positive for an immunoglobulin G (IgG) paraprotein. Which of the following is the most likely mechanism for the renal injury?
(A) plasma cell infiltrates
(B) tubular damage by light chains
(C) glomerular injury
(D) vascular injury by light chains
(E) uric acid crystals
103. 25-year-old man is referred to you because of hematuria. He noticed brief reddening of the urine with a recent respiratory infection. The gross hematuria resolved, but his physician found microscopic hematuria on two subsequent first-voided morning urine specimens. The patient is otherwise healthy; he does not smoke. His blood pressure is 114/72 and the physical examination is normal. The urinalysis shows 2+ protein and 10 to 15 RBC/hpf, with some dysmorphic erythrocytes. No WBC or casts are seen. What is the most likely cause of his hematuria?
A. Kidney stone
B. Renal cell carcinoma
C. Acute poststreptococcal glomerulonephritis
D. Chronic prostatitis
E. IgA nephropathy (Berger disease)
104. A 17-year-old man is brought to the emergency room with confusion and incoordination. He is uncooperative and refuses to provide further history. Physical examination reveals an RR of 30; the vital signs are otherwise normal as is the general physical examination. Laboratory values are as follows: Na: 135 mEq/L K: 2.7 mEq/L HCO3: 15 mEq/L Cl: 110 mEq/L Arterial blood gases: PO2 92, PCO2 30, pH 7.28 Urine: pH 7.5, glucose—negative Ca: 9.7 mg/dL PO4: 4.0 mg/dL Which of the following is the most likely cause of the acid base disorder?
A. GI loss owing to diarrhea
B. Proximal renal tubular acidosis
C. Disorder of the renin-angiotensin system
D. Distal renal tubular acidosis
E. Respiratory acidosis
105. A 56-year-old man presents with hypertension and peripheral edema. He is otherwise healthy and takes no medications. Family history reveals that his father and a brother have kidney disease. His father was on hemo-dialysis before his death at age 68 of a stroke. Physical examination reveals BP 174/96 and AV nicking on funduscopic examination. He has a soft S4 gallop. Bilateral flank masses measuring 16 cm in length are palpable. Urinalysis shows 15 to 20 RBC/hpf and trace protein but is otherwise normal; his serum creatinine is 2.4 mg/dL. Which is the most likely long-term complication of his condition?
A. End-stage renal disease requiring dialysis or transplantation
B. Malignancy
C. Ruptured cerebral aneurysm
D. Biliary obstruction owing to cystic disease of the pancreas
E. Dementia
106. A 64-year-old man presents with symptoms of malaise, shortness of breath, edema, and no urine output for 24 hours. His past medical history is not significant, and his only medication is daily aspirin. On examination his JVP is 4 cm, heart sounds are normal, lungs are clear, and the abdomen is soft. A Foley catheter is inserted into his bladder for 200 cc of urine, which is sent for urinalysis. His urine output still remains low. Which of the following is the most appropriate initial diagnostic test?
(A) renal ultrasound
(B) blood cultures
(C) urine cultures
(D) inferior vena cavagram with selective renal venogram
(E) blood urea nitrogen (BUN)/creatinine ratio
07. 28-year-old woman presents with a recent episode of coughing up some blood, frequent nosebleeds, and now decreased urine output. A nasal mucosa ulcer was seen on inspection. Her urinalysis is positive for protein and red cells consistent with a GN. The CXR shows two cavitary lesions and her serology is positive for antineutrophil cytoplasmic antibodies (ANCA). Which of the following is the most likely diagnosis?
(A) Wegener’s granulomatosis
(B) bacterial endocarditis
(C) Goodpasture’s syndrome
(D) lupus erythematosus
(E) poststreptococcal disease
108. 74-year-old woman develops acute sepsis from pneumonia and is admitted to the intensive care unit because of hypotension. She is started on antibiotics, and her blood pressure is supported with intravenous normal saline. Despite this she remains oliguric and develops ARF. Her urinalysis has heme-granular casts and the urine sodium is 56 mEq/L. Which of the following is the most likely cause of her ARF?
(A) nephrotoxic antibiotics
(B) acute infectious GN
(C) acute tubular necrosis (ATN)
(D) contrast nephropathy
(E) cholesterol emboli
109. A 46-year-old woman with nausea and vomiting presents to hospital because of light- headedness when standing and decreased urine output. She looks unwell; the blood pressure supine is 90/60 mm Hg and 80/60 mm Hg when standing. Her abdominal, heart, and lung examinations are normal. Which of the following laboratory values suggests prerenal azotemia in this patient?
(A) markedly elevated urea, unchanged creatinine
(B) unchanged urea, elevated creatinine
(C) little change in either creatinine or urea for several days after oliguria develops
(D) urea/creatinine ratio of 10
(E) urea/creatinine ratio of 25
110. A 76-year-old man presents to the emergency room. He had influenza and now presents with diffuse muscle pain and weakness. His past medical history is remarkable for osteoarthritis for which he takes ibuprofen, and hypercholesterolemia for which he takes lovastatin. Physical examination reveals blood pressure of 130/90 with no orthostatic change. The only other finding is diffuse muscle tenderness. Laboratory data include BUN: 30 mg/dL Creatinine: 6 mg/dL K: 6.0 mEq/L Uric acid: 18 mg/dL Ca: 6.5 mg/dL PO4: 7.5 mg/dL UA: large blood, 2+ protein. Microscopic study shows muddy brown casts and 0 to 2 rbc/hpf (red blood cells/high power field). Which of the following is the most likely diagnosis?
A. Nonsteroidal anti-inflammatory drug-induced acute kidney injury (AKI)
B. Volume depletion
C. Rhabdomyolysis-induced acute kidney injury
D. Urinary tract obstruction
E. Hypertensive nephrosclerosis
111. A 20-year-old man presents with obtundation. Past medical history is unobtainable. Blood pressure is 120/70 without orthostatic change, and he is well perfused The neurological examination is nonfocal. His laboratory values are as follows: Na: 138 mEq/L K: 4.2 mEq/L HCO3: 5 mEq/L Cl: 104 mEq/L Creatinine: 1.0 mg/dL BUN: 14 mg/dL peripherally. Ca: 10 mg/dL Arterial blood gas on room air: PO2 96, PCO2 15, pH 7.02 Blood glucose: 90 mg/dL Urinalysis: normal, without blood, protein, or crystals. Which of the following is the most likely acid-base disorder?
A. Pure normal anion-gap metabolic acidosis
B. Respiratory acidosis
C. Pure high anion-gap metabolic acidosis
D. Combined high anion-gap metabolic acidosis and respiratory alkalosis
E. Combined high anion-gap metabolic acidosis and respiratory acidosis
112. A 23-year-old woman with no other past medical history was diagnosed with hypertension 6 months ago. She was initially treated with hydrochlorothiazide, followed by the addition of lisinopril, followed by high doses of a beta-blocker, but her blood pressure has not been well controlled. She assures the provider that she is taking all of her medicines. On examination her blood pressure is 165/105 in each arm, and 168/105 when checked by large cuff in the lower extremities. Her pulse is 60. Cardiac examination reveals an S4 gallop but no murmurs. She has a soft mid-abdominal bruit. Distal pulses are intact and equal. She does not have hyperpigmentation, hirsutism, genital abnormalities, or unusual distribution of fat. Her sodium is 140, potassium 4.0, HCO3 22, BUN 15, and creatinine 1.5. Which of the following is the most likely cause of her difficult-to-control hypertension?
A. Primary hyperaldosteronism (Conn syndrome)
B. Cushing syndrome
D. Fibromuscular dysplasia
E. Coarctation of the aorta
C. Congenital adrenal hyperplasia
113. A 73-year-old man undergoes abdominal aortic aneurysm repair. The patient develops hypotension to 80/50 for approximately 20 minutes during the procedure according to the anesthesia record. He received 4 units of packed red blood cells. Postoperatively, his blood pressure is 110/70, heart rate is 110, surgical wound is clean, and a Foley catheter is in place. Over the next 2 days his urine output slowly decreases. His creatinine on post-op day 3 is 3.5 mg/dL (baseline 1.2). His sodium is 140 mEq/L, K 4.6 mEq/L, and BUN 50 mg/dL. Hemoglobin and hematocrit are stable. Urinalysis shows occasional granular casts but otherwise is normal. Urine sodium is 50 mEq/L, urine osmolality is 290 mosmol/L, and urine creatinine is 35 mg/dL. The FeNa (fractional excretion of sodium) based on these data is 3.5. What is the most likely cause of this A. Acute interstitial nephritis B. Acute glomerulonephritis C. Acute tubular necrosis@ D. Prerenal azotemia E. Contrast induced nephropathy patient’s acute renal failure?
A. Acute interstitial nephritis
B. Acute glomerulonephritis
C. Acute tubular necrosis
D. Prerenal azotemia
E. Contrast induced nephropathy
114. A 73-year-old woman with arthritis presents with confusion. Neurologic examination is nonfocal, and CT of the head is normal. Laboratory data include Na: 140 mEq/L K: 3.0 mEq/L Cl: 107 mEq/L HCO3: 12 mEq/L Arterial blood gases: PO2 62, PCO2 24, pH 7.40. What is the acid-base disturbance?
A. Respiratory alkalosis with appropriate metabolic compensation
B. High anion-gap metabolic acidosis with appropriate respiratory compensation
C. Combined metabolic acidosis and respiratory alkalosis
D. No acid-base disorder
E. Hyperchloremic (normal anion gap) metabolic acidosis with appropriate respiratory compensation
115. A 17-year-old woman presents with peripheral and periorbital edema. She has previously been healthy and takes no medications. Her blood pressure is 146/92; she is afebrile. The patient has mild basilar dullness on lung examination; her cardiac examination is normal. She has periorbital edema and soft, doughy 3+ edema in her legs. Her serum creatinine is 0.6 mg/dL and her serum albumin is 2.1 g/L. Urinalysis shows 3+ protein, no RBC or WBC, and some oval fat bodies. What is the next best step to take in evaluating this patient?
A. Order serum and urine protein electrophoresis.
B. Request a nuclear medicine renal scan.
C. Measure plasma aldosterone and renin activity.
D. Order a 24-hour urine collection to quantitate the degree of proteinuria.
E. Ask a nephrologist or radiologist to perform a renal biopsy.
116. A 63-year-old man alcoholic with a 50-pack-year history of smoking presents to the emergency room with fatigue and confusion. Physical examination reveals a blood pressure of 110/70 with no orthostatic change. Heart, lung, and abdominal examinations are normal and there is no pedal edema. Laboratory data are as follows: Na: 110 mEq/L K: 3.7 mEq/L Cl: 82 mEq/L HCO3: 20 mEq/L Glucose : 100 mg/dL BUN : 5 mg/dL Creatinine: 0.7 mg/dL Urinalysis: normal Specific gravity: 1.016 Which of the following is the most likely diagnosis?
A. Volume depletion
B. Inappropriate secretion of antidiuretic hormone
C. Psychogenic polydipsia
D. Cirrhosis
E. Congestive heart failure
117. A 63-year-old woman has Type II diabetes mellitus, which is well-controlled. Her physical examination is positive for peripheral neuropathy in the feet and nonproliferative retinopathy. A urinalysis is positive for proteinuria. Which of the following treatments is most likely to attenuate the course of renal disease?
(A) calcium channel blockers
(B) ACE inhibitors
(C) hepatic hydroxymethylglutaryl- coenzyme A (HMG-CoA) inhibitors
(D) dietary carbohydrate restriction
(E) weight reduction
118. A 56-year-old man is involved in a severe motor vehicle accident. He develops ARF after admission to hospital. One of the possibilities for his ARF is posttraumatic renal vein thrombosis. Which of the following findings is most likely to suggest renal vein thrombosis?
(A) white cell casts on urinalysis
(B) heme-granular casts
(C) heavy proteinuria
(D) urine supernatant pink and tests positive for heme
(E) specific gravity >1.020

119. A 69-year-old woman presents with left flank pain and hematuria. Physical examination suggests a left-sided abdominal mass. Computerized tomography (CT) scan of the abdomen reveals a 5-cm mass in the left kidney. Which of the following laboratory abnormalities might also be present? (See Fig.)
(A) polycythemia
(B) thrombocytopenia
(C) hypocalcemia
(D) leukocytosis
(E) high renin hypertension
120. A 60-year-old woman with heart failure and normal renal function is started on furosemide (Lasix) 80 mg/day. She notices a good diuretic response every time she takes the medication. A few weeks later, she is feeling unwell because of fatigue and muscle weakness, but her heart failure symptoms are better. Which of the following is the most likely explanation for her muscle weakness?
(A) hyponatremia
(B) hypernatremia
(D) hyperkalemia
(C) hypokalemia
(E) anemia
121. A 65-year-old diabetic man with a creatinine of 1.6 was started on an angiotensin- converting enzyme inhibitor for hypertension and presents to the emergency room with weakness. His other medications include atorvastatin for hypercholesterolemia, metoprolol and spironolactone for congestive heart failure, insulin for diabetes, and aspirin. Laboratory studies include K: 7.2 mEq/L Creatinine: 1.8 mg/dL Glucose: 250 mg/dL CK: 400 IU/L Which of the following is the most likely cause of hyperkalemia in this patient?
A. Worsening renal function
B. Uncontrolled diabetes
C. Statin-induced rhabdomyolysis
D. Drug-induced effect on the renin-angiotensin-aldosterone system
E. High-potassium diet
122. A 27-year-old alcoholic man presents with decreased appetite, mild generalized weakness, intermittent mild abdominal pain, perioral numbness, and some cramping of his hands and feet. His physical examination is initially normal. His laboratory returns with a sodium level of 140 mEq/L, potassium 4.0 mEq/L, calcium 6.9 mg/dL, albumin 3.5 g/dL, magnesium 0.7 mg/dL, and phosphorus 2.0 mg/dL. You go back to the patient and find that he has both a positive Trousseau and a positive Chvostek sign. Which of the following is the most likely cause of the hypocalcemia?
A. Poor dietary intake
B. Hypoalbuminemia
C. Pancreatitis
D. Decreased end-organ response to parathyroid hormone because of hypomagnesemia
E. Osteoporosis caused by hypogonadism
123. A 27-year-old woman presents to the emergency room with a panic attack. She appears healthy except for tachycardia and a respiratory rate of 30. Electrolytes include calcium 10.0 mg/dL, albumin 4.0 g/dL, phosphorus 0.8 mg/dL, and magnesium 1.5 mEq/L. Arterial blood gases include pH of 7.56, P CO2 21 mm Hg, and PO2 99 mm Hg. The most likely cause of the hypophosphatemia?
A. Hypomagnesemia
B. Hyperparathyroidism
C. Respiratory alkalosis with intracellular shift
D. Poor dietary intake
E. Vitamin D deficiency
124. A 60-year-old man is brought in by ambulance and is unable to speak. The EMS personnel tell you that a neighbor informed them he has had a stroke in the past. There are no family members present. His serum sodium is 118 mEq/L. Which of the following is the most helpful first step in the assessment of this patient’s hyponatremia?
A. Order a chest x-ray
B. Place a Foley catheter to measure 24-hour urine protein
C. Clinical assessment of extracellular fluid volume status
D. CT scan of head
E. Serum AVP (arginine vasopressin) level
125. A 39-year-old woman is admitted to the gynecology service for hysterectomy for symptomatic uterine fibroids. Postoperatively the patient develops an ileus accompanied by severe nausea and vomiting; ondansetron is piggybacked into an IV of D5 1❄2 normal saline running at 125 cc/h. On the second postoperative day the patient becomes drowsy and displays a few myoclonic jerks. Stat labs reveal Na 118, K 3.2, Cl 88 HCO3 22, BUN 3, and creatinine 0.9. Urine studies for Na and osmolality are sent to the lab. What is the most appropriate next step?
A. Change the IV fluid to 0.9% (normal) saline and restrict free-water intake to 600 cc/d.
B. Change the ondansetron to promethazine, change the IV fluid to lactated Ringer solution, and recheck the Na in 4 hours.
C. Start 3% (hypertonic) saline, make the patient NPO, and transfer to the ICU.
D. Change the IV fluid to normal saline and give furosemide 40 mg IV stat.
E. Make the patient NPO and send for stat CT scan of the head to look for cerebral edema.
126. You evaluate a 48-year-old man for chronic renal insufficiency. He has a history of hypertension, osteoarthritis, and gout. He currently has no complaints. His medical regimen includes lisinopril 40 mg daily, hydro-chlorothiazide 25 mg daily, allopurinol 300 mg daily, and acetaminophen for his joint pains. He does not smoke but drinks 8 oz of wine on a daily basis. Examination shows BP 146/86, pulse 76, a soft S4 gallop, and mild peripheral edema. There is no abdominal bruit. His UA reveals 1+ proteinuria and no cellular elements. Serum creatinine is 2.2 mg/dL and his estimated GFR from the MDRD formula is 42 mL/minute. What is the most important element is preventing progression of his renal disease?
A. Discontinuing all alcohol consumption
B. Discontinuing acetaminophen
C. Adding a calcium channel blocker to improve blood pressure control
D. Obtaining a CT renal arteriogram to exclude renal artery stenosis
E. Changing the lisinopril to losartan
127. A 45-year-old woman with cirrhosis secondary to autoimmune hepatitis is seeing her hepatologist for routine follow-up. She reports that she has been feeling relatively well lately, and complains only of mild fatigue. Her medical history is otherwise unremarkable. Her medications include lactulose, spironolactone, propranolol and furosemide. Her vital signs are stable and the remainder of her physical exam is consistent with compensated cirrhosis. Her laboratory values are given below: Sodium 132 mEq/L Potassium 4.1 mEq/L Chloride 100 mEq/L Bicarbonate 24 mEq/L Glucose 102 mg/dl Creatinine 0.9 mg/dl Calcium 7.4 mg/dl Total protein 6.1 g/dl Albumin 2.5 g/dl Total bilirubin 2.1 mg/dl AST 80 units/L ALT 102 units/L What is the most appropriate next step in the management of this patient's hypocalcemia?
A. Calcium gluconate infusion
B. Measurement of vitamin D levels
C. Replace furosemide with hydrochlorothiazide (HCTZ)
D. Initiate oral calcium and vitamin D replacement
E. No intervention is required
128. A 57-year-old male is hospitalized for hyponatremia. Physical examination reveals no signs of fluid overload. Serum analysis reveals a sodium concentration of 125mEq/1, glucose level of 12mg/dl, BUN of 8mg/dl, and creatinine of 0.7mg/dl. The urine osmolarity is 330mOsm/l and urine sodium concentration is 45mEq/1. After a 2L normal saline infusion, the serum sodium is 126mEq/1 and the urine sodium excretion is increased to 90 mEq/1. Which of the following is the most likely cause of this patient's hyponatremia?
A. Inappropriate ADH secretion
B. Psychogenic polydipsia
C. Surreptitious diuretic use
D. Advanced liver disease
E. Interstitial renal disease
129. A 69-year-old man is brought to the ER by his family for increasing confusion. At baseline the patient is interactive and pleasant, but he has become withdrawn and confused over the last several months. He has also complained of abdominal pain, nausea, vomiting and back pain over the same period of time. His medical history is significant for diabetes controlled with metformin and hypertension treated with hydrochlorothiazide. Exam reveals normal vital signs and a disheveled, confused man. His neurologic exam is otherwise normal. Examination of the heart and lungs is unremarkable and no neck masses or nodes are appreciated. Laboratory results are given below. Sodium 139 mEq/L Potassium 4.2 mEq/L Chloride 111 mEq/L Bicarbonate 26 mEq/L Creatinine 1.4 mg/dl Glucose 142 mgldl Calcium 12.8 mEq/L WBC 3,200/mm3 Hematocrit 32% Platelets 47,000/mm3 What is the most appropriate next step for this patient?
A Hemodialysis
B. 0.9% saline infusion
C. Pamidronate
D. Calcitonin
E. Furosemide
130. A 38-year-old woman presents to the emergency department and complains of persistent vomiting that has increased in severity over the last week. Her other complaints are muscular weakness, twitching and cramps. Her urine output has decreased over the last 20 hours. Her past medical history is significant for a previously diagnosed prepyloric peptic ulcer. Her pulse is 100/min, blood pressure is 100/60 mmHg, respirations are 12/min, and temperature is 37.2 C (99F). Physical examination reveals dry oral mucosa and decreased skin turgor. Abdominal examination reveals hypoactive bowel sounds and mild tenderness on palpation of the epigastrium. Nasogastric suction is started, and intravenous normal saline is given. Laboratory studies show: Serum sodium 135 mEq/L Serum potassium 2.8 mEq/L Chloride 81 mEq/L Bicarbonate 40 mEq/L Blood urea nitrogen (BUN) 42 mg/dl Serum creatinine 1.3 mg/dl Calcium 8.6 mg/dl Ionized calcium 0.7 mmoi/L (1.1-1.3 mmoi/L) Serum pH 7.54 Which of the listed agents should be added to the patient's current therapy?
A. Ammonium chloride
B. Potasium chloride
C. Calcium chloride
D. Furosemide
E. Sodium bicarbonate
131. A 43-year-old female with history of hepatitis C, alcohol use and cirrhosis is admitted to the hospital for severe vomiting for the last 2 days. Her temperature is 36.7C (98.2F), pulse is 90/min, respirations are 14/min and blood pressure is 100/70 mmHg supine. Her lungs are clear to auscultation. She has mild epigastric tenderness, but there is no abdominal distention. Extremities have no edema. Her laboratory profile shows: Blood PH 7.49 PaO2 100 mmHg PaCO2 41 mm Hg HCO3- 30 mEq/L Sodium 138 mEq/L Potassium 3.0 mEq/L Chloride 95 mEq/L Which of the following is the most appropriate treatment for the patient's alkalosis?
A. Intravenous ammonium chloride and potassium
B. Intravenous hydrochloric acid and potassium
C. Intravenous mannitol
D. Intravenous normal saline and potassium
E. Dialysis
132. A 27-year-old female is brought into the emergency room by the local paramedics. She was found unconscious at the scene of a house fire. On examination it does not appear that she has suffered any burns. Black soot is noted near her nares and mouth. Her respirations are slow but spontaneous. Her capillary refill time is 4 seconds. Supplemental oxygen by a non-rebreather mask is begun. Her arterial blood gas and preliminary laboratory values are shown below: Blood pH 7.22 PaO2 1 00 mmHg PaCO2 39 mmHg HC03- 11 mEq/L WBC count 9,000/cmm Hb 14 mg/dl Na+ 138 mEq/L K+ 4 mEq/1 CI- 98 mEq/L Troponin 0.4ng/ml Which of the following is the most likely primary cause of the patient's acid-base disturbance?
A. Increased metabolic rate
B. Decreased oxygen delivery to tissue
C. Reduced oxygen utilization by tissues
D. Impaired excretion of lactic acid
E. Increased gut absorption
133. A 32-year-old female is brought to the emergency department with complaints of weakness, tingling and numbness of her extremities. She is not on any medication. Her pulse is 90/min, respirations are 14 /min and blood pressure is 110/70 mm Hg. The physical examination is unremarkable. Her laboratory profile is shown below: Blood pH 7.56 HCO3- 37 mEq/L Urine Na+ 16 mEq/L Urine K+ 20 mEq/L Urine Cl- 7 mEq/L Serum sodium 135 mEq/L Serum potassium 2.9 mEq/L Serum chloride 92 mEq/L Blood urea nitrogen 22 mg/dl Serum creatinine 0.9 mg/dl Which of the following is the most likely cause of this patient's condition?
A. Surreptitious vomiting
B. Persistent diarrhea
C. Bartter's syndrome
D. Type I renal tubular acidosis
E. Hyperventilation syndrome.
134. A 60-year-old male who emigrated from Russia comes to you with complaints of dizziness, fatigue and weight loss. A review of systems reveals that the patient experiences daily fevers and cough. He does not use tobacco, alcohol or drugs. He does not take any medication. His blood pressure is 108/64 mmHg while standing. His respiratory rate is 14/min and is unlabored. Laboratory studies reveal the following: Chemistry panel: Serum sodium 130 mEq/L Serum potassium 5.9 mEq/L Chloride 102 mEq/L Serum creatinine 0.8 mg/dL Blood glucose 58 mg/dL Complete blood count: Hemoglobin 10.0g/L Platelets 430,000/mm3 Leukocyte count 4,500/mm3 NeutrophiIs 46% Lymphocytes 45% Eosinophils 9% Chest x-ray shows a right upper lobe cavity. Which of the following acid-base disturbances is expected in this patient?
A. Elevated anion gap metabolic acidosis
B. Normal anion gap metabolic acidosis
C. Metabolic alkalosis
D. Respiratory acidosis
E. Respiratory alkalosis
135. A 55-year-old homeless man presents to the emergency room complaining of muscle cramps and perioral numbing. The patient looks malnourished. He says that he consumed a lot of alcohol recently. His past medical history is significant for chronic and recurrent abdominal pain for which he was advised to quit drinking alcohol. His temperature is 36.7 C (98 F), blood pressure is 110/65 mmHg, pulse is 80/min, and respirations are 18/min. The laboratory values are: Hemoglobin 7.2 g/dl MCV 105 fl Leukocyte count 9,000/cmm Platelets 200,000/cmm ESR 20 mm/hr Serum sodium 145 mEq/L Serum potassium 4.0 mEq/L Serum calcium 6.8 mg/dl Serum phosphorus 2.5 mg/dl What is the most probable cause of hypocalcemia observed in this patient?
A. Renal failure
B. Primary hypoparathyroidism
C. Pseudohypoparathyroidism
D. Hypoalbuminemia
E. Malabsorption
136. A 20-year-old white male is found to have an elevated calcium level on routine pre-employment screening blood tests. He denies any polyuria, polydipsia or constipation. He has no significant past medical history and does not take any medication. He does not use tobacco, alcohol or drugs. His pulse rate is 82/min, blood pressure is 110/70 mmHg, temperature is 37.0C (99F) and respirations are 14/min. Complete physical examination is unremarkable. Laboratory studies show the following: Serum sodium 140 mEq/L Serum potassium 4.0 mEq/L Chloride 103 mEq/L Bicarbonate 24 mEq/L Blood urea nitrogen (BUN) 18 mg/dl Serum creatinine 0.8 mg/dl Calcium 11.2 mg/dl Blood glucose 98 mg/dl Serum PTH level 55 pg/ml (normal 10-65 pg/ml) Urine calcium/creatinine clearance ratio < 0.01 Which of the following conditions is most consistent with this patient's findings?
A. Primary hyperparathyroidism
B. Vitamin D overproduction
C. Multiple myeloma
D. Sarcoidosis
E. Familial hypocalciuric hypercalcemia
137. A four-week-old male infant is brought to the emergency department because of persistent vomiting immediately after feeding for the past several days. Examination shows an emaciated infant with dry mucus membranes. An olive-shaped mass is palpated in the right upper quadrant of the abdomen. Which of the following acid-base abnormalities is most likely in this patient? pH, PaCO2 (mm Hg), HCO3- (mEq/L)
A.7.10, 80, 24
B. 740, 40, 24
C. 7.55, 46, 42
D. 7.62, 21, 21
E. 7.62, 30, 30
138. A 21-year-old woman complains of progressive weakness and loss of energy. She nearly collapsed yesterday while performing one of her routine 3 hour workouts. Additionally, she has been performing badly in college despite persistent attempts to improve her grades. Physical exam reveals a blood pressure of 102/58 mmHg, heart rate of 113/min, fine hair covering her face, and normal heart and lungs. Laboratory studies show the following findings: Sodium 140 mEq/L Potassium 24 mEq/L Calcium 10.1 mg/dL Chloride 90 mEq/L Bicarbonate 40 mEq/L Urine chloride 14 mEq/L Which of the following is most likely to correct the laboratory abnormalities in this patient?
A. Calcium gluconate infusion
B. Normal saline infusion
C. Sodium bicarbonate solution infusion
D. Loop diuretics
E. Hyperventilation
139. A 24-year-old female is brought to the emergency room because of dizziness and near syncope. She says that every time she stands up, she feels lightheaded. She has no significant past medical problems. She does note having broken up with her boyfriend three months ago, which has caused her to have decreased appetite and an associated ten-pound weight loss. She has also missed her last two menstrual periods. She denies using tobacco, alcohol or drugs. On physical examination, her temperature is 36.7C (98.F). When lying supine, her blood pressure is 100/70 mm Hg and her pulse is 88/min. When she stands up, her blood pressure is 80/50 mm Hg and her pulse is 120/min. Other than dry skin and mucous membranes, her physical examination is unremarkable. Initial laboratory studies reveal: Serum sodium low Serum potassium low Urine sodium increased Urine potassium increased This patient's dizziness is most likely due to which of the following?
A. Low caloric intake
B. Self-induced vomiting
C. Laxative abuse
D. Diuretic abuse
E. Mineralocorticoid deficiency
140. A 52-year-old alcoholic man presents to the emergency department because of anxiety and tremors. His last drink of alcohol was 2 days ago. His initial electrolyte panel is: Sodium 132 mEq/L Potassium 2.9 mEq/L Chloride 100 mEq/L Bicarbonate 25 mEq/L He is treated for alcohol withdrawal, and given aggressive intravenous and oral potassium supplementation. Three days later, his electrolyte panel is: Sodium 135 mEq/L Potassium 3.1 mEq/L Chloride 102 mEq/L Bicarbonate 28 mEq/L Which of the following explains why this patient's potassium level is so difficult to correct?
A. Poor oral absorption
B. Hypophosphatemia
C. Alcohol withdrawal
D. Hypomagnesemia
E. Thiamine deficiency
141. A 52-year-old man with Burkitt lymphoma is admitted to the hospital for chemotherapy. He is started on chemotherapy without incident. Two days into his hospitalization, he develops new peaked T-waves on his ECG. Laboratory analysis reveals a serum potassium concentration of 6.2 mEq/L, and the patient is given one ampule of calcium gluconate emergently. His renal function is within normal limits. Which of the following additional interventions will most rapidly correct his hyperkalemia?
A Hemodialysis
B. Sodium polystyrene sulfonate
C. Furosemide
D. Insulin and glucose
E. High-dose inhaled β2 agonist
142. A 65-year-old chronic smoker presents to the hospital with increasing shortness of breath for the past few hours. He has been using albuterol occasionally, but it has not been helping him. He has been non-adherent to doctor's appointments and continues to smoke. He is afebrile. His oxygen saturation on room air is 86%. Examination shows elevated jugular venous pressure and lung auscultation reveals diffuse wheezing with no crackles. His heart sounds are muffled. Mild hepatomegaly and bilateral pitting pedal edema is present. Chest x-ray reveals hyperinflated lungs and a flattened diaphragm with no infiltrates. He is started on systemic steroids, bronchodilator nebulization and furosemide. His laboratory studies are shown below at the time of admission and five days later.Which of the following best explains the acid-base status change in this patient?
A. Acute renal failure
B. Development of ketoacidosis
C. Glucocorticoid treatment
D. Obstructive sleep apnea
E. Worsening respiratory failure
143. A 65-year-old white female comes to the ER because of persistent vomiting and epigastric pain. She has been suffering from left knee osteoarthritis for the past 6 years, and has been taking ibuprofen for the past year. She also has a history of chronic obstructive pulmonary disease but is well controlled on her current medications. She quit smoking a few years ago. Her laboratory results are given below. ABG: pH 7.55 PCO2 46 mm Hg Chemistry panel: Serum sodium 132 mEq/L Serum potassium 3.0 mEq/L Chloride 88 mEq/L Bicarbonate 38 mEq/L Serum creatinine 0.8 mg/dl Which of the following would describe her primary acid-base status?
A. Normal profile
B. Metabolic acidosis
C. Metabolic alkalosis
D. Respiratory acidosis
E. Respiratory alkalosis
144. A 35-year-old male with severe persistent bronchial asthma requiring multiple medications presents complaining of weight gain over the past several months despite no changes in appetite, diet, or activity level. He denies alcohol, tobacco, and drug use and has no other significant past medical history. On physical examination, he has a blood pressure of 143/92 mm Hg, a heart rate of 65/min, a temperature of 98.7°F, and a respiratory rate of 16/min. There is moderate supraclavicular fullness, and his skin is thin with areas of bruising and acne. Neurologic exam reveals decreased proximal muscle strength. Which of the following findings is most likely to also be present in this patient?
A Hyperkalemia
B. Hypokalemia
C. Hypercalcemia
D. Hyponatremia
E. Hypomagnesemia
145. A 36-year-old male is brought to the emergency department due to confusion, nausea and decreased arousal. He is unable to answer questions and no other history is available. His temperature is 36.7C (98.2 F), respirations are 22/min and pulse is 86/min. His ABG and serum electrolyte levels are shown below: pH 7.21 PaO2 96 mmHg PaCO2 28 mmHg Serum sodium 140 mEq/L Serum potassium 3.6 mEq/L Chloride 90 mEq/L Bicarbonate 12 mEq/L Blood urea nitrogen (BUN) 30 mg/dl Serum creatinine 1.2 mg/dl What is the most likely primary acid-base disorder in this patient?
A. Non-anion gap metabolic acidosis
B. Anion gap metabolic acidosis
C. Metabolic alkalosis
D. Respiratory alkalosis
E. Respiratory acidosis
146. A 58-year-old alcoholic is admitted with diagnosis of decompensated liver cirrhosis. The lab panel is shown below on the day of admission and 3 days later.Which of the following best explains the acid-base status change in this patient?
A. Acute renal failure
B. Bowel ischemia
C. Loop diuretic therapy
D. Opioid medication use
E. Right lower lobe atelectasis
147. A 32-year-old pregnant female is being evaluated at her 32nd week of gestation. Her lab profile shows the following: Blood pH 7.44  PaO2 100 mmHg PaCO2 30 mmHg HCO3- 20 mEq/L WBC count 9,000/cmm Hb 11 mg/dl Na+ 134 mEq/L K+ 3.6 mEq/1 Cl- 98 mEq/L BUN 5 mg/dl Creatinine 0.6 mg/dl Which of the following can best explain her acid-base status?
A. Anemia
B. Pulmonary embolism
C. Obesity
D. Normal phenomenon of pregnancy
E. Hyperemesis gravidarum
148. A 59-year-old female is hospitalized due to lower gastrointestinal bleeding. Her past medical history includes diabetes mellitus, hypertension, chronic obstructive pulmonary disease, cor pulmonale and recurrent urinary tract infections. Her condition initially stabilized with fluid resuscitation and blood transfusions, but she subsequently developed an acute renal failure. Her urine output has been between 300 and 400 ml per day for the last couple of days. On the 1Oth day of her hospitalization she is lethargic. Serum analysis reveals: Hemoglobin 10.2 g/dl Hematocrit 30% WBC 14,300/mm3 Blood glucose 93 mg/dl BUN 141 mg/dl Creatinine 4.1 mg/dl Sodium 133 mEq/L Potassium 5.0 mEq/L pH 7.15 pO2 90 mmHg pCO2 60 mmHg HCO3 18 mEq/L Which of the following is the most likely cause of her lethargy?
A. Poor tubular bicarbonate reabsorption
B. Low tubular ammonium production
D. Decreased anion gap
C. Renal tubular chloride loss
E. Hypoventilation
149. A 42-year-old woman presents to the emergency department with multiple complaints. She reports that she had been feeling well until approximately one month ago, when she began to feel increasingly fatigued and weak. For the past two weeks, she has had anorexia, nausea, and abdominal pain. In the past three days, she has had two syncopal episodes. Her medical history is unremarkable and she takes no medications. She denies tobacco and drug use and drinks wine only occasionally. Physical exam reveals a temperature of 36.7C (98F), blood pressure of 86/52 mmHg, heart rate of 90/min, and respiratory rate of 18/min. Her cardiac exam is normal and her lungs are clear to auscultation bilaterally. You note hyperpigmentation of the skin in the palmar creases. Which of the following additional findings is most likely to be present in this patient?
A Hyperkalemia
B. Hypokalemia
C. Hypernatremia
D. Hypochloremia
E. Hypomagnesemia
150. A 58-year-old man is admitted to the intensive care unit with an exacerbation of his chronic obstructive pulmonary disease (COPD) and respiratory failure. After several hours on noninvasive ventilation the patient develops worsening respiratory distress and requires endotracheal intubation. Which of the following is a contraindication to the use of succinylcholine for rapid-sequence intubation?
A Hyperkalemia
B. COPD exacerbation
D. Hypokalemia
C. Hepatic failure
E. Hypercalcemia
151. A 42-year-old male is found unconscious in a subway station. He is brought to the emergency department where cardio-pulmonary resuscitation (CPR) is done and IV glucose and thiamine are given. His lab profile shows: Blood pH 7.20 PaO2 90mmHg PaCO2 30mmHg HCO3· 12 mEq/L Which of the following is the best next step in the diagnosis of this patient's acid-base status?
A. Calculate the plasma anion gap
B. Calculate the plasma osmolar gap
C. Calculate the urine anion gap
D. Calculate the urine osmolar gap
E. Obtain venous blood gas
152. A 56-year-old male comes to the emergency room because of a 2-day history of fever, chills, shortness of breath and productive cough. He also threw up once in the emergency room. He has been smoking for several years and occasionally drinks alcohol. On admission, his BP was 90/60, but with one liter of normal saline it improved to 120/80 mm Hg. His temperature is 38.8C (102F). His arterial blood gas (ABG) analysis is as follows: Blood pH 7.53 PaO2 70 mmHg PaCO2 30 mmHg HCO3- 22 mEq/L Which of the following best describes his primary acid-base status?
A. Respiratory acidosis
B. Respiratory alkalosis
C. Metabolic acidosis
D. Metabolic alkalosis
E. Normal acid base status
153. A 22-year-old man presents to the emergency department complaining of fever, nausea, vomiting, and right lower quadrant pain. He has no significant medical history and does not take any medications. He is a senior in college and denies cigarette smoking or drug use. He drinks alcohol occasionally. Physical examination reveals a temperature of 38.6°C, with all other vital signs within normal limits. ACT scan of his abdomen confirms acute appendicitis. Laboratory analyses reveal a leukocytosis but no electrolyte abnormalities. He is taken to the operating room and undergoes a successfullaparoscopic appendectomy. Following the procedure, he is given intravenous fluids containing 5% dextrose in a 0.45% (1❄2normal) saline solution at a rate of 150 ml/hr. The next morning the patient feels well but he then becomes progressively confused throughout the afternoon. You are called to his bedside after he has two grand mal seizures lasting 30 seconds apiece. Serum chemistries drawn at that time reveal a sodium concentration of 115mEq/L. What is the most appropriate therapy for this patient?
A. Fosphenytoin
B. 3% saline
C. Normal saline
D. Phenobarbital
E. Lorazepam
154. A 71-year-old man with inclusion body myositis is brought to the emergency department from his nursing home after becoming less interactive. His temperature is 37.1°C, blood pressure is 90/60 mmHg, heart rate is 98/min, and respiratory rate is 16/min. He has orthostatic vital signs. Physical examination reveals a frail man with dry oral mucosa and decreased axillary perspiration. Laboratory studies reveal the following: Sodium 164 mEq/L Potassium 4.9 mEq/L Bicarbonate 29 mEq/L Chloride 122 mEq/L What is the most appropriate next step in the management of this patient?
A. Oral free water
B. IV 0.9% saline
C. IV 5% dextrose in water
D.IV 5% dextrose in 04 5% saline
E. IV free water
155. A 32-year-old Caucasian male presents to the ER with a 12-hour history of anorexia and vomiting. He says that he feels “a little dizzy”. He denies abdominal pain or diarrhea. His past medical history is insignificant His blood pressure is 110/70 mmHg while supine and 100/60 mmHg while sitting. His heart rate is 90/min. His laboratory values are: Serum sodium 139 mEq/L Serum potassium 3.1 mEq/L Serum calcium 8.9 mEq/L Serum chloride 88 mEq/L Serum bicarbonate 33 mEq/L Blood glucose 95 mg/dl BUN 20 mg/dl Serum creatinine 1.1 mg/dl Which of the following is the most likely cause of the decreased chloride level in this patient?
A. Gastrointestinal loss
B. Bicarbonate reabsorption in the kidney
C. Metabolic alkalosis
D. Intracellular shift
E. Volume depletion
156. A 66-year-old white male comes to the physician's office for the first time because of generalized muscle weakness. His review of systems is otherwise negative. He has a past medical history of hypertension, type-2 diabetes, hyperlipidemia, chronic renal insufficiency and ischemic cardiomyopathy. Neurological examination shows mild weakness of the lower limbs, depressed reflexes and normal sensation. Laboratory studies show: Serum sodium 134 mEq/L Serum potassium 6.0 mEq/L Bicarbonate 24 mEq/L Blood urea nitrogen (BUN) 38 mg/dl Serum creatinine 2.8 mg/dl Calcium 8.2 mg/dl Blood glucose 298 mg/dl A dose of sodium polystyrene sulfonate is given. Which of the following additional interventions is most important in this patient's management?
A. Review all his current medications
B. Measure serum renin and aldosterone levels
C. Obtain electromyography
D. Obtain acetylcholine receptor antibodies
E. Start oral prednisone therapy
157. A 43-year-old woman presents to the emergency department complaining of confusion. Her other complaints include increased thirst and "using the bathroom more frequently." She denies any fever, chills, headache, chest pain, shortness of breath, or cough. Her past medical history is significant for bipolar disorder that is well-controlled by medication. She does not drink alcohol, smoke cigarettes, or use illicit drugs. Her vital signs are stable, and physical exam is unremarkable. Laboratory studies reveal the following: Sodium 154 mEq/L Potassium 4.1 mEq/L Chloride 116 mEq/L Bicarbonate 28 mEq/L Glucose 95 mg/dl Urine osmolality 250 mOsm/L Plasma osmolality 326 mOsm/L What is the most likely cause of this patient's symptoms and laboratory findings?
A. Dehydration
B. Lithium
C. Divalproic acid
D. Craniopharyngioma
E. Head trauma
158. A 22-year-old female is hospitalized after a car accident. She sustained a hip fracture, fractures of several ribs and a blunt abdominal injury that required a laparotomy. The laparotomy revealed a liver laceration and extensive hemoperitoneum. In the early postoperative period, the patient is noted to have hyperactive deep tendon reflexes. Which of the following electrolyte abnormalities may be responsible for this condition?
A Hypokalemia
B. Hyperkalemia
D. Hypocalcemia
E. Hypermagnesemia
C. Hyponatremia
159. A 67 -year-old male is brought to the ER because of increasing abdominal pain and nausea for the past few hours. He has multiple medical problems including type-2 diabetes, hypertension, hyperlipidemia, coronary artery disease, cerebrovascular accident, peripheral vascular disease, ischemic cardiomyopathy and atrial fibrillation. He has not been on anticoagulation because of recurrent bleeding peptic ulcer disease. He has had a cholecystectomy. He takes multiple medications at prescribed doses and lives at home with his family. He quit smoking 10 years ago and does not use alcohol or drugs. His temperature is 37.8C (100.0F), blood pressure is 150/90 mm Hg, pulse is 110/min and respirations are 22/min. Physical examination shows an elderly male in acute distress. Lungs have few crackles at the bases. Heart rate is irregular. Bowel sounds are decreased and diffuse tenderness is present. There is no peripheral edema. Initial laboratory studies show the following: Serum sodium 140 mEq/L Chloride 103 mEq/L Bicarbonate 14 mEq/L Blood urea nitrogen (BUN) 20 mg/dl Serum creatinine 0.8 mg/dl Blood glucose 198 mg/dl Amylase 255 U/L Which of the following is the most likely diagnosis in this patient?
A. Diabetic ketoacidosis
B. Bowel ischemia
C. Acute pancreatitis
D. Acute appendicitis
E. Peptic ulcer perforation
160. A 79-year-old female presents to your office with a three-day history of nausea, diarrhea, poor oral intake and weakness. Her past medical history is significant for hypertension treated with enalapril and diltiazem. Her serum chemistry shows the following: Sodium 139 mEq/L Potassium 7.8 mEq/L Bicarbonate 14 mEq/L Chloride 95 mEq/L Glucose 155 mg/dl BUN 80 mg/dl Creatinine 3.1 mg/dl EKG reveals QRS prolongation and prominent T wave peaking in precordial leads. Which of the following pharmacologic therapies plays a role in treating this patient's electrolyte condition?
A. Stimulating alpha 1-adrenoreceptors
B. Stimulating beta 1-adrenoreceptors
C. Stimulating beta2-adrenoreceptors
D. Blocking alpha 1-adrenoreceptors
E. Blocking beta 1-adrenoreceptors
161. A 56-year-old male with a history of type-2 diabetes presents for a routine office visit. His blood work from two months ago showed hyperkalemia, and at that time his physician discontinued lisinopril. His repeat blood work done today is shown below: Chemistry panel: Serum sodium 136 mEq/L Serum potassium 5.6 mEq/L Chloride 110 mEq/L Bicarbonate 18 mEq/L Blood urea nitrogen (BUN) 26 mg/dl Serum creatinine 1.9 mg/dl He currently takes glipizide, furosemide, nifedipine and aspirin. His blood pressure is 150/90 mmHg. Examination is unremarkable. Which of the following is the most likely cause of his low bicarbonate and elevated potassium?
A Chronic renal failure
B. Renal tubular acidosis
C. Furosemide
D. Glipizide
E. Nifedipine
162. A 44-year-old obese female undergoes an open cholecystectomy for a complicated acute cholecystitis. On her third post-operative day, her temperature is 36.7C (98.2F), blood pressure is 110/80 mm Hg and pulse is 92/min. Her arterial blood gas shows the following: Blood pH 7.28 PaO2 62 mmHg PaCO2 54 mmHg HCO3- 30 mEq/L What is the most likely cause of acidosis in this patient?
A. Alveolar hypoventilation
B. Acute pulmonary embolism
C. Atelectasis
D. Pulmonary edema
E. Pleural effusion
163. A 33-year-old woman is brought to the emergency room because of altered mental status. En route to the ER, she suffers a generalized tonic clonic seizure, and once at the hospital she is confused and no further history can be obtained. You know only that she has a history of schizophrenia. On physical examination, her temperature is 36.7°C (98°F), blood pressure is 130/76 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows normal pupils. Her chest is clear to auscultation and her heart sounds are normal. Her abdomen is soft and nontender. Extremities have no edema. Laboratory studies show: Serum sodium 118 mEq/L Serum creatinine 0.8 mg/dL Serum calcium 8.4 mg/dL Serum glucose 98 mg/dL Urine osmolality 100 mosm/kg Urine specific gravity 1.002 Which of the following is the most likely cause of her symptoms?
A Primary polydipsia
B. Drug-induced ADH resistance
C. Increased ADH production
D. Drug-induced water retention
E. Deficient ADH secretion
164. A 56-year-old male comes to the emergency room because of increasing shortness of breath for the last 3 days. He had a cold recently, and since then his symptoms have been worse. He has a mild productive cough but denies fever or chills. He has a several year history of smoking and has been diagnosed with emphysema. He also has a history of diabetes, hypertension, hyperlipidemia, and hypothyroidism. He takes glipizide, metformin, lisinopril, furosemide, aspirin, atorvastatin and levothyroxine. Physical examination shows trace bilateral lower extremity edema and a diffuse decrease in breath sounds along with wheezing. Heart sounds are distant. His arterial blood gas shows the following: Blood pH 7.23 PaO2 88mm Hg PaCO2 40 mm Hg HCO3- 16mEq/L Which of the following best describes the acid-base status of this patient?
A. Metabolic acidosis
B. Respiratory acidosis
C. Mixed metabolic and respiratory acidosis
D. Mixed metabolic acidosis and respiratory alkalosis
E. Normal acid-base balance
165. A 55-year-old male is brought to the emergency department with a gunshot wound to his abdomen. He went to the operating room for repair of his injuries. On postoperative day 4, he develops a waxing and waning fever, tachypnea and shortness of breath. His temperature is 40C (104F), blood pressure is 90/60 mm Hg, pulse is 110/min and respirations are 22/min. Physical examination reveals an altered sensorium, crackles at the right lung base and a well healing abdominal wound. His urine output over the last 12 hours is 100ml. His laboratory profile shows: Blood pH 7.23 PaO2 60 mm Hg PaCO2 32 mmHg HCO3- 16 mEq/L Broad-spectrum antibiotics are started. Which of the following additional treatments is most appropriate in this patient?
A. Intravenous sodium bicarbonate
B. Intravenous Dextrose in water (0 5W)
C. Intravenous 3% saline
D. Intravenous 0.9% saline
E. Intravenous dopamine
166. A 32-year-old male with type 1 diabetes and severe depression is brought to the emergency department because of a 2-day history of nausea and abdominal pain. His temperature is 37.6C (99.7F), blood pressure is 122/86 mmHg, respirations are 25/min and pulse is 88/min. His lab values are as follows: Blood pH 7.31 Pa02 90mm Hg PaC02 29 mmHg HCO3- 14 mEq/L Blood glucose 450 mg/dl Serum sodium 132 mEq/L Serum potassium 5.0 mEq/L Serum chloride 85mEq/L Blood urea nitrogen 19 mg/dl Serum creatinine 1.1 mg/dl Which of the following best describes this patient's acid-base status?
A. Primary metabolic acidosis with respiratory compensation
B. Primary metabolic acidosis without compensation
C. Respiratory acidosis with compensation
D. Primary metabolic alkalosis with renal compensation
E. Normal acid base status
167. A 28-year-old primigravida is admitted to the hospital at 10weeks gestation. Her right leg is swollen. Her BMI is 30 Kg/m2. Her temperature is 36.7C (98.2F), respirations are 12/min and pulse is 96/min. Her ABG shows the following: pH 7.49 PaCO2 50 mm Hg HCO3- 44 mEq/L Which of the following is the most likely cause of her abnormal arterial blood gas?
A. Normal phenomenon of pregnancy
B. Pulmonary embolism
C. Obesity
D. Aspiration pneumonitis
E. Hyperemesis gravidarum
168. An 87-year-old female is brought to the emergency department for evaluation of altered mental status. Her medical history is significant for multi-infarct dementia, hypertension, stroke, coronary artery disease, severe degenerative joint disease, chronic atrial fibrillation, constipation and urinary incontinence. Her medications include aspirin, acetaminophen, atenolol, nitroglycerin, multivitamins, pravastatin, docusate, senna, digoxin and glucosamine. She lives in a local nursing home, and the people who brought her to the ED deny any history of new symptoms. Her blood pressure is 110/70 mmHg, pulse is 98/min, respirations are 16/min and temperature is 36.1 C (97F). Physical examination reveals dry mucus membranes and decreased skin turgor. There are no new focal neurologic deficits. Which of the following is most likely to be present in this patient?
A. Hyponatremia
B. Hypokalemia
D. Hyperkalemia
C. Hypernatremia
E. Hypocalcemia
169. A 45-year-old male is brought to the emergency department in a stuporous state. He appears agitated and disoriented. His temperature is 37.2C (99F), respirations are 22/min, pulse is 90/min and blood pressure is 110/70 mm of Hg. His lab findings are as follows Blood pH 7.21 PaO2 100 mmHg PaCO2 30 mmHg HCO3- 13 mEq/L Serum osmolarity 350 mOsm/L Blood glucose 90 mg/dl Na+ 141 mEq/L K+ 4.6 mEq/L CI- 100 mEq/L BUN 28mg/dl Creatinine 2.5 mg/dl His urine shows the presence of rectangular, envelope-shaped crystals. His creatinine three months ago was 1.2 mg/dl. What is the most likely cause of this lab abnormality in this patient?
A. Aspirin ingestion
B. Ethylene glycol poisoning
C. Methyl alcohol poisoning
D. Uremic acidosis
E. Lactic acidosis
170. A 56-year-old diabetic male is brought to the emergency department due to nausea and vomiting. While you are examining the patient, a nurse asks if determination of the patient's acid-base status will help ascertain the etiology and subsequent management of the patient's primary problem. Which of the following pairs of laboratory values will help get the best picture of the patient's acid-base status?
A pH and PaCO2
B. pH and PaO2
C. PaO2 and PaCO2
D. Urinary pH and PaCO2
E. Urinary pH and HCO3-
171. A 45-year-old female with severe depression, migraine and rheumatoid arthritis is brought in after she was found to have nausea, fever and upper abdominal discomfort. The patient describes severe tinnitus and vertigo. She admits that she overdosed on one of her medications. Her temperature is 38.5C (101.3F), blood pressure is 120/76 mm Hg, pulse is 90/min and respirations are 24/min. Physical examination is unremarkable. Which of the following acid-base statuses is most likely in this patient? pH, PaCO2 (mm Hg), HCO3- (mEq/L)
A 7.36, 22, 12
B. 7.29, 50, 23
C. 7.22, 35, 14
D. 7.40, 40, 24
E. 7.45, 30, 20
172. As you are walking across the hospital lobby, you stumble upon the arterial blood gas (ABG) results of a patient. The ABG (on room air) results are shown below: Blood pH 7.43 PaO2 100 mm Hg PaCO2 25 mm Hg HCO3- 16 mEq/L Which of the following patients is most likely to have these laboratory values?
A 42-year-old female with aspirin toxicity
B. 52-year-old female with persistent vomiting
C. 42-year-old patient with severe asthma exacerbation
D. 36-year-old patient with pulmonary embolism
E. 64-year-old male with excessive diuresis
173. A 42-year-old male is brought to the emergency department immediately after having a prolonged seizure episode. His family describes a past medical history of grand mal seizures. He has been on phenytoin for the past 10 years, but stopped taking the drug six months ago because he had not had any seizures in the last nine years. He is otherwise healthy and had been doing well until this seizure episode. He does not use tobacco, alcohol or drugs. He is afebrile. His blood pressure is 136/88 mm Hg, respirations are 18/min and pulse is 96/min. He appears confused and lethargic. Chest auscultation is unremarkable, and his abdomen is soft and nontender. A limited neurologic examination is non-focal. His laboratory report shows: Serum sodium 140 mEq/L Serum potassium 4.0 mEq/L Chloride 103 mEq/L Bicarbonate 17 mEq/L Blood urea nitrogen (BUN) 20 mg/dl Serum creatinine 0.8 mg/dl Blood glucose 98 mg/dl Chest x-ray and urinalysis are within normal limits, and a CT scan of the head is unremarkable. Which of the following is the most appropriate next step in the management of this patient's metabolic acidosis?
A. Give intravenous bicarbonate
B. Check serum ketones
D. Observe and repeat the labs after 2 hours
C. Check serum lipase
E. Start dopamine
{"name":"QCU\/DES\/USMLE\/NEPHROLOGY&ELECTROLYTE", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"Test your knowledge in nephrology and electrolyte management with this comprehensive quiz. Designed for medical professionals, students, and those interested in enhancing their understanding of renal disorders, this quiz presents a series of clinically relevant questions.Whether you're preparing for the USMLE, studying for a nephrology course, or simply looking to challenge yourself, this quiz covers:Clinical presentationsDiagnostic approachesTreatment modalitiesRenal physiology","img":"https:/images/course6.png"}