
Med emergency 2 Q1 to Q 80
1) An 81-year-old diabetic woman with a history of atrial fibrillation is transferred to your emergency department (ED) from the local nursing home. The note from the facility states that the patient is complaining of abdominal pain, having already vomited once. Her vital signs in the ED are temperature 100.1°F, blood pressure (BP) 105/75 mmHg, heart rate (HR) 95 beats per minute, and respiratory rate (RR) 18 breaths per minute. You examine the patient and focus on her abdomen. Considering that the patient has not stopped moaning in pain since arriving to the ED, you are surprised to find that her abdomen is soft on palpation. You decide to order an abdominal radiographic series. Which of the findings on plain abdominal film is strongly suggestive of mesenteric infarction?
. Sentinel loop of bowel
. No gas in the rectum
. Presence of an ileus
. Pneumatosis intestinalis
. Air fluid levels
2) A husband and wife present to the ED with 1 day of subjective fever, vomiting, watery diarrhea, and abdominal cramps. They were at a restaurant a day before for dinner and both ate the seafood special, which consisted of raw shellfish. In the ED, they are both tachycardic with temperatures of 99.8°F and 99.6°F for him and her, respectively. Which of the following is responsible for the majority of acute episodes of diarrhea?
. Parasites
. Viruses
. Enterotoxin-producing bacteria
. Anaerobic bacteria
. Invasive bacteria
. Parasites . Viruses . Enterotoxin-producing bacteria . Anaerobic bacteria . Invasive bacteria
. Normal saline (NS) solution
. Half normal saline (1/2 NS)
. Glucose solution (D5W)
. Solution containing both saline and glucose (D5/NS or D5 1/2 NS)
. The type of solution is irrelevant
4) As you palpate the right upper quadrant (RUQ) of a 38-year-old woman’s abdomen, you notice that she stops her inspiration for a brief moment. During the history, the patient states that over the last 2 days she gets pain in her RUQ that radiates to her back shortly after eating. Her vitals include a temperature of 100.4°F, HR of 95 beats per minute, BP of 130/75 mmHg, and RR of 16 breaths per minute. What is the initial diagnostic modality of choice for this disorder?
. Plain film radiograph
. Computed tomography (CT) scan
. Magnetic resonance imaging (MRI)
. Radioisotope cholescintigraphy (HIDA scan)
. Ultrasonography
5) A 31-year-old man from Florida presents to the ED complaining of severe pain that starts in his left flank and radiates to his testicle. The pain lasts for about 1 hour and then improves. He had similar pain last week that resolved spontaneously. He noted some blood in his urine this morning. His BP is 145/75 mmHg, HR is 90 beats per minute, temperature is 98.9°F, and his RR is 24 breaths per minute. His abdomen is soft and nontender. As you examine the patient, he vomits and has trouble lying still in his stretcher. Which of the following is the most appropriate next step in management?
. Call surgery consult to evaluate the patient for appendicitis
. Order an abdominal CT
. Start intravenous (IV) fluids and administer an IV nonsteroidal anti-inflammatory drug (NSAID) and antiemetic
. Perform an ultrasound to evaluate for an abdominal aortic aneurysm (AAA)
. Perform an ultrasound to evaluate for testicular torsion
6) A 48-year-old man with a past medical history of hepatitis C and cirrhosis presents to the ED complaining of acute-onset abdominal pain and chills. His BP is 118/75 mmHg, HR is 105 beats per minute, RR is 16 breaths per minute, temperature is 101.2°F rectally, and oxygen saturation is 97% on room air. His abdomen is distended, and diffusely tender. You decide to perform a paracentesis and retrieve 1 L of cloudy fluid. Laboratory analysis of the fluid shows a neutrophil count of 550 cells/mm 3. Which of the following is the most appropriate choice of treatment?
. Metronidazole
. Vancomycin
. Sulfamethoxazole/trimethoprim (SMX/TMP)
. Neomycin and lactulose
. Cefotaxime
7) A 24-year-old man woke up from sleep 1 hour ago with severe pain in his right testicle. He states that he is sexually active with multiple partners. On examination, the right scrotum is swollen, tender, and firm. You cannot elicit a cremasteric reflex. His BP is 145/75 mmHg, HR is 103 beats per minute, RR is 14 breaths per minute, temperature is 98.9°F, and oxygen saturation is 99% on room air. Which of the following is the most appropriate next step in management?
Administer one dose of ceftriaxone and doxycycline for 10 days and have him follow-up with a urologist
. Swab his urethra, send a culture for gonorrhea and Chlamydia, and treat if positive
. Send a urinalysis and treat for a urinary tract infection (UTI) if positive
. Treat the patient for epididymitis and have him return if symptoms persist
. Order a statim (STAT) color Doppler ultrasound and urologic consultation
8) A 55-year-old woman with a past medical history of diabetes walks into the emergency department (ED) stating that her tongue and lips feel like they are swollen. During the history, she tells you that her doctor just started her on a new blood pressure (BP) medication. Her only other medication is a baby aspirin. Her vitals at triage are: BP 130/70 mmHg, heart rate (HR) 85 beats per minute, respiratory rate (RR) 16 breaths per minute, oxygen saturation 99% on room air, and temperature 98.7°F. On physical examination, you detect mild lip and tongue swelling. Over the next hour, you notice that not only are her tongue and lips getting more swollen, but her face is starting to swell, too. What is the most likely inciting agent?
. Metoprolol
. Furosemide
. Aspirin
. Lisinopril
. Diltiazem
9) A 45-year-old woman presents to the ED immediately after landing at the airport from a transatlantic flight. She states that a few moments after landing she felt short of breath and felt pain in her chest when she took a deep breath. Her only medications are oral contraceptive pills and levothyroxine. She is a social drinker and smokes cigarettes occasionally. Her BP is 130/75 mmHg, HR is 98 beats per minute, temperature is 98.9°F, RR is 20 breaths per minute, and oxygen saturation is 97% on room air. You send her for a duplex ultrasound of her legs, which is positive for deep vein thrombosis. What is the most appropriate management for this patient?
. Place patient on a monitor, provide supplemental oxygen, and administer unfractionated heparin
. Place patient on a monitor, order a chest computed tomography (CT) scan to confirm a pulmonary embolism (PE), and then administer unfractionated heparin
. Place patient on a monitor and administer aspirin
. Instruct the patient to walk around the ED so that she remains mobile and does not exacerbate thrombus formation
. Place the patient on a monitor, provide supplemental oxygen, and administer warfarin
10) A tall, thin 18-year-old man presents to the ED with acute onset of dyspnea while at rest. The patient reports sitting at his desk when he felt a sharp pain on the right side of his chest that worsened with inspiration. His past medical history is significant for peptic ulcer disease. He reports taking a 2-hour plane trip a month ago. His initial vitals include an HR of 100 beats per minute, a BP of 120/60 mmHg, an RR of 16 breaths per minute, and an oxygen saturation of 97% on room air. On physical examination, you note decreased breath sounds on the right side. Which of the following tests should be performed next?
. Electrocardiogram (ECG)
. D-dimer
. Ventilation perfusion scan (V/Q scan)
. Upright abdominal radiograph
. Chest radiograph
11) A 30-year-old obese woman with no significant past medical history presents to the ED complaining of shortness of breath and coughing up blood-streaked sputum. The patient states that she traveled to Moscow a month ago. Upon returning to the United States, the patient developed a persistent cough associated with dyspnea. She was seen by a pulmonologist, who diagnosed her with bronchitis and prescribed an inhaler. However, over the following weeks, the patient’s symptoms worsened, and she developed pleuritic chest pain. In the ED, she lets you know that she smokes half a pack per day. Her vitals include a temperature of 99°F, BP of 105/65 mmHg, HR of 124 beats per minute, RR of 22 breaths per minute, and an oxygen saturation of 94% on room air. Physical examination is noncontributory, except for rales at the left-mid lung. Her ECG reveals sinus tachycardia with large R waves in V1 to V3 and inverted T waves. Given this patient’s history and presentation, what is the most likely etiology of her symptoms?
. Mycoplasma pneumoniae (“walking” pneumonia)
. Q fever pneumonia
. Pneumocystis jiroveci pneumonia (PCP)
. PE
. Acute respiratory distress syndrome (ARDS)
12) A 24-year-old woman is brought to the ED after being found on a nearby street hunched over and in mild respiratory distress. Upon arrival, she is tachypneic at 24 breaths per minute with an oxygen saturation of 97% on face mask oxygen administration. Upon physical examination, the patient appears to be in mild distress with supraclavicular retractions. Scattered wheezing is heard throughout bilateral lung fields. Which of the following medications should be administered first?
. Corticosteroids
. Magnesium sulfate
. Epinephrine
. Anticholinergic nebulizer treatment
. β2-Agonist nebulizer treatment
13) An 81-year-old woman presents to the ED with acute onset of shortness of breath just before arrival. She refuses to answer questions for the interview, but repeatedly states that she is feeling short of breath. Her initial vitals include an HR of 89 beats per minute, a BP of 168/76 mmHg, and an RR of 18 breaths per minute with an oxygen saturation of 89% on room air. A portable chest x-ray appears normal. Her physical examination is unremarkable, except for a systolic ejection murmur. Intravenous (IV) access is successfully obtained. After placing the patient on oxygen and a monitor, which of the following should be performed first?
. Evaluation of troponin level
. Evaluation of D-dimer level
. Rectal temperature
. Repeat chest x-ray
. ECG
14) As you evaluate a patient with shortness of breath, you appreciate decreased breath sounds at the left-lung base. You suspect the patient has a small pleural effusion. In which of the following views of the chest is this small pleural effusion most likely to be detected?
. Supine
. Lateral decubitus right-side down
. Lateral decubitus left-side down
. Lateral
. Posterior-anterior (PA)
15) A 32-year-old firefighter presents to the ED in acute respiratory distress. He was taken to the ED shortly after extinguishing a large fire in a warehouse. His initial vitals include an HR of 90 beats per minute, a BP of 120/55 mmHg, and an RR of 18 breaths per minute with an oxygen saturation of 98% on 2-L nasal cannula. An ECG shows a first-degree heart block. Upon physical examination, there are diffuse rhonchi bilaterally. The patient is covered in soot and the hairs in his nares are singed. Given this clinical presentation, which of the following maybe responsible for this patient’s respiratory distress?
. Reactive airway disease
. Foreign body aspiration
. Decompression sickness
. Thermal burns
. Pneumothorax
16) A 76-year-old man presents to the ED in acute respiratory distress, gasping for breath while on face mask. Paramedics state that he was found on a bench outside of his apartment in respiratory distress. Initial vitals include an HR of 90 beats per minute, a BP of 170/90 mmHg, and an RR of 33 breaths per minute with an oxygen saturation of 90%. Upon physical examination, the patient is coughing up pink, frothy sputum, has rales two-thirds of the way up both lung fields, and has pitting edema of his lower extremities. A chest radiograph reveals bilateral perihilar infiltrates, an enlarged cardiac silhouette, and a small right-sided pleural effusion. After obtaining IV access and placing the patient on a monitor, which of the following medical interventions is most appropriate?
. Morphine sulfate only
. Nitroglycerin only
. Nitroglycerin and a loop diuretic
. Aspirin
. Antibiotics
17) A 67-year-old man is brought to the ED in respiratory distress. His initial vitals include an HR of 112 beats per minute, a BP of 145/88 mmHg, and an RR of 18 breaths per minute with an oxygen saturation of 92% on room air. He is also febrile at 102°F. After obtaining IV access, placing the patient on a monitor, and administering oxygen via nasal cannula, a chest radiograph is performed and shows patchy alveolar infiltrates with consolidation in the lower lobes. On review of systems, the patient tells you that he had five to six watery bowel movements a day for the last 2 days with a few bouts of emesis. Which of the following infectious etiologies is most likely responsible for the patient’s presentation?
. Streptococcus pneumoniae
. Haemophilus influenzae
. Mycoplasma pneumoniae
. Chlamydophila pneumoniae
. Legionella pneumophila
18) A 32-year-old woman presents to the ED with a 1-month history of general malaise, mild cough, and subjective fevers. She states that she is human immunodeficiency virus (HIV) positive and her last CD4 count, 6 months ago, was 220. She is not on antiretroviral therapy or any other medications. Initial vitals include an HR of 88 beats per minute, a BP of 130/60 mmHg, and an RR of 12 breaths per minute with an oxygen saturation of 91% on room air. Her chest radiograph shows bilateral diffuse interstitial infiltrates. Subsequent laboratory tests are unremarkable except for an elevated lactate dehydrogenase level. Given this patient’s history and physical examination, which of the following is the most likely organism responsible for her clinical presentation?
. Coccidioides immitis
. Mycobacterium tuberculosis
. Pneumocystis jiroveci
. Mycoplasma pneumoniae
. Haemophilus influenzae
19) A 27-year-old woman presents to the ED complaining of an intensely pruritic rash all-over her body, abdominal cramping, and chest tightness. She states that 1 hour ago she was at dinner and accidentally ate some shrimp. She has a known anaphylactic allergy to shrimp. Her BP is 115/75 mmHg, HR is 95 beats per minute, temperature is 98.9°F, RR is 20 breaths per minute, and oxygen saturation is 97% on room air. She appears anxious, and her skin is flushed with urticarial lesions. Auscultation of her lungs reveals scattered wheezes with decreased air entry. Which of the following is the most appropriate next step in management?
. Administer oxygen via non-rebreather, place a large-bore IV, begin IV fluids, and administer methylprednisolone intravenously
. Administer oxygen via non-rebreather, place a large-bore IV, begin IV fluids, and administer methylprednisolone and diphenhydramine intravenously
. Administer oxygen via non-rebreather, place a large-bore IV, begin IV fluids, administer methylprednisolone and diphenhydramine intravenously, and give intramuscular epinephrine
. Administer oxygen via non-rebreather, place a large-bore IV, begin IV fluids, and start aerosolized albuterol
. Administer oxygen via non-rebreather, place a large-bore IV, begin IV fluids, and start aerosolized epinephrine
20) A 72-year-old man presents to the ED with worsening dyspnea. His initial vitals include an HR of 93 beats per minute, BP of 110/50 mmHg, and RR of 20 breaths per minute with an oxygen saturation of 88% on room air. The patient appears thin and anxious. He is using accessory muscles to breathe. Despite distant breath sounds, you hear end-expiratory rhonchi and a prolonged expiratory phase. An ECG shows peaked P waves in leads II, III, and aVF. Given this patient’s history and physical examination, which of the following conditions does this patient most likely have?
. Chronic bronchitis
. Asthma
. Emphysema
. Congestive heart failure (CHF)
. Pneumothorax
21) A 71-year-old woman presents to the ED after a reported mechanical fall 2 days ago. Her initial vitals include an HR of 55 beats per minute, a BP of 110/60 mmHg, an RR of 14 breaths per minute, and an oxygen saturation of 96% on room air. The patient does not appear to be taking deep breaths. Her physical examination is significant for decreased breath sounds bilaterally and tenderness to palpation along the right side of her chest. After initial stabilization, which of the following is the diagnostic test of choice for this patient’s condition?
. Chest x-ray
. Chest CT scan
. ECG
. Rib radiographs
. Thoracentesis
22) A 29-year-old woman presents to the ED for hyperventilation. Her initial vitals include an RR of 28 breaths per minute with an oxygen saturation of 100% on room air. She is able to speak in full sentences and tells you that she cannot breathe and that her hands and feet are cramping up. She denies any trauma, past medical history, or illicit drug use. Chest auscultation reveals clear breath sounds bilaterally. A subsequent chest radiograph is normal. Upon reevaluation, the patient reports that she is breathing better. Her vitals include an RR of 12 breaths per minute with an oxygen saturation of 100% on room air. Which of the following conditions is most likely the etiology of this patient’s symptoms?
. Pneumothorax
. Hemopneumothorax
. Pleural effusion
. Anxiety attack
. Asthma exacerbation
23) A 42-year-old man presents to the ED via ambulance after activating EMS for dyspnea. He is currently on an oxygen face mask and was administered one nebulized treatment of a β2-agonist by the paramedics. His initial vitals include an RR of 16 breaths per minute with an oxygen saturation of 96% on room air. The patient appears to be in mild distress with some intercostal retractions. Upon chest auscultation, there are minimal wheezes localized over bilateral lower lung fields. The patient’s symptoms completely resolve after two more nebulizer treatments. Which of the following medications, in addition to a rescue β2-agonist inhaler, should be prescribed for outpatient use?
. Magnesium sulfate
. Epinephrine injection (EpiPen)
. Corticosteroids
. Cromolyn sodium
. Ipratropium
24) A 22-year-old woman is brought to the ED by paramedics who state that they found the patient hunched over on a park bench barely breathing. The patient is rousable only to painful stimuli. Her initial vitals include an HR of 78 beats per minute, a BP of 125/58 mmHg, and a respiratory rate of 6 breaths per minute with an oxygen saturation of 94% on 2-L nasal cannula. Upon physical examination, the patient has clear breath sounds bilaterally and no signs of trauma. Her pupils are 2 mm bilaterally and reactive to light. Which of the following agents may be used to restore this patient’s respirations?
. Oxygen
. Flumazenil
. Anticholinergic inhaler treatment
. β2-Agonist nebulized treatment
. Naloxone
25) A 43-year-old undomiciled man is brought to the ED after being found intoxicated on the street. He is currently rousable and expresses a request to be left alone. Initial vitals include an HR of 92 beats per minute, a BP of 125/80 mm Hg, and an RR of 14 breaths per minute with an oxygen saturation of 93% on room air. His rectal temperature is 101.2°F. A chest radiograph shows infiltrates involving the right lower lobe. Given this clinical presentation, what initial antibiotic coverage is most appropriate for this patient?
. Gram-negative coverage only
. Gram-positive coverage only
. Broad-spectrum with anaerobic coverage
. PCP coverage
. Antifungal therapy
26) A 32-year-old man is brought into the ED by EMS with fever, shortness of breath, and stridor. The patient was treated yesterday in the ED for a viral syndrome. His BP is 90/50 mmHg, HR is 110 beats per minute, temperature is 101.2°F, and his RR is 28 breaths per minute. A chest radiograph reveals a widened mediastinum. The patient is endotracheally intubated, given a 2-L bolus of normal saline, and started on antibiotics. His BP improves to 110/70 mmHg and he is transferred to the intensive care unit (ICU). You see a friend that accompanied the patient to the hospital and ask him some questions. You find out that the patient is a drum maker and works with animal hides. What is the most likely organism that is responsible for the patient’s presentation?
. Streptococcus pneumoniae
. Corynebacterium diphtheriae
. Coxiella burnetii
. Haemophilus influenzae
. Bacillus anthracis
27) A 62-year-old man presents to the ED with gradual dyspnea over the last few weeks. He reports that he is a daily smoker and has not seen a physician in years. Upon physical examination, there are decreased breath sounds on the right as compared to the left. A chest radiograph indicates blunting of the right costophrenic angle with a fluid line. A thoracentesis is performed. Given this patient’s history, which of the following most likely describes his effusion?
. Transudative effusion
. Exudative effusion
. Transudative and exudative effusion
. Lactate dehydrogenase < 200 units
. Fluid-to-blood protein ratio < 0.5
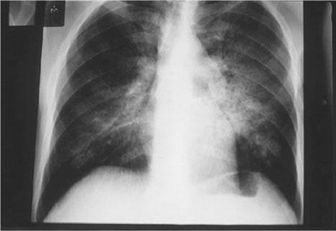
28) A 40-year-old man with a history of untreated HIV for 8 years comes into the ED complaining of cough, fever, and malaise for 3 days. He is tachypneic and diaphoretic. Chest radiograph reveals bilateral infiltrates. Arterial blood gas (ABG) analysis is significant for a PaO2 of 62 on room air. His chest radiograph is seen below. Which of the following is the most appropriate initial management?
Image

. Treat with corticosteroid prior to antibiotic therapy
. Treat immediately with IV trimethoprim/sulfamethoxazole (TMP/SMX)
. Administer antibiotics after a rapid sputum Gram stain is obtained
. Treat with nebulizer
. Treat with racemic epinephrine
29) A 34-year-old Caucasian female comes to the emergency department and complains that her heart is "racing out of control." She began to feel this way only this morning. She denies any chest pain or shortness of breath. Over the past few months, she has unintentionally lost 10 pounds. Her past medical history is significant for panic attacks, but she claims she has not had an attack for over 10 years. She is very concerned because her father died of a heart attack at the age of 40. The EKG reveals sinus tachycardia at a rate of 120/min. The initial labs show: CBC: Hb 12.9g/dL, Ht 39%, MCV 88 fl, Platelet count 200,000/cmm, Leukocyte count 8,500/cmm, Neutrophils 67%, Eosinophils 1%, Lymphocytes 24%, Monocytes 8%. Serum: Serum Na 139 mEq/L, Serum K 4.2 mEq/L, Chloride 100 mEq/L, Bicarbonate 25 mEq/L, BUN 10 mg/dL, Serum Creatinine 1.0 mg/dL, Calcium 9.1 mg/dL, Blood Glucose 102 mg/dL, TSH < 0.1 microU/mL, Free T4 4.6 ng/dL (N0.9-24). Which of the following is the best immediate step to control this patient's symptoms?
. Propylthiouracil
. Subtotal thyroidectomy
. Alprazolam
. Radioactive Iodine
. Propanolol
30) A 45-year-old male, found unconscious, is brought to the emergency room. His airway is maintained, and oxygen is administered. His temperature is 39.0°C (102.5°F), pulse is 102/min, blood pressure is 90/65 mmHg and respirations are 23/min. Intravenous access is secured and blood and urine samples are drawn. Lab results are as follows: Sodium 134 mEq/L, Potassium 5.9 mEq/L, Chloride 101 mEq/L, Bicarbonate 22 mEq/L, Blood urea nitrogen 110 mg/dl, Glucose 1000 mg/dl, Serum calcium 10.2 mg/dl, Amylase 100 U/L, Aspartate aminotransferase 15 U/L, Alanine aminotransferase 17 U/L, Ammonia 15 micro-moi/L (Normal is 9-33 micro-moi/L), PT 13 sec, APTT 30 sec. Arterial blood gases: PH 7.40, PaCO2 38 mm Hg, PaO2 90 mm Hg. Which of the following is the most appropriate initial infusion you should order for this patient?
. Normal saline
. 0.45% saline
. 5% dextrose
. Regular insulin
. Potassium
31) A 24-year-old woman comes into the emergency department with recurrent episodes of palpitations, headache, and tremor. Her blood pressure is 155/95 mmHg, heart rate is 135/min, temperature is 37.9°C (100.2°F), and respiratory rate is 12/min. A CT of the abdomen shows a suprarenal mass. After confirming the diagnosis with a laboratory test, the physician informs the patient that she will require immediate therapy and surgical resection of the mass within the next few weeks. In order to achieve short-term control of her blood pressure, which of the following agents is most appropriate?
Furosemide
Hydralazine
Phenelzine
Prazosin
Propanolol
32) An 18-year-old woman presents to the emergency department with acute mental status changes, rapid and deep breathing, abdominal pain, and vomiting. On examination she is tachypneic and tachycardic, her abdomen is soft and nontender, and her mucous membranes are dry. Laboratory values are notable for a potassium level of 5.5 mEq/L, bicarbonate of 12 mEq/L, and serum glucose of 400 mg/dL. Which of the following is the most appropriate strategy during the first 24 hours?
Diuresis and ventilatory support
Diuresis, strict potassium restriction, and insulin
Intravenous fluids, insulin, and potassium
Intravenous fluids, insulin, and strict potassium restriction
Intravenous fluids, loop diuretic, and potassium
33) A 13-year-old boy is brought to the pediatrician by his mother because of increasing body hair. Several months earlier he had been diagnosed with 17α-hydroxylase deficiency and treated with hydrocortisone. Physical examination reveals an overweight boy with a moderate amount of both chest and genital hair, and some facial hair growth. His physical examination is otherwise unremarkable. Which of the following is the best treatment for this patient?
Add cosyntropin
Add dexamethasone
Add spironolactone
Increase hydrocortisone
Keep the current dose of hydrocortisone
34) A 72-year-old man with atrial fibrillation presents with complaints of fatigue and feeling cold. He also notes constipation and dry skin. His daughter states he has seemed more forgetful over the past several months. His temperature is 37.3°C (99.1°F), heart rate is 48/min, and blood pressure is 130/82 mmHg. Cardiac examination shows bradycardia but normal rhythm, and normal S1 and S2 with no murmurs; the lungs are clear to auscultation bilaterally and the abdomen is soft and nontender. The patient’s extremities are cool and puffy with dry, coarse skin. Laboratory studies show a thyroid-stimulating hormone level of 32 μU/L, free thyroxine of 0.3 ng/dL, and total tri-iodothyronine of 30 ng/dL. What medication is the patient likely taking for his atrial fibrillation?
Amiodarone
Flecainide
Lithium
Methimazole
Sotalol
35) A 75-year-old woman is brought to the emergency department after being found unresponsive at her home. She was last spoken to by her daughter on the phone 24 hours earlier, at which time she complained of chills, lethargy, and weakness. The woman has had a heart attack in the past, she has high blood pressure, and she had a total thyroidectomy performed a decade ago for cancer. The daughter had returned from several months out of town, and is unsure if the patient was taking her medications. Her temperature is 34.9°C (94.9°F), pulse is 48/min, blood pressure is 110/65 mmHg, oxygen saturation is 99% on 100% oxygen, and glucose is 85 mg/dL. On examination the patient is unresponsive, obese, and edematous with periorbital edema. Her cardiac and pulmonary examinations are normal. CT of the head reveals no signs of trauma or increased intracranial pressure, and ECG demonstrates no acute ischemic changes. Blood is drawn for laboratory testing. Which of the following is most appropriate for treating the patient’s mental status change?
Aspirin
Glucagon
Hemodialysis
Levothyroxine
Metoprolol
36) A family brings their 82-year-old grandmother to the emergency room stating that they cannot care for her anymore. They tell you, “She has just been getting sicker and sicker.” Now she stays in bed and won’t eat because of stomach pain. She has diarrhea most of the time and can barely make it to the bathroom because of her weakness. Her symptoms have been worsening over the past year, but she has refused to see a doctor. The patient denies symptoms of depression. Blood pressure is 90/54 mmHg with the patient supine; it drops to 76/40 mmHg when she stands. Heart and lungs are normal. Skin examination reveals a bronze coloring to the elbows and palmar creases. What laboratory abnormality would you expect to find in this patient?
. Low serum Ca+
. Low serum K+
. Low serum Na+
. Normal serum K+
. Microcytic anemia
37) A 58-year-old woman presents to her physician because of neck discomfort and difficulty swallowing. She first began to have difficulty with swallowing solids 2 years ago, but the problem is getting progressively worse. She denies hemoptysis, hematemesis, abdominal pain, or change in bowel habits. She is a nonsmoker and past medical history is significant only for mild hypertension. Her temperature is 36.9°C (98.4°F), heart rate is 72/min, and blood pressure is 132/78 mmHg. She has an asymmetrically enlarged thyroid gland that is particularly firm on the right, with poorly palpable borders. Laboratory evaluation reveals a free thyroxine level of 4.1 ng/dL and thyroid-stimulating hormone of 5μU/mL. Based on the results of a radioisotope scan and a fine needle aspiration biopsy, the physician decides to perform surgery. For which of the following is the patient at increased risk postoperatively?
Bone metastases
Hypercalcemia
Hypocalcemia
Hypophosphatemia
Pheochromocytoma
38) A 53-year-old woman presents to the clinic with complaints of headache and blurred vision for the past several months. She also says her family has commented that her face looks different, and her nose is bigger than it used to be. In addition, she says her shoes feel tighter. On physical examination she has coarse facial features with a prominent mandible and widely spaced incisors. MRI of the brain reveals a mass in the pituitary. This patient may be at increased risk of developing which of the following malignancies?
Colon cancer
Hepatocellular carcinoma
Lung cancer
Malignant brain tumor
Pancreatic adenocarcinoma
39) A 35-year-old white female comes to her primary care physician for the evaluation of palpitations, weight loss, increased appetite and diarrhea for the past 2 months. She denies smoking cigarettes or drinking alcohol. Her temperature is 37.1°C (98°F), blood pressure is 135/80 mmHg, respirations are 14/min, and pulse is 90/min. Physical examination shows exophthalmos, lid lag, lid retraction, and a diffusely enlarged, non-tender thyroid gland. Lab studies show very low levels of serum TSH, and increased levels of serum free T4 and T3. The diagnosis of Graves' disease is established. Various treatment options are discussed with the patient, and she opts for long-term treatment with propylthiouracil. Which of the following conditions is this patient at risk for developing?
. Agranulocytosis
. Hypocalcemia
. Permanent hypothyroidism
. Recurrent laryngeal nerve palsy
. Thyroid cancer
40) A 35-year-old white female presents with complaints of weight gain, lethargy and constipation for the last 2 months. She also complains of cold intolerance and oligomenorrhea. She is not taking any medication. She is a non-smoker, and does not drink alcohol. Her pulse is 67/min, and blood pressure is 130/90 mmHg. She is afebrile. Her hands are dry and cold. There is a non-tender, diffuse rubbery enlargement of the thyroid gland without any discrete nodularity. She does not have exophthalmos, lid lag or lid retraction. Labs show decreased serum T4 levels, elevated serum TSH levels and positive anti-thyroperoxidase (TPO) antibodies. Which of the following complications may develop in this patient?
. Lymphoma of the thyroid
. Papillary carcinoma of the thyroid
. Follicular carcinoma of the thyroid
. Anaplastic carcinoma of the thyroid
. Medullary carcinoma of the thyroid
41) A 36-year-old female presents with weight loss, palpitations, mild shortness of breath, heat intolerance, tremors, and increased sweating. She does not have any past medical problems. Her family history is unremarkable. Her blood pressure is 140/70 mmHg, heart rate is 104/min and regular, temperature is 99.0°F (37.2°C) and respiratory rate is 22/min. Physical examination reveals a 2 x 2 cm nodule in her left thyroid lobe. The rest of her thyroid gland feels normal. There are no palpable lymph nodes in her neck. Eye examination reveals minimal lid lag, but no signs of proptosis or chemosis. She has tremors in both of her upper extremities. Her hands are moist and warm. Thyroid function testing reveals: Serum TSH < 0.03 micro IU/ml, Total T3 330 ng/dl, Total T4 14 mcg/dl. Radioactive iodine scan shows uptake only in her left-sided nodule. Which of the following disorders is this patient at risk of developing if she is left untreated?
. Bone loss
. Airway compression
. Thyroid cancer
. Coronary artery disease
. Proptosis
42) A 55-year-old male presents with complaints of an ulcer over the sole of his right great toe for one week. His medical problems include a ten year history of hypertension, diabetes and hypercholesterolemia. His current medications are ramipril, aspirin, metformin, glibenclamide and pravastatin. He has a 20-pack year history of smoking and occasionally drinks alcohol. He denies illegal drug use or multiple sexual partners. Which of the following is most likely contributing to the development of his foot ulcer?
. History of smoking
. Diabetic neuropathy
. Poor glycemic control
. Peripheral vascular disease
. Bony abnormality of the foot
43) A 49-year-old woman presents to the emergency department (ED) with profuse, foul-smelling, watery diarrhea and abdominal pain. Five days ago, she was hospitalized for urosepsis and treated with amoxicillin and sulbactam. She recovered well, and was discharged three days ago with a prescription for oral amoxicillin plus clavulanic acid. Her current temperature is 38.8°C (101.9°F), blood pressure is 110/70 mmHg, pulse is 102/min, and respirations are 15/min. Abdominal examination shows tenderness in the left lower quadrant. CBC shows a WBC count of 25,000/microl. She is started on intravenous normal saline in the ED. Which of the following is the most appropriate next step in management?
. Continue rehydration
. Start oral metronidazole
. Discontinue antibiotics
. Discontinue antibiotics and start oral metronidazole
. Discontinue antibiotics and start oral vancomycin
44) A 64-year-old man is brought to the ER after an episode of coffee ground emesis followed by lightheadedness. He has been having black, tarry stools for the past few days. He has a history of coronary artery disease and he underwent coronary artery bypass surgery three years ago. He is currently taking aspirin, metoprolol, lisinopril, and pravastatin. He drinks 2-3 beers over the weekend but he quit smoking after the bypass surgery. His temperature is 36.7°C (98°F), pulse is 110/min, respirations are 16/min, and blood pressure is 90/60 mmHg. Examination shows coffee ground-like material in the oropharynx. His lungs are clear. Abdomen is slightly tender in the epigastrium. Laboratory studies show: Complete blood count: Leukocyte count 9,500/mm3, Hemoglobin 8.1 g/L, Platelets 130,000/mm3. Chemistry panel: Serum sodium 140 mEq/L, Serum potassium 3.5 mEq/L, Bicarbonate 27 mEq/L, Blood urea nitrogen (BUN) 54 mg/dL, Serum creatinine 1.2 mg/dL Which of the following is the most appropriate next step in management of this patient?
. Whole blood transfusion
. Packed red blood cell transfusion
. Fresh frozen plasma infusion
. Hemodialysis
. Platelet transfusion
45) A 50-year-old female presents with heartburn and gnawing abdominal pain. She was diagnosed with peptic ulcer disease 3 years ago, but she has been non-adherent to her medications. She asks you if her nonadherence puts her at increased risk of any complications. Which of the following is the most common complication of peptic ulcer disease?
. Perforation
. Penetration
. Gastric outlet obstruction
. Hemorrhage
. Atrophic gastritis
46) A 37 -year-old male is brought to the emergency department due to an episode of hematemesis. He has a history of peptic ulcer disease. A nasogastric tube lavage yields coffee-ground-like material. Physical examination reveals pallor and delayed capillary refill, without cyanosis. His temperature is 36.7°C (98°F), blood pressure is 85/40 mmHg, pulse is 125/min, and respirations are 18/min. Which of the following is the most appropriate first step in management?
. Upper GI endoscopy
. Surgical intervention
. Intravenous pantoprazole
. Fluid resuscitation
. Intravenous octreotide
47) A 54-year-old man is brought to the ER because of an episode of coffee ground emesis and lightheadedness. He has a history of intravenous drug use, hepatitis C infection, and alcohol use. He says he has not had an alcoholic drink for about three days. He has been noncompliant with medications and follow-ups. He takes no medications. His temperature is 36.7°C (98°F), pulse is 110/min, respirations are 16/min, and blood pressure is 90/60 mmHg. Scleral icterus is present. Examination shows coffee ground material in the oropharynx. His lungs are clear. His abdomen is distended and a fluid wave is present. He is slightly tender to palpation in the epigastrium. Laboratory studies show: Complete blood count:Leukocyte count 9,500/mm3, Hemoglobin 10.0 g/L, Platelets 120,000/mm3. Chemistry panel:Serum sodium 140 mEq/L, Serum potassium 3.5 mEq/L, Bicarbonate 27 mEq/L, Blood urea nitrogen (BUN) 34 mg/dL, Serum creatinine 0.8 mg/dL. Coagulation studies :Prothrombin time 27 sec, Partial thromboplastin time 42 sec. Which of the following is the most appropriate next step in the management of this patient?
. Whole blood transfusion
. Fresh frozen plasma infusion
. Hemodialysis
. Pooled platelet transfusion
. Plasmapheresis
48) An undomiciled 41-year-old man walks into the ED complaining of abdominal pain, nausea, and vomiting. He tells you that he has been drinking beer continuously over the previous 18 hours. On examination, his vitals are BP 150/75 mm Hg, HR 104 beats per minute, RR 16 breaths per minute, oxygen saturation 97% on room air, temperature of 99.1°F rectally, and finger stick glucose 81 mg/dL. The patient is alert and oriented, his pupils anicteric. You notice gynecomastia and spider angiomata. His abdomen is soft but tender in the RUQ. Laboratory tests reveal an AST of 212 U/L, ALT 170 U/L, alkaline phosphatase of 98 U/L, total bilirubin of 1.9 mg/dL, international normalized ratio (INR) of 1.3, WBC 12,000/μL. Urinalysis shows 1+ protein. Chest x-ray is unremarkable. Which of the following is the most appropriate next step in management?
. Place a nasogastric tube in the patient’s stomach to remove any remaining ethanol
. Order a HIDA scan to evaluate for acute cholecystitis
. Administer hepatitis B immune globulin
. Send viral hepatitis titers
. Provide supportive care by correcting any fluid and electrolyte imbalances
49) An 84-year-old woman with coronary artery disease, congestive heart failure, peripheral vascular disease, and atrial fibrillation presents to the emergency department with dizziness, weakness, and sudden-onset crampy periumbilical pain. The pain is associated with one episode of diarrhea and one episode of emesis. The patient notes she has been having similar pain after meals for “several months” but never this severe. Her temperature is 37.2°C (98.9°F), heart rate is 135/min, blood pressure is 96/60 mm Hg, and respiratory rate is 16/min. Physical examination is notable for a slightly distended abdomen that is extremely tender to palpation with diminished bowel sounds. There is no rigidity or rebound tenderness noted on the abdominal examination. In addition, the patient has heme positive stool. Her WBC count is 19,500/mm³, hemoglobin is 10.9 g/dL, and platelet count is 159,000/mm³. Liver function testing results are normal. After stabilizing the patient, what is the best next step in management?
Barium enema
Colonoscopy
Laparotomy
Obstruction series
Warfarin therapy
50) A 51-year-old man is brought to the emergency department (ED) by emergency medical services (EMS) with a blood pressure (BP) of 90/60 mm Hg, heart rate (HR) of 110 beats per minute, respiratory rate (RR) of 18 breaths per minute, and oxygen saturation of 97% on room air. The patient tells you that he has a history of bleeding ulcers. On examination, his abdomen is tender in the epigastric area. He is guaiac positive, with black stool. He has a bout of hematemesis and you notice that his BP is now 80/50 mm Hg, HR is 114 beats per minute, as he is slowly starting to drift off. Which of the following is the most appropriate next step in therapy?
. Assess airway, establish two large-bore intravenous (IV) lines, cross-match for two units of blood, administer 1 to 2 L of normal saline, and schedule an emergent endoscopy
. Assess airway, establish two large-bore IVs, cross-match for 2 units of blood, and administer a proton pump inhibitor
. Place two large-bore IVs, cross-match for 2 units of blood, administer 1 to 2 L of normal saline, and schedule an emergent endoscopy
. Intubate the patient, establish two large-bore IVs, cross-match for 2 units of blood, administer 1 to 2 L of normal saline, and schedule an emergent endoscopy
. Intubate the patient, establish two large-bore IVs, cross-match for 2 units of blood, and administer a proton pump inhibitor
51) A 19-year-old woman presents to the ED with 1 hour of acute-onset progressively worsening pain in her RLQ. She developed nausea shortly after the pain and vomited twice over the last hour. She had similar but less severe pain 2 weeks ago that resolved spontaneously. Her BP is 123/78 mm Hg, HR is 99 beats per minute, temperature is 99.1°F, and her RR is 16 breaths per minute. On physical examination, the patient appears uncomfortable, not moving on the gurney. Her abdomen is nondistended, diffusely tender, worst in the RLQ. Pelvic examination reveals a normal-sized uterus and moderate right-sided adnexal tenderness. Laboratory results reveal WBC 10,000/μL, hematocrit 38%, and a negative urinalysis and β-hCG. Pelvic ultrasound reveals an enlarged right ovary with decreased flow. Which of the following is the most appropriate management for this patient?
. Admit to the gynecology service for observation
. Administer IV antibiotics and operate once inflammation resolves
. Attempt manual detorsion
. Order an abdominal CT
. Go for immediate laparoscopic surgery
52) A 22-year-old woman is brought to the ED by ambulance complaining of sudden onset of severe abdominal pain for 1 hour. The pain is in the RLQ and is not associated with nausea, vomiting, fever, or diarrhea. On the pelvic examination you palpate a tender right adnexal mass. The patient’s last menstrual period was 6 weeks ago. Her BP is 95/65 mm Hg, HR is 124 beats per minute, temperature is 99.8°F, and RR is 20 breaths per minute. Which of the following are the most appropriate next steps in management?
. Provide her oxygen via face mask and administer morphine sulfate
. Administer morphine sulfate, order an abdominal CT with contrast, and call an emergent surgery consult
. Send the patient’s urine for analysis and order an abdominal CT
. Bolus 2 L NS, order a type and crossmatch and β-hCG, and call gynecology for possible surgery
. Provide oxygen via face mask, give morphine sulfate, and order a transvaginal ultrasound
53) A 67-year-old man is brought to the ED by emergency medical service (EMS). His wife states that the patient was doing his usual chores around the house when all of a sudden he started complaining of severe abdominal pain. He has a past medical history of coronary artery disease and hypertension. His BP is 85/70 mm Hg, HR is 105 beats per minute, temperature is 98.9°F, and his RR is 18 breaths per minute. On physical examination, he is diaphoretic and in obvious pain. Upon palpating his abdomen, you feel a large pulsatile mass. An electrocardiogram (ECG) reveals sinus tachycardia. You place the patient on a monitor, administer oxygen, insert two largebore IVs, and send his blood to the laboratory. His BP does not improve after a 1-L fluid bolus. Which of the following is the most appropriate next step in management?
. Order a CT scan to evaluate his aorta
. Call the angiography suite and have them prepare the room for the patient
. Order a portable abdominal radiograph
. Call surgery and have them prepare the operating room (OR) for an exploratory laparotomy
. Call the cardiac catheterization laboratory to prepare for stent insertion
54) A 32-year-old man with Crohn’s disease presents to the emergency department with acute-onset diffuse abdominal pain and emesis. The patient states these symptoms are different than his usual Crohn’s disease flare-ups. The pain is severe (10/10) and is cramping in nature. He says his abdomen feels larger than usual. His Crohn’s disease has been well managed on 6-mercaptopurine for the past 6 months. The patient denies any recent sick contacts or eating underprepared foods. He states he had a bowel movement and flatus since the abdominal pain began. In addition to Crohn’s disease, the patient had appendicitis for which he underwent an appendectomy 12 years ago. His temperature is 37.1°C (98.7°F), blood pressure is 135/86 mm Hg, pulse is 84/min, and respiratory rate is 14/ min. On physical examination the abdomen is distended and diffusely tender with high-pitched bowel sounds. There is rebound tenderness throughout the abdomen along with guarding. The remainder of the physical examination is noncontributory. An x-ray of the abdomen shows dilated small loops of bowel along with absence of gas in the colon. What is the best next step in management?
Bowel rest only
Intravenous fluids and antibiotics only
Laparotomy
MRI of the abdomen
Ultrasound
55) A 24-year-old man with a history of depression is brought to the emergency room because of a drug overdose. He is experiencing some nausea and vomiting, but no other symptoms. Physical examination and vital signs are normal. Six hours prior to presentation, he intentionally took 40 tablets of acetaminophen (500mg/tablet). Which of the following is the most appropriate next step in management?
. Give ethanol to compete with the parent drug for metabolism, therefore preventing formation of toxic metabolites
. give Narcan to block its actions directly
. Give intravenous prostacyclins to maintain cellular integrity
. give N-acetylcysteine to allow binding of the toxic metabolite
. Give glucocorticoids to block the immune cascade
56) A 58-year-old man comes to the emergency department complaining of colicky abdominal pain over the past 3 days that suddenly became more severe and constant over the past 6 hours. A contrast study is performed and results are shown in the image. What is the first-line treatment after fluid resuscitation and nasogastric tube placement?

Image

Colonoscopy
Hemicolectomy
Proximal colostomy with delayed resection
Sigmoid colectomy
Sigmoidoscopy
57) A 59-year-old woman with renal cell carcinoma presents to the emergency department with severe right upper quadrant (RUQ) pain. She is afebrile, acutely tender in the RUQ, and has shifting dullness and a palpable liver edge. Murphy’s sign is negative. Laboratory studies show: Na+: 138 mEq/L, K+: 3.6 mEq/L, Glucose: 80 mg/dL. Aspartate aminotransferase: 50 U/L Alanine aminotransferase: 43 U/L Alkaline phosphatase: 138 U/L Total protein: 6.4 g/dL, Albumin: 3.8 g/dL, Total bilirubin: 1.1 mg/dL. Imaging demonstrates a spider web of collateral veins in the liver. Although extensive measures are taken, the patient dies 6 hours after arriving. Which of the following was the most likely initial treatment?
β-Blocker followed by lactulose
Cholecystectomy
Endoscopic retrograde cholangiopancreatography with dilation of the common bile duct
Exploratory laparotomy
Tissue plasminogen activator followed by anticoagulation
58) A 67-year-old woman with a history of hypertension and congestive heart failure presents with “burning” epigastric pain that began 2 hours after eating a meal. She states that she has had similar pain over the past several weeks, and has been taking antacids and a medication that her primary care physician had prescribed with moderate relief. The pain has occurred with increasing frequency and now awakens her from sleep. She states she came to the ED today because the pain was not relieved with her usual medications. She denies nausea, vomiting, diarrhea, or fever. She also denies hematemesis, black stool, or bright red blood per rectum. On physical examination, she is tender at the epigastrium, with an otherwise normal abdominal, pulmonary, and heart examination. Stool guaiac tests positive for occult blood. Which of the following is the most common serious complication of peptic ulcer disease?
. GI haemorrhage
. GI perforation
. GI penetration
. Gastric outlet obstruction
. Pernicious anemia
59) A 70-year-old man with a history of constipation has been experiencing intermittent left-sided abdominal pain and fevers for 2 days. He came to the emergency department immediately after he noticed blood in his toilet this morning. His heart rate is 110/min, blood pressure is 90/50 mm Hg, respiratory rate is 18/ min, and oxygen saturation is 95% on room air. On physical examination the physician notes copious amounts of bright red blood per rectum. The physician immediately places two large bore intravenous lines, administers fluid, and sends blood for type and screen. Which of the following is the best next step in management?
Arteriography
Colonoscopy
Endoscopy
Nasogastric tube aspiration
Surgical consultation
60) A 75-year-old woman with a history of diabetes and coronary heart failure presents to the emergency department because of increasing abdominal girth. In recent months she has been feeling increasingly fatigued, and although she has had decreased appetite, she has gained weight. Her heart rate is 100/min and blood pressure is 112/70 mm Hg. She has scleral icterus; the skin over her face, neck, and lower legs is slightly bronze in color; she has palmar erythema; and she has numerous ecchymoses over her body. Her abdominal examination is significant for ascites. Laboratory tests show: Aspartate transaminase: 102 U/L, Alanine transaminase: 97 U/L, Alkaline phosphatase: 300 U/L, Total bilirubin: 1.9 mg/dL, Albumin: 2.9 g/dL, Prothrombin time: 22 sec, Partial thromboplastin time: 42 sec. An ultrasound of her abdomen shows a shrunken and nodular liver. A liver biopsy using Perls Prussian blue stain is shown in the image. Which of the following is the most likely complication of her disease?
Acute pancreatitis
Amyloidosis
Bone marrow failure
Hepatocellular carcinoma
Splenomegaly
61) A 62-year-old woman with a history of diabetes mellitus presents to the emergency department complaining of severe abdominal pain for the past 12 hours, first beginning as dull pain near the umbilicus but now localized to the right lower quadrant. She initially thought she was suffering from heartburn, but decided to come to the hospital because of the unrelenting pain. The patient reports that just prior to examination by the physician, she experienced a sudden decrease in intensity of pain, but she remains feeling very uncomfortable and must remain on the stretcher. On examination the patient appears in distress secondary to pain, tachycardic, slightly hypotensive, and febrile at 39°C (102°F). She has a diffusely tender abdomen with point tenderness over her right lower quadrant, accompanied by guarding and rebound. Laboratory values showed a leukocytosis of 20,000/mm³ with 95% polymorphonuclear lymphocytes. After confirming the diagnosis with imaging, which of the following is the most appropriate management?
Emergent appendectomy and postoperative antibiotics
Give nothing by mouth with intravenous hydration
Percutaneous drainage and interval appendectomy
Serial abdominal examinations
Urgent ECG and cardiac enzymes
62) A 47-year-old woman presents to the emergency department with an 8-day history of left lower quadrant pain and semi-formed stools. Starting this afternoon, she has noticed blood in her stool as well as dizziness when she gets up from sitting. She denies fever, nausea, vomiting, weight loss, and night sweats. Her temperature is 37°C (98.6°F), heart rate is 104/ min, blood pressure is 120/82 mm Hg supine and 103/63 mm Hg when she sits up, and respiratory rate is 18/min. Physical examination reveals no peritoneal signs and is remarkable only for fecal occult blood on rectal examination. Laboratory results reveal a WBC count of 13,000/mm³ and hematocrit of 29%. Results of an x-ray of the abdomen are shown in the image. What is the best next step in management?

Image

Angiography with embolization
Immediate surgery for partial colectomy
Intravenous hydration and blood transfusion
Nothing by mouth, nasogastric tube, and broad-spectrum antibiotics
Place the patient on a high-fiber diet
63) A 57-year-old woman presents to the ED with a basin in her hand and actively vomiting. You insert an IV catheter, start IV fluids, and administer an antiemetic agent. The patient feels much better but also complains of severe crampy abdominal pain that comes in waves. You examine her abdomen and note that it is distended and that there is a small midline scar in the lower abdomen. Upon auscultation, you hear high-pitched noises that sound like “tinkles.” Palpation elicits pain in all four quadrants but no rebound tenderness. She is guaiac negative. Which of the following is the most common cause of this patient’s presentation?
. Travel to Mexico
. Ethanol abuse
. Hysterectomy
. Hernia
. Constipation
64) A 48-year-old woman comes to the office because her regular screening mammogram revealed irregular densities. Radiographic-guided needle biopsy shows evidence of invasive lobular carcinoma. The tumor is hormone receptor positive (HR +). Further investigation reveals involvement of the axillary lymph nodes; the other breast seems to be spared. No distant metastasis is detected. She undergoes modified radical mastectomy, along with radiotherapy. She is then prescribed adjuvant chemotherapy and tamoxifen for 5 years. This patient's use of tamoxifen increases her risk for developing which of the following cancers:
. Ovarian cancer
. Endometrial cancer
. Lung cancer
. Pancreatic cancer
. Cervical cancer
65) A 54-year-old Caucasian woman presents to your office with fatigue. She also reports dizziness and palpitations after moderate physical activity. Additionally, her feet feel "numb" and are less sensitive to cold than they used to be. She has no significant past medical history. Physical examination reveals pale conjunctivae and a shiny tongue. Ankle reflex is decreased bilaterally. Laboratory findings include: Hemoglobin 7.6 mg/dL, MCV 110 fL, MCHC 36 g/dL, WBC count 3,900/mm3, Platelet count 150,000/mm3. This patient should be monitored for which of the following long-term complications?
. Acute myelogenous leukemia
. Hodgkin's disease
. Celiac sprue
. Gastric cancer
. Liver cirrhosis
66) A 34-year-old male is brought to the emergency room after being involved in a motor vehicle accident. He suffers blunt abdominal trauma and bilateral femur fractures. He has no significant past medical history. On physical examination, his blood pressure is 80/40 mmHg and his heart rate is 110/min. He receives several units of packed red blood cells. Once stabilized, the patient begins complaining of a tingling sensation in his toes and fingers. His serum calcium level is noted to be 7.2 mg/dL. Which of the following is the most likely cause of this patient's current symptoms?
. Increased renal tubular secretion of calcium
. Calcium chelation by a substance in the transfused blood
. Electrolyte leakage from red blood cells during pre-transfusion storage
. Antibody-mediated red blood cell membrane damage
. Parathyroid gland suppression due to fluid overload
67) An 81-year-old man is brought to the hospital due to complaints of very severe pain in his back and thighs. Seven months ago, he was diagnosed with stage IV prostate cancer which reached the spine. He has had palliative radiotherapy of his spine, and is now taking leuprolide. He is restless and very irritable, even after the nursing home staff gave him ibuprofen. He has never received any narcotics. What is the best next step in this patient's pain management?
. Give high dose NSAIDs
. T ransdermal fentanyl patch
. Start with short-acting morphine
. Long-acting opiates
. Repeat radiotherapy
68) A 45-year-old previously healthy male is brought to the emergency room because of headaches and confusion for 2 days. He denies any focal weakness or sensory symptoms. He has no significant past medical history and does not use any medications. He does not use tobacco, alcohol or drugs. On physical exam, the patient has a temperature of 37.9°C (100.2°F), a blood pressure of 140/86 mm Hg, a pulse of 96/min, and respirations of 16/min. Mild icterus is present. The patient's oropharynx is clear and his neck is supple and without rigidity. Examination of the patient's chest and abdomen is unremarkable. Neurologic examination reveals no focal deficits. Laboratory studies show: Complete blood count: Hemoglobin 84 g/L, Platelet count 80,000/mm3, Leukocyte count 5,500/mm3. Chemistry panel:Blood urea nitrogen (BUN) 30 mg/dL, Serum creatinine 2.2 mg/dL, Serum calcium 10.0 mg/dL, Blood glucose 98 mg/dL. A peripheral blood smear shows many fragmented red blood cells. The prothrombin time is normal. Which of the following is the most appropriate next step in the management of this patient?
. Hemodialysis
. MRI of the brain
. Electroencephalogram
. Plasma exchange
. Platelet transfusion
69) A 54-year-old male comes to the emergency department with complaints of cough and bloody sputum. He used to smoke 2 packs of cigarettes daily for 22 years, but states that he quit last month. He also complains of weight loss, anorexia, constipation, increased thirst, and easy fatigability, which he attributes to depression. He lost his wife 4 months ago and "life never felt the same after that." He is sure that he cannot have cancer because he does not smoke anymore. His vital signs are stable. He appears slim, pale, slightly irritable, and short of breath. The laboratory studies and chest x-ray results are as follows: Sodium 144 mEq/dL, Potassium 4.3 mEq/dL, Chloride 98 mEq/dL, Bicarbonate 21 mEq/dL, Calcium 14.5 mg/dl, BUN 48 mg/dl, Creatinine 2.0 mg/dl, Chest x-ray hilar mass in the left lung. While in the ED, he becomes more somnolent and vomits twice. What is the best next step in the management of this patient?
. IV furosemide
. CT scan of the head
. IV normal saline
. Emergency hemodialysis
. IV pamidronate
70) A 75-year-old Caucasian male who was diagnosed with carcinoma of the prostate presents to ER with worsening back pain for the past 2-3 days. He never had this pain before. He denies any weakness of the legs. On examination, his muscle power in the lower extremities is 4.5/5 and has brisk reflexes. Rectal sphincter tone is weak. He has point tenderness over the L5 and S1 region. His vital signs are, BP: 122/80 mm Hg, PR 80/min, RR 16/min and Temperature 37°C (98°F). What is the most appropriate next step in management of this patient?
. Radiotherapy.
. Intravenous dexamethasone.
. Immediate MRI of spine
. Decompression surgery of spine.
. CT myelogram.
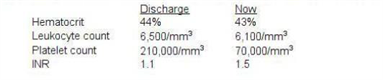
71) A 55-year-old woman complains of right leg swelling and tenderness following an international flight. A venous scan of the right lower extremity showed thrombosis of the right popliteal vein. She is sent home with oral warfarin and subcutaneous enoxaparin. One week later, she returns to the office for a follow-up appointment. Laboratory studies at the time of discharge and now are shown below: This patient's current condition predisposes her to which of the following?
Image

. Acute interstitial nephritis
. Arterial thrombosis
. Hemarthrosis
. Pneumothorax
. Fat embolism
72) A 22-year-old African American male suffering from sickle cell anemia presents in the emergency department with a sustained painful penile erection for the last 4 hours. Previously, he had one episode of acute chest syndrome that was treated with oxygenation, hydration and blood transfusion. His pulse is 76/min, respirations are 16/min, blood pressure is 115/76 mm Hg, and temperature is 37°C (98.6°F). Examination of all his systems is unrevealing. What is the best next step in the management of this patient?
. Observation
. Hyperbaric oxygen therapy
. Exchange transfusion
. Surgical intervention
. Hydroxyurea
73) A 65-year-old man presents to the emergency department with a two-day history of fever, headache, altered mental status, and vomiting. His past medical history is significant for renal transplantation secondary to polycystic kidney disease, hypertension, and diabetes. He takes aspirin, insulin, nifedipine, cyclosporine, and prednisone. He has no known drug allergies. His temperature is 39.2°C (102.5°F), pulse is 102/min, respirations are 18/min, and blood pressure is 120/75 mm Hg. He is alert but confused. Fundoscopy does not show any abnormalities. His neck is stiff. Lungs are clear to auscultation. He has a normal S1 and S2 with a II/IV systolic ejection murmur heard best in the right infraclavicular area. Complete blood count shows a WBC count of 17,000/cm3 with neutrophilic leukocytosis. His blood is drawn and sent for culture. Lumbar puncture is performed and the results are pending. Which of the following is the most appropriate empiric antibiotic therapy for this patient?
. Ceftriaxone
. Ceftriaxone and vancomycin
. Cefotaxime and ampicillin
. Ceftriaxone, vancomycin, and ampicillin
. Ceftazidime and vancomycin
74) A 7-year-old Caucasian boy with a history of cystic fibrosis presents to the emergency department with a two-day history of high-grade fever and cough productive of purulent, green-colored sputum. He also complains of chest pain, which is worsened by breathing. His temperature is 39.6°C (103.2°F), pulse is 112/min, respirations are 26/min, and blood pressure is 90/60 mm Hg. Chest examination shows dullness on percussion and increased tactile fremitus in the right lung base. Chest x-ray shows a right lower lobe infiltrate. Which of the following is the most appropriate pharmacotherapy for this patient?
. Ceftriaxone and gentamicin
. Azithromycin
. Piperacillin and tobramycin
. Piperacillin and ciprofloxacin
. Dicloxacillin
75) A 28-year-old man presents to ER with fever, chills, and generalized weakness for the past one week. He has no history of pre-existing heart disease, but he was admitted to the hospital six months ago for cellulitis of the right arm. His temperature is 40.0°C (104°F), pulse is 110/min, respirations are 22/min, and blood pressure is 110/65 mmHg. Oropharynx is clear. Lungs are clear to auscultation. A holosystolic murmur is heard at the lower sternum which increases in intensity with inspiration. His blood is drawn and sent for culture. What is the most appropriate initial antibiotic therapy for this patient?
. Ampicillin-sulbactam
. Clindamycin
. Oxacillin
. Penicillin G and gentamycin
. Vancomycin
76) A 45-year-old female presents to emergency room complaining of urinary frequency, burning during urination, and weakness. Her last menstrual period was one year ago, and she is not sexually active. She is not taking any medications. Her temperature is 37.8°C (100°F), blood pressure is 120/76 mmHg, pulse is 80/min, and respirations are 14/min. Very mild costovertebral angle tenderness is present. IV ceftriaxone is started. Two days later, the patient feels much better. Antibiotic susceptibility testing returned with an uropathogen (E.coli) highly sensitive to ceftriaxone, gentamicin, ciprofloxacin and trimethoprim/sulfamethoxazole (TMP/SMX). Which of the following is the most reasonable next step in the management of this patient?
. Add ciprofloxacin to the regimen
. Switch to TMP/SMX
. Switch to gentamicin
. Continue ceftriaxone
. Discontinue antibiotic therapy
77) A 65-year-old man presents to the emergency department with a two-day history of fever, headache, altered mental status, and vomiting. His past medical history is significant for renal transplantation secondary to polycystic kidney disease, hypertension, and diabetes. He takes aspirin insulin, nifedipine, cyclosporine, and prednisone. He has no known drug allergies. His temperature is 39.2°C (102.5°F), pulse is 102/min, respirations are 18/min, and blood pressure is 120/75 mm Hg. He is alert but confused. Fundoscopy does not show any abnormalities. His neck is stiff. Lungs are clear to auscultation. He has a normal S1 and S2 with a II/IV systolic ejection murmur heard best in the right infraclavicular area. Complete blood count shows a WBC count of 17,000/cm3 with neutrophilic leukocytosis. His blood is drawn and sent for culture. Lumbar puncture is performed and the results are pending. Which of the following is the most appropriate empiric antibiotic therapy for this patient?,
. Ceftriaxone
. Ceftriaxone and vancomycin
. Cefotaxime and ampicillin
. Ceftriaxone, vancomycin. And ampicillin
. Ceftazidime and vancomycin
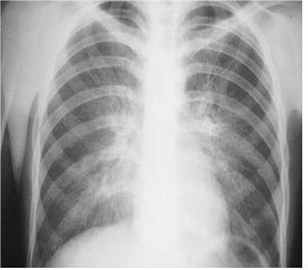
78) A 29-year-old male, known intravenous drug user presents to the emergency department with a chief complaint of dyspnea. Over the last few days, he has become short of breath and he has very little exercise tolerance. His other symptoms are a persistent dry cough, low-grade fever for the past two days, watery diarrhea, abdominal cramps, and general malaise. He self-treated his fever with acetaminophen. He has a history of anaphylaxis with sulfonamides. Physical examination reveals an emaciated man with numerous needle marks on his hands. Arterial blood gas analysis reveals a PCO2 of 32 mm Hg and PO2 of 64 mm Hg on room air. The chest x-ray is shown below. Which of the following is the most appropriate initial treatment regimen for this patient?
Image

. Penicillin and acyclovir
. Pentamidine and azithromycin
. Tetracycline and azithromycin
. Acyclovir and azithromycin
. Ganciclovir and azithromycin
79) A 54-year-old diabetic woman comes to the emergency department because of increasing neck and facial pain, fever, and chills. A few weeks ago, she developed an infection on the side of her neck. She thought it would go away with over-the-counter medication, but the infection has now started to drain. For the past twenty years, she has had diabetes, which is well-controlled with an oral hypoglycemic. She denies trauma, travel, and smoking. Physical examination reveals an area of erythema and induration at the base of the neck. Serosanguineous fluid is draining from a small defect in the skin near the center of the lesion. There is no crepitus. Histological analysis of the discharge reveals the presence of gram positive, branching bacteria. The treatment for this patient is?
. Surgical debridement
. Start triple combination TB therapy
. Start amphotericin
. Hyperbaric oxygenation
. Intravenous penicillin
80) A 72-year-old man presents to the ED during the month of January complaining of non-productive cough, fever, malaise, runny nose, and severe body aches. The symptoms came on suddenly last night. He has no other medical problems. Physical examination reveals a temperature of 38.9°C (102.0°F) and oxygen saturation of 88% on room air. His lung exam reveals diffuse crackles with occasional wheezes. Laboratory values are: Hematocrit 44%, Platelets 219,000/mm3, Leukocyte count 4,100/mm3, Neutrophils 65%, Lymphocytes 32%. His chest x-ray reveals diffuse interstitial infiltrates bilaterally. What is the most appropriate initial therapy for this patient?
. Ganciclovir
. Tenofovir
. Oseltamivir
. Valacyclovir
. Nevirapine
{"name":"Med emergency 2 Q1 to Q 80", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"1) An 81-year-old diabetic woman with a history of atrial fibrillation is transferred to your emergency department (ED) from the local nursing home. The note from the facility states that the patient is complaining of abdominal pain, having already vomited once. Her vital signs in the ED are temperature 100.1°F, blood pressure (BP) 105\/75 mmHg, heart rate (HR) 95 beats per minute, and respiratory rate (RR) 18 breaths per minute. You examine the patient and focus on her abdomen. Considering that the patient has not stopped moaning in pain since arriving to the ED, you are surprised to find that her abdomen is soft on palpation. You decide to order an abdominal radiographic series. Which of the findings on plain abdominal film is strongly suggestive of mesenteric infarction?, 2) A husband and wife present to the ED with 1 day of subjective fever, vomiting, watery diarrhea, and abdominal cramps. They were at a restaurant a day before for dinner and both ate the seafood special, which consisted of raw shellfish. In the ED, they are both tachycardic with temperatures of 99.8°F and 99.6°F for him and her, respectively. Which of the following is responsible for the majority of acute episodes of diarrhea?, . Parasites . Viruses . Enterotoxin-producing bacteria . Anaerobic bacteria . Invasive bacteria","img":"https://www.quiz-maker.com/3012/images/ogquiz.png"}