
Hematology& Oncology ( USMLE)

USMLE Hematology & Oncology Quiz
Test your knowledge and understanding of hematology and oncology with our comprehensive quiz designed specially for USMLE candidates. This quiz covers a range of clinical scenarios and intricate details that challenge your diagnostic and management skills.
Enhance your learning and prepare for your exams with:
- 30 carefully crafted questions
- Real-world clinical cases
- Immediate feedback on your answers
1. A 58-year-old nurse with node-positive metastatic breast cancer comes to the office for her monthly follow-up visit. The tumor is estrogen receptor (ER) and progesterone receptor (PR) positive, and her whole body bone scan is positive for metastatic disease. She is being treated with systemic chemotherapy and hormonal therapy (Tamoxifen). She feels weak with vague muscle, joint, and bone pains. Physical examination reveals a hard, well-defined dominant mass in the left breast. Mucus membranes are moist. Laboratory studies show the following results. Sodium 145 mEq/dL Potassium 3.9 mEq/dL Chloride 103 mEq/dL Bicarbonate 24 mEq/dL Calcium 11.3 mg/dl BUN 18 mg/dl Creatinine 0.8 mg/dl Glucose 146 mg/dl Which of the following is the best next step in the management of her hypercalcemia?
A. Corticosteroid therapy
B. Zoledronic acid therapy
C. Intravenous normal saline
D. Furosemide therapy
D. Furosemide therapy
2. A 55-year-old male comes to you with complaint of fatigue for the past month. He also complains of occasional heartburn. His past medical history is significant for hepatomegaly, secondary to fatty liver. He has been drinking 3-4 shots of alcohol per day for the past 30 years. He denies smoking. His physical examination reveals pallor of skin and mucous membranes, and mild hepatomegaly. His laboratory report shows: Hb 8.5 g/dl WBC 8,000/cmm MCV 110 fl Platelets 150,000/cmm Blood glucose 118 mg/dl BUN 16 mg/dl Serum creatinine 1.0 mg/dl What is the most likely cause of anemia in this patient?
A Vitamin B- 12 deficiency
E. Thiamine deficiency
D. Anemia of chronic disease
C. Chronic blood loss from peptic ulcer
B. Folate deficiency
3. A 62-year-old Caucasian man presents to your office with occasional ear pain and a lump in his neck. His past medical history is significant for hypertension treated with hydrochlorothiazide and diabetes mellitus treated with metformin. He smokes two packs of cigarettes per day and consumes alcohol occasionally. He is not sexually active. Physical examination reveals a hard, non-tender submandibular mass that is 3 cm in diameter. Chest examination is unremarkable. Abdomen is soft and non-tender. The liver span is 8 cm and the spleen is not palpable. His extremities have no cyanosis, clubbing, or edema. Complete blood count is within normal limits. Which of the following is the most likely cause of this patient's complaint?
A. Bacterial infection
E. Hodgkin's lymphoma
D. Connective tissue disease
C. Herpes simplex infection
B. Squamous cell carcinoma
4. A 50-year-old man wants to talk to you about something, "absolutely confidential". After you assure him, he admits, "He is unable to get an erection and just can't have sex." He wants to figure it out quickly because "he simply can't live like this." He has never been diagnosed with diabetes and denies other complaints. He has a 2 pack/day history of smoking for 30 years. On examination, his BP: 158/90mm of Hg; Temperature: 37.1 C (98.8F); RR 14/min; PR 82/min. There is upper body obesity, rounded face, increased fat around the neck, and thinning of arms and legs. You find his skin to be bruised, fragile and thin. Laboratory reveals the following results. Serum: Glucose 186 mg/dl Sodium 142 mEq/L Potassium 2.5 mEq/L Chloride 94 mEq/L Bicarbonate 38 mEq/L Chest-X ray shows a large mass in left bronchus. What is the most likely cause of patient's condition?
A Pituitary adenoma
E. Exogenous steroid intake
D. Familial cushing's syndrome
C. Ectopic ACTH syndrome
B. Adrenal tumors
5. Her son brings a 50-year-old female to the emergency room because she is confused and sweating a lot. She does not have any medical problems, except hypertension for which she takes hydrochlorothiazide. She is not taking any other medication. He tells you that his mother complained of profound weakness, and inability to stand, because of lightheadedness 3 hours ago. On examination, the patient is drowsy, confused, and appears sick. Her temperature 36.8C (98.2F) BP 153/83mm Hg PR 128/min. Her clothes are damp from perspiration. No other abnormalities are noted on physical examination. Initial laboratory studies show: Sodium 144 mEq/L Potassium 3.6 mEq/L Bicarbonate 26 mEq/L Blood urea nitrogen: 12 mg/dl Creatinine 0.6 mg/dl You order a few more tests and on the basis of which you diagnose insulinoma. What set of following results leads to this diagnosis? Serum Glucose, Insulin, C-Protein
A. Increased, Decreased, Increased
E. Normal,Normal,Normal
D. Decreased, Increased, Decreased
C. Decreased, Increased, Increased
B. Increased, Increased, Increased
6. A 67-year-old woman comes to her physician because she is feeling tired, all the time. She thinks that it is due to multiple surgeries she had over the past several years. She had two caesarian sections at the age of 22 and 26. She also had a thyroid surgery for Graves’s disease, 30 years ago. 12 years ago she was diagnosed with colon cancer and had undergone left hemicolectomy. She denies smoking or alcohol use. Her vitals are Temperature 36.7C (98.2F); BP 138/86 mm Hg; PR 77/min; RR 12/min. She looks markedly pale and has weakness in all four extremities. There is some sensory loss in lower limbs. The test for occult blood was negative. Labs came back as: Sodium 144 mEq/L Potassium 4.2 mEq/L Bicarbonate 24mEq/L Blood urea nitrogen 18mg/dl Creatinine 1.0 mg/dl Glucose 82 mg/dl WBC 8,600/cmm Hemoglobin 7.9 Hematocrit 25%, Platelets 176,000/cmm The physician decides to further investigate anemia and order RBC indices and peripheral blood smear. The results are: MCV 120 fl MCH 36 pg MCHC 28% Reticulocyte count 04% Peripheral smear showed anisocytosis, poikilocytosis, 4+ macrocytes, polychromatophilia and basophilic stippling. A whole new bunch of tests are ordered and the following report is seen on the computer. Vitamin B 12 1 06 pg/ml (N=210-911 pg/ml) Serum Folate 16.4 ng/ml (N=2.8-17.8 ng/ml) Serum Bilirubin 1 .8 mg/dl Serum LDH 2500 U/L Gastric analysis demonstrated an absence of hydrochloric acid. What is the most probable cause of her anemia?
A. Folate deficiency
E. Malabsorption syndrome
D. Hemicolectomy
C. Pernicious anemia
B. Dietary B 12 deficiency
7. A 34-year-old Caucasian man presents to your office with easy fatigability, difficulty concentrating, insomnia, and occasional muscle pain. He also complains of right hand clumsiness and some memory loss. He does not smoke and drinks one to two cans of beer on the weekends. Physical examination reveals extensor weakness of the right hand. Ankle reflexes are symmetric and there is no Babinski reflex. Laboratory studies show: Hemoglobin 8.5 g/dl MCV 81 fl AST 18 U/L ALT 16 U/L Bilirubin 0.8 mg/dl Creatinine 2.1 mg/dl Which of the following is most important in revealing the cause of this patient's condition?
A. Vaccination history
E. Childhood infections
D. Nutrition
C. Occupational history
B. Family history
8. You are called to the oncology floor to examine a 57-year-old female who is complaining of severe nausea and vomiting. Her other symptoms include some general malaise and a sore throat. She is receiving combination ABVD chemotherapy (Doxorubicin, Bleomycin, Prednisone, and Procarbazine). She was diagnosed with stage II Hodgkin's lymphoma 4 weeks ago. She tells you that she does not want to continue her therapy anymore since it is "making life even more miserable." She has lost 30 lbs (12 .6kg) in a month. Her temperature is 38.5C (101.3F), pulse is 88/min, respirations are 18/min, and blood pressure is 109/68mm Hg. Her pulse oximetry reading in room air is 92%. Physical examination reveals a significantly cachectic patient with a dry mouth, enlarged cervical lymph nodes and hepatomegaly. How can this patient's vomiting be best managed?
A. Stop the chemotherapy drugs
E. Prochlorpera zine
D. Tell the patient that her nausea will get better with time
C. Metoclopramide
B. Ondansetron
9. A 65-year-old male is brought by his wife to the emergency department because of a very high fever. He has also had a cough productive of greenish, nonbloody sputum for the past two days. He is diabetic, and had pneumonia 3 months ago. He has been smoking one pack of cigarettes daily for 27 years. His temperature is 38.4 C(101.2F), blood pressure is 118/74 mm Hg, pulse is 98/min, and respirations are 24/min. Physical examination reveals cervical lymphadenopathy, and some scattered rales are heard on the right lung base. Chest-x ray shows a right lower lobe infiltrate. Laboratory studies reveal: Hb 12.6 gm/dL WBC 40,000/cmm Platelets 190,000/cmm Peripheral smear: Segmented neutrophils 10% Bands 4% Lymphocytes 85% Monocytes 1% Some variant lymphocytes, and smudge cells are seen on the peripheral smear. What is the most appropriate way to confirm the diagnosis of this patient?
A. Epstein Barr virus serology
E. Lung biopsy
D. Cytogenetic analysis
C. Lymph node biopsy
B. Bone marrow biopsy
10. A 26-year-old woman presents to your office complaining of fatigue. Her past medical history is insignificant. She was adopted in Greece and came to the United States when she was three years old. Her menstrual periods are regular and bleeding lasts three days. She does not use tobacco, alcohol, or illicit drugs. She takes no medication. Laboratory studies show: Complete blood count: Hemoglobin 10.1 g/L MCHC 28% MCV 70 fL Platelets 200,000/mm3 Leukocyte count 7,500/mm3 Neutrophils 56% Eosinophils 1% Lymphocytes 33% Monocytes 10% Fecal occult blood test is negative. Iron therapy is initiated. When the patient returns four weeks later, her lab findings are essentially the same. This patient most likely suffers from:
A. Iron deficiency
E. Hemoglobinopathy
D. Erythropoietin deficiency
C. Cobalamin deficiency
B. Folic acid deficiency
11. An 8-month-old pale child is referred by a nurse practitioner due to "pale mucous membranes, irritability, and listlessness." The stool examination is negative for occult blood, ova and parasites. Laboratory studies reveal: Hemoglobin 6.0 g/L MCHC 25% MCH 16.5 pg MCV 68 fl Reticulocytes 0.6% Platelets 230,000/mm3 Leukocyte count 5,500/mm3 Neutrophils 56% Eosinophils 1% Lymphocytes 33% Monocytes 10% Serum Iron 40 mg/dL TIBC 460 mg/dL (normal 300-350 mg/dL) Percent saturation of transferrin 8.7% Total serum bilirubin 0.9 mg/dL The peripheral blood smear shows marked anisocytosis, microcytosis, hypochromia, and poikilocytosis. Which of the following is the most likely diagnosis?
A. Iron deficiency anemia
E. Anemia of chronic disease
D. Megaloblastic anemia
C. Dimorphic anemia
B. Sideroblastic anemia
12. A 54-year-old Caucasian man presents to his family physician's office complaining of several months of increased fatigability. He eats meat occasionally and drinks two to three cans of beer on weekends. Physical examination reveals pale conjunctivae and hyperdynamic carotid pulses. His blood hemoglobin level is 7.7 mg/dl, WBC count is 4,500/mm3, and platelet count is 170,000/mm3 Folic acid therapy is initiated. Four weeks later the patient's hemoglobin level is 9.1 mg/dl, but he complains of new tingling in his toes. Which of the following is a likely cause of this patient's current symptoms?
A. Drug toxicity
C. Vitamin deficiency
B. Iron deficiency
D.Glucose intolerance
E. Extramedullary hematopoiesis
13. An 80-year-old man with advanced prostate cancer and bony metastasis is complaining of severe back pain that has been progressively worsening for the past two weeks. His pain is so severe that it restricts him from playing golf. Eight months ago, he underwent orchiectomy, after which he was free from bone pain until now. Physical examination reveals tenderness at two sites in the lumbar region. Radionuclide bone scan shows an increased uptake in these areas. Which of the following is the most appropriate next step in the management of this patient?
A. Cervical cordotomy
E. Radiation therapy
D. Hypophysectomy
C. Flutamide therapy
B. Etidronate disodium therapy
14. A 46-year-old bank executive is referred to the clinic by her dentist. For the past 6 weeks, she has had swollen, bleeding gums. She appears pale and feels weak. She smokes half a pack of cigarettes daily and drinks alcohol socially. Her family history is not significant. Her vital signs are stable. She is afebrile. WBC 44,100 mm3 Hemoglobin 9.0 g/dL Hematocrit 27% Platelets 16,000/mm3 Leukocyte distribution: Blast forms 79% Promonocytes 12% Monocytes 8% Lymphocytes 1% Cytochemical analysis: Sudan black: slightly positive Alpha-naphthyl esterase: positive PAS reaction: negative Which of the following is the most likely diagnosis?
A. AML with maturation
E. Acute monocytic leukemia
D. Acute erythroleukemia
C. Acute lymphoblastic leukemia
B. Acute promyelocytic leukemia
15. A 65-year-old woman is being evaluated for "generalized depression." She has felt weak and fatigued ever since her husband died 4 months ago. She does not have any suicidal thoughts, but is losing interest in her daily activities. She quit smoking 24 years ago, and drinks 1-2 beers weekly. Physical examination reveals pallor and cervical lymphadenopathy. Blood work reveals: Hemoglobin 12.0 g/L MCV 85 fl Platelets 224,000/mm3 Leukocyte count 54,500/mm3 Neutrophils 16% Lymphocytes 75% Monocytes 9% Some variants of lymphocytes and smudge cells are present. Which of the following is the most likely diagnosis?
A Lymphoblastic leukemia
E. Hairy cell leukemia
D. Chronic myeloid leukemia
C. Chronic lymphocytic leukemia
B. Hodgkin's disease
16. A 66-year old female has been your patient for the last 8 years. She was diagnosed with colorectal carcinoma 2 years ago, and eventually underwent an endoscopic resection. Since then, she has been healthy, and has been coming to the office regularly for follow-up visits. She is very grateful, and has stated many times that she owes her life to you. You are currently a co-investigator of a retrospective observational study of patients with colon cancer, and you believe that including her medical information will be extremely beneficial. What course of action must you take so that you can include this patient's data in your study?
A. Include the data, as she has been your patient for so many years.
E. Include the data only after taking informed consent.
D. Have the data de-identified by a colleague, then include it in the study.
C. Call her and obtain verbal consent to include her data.
B. Include the data and inform her whenever she comes next time.
17. A 65-year-old Hispanic male is brought to the emergency department after having one seizure episode. His past medical history is significant for non-small cell lung carcinoma, which was diagnosed two years ago and treated surgically. He had no residual disease at that time. CT scan of the brain with contrast now shows a solitary cortical mass in the right hemisphere of the brain at the grey-white matter junction. His chest x-ray is clear. He is admitted for further management and started on phenytoin. Which of the following is the most appropriate management for this patient?
A. Focal radiation to brain mass
E. Palliative pain therapy and seizure prophylaxis
D. Combination chemotherapy
C. Surgical resection of the mass
B. Whole brain radiation
18. A 54-year-old male is brought to the emergency department because of severe abdominal pain and diarrhea for the past 24 hours. He is confused and crying out in pain. His temperature is 38.6C (101.6F), blood pressure is 82/58 mm Hg, pulse is 118/min, and respirations are 24/min. Physical examination reveals extensive abdominal distention. There is fresh blood in his stools. Intravenous administration of normal saline is started after drawing blood for the necessary laboratory tests. The results of these tests are: Sodium 136 mEq/L Potassium 3.6 mEq/L Bicarbonate 18 mEq/L Blood urea nitrogen 32 mg/dL Creatinine 1.3 mg/dL Glucose 86 mg/dL WBC 35,000mm3 Hemoglobin 13.0 g/dL Hematocrit 36% Platelets 460,000mm3 Leukocyte distribution: Promyelocyte 2% Myelocytes 7% Metamyelocytes 18% Bands 32% Segmented neutrophils 24% Lymphocytes 15% The patient's temperature continues to remain elevated during the night of admission. A broad-spectrum antibiotic is added to the IV infusion. Repeat CBC on the following morning shows a WBC count of 118,000/mm3 with essentially the same differential distribution of leukocytes. His leukocyte alkaline phosphatase score is elevated. What is the most probable diagnosis of this patient?
A CML with blast crisis
E. Myelodysplastic syndrome
D. Secondary polycythemia
C. Leukemoid reaction
B. Chronic lymphocytic leukemia
19. A 65-year-old woman comes to the office for a health maintenance visit. She has been your patient for the last 15 years. When you ask how she has been, she replies with, "Well, I'm very health-conscious now. I read all the health magazines regularly, and exercise for 30 minutes daily. I eat a lot of garlic to control my cholesterol, and drink cranberry juice to keep my kidneys strong. I don't smoke, but I drink alcohol during social events. I've been compliant with regular screening colonoscopies, mammograms, and pap smears. Doc, since my mother died from ovarian cancer, do you think I can have an abdominal ultrasound every 6 months, plus any additional necessary tests, so that any cancer can be detected early?" What is the best response to this patient's concerns?
E. Reassure her that with a healthy lifestyle, cancer is unlikely.
D. Perform an ultrasound every six months since it is a non-invasive procedure that can save you from any risk of being sued for malpractice.
C. Abdomen ultrasound is not effective for detecting ovarian cancer early, but CXR surveillance has helped decrease the mortality of lung cancer.
B. CXR, EGO, and abdominal ultrasound can be done to help detect cancers early.
A. There is no evidence that ultrasound surveillance has any role in decreasing mortality from ovarian cancer.
20. A 22-year-old African-American man presents to the ER with fever, jaundice, abdominal pain, and dark urine. His heart rate is 100/min and blood pressure is 100/60. Peripheral blood smear reveals bite cells and red blood cell inclusions seen after crystal violet staining. The patient most likely suffers from which of the following conditions?
A. Acute viral hepatitis
E. Sickle cell trait
D. Thalassemia minor
C. Enzyme deficiency
B. Acute glomerulonephritis
21. A 34-year-old male is brought to the emergency department with altered mental status. His girlfriend reports that he has had fever and cough for the past two days. His past medical history is significant for abdominal trauma two years ago that required splenectomy and left-sided nephrectomy. On physical examination, his temperature is 39 C (102.2F), blood pressure is 80/50 mm Hg, pulse is 110/min, and respirations are 32/min. Gram-positive cocci are cultured from his blood. Which of the following is most likely impaired in this patient?
A. Intracellular killing
E. Cell-mediated immunity
D. Chemotaxis
C. Number of circulating lymphocytes
B. Phagocytosis
22. A 35-year-old Caucasian female is hospitalized with swelling and tenderness of her right calf. Deep venous thrombosis is diagnosed through imaging studies, and the appropriate therapy is initiated. Three days later, she complains of right arm pain. Physical examination reveals a cold right upper extremity with no palpable peripheral pulse. Her laboratory values are listed below. Hematocrit 42% WBC count 8,500/mm3 Platelets 76,000/mm3 PT 13 sec aPTT 63 sec Which of the following drugs was most likely used to treat this patient's deep venous thrombosis?
A. Aspirin
E. Warfarin
D. Unfractionated heparin
C. Enoxaparin
B. Danaparoid
23. A 21-year-old previously healthy man presents to your office for a routine check-up. He has no current complaints. He does not smoke or consume alcohol. His family history is significant for cystic fibrosis in his older brother. He is sexually active with one partner and uses condoms regularly. He visits a dentist twice per year. His temperature is 36.6C (97.9F), pulse is 78/min, respirations are 14/min, and blood pressure is 120/76 mmHg. Physical examination reveals several non-tender, rubbery cervical lymph nodes, each measuring approximately 1 cm in diameter. There is no hepatosplenomegaly. Which of the following is the best next step in management of this patient?
A Lymph node biopsy
E. Observation
D. Erythromycin
C. Prednisone
B. Dicloxacillin
24. A 25-year-old African American man presents to your office complaining of nocturia over the past several months. He reports having to wake to urinate 2 to 3 times per night despite restricting his fluid intake. He denies any back pain, fever, dysuria, or urinary urgency. His past medical history is significant for recurrent otitis media in childhood and hepatitis A infection two years ago. He is sexually active with one partner and does not use condoms. His brother died of a "blood disease" at age 10. The man's hematocrit is 49%. Urinalysis reveals no proteinuria or sediment abnormalities. His nocturia is most likely related to:
A. Childhood infections
E. Glomerular pathology
D. Family history
C. Sexual history
B. Nephrolithiasis
25. A 43-year-old man presents to your office with low energy and increased fatigability. He also complains of daytime sleepiness and occasional headaches. He drinks two to three glasses of wine daily but does not smoke. He sleeps in a separate room from his wife because she finds his constant snoring annoying. On physical examination, his blood pressure is 160/100 mmHg and his heart rate is 80/min. His BMI is 31.5 kg/m2. His abdomen is soft and non-tender. The liver span is 10 cm and the spleen is not palpable. Laboratory findings are: Hematocrit 60% WBC count 9,000/mm3 Platelets 190,000/mm3 Which of the following is most likely responsible for this patient's increased hematocrit?
A. Plasma volume contraction
E. Ineffective erythropoiesis
D. Increased erythropoietin production
C. Carboxyhemoglobinemia
B. Clonal proliferation of myeloid cells
26. A 32-year-old Caucasian female presents to your office for a routine check-up. Her past medical history is significant for generalized seizures controlled with chronic phenytoin therapy. The last seizure was six months ago. She does not smoke or consume alcohol. Physical examination is insignificant, except mild pallor. Laboratory values are: Hb 10.8 g/dL MCV 105 fl Platelet count 180,000/cmm Leukocyte count 7,500/cmm Segmented neutrophils 68% Bands 1% Eosinophils 1% Lymphocytes 24% Monocytes 6% Which of the following supplementations could have prevented this patient's anemia?
A. Folic acid
E. Vitamin B1
D. Vitamin B6
C. lron
B. Vitamin B 12
27. A 46-year-old female is brought to the emergency department because of visual blurring and altered mental status. She was recently treated for gout. Physical examination shows moderate to severe splenomegaly and positive sternal tenderness. Laboratory studies reveal a WBC count of 120, 000/uL with left shifted myeloid series and basophilia. Bone marrow exam shows 3% blasts. Repeat CBC is ordered. The hematologist-on-call decides to start leukophereses emergently. What another drug should be given to this patient?
A Cladribine
E. Lmatinib mesylate
D. Interferon alpha
C. Cyclophosphamide
B. Hydroxyurea
28. A father brings his 7-year-old boy to the office because "his eyes are getting yellow". The boy has no other complaints. However, he is feeling tired and does not feel like going to the next Steelers game. There is a history of diabetes and lung cancer in the family. His vitals are stable, but he has pallor, jaundice, and splenomegaly. His labs revel: WBC 10,000cmm Hemoglobin 10 gm/dl Hematocrit 28% RBC count 3.5 million Platelets 240,000cmm Reticulocyte count 4% RBC indices were as follows: MCV 90 fl MCHC 38% MCH 28 pg Peripheral smear revealed anisocytosis, some spherocytosis, and polychromatophilia. Coomb's test was negative. LFTs showed: Albumin 5.2 g/dl AST 47U/L ALT 52U/L Alkaline phosphatase 120 U/L Total bilirubin 3.0 mg/dl Direct bilirubin 0.2 mg/dl What is the next step?
A. Bone marrow biopsy
E. Serum B 12 level
D. Hemoglobin electrophoresis
C. Sugar water test
B. Osmotic fragility test
29. A 25-year-old African American male comes to the office with sudden-onset back pain, dark urine and an one day history of fatigue. Two days ago, he was started on trimethoprim-sulfamethoxazole for his sinusitis. Otherwise, his past medical history is unremarkable. Physical examination reveals significant pallor. His laboratory report shows: Hb 7.5 g/dl Total bilirubin 3.5 mg/dl Direct bilirubin 0.8 mg/dl Haptoglobin decreased LDH increased The peripheral smear shows bite cells. His G6PD level is normal. Which of the following is the most likely cause of his hemolysis?
A. G6PD deficiency
E. Mechanic trauma
D. Sickle cell disease
C. Galactokinase deficiency
B. Pyruvate kinase deficiency
30. A 50-year-old pale man comes to the office and says, "For the past year, I've been feeling very weak. I get tired early, and I feel that I've lost my sense of humor. I find it difficult to remember things now." When asked about his social history, he says, "I'm jobless and am living on social security benefits. I don't drink or smoke anymore, but I was charged with driving under the influence three times before." His parents died of old age. He shares his room with four friends. His vital signs are normal. CBC reveals: WBC 5,500 mm3 Hemoglobin 7.0 mg/dl Hematocrit 22% Platelets 196,000mm3 RBC count 1.7 million MCV 119 fl MCH 36 MCHC 28% Reticulocyte count 04% Peripheral smear shows anisocytosis, poikilocytosis, and basophilic stippling. What is the best next step in the management of this patient?
A. Iron studies
E. Bone marrow biopsy with prussian blue staining
D. Sugar water test
C. Serum B 12 and folate levels
B. Osmotic fragility test
31. A 75-year-old Caucasian male comes to the office for his routine medical check-up. He complains of fatigue for the past month. His previous medical history is significant for calcified aortic valves and hypertension. His vital signs are stable; except for a blood pressure of 150/90 mm Hg. Physical examination reveals pallor and a 4+ ejection systolic murmur in the aortic area. Lab reports show: Hb 9 g/dl MCV 75 fl Reticulocyte count increased Serum LDH increased Haptoglobin decreased Peripheral smear fragmented RBC Which of the following is the most likely cause of this patient's anemia?
A. Bleeding peptic ulcer.
E. G6PD deficiency anemia.
D. Warm antibody hemolysis.
C. Macrovascular traumatic hemolysis.
B. Diverticulosis.
32. A 64-year-old male patient with deep vein thrombosis is being treated with unfractionated heparin. On the 4th day of treatment, his platelet count drops to 80,000/cmm. His previous platelet count on day 2 was within normal range. He denies any bleeding-related complications, and is completely asymptomatic. His complete examination does not reveal any signs of bleeding. His blood pressure is 128/80mm of Hg, pulse is 78/min, and respirations are 20/min. He is afebrile. What is the most appropriate next step in the management of this patient?
A. Switch to low molecular weight heparin
D. Start plasmapheresis
C. Stop heparin
B. Stop heparin and start warfarin
E. Stop heparin and start platelet transfusion
33. A 6-year-old African-American child is brought in by his father for complaints of easy fatigability and pallor. These symptoms occurred after the son was treated with "some medication" for a recent diarrhea. Physical examination is normal except for pallor and multiple petechiae. Laboratory values are as follows: Hb 8.0 g/dL WBC 12,000/cmm Platelets 50,000/cmm Blood glucose 118 mg/dL Serum Na 135 mEq/L Serum K 5.3 mEq/L Chloride 110 mEq/L Bicarbonate 18 mEq/L BUN 38 mg/dL Serum creatinine 2.5 mg/dL Total bilirubin 3 mg/dL Direct bilirubin 0.5 mg/dL PT 12 seconds APTT 30 seconds LDH 900 IU/L Reticulocyte count 6% A peripheral blood smear reveals giant platelets and multiple schistocytes. What is the most likely underlying pathophysiology for this boy's pallor?
A. Sickle cell anemia
E. Microangiopathic hemolytic anemia
D. Folate deficiency
C. Vitamin B 12 deficiency
B. Thalassemia
34. A 68-year-old unconscious man is brought to the emergency department by a hospice nurse. He had seizures 2 hours ago, after which he lost consciousness. The hospice staff responded by securing his airway and giving him 2L of oxygen. He is in hospice for terminal care for stage IV esophageal carcinoma. He also had a part of his finger removed 1.5 years ago due to a skin cancer. His pulse oximetry reading is 91%. His temperature is 37.9C (100.2F), respirations are 23/min, pulse is 96/min, and blood pressure is 140/85 mmHg. He does not respond to painful stimuli. Rectal examination reveals a hard, irregular surface of an enlarged prostate. His recent prostate specific antigen level is 40. MRI shows an intracranial lesion with bleeding inside, and these findings are consistent with metastasis. What is the most likely diagnosis?
A. Metastatic prostatic carcinoma
E. Metastatic esophageal carcinoma
B. Glioblastoma multiforme
D. Metastatic squamous cell carcinoma of the skin
C. Metastatic melanoma
35. A 19-year-old man comes to the office and says, "Doctor! I have been having a peculiar problem lately. My stool has a funny color. First, it was black and almost sticky. Yesterday, it became maroon. In fact, today I saw some bright red blood." He denies any associated pain or fever. He is adopted, and his family history is unknown. His vital signs are stable. Physical examination is normal, but his stool is positive for occult blood. Laboratory studies reveal a hematocrit of 29% and hemoglobin concentration of 9.6 g/dL. Colonoscopy reveals hundreds of colonic polyps, which are identified as adenomatous polyps with the biopsy. What is the appropriate recommendation for this patient at this point?
A. Reassure the patient as the polyps are most probably benign and have no long-term complications.
E. The patient needs close surveillance with regular F OBT and CEA levels.
D. The patient needs elective procto-colectomy.
C. Start regular colonoscopy and biopsy eight years from now.
B. Perform regular colonoscopy and biopsy every three years from now on to check for any malignant change.
36. A 44-year-old woman comes to the office with complaints of weight loss and blood in her stools for the last year. Her mother is on chemotherapy for colon carcinoma. Her maternal uncle also had colon cancer, as did her first cousin who died of colon cancer at the age of 46. She is very worried that she might have the same cancer. Based on her history, she falls within the criteria for Lynch syndrome (also known as HNPCC/ Hereditary Nonpolyposis Colorectal Cancer). Apart from the complete work-up for colon cancer, this patient should be evaluated for which of the following condition?
A. Pancreatic carcinoma
E. Endometrial carcinoma
D. Diverticulitis
C. Pseudomembranous colitis
B. Hepatic carcinoma
37. A 72-year-old Hispanic man comes to the clinic with complaints of mild headache and lethargy for the past several days. He complains of cough for the past 12 years but, has been bothering him more lately. The cough is mucoid in nature. He has noticed blood in it once in a while. He has been smoking 1 pack/day for 29 years. His Temperature 37C (98.6F); BP 120/84 mmHg; PR 78/min; RR 24/min. On examination of the lungs, adventitious sounds are heard in all the lobes and scant basilar crackles. Laboratory studies show: WBC 7,600mm3 Hemoglobin 13.6 Hematocrit 40%, Platelets 214,000mm3 Sodium 131 mEq/L Potassium 3.6 mEq/L Bicarbonate 18 mEq/L Blood urea nitrogen 16 mg/dL Creatinine 0.6 mg/dL Glucose 95 mg/dL Serum osmolality 260 mOsm/kg (275-295 mosm/kg H2O) Urine osmolality 310 mOsm/kg (38- 1400 mosm/kg H2O) A chest x-ray shows a 2-centimeter left upper lobe nodule and mediastinal adenopathy your diagnosis is?
A Chronic obstructive pulmonary disease
E. Adenocarcinoma
D. Small cell carcinoma
C. Large cell carcinoma
B. Squamous cell carcinoma
38. A 6-year-old, African-American boy presents with fever and pain in his extremities for the last several hours. The pain is unrelated to movement or posture. His pulse is 102/min, blood pressure is 110/70 mm Hg, temperature is 38C (100.4F), and respirations are 18/min. Physical examination reveals pallor, jaundice, and splenomegaly. Both lower legs are tender to palpation. Lab tests show the following: Hematocrit 20% WBC count 13,000/micro-L Platelet count 180,000/miro-L Bilirubin 5.0 mg/dL Direct bilirubin 1.2 mg/dL Reticulocyte count 11% Peripheral blood smear shows sickle shaped cells. Hemoglobin electrophoresis confirms the diagnosis of sickle cell anemia. After treating the child with analgesia, hydration, and oxygen therapy, the painful episode subsides. Which of the following measures should be employed to prevent aplastic crisis in this child?
A. Supplementation with folic acid
E. Treatment with hydroxyurea
D. Vaccination against pneumococcus
C. Vaccination against parvovirus
B. Supplementation with iron
39. A 22-year-old white male presented to the emergency room (ER) with the sudden onset of acute right upper quadrant pain. The ultrasound showed cholelithiasis. Initial evaluation revealed hemoglobin of 9 gm/dl with an MCV of 90 fl and a total reticulocyte count of 1000 cells per microliter. Peripheral smear revealed polychromatophilia and spherocytes. Liver function tests revealed an elevated indirect bilirubin and normal hepatic enzyme levels. Physical examination is consistent with pallor. The patient's parents were killed in an accident when he was 8-year-old, and the patient does not know anything about the family history. Which of the following is the most correct statement about this patient's condition?
A. His condition is classically transmitted as autosomal recessive disorder.
E. This patient's mean corpuscular hemoglobin concentration (MCHC) is likely to be very low.
D. Vaccination against parvovirus has shown to decrease morbidity and mortality.
C. This patient should be placed on folic acid supplementation.
B. He will probably depend on transfusions.
40. A 70-year-old man presents to the urgent care clinic complaining of extensive bruising and bleeding gums. His medical history is significant for atrial fibrillation for which he takes metoprolol and warfarin. He has been stable on his current dose of warfarin for several months. He denies any recent use of NSAIDs or other over-the-counter medications. The patient reports that he has been taking his warfarin as prescribed and has been trying to "live a healthier life" lately. On further questioning, he reports trying to exercise more often, taking numerous vitamin supplements daily, and eating more vegetables. His new diet consists mainly of vegetables like spinach, Brussels sprouts, and broccoli, as well as copious amounts of green tea. Which of the following lifestyle changes is most likely responsible for this patient's bleeding?
A. Brussels sprouts
E. Vitamin supplements
D. Increased exercise
C. Spinach
B. Green tea
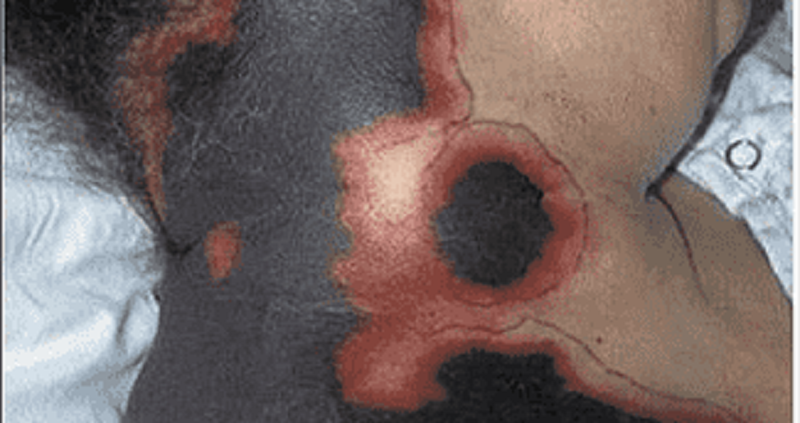
41. A 54-year-old female with a long history of hypertension and a recent hospitalization for atrial fibrillation with rapid ventricular response now returns to the hospital complaining of skin changes. Her medications include warfarin, hydrochlorothiazide and metoprolol. On physical examination, her temperature is 36.7°C (98°F), blood pressure is 130/80 mm Hg, pulse is 80/min and irregular, and respirations are 16/min. You observe the skin changes pictured below. Her exam is otherwise unremarkable. Which of the following is the primary cause of her condition?
A. Antithrombin Ill deficiency
E. Protein C deficiency
D. Vitamin K deficiency
C. Excessive platelet aggregation
B. Factor VII deficiency
42. A 26-year-old man comes with his girlfriend to the emergency department due to a very high fever. He just finished his second cycle of BEP (bleomycin, etoposide, cisplatin) chemotherapy for metastatic seminoma 4 days ago. Other than his fever, he has no complaints. He denies any chest pain, cough, diarrhea or any rash. He stopped smoking ever since he was diagnosed with his "deadly disease," but drinks alcohol occasionally. His temperature is 38.9 C (102 F), blood pressure is 118/70 mm Hg, pulse is 102/min, and respirations are 19/min. Physical examination reveals a pale man without any eyebrows or eyelashes. Chest auscultation is clear. Blood tests reveal: WBC 690/mm3 with 9% neutrophils Hemoglobin 8.6 g/dl Hematocrit 25% Platelets 7 4,000/mm3 What is the best next step in the management of this patient?
A. Give acetaminophen and send him home
E. Give blood, platelet, and G-CSF transfusion
D. Order blood cultures and wait for the results
C. Obtain blood cultures and give vancomycin
B. Obtain blood cultures and give cefepime
43. A 45-year-old white male presented to his primary care physician due to easy fatigability. He is a pure vegetarian and a known alcoholic. Physical examination revealed significant pallor. His hemoglobin level was 10.8gm/dl, and serum iron studies were within normal limits. His physician placed him on folic acid (1 mg daily), and his hemoglobin level increased to 13gm/dl over a period of several months. The patient continued to take folic acid for the next two years. On his next follow-up visit, he complained of gradual memory loss and difficulty in maintaining his balance for the past six months. Which of the following is the most likely thing to consider at this point?
A. He has been treated with subtherapeutic doses of folic acid.
E. The patient should have been started on pyridoxine.
D. Order FTA-ABS to rule out syphilis.
C. The physician should have checked his vitamin B 12 levels.
B. He should be referred for CT of the abdomen with and without contrast.
44. A 63-year-old Caucasian man reports occasional palpitations when exercising. He denies chest pain. Past medical history includes coronary artery disease status post coronary artery stenting, mitral valve replacement with mechanical valve, and diabetes mellitus. He consumes a well-balanced diet and takes one multivitamin tablet daily. His medications include warfarin, simvastatin, metoprolol, lisinopril, and metformin. Physical examination reveals conjunctival pallor and heart sounds consistent with the presence of a mechanical mitral valve. His hematocrit is 30%. The peripheral blood smear shows occasional schistocytes and his serum LDH level is elevated. His stool is negative for occult blood. Which of the following is the most likely cause of this patient's anemia?
A. Iron deficiency
E. Autoimmune hemolysis
D. Glucose-6-phosphate dehydrogenase deficiency
C. Traumatic hemolysis
B. Folate deficiency
45. An 80-year-old female is brought to your office, by her son, because of severe fatigue. She lives alone and is suffering from severe degenerative joint disease, which puts her in a house arrest-type state. Her son usually helps with getting grocery. Her only other medical problem is hypertension. She takes hydrochlorothiazide and acetaminophen. Her vitals are stable. On examination, she has pallor, and evidence of severe degenerative joint disease. Which of the following is the most likely cause of pallor in this patient?
A Vitamin D deficiency
E. Chronic hemolysis
D. Folate deficiency
C. Iron deficiency
B. Vitamin C deficiency
46. A 39-year-old woman comes to the office and complains of double vision. She feels "weak all over," especially at the end of the day. She had the same complaints 8 months ago that persisted for several weeks, but she didn't see a doctor because she had no insurance then. She has no past medical history. Her mother has rheumatoid arthritis, and her brother has type 1 diabetes mellitus. Her vital signs are normal. She has diplopia and mild ptosis. Her blood profile, CBC and thyroid tests are within normal limits. Electromyography and repetitive nerve stimulation reveals a decremental response in compound action potentials. Her acetylcholine receptor antibody test is positive. Which of the following tests should be ordered next?
A Muscle biopsy
E. CT scan of chest
D. Anti-RNP antibodies
C. Anti-Jo antibodies
B. Edrophonium (Tensilon) test
47. A 34-year-old woman comes to the ER because of right lower leg swelling, redness, and pain. She has no significant past medical history and does not use any medications. Her mother has a history of pulmonary embolism. Her temperature is 36.7C (98F), pulse is 80/min, respirations are 16/min, and blood pressure is 120/76 mmHg. Examination shows tenderness to palpation in the right calf. Compressive ultrasonogram shows a deep vein thrombosis of the right leg. Further evaluation reveals an elevated plasma homocysteine level. She is started on heparin and warfarin therapy. What other additional therapy is indicated in this patient?
A Clopidogrel
E. Simvastatin
D. Pyridoxine
C. Vitamin E
B. Streptokinase
48. A 79-year-old woman presents to your office complaining of an intermittent skin rash over the last several months. She denies fever, headache, and recent weight loss. Her past medical history is significant for diet-controlled diabetes and right knee osteoarthritis treated with acetaminophen. Physical examination reveals several dark purple ecchymotic areas over the dorsum of both arms. Her abdomen is soft and non-tender. The liver span is 8 cm and the spleen is not palpable. Laboratory studies reveal: Hematocrit 47% WBC count 5,800/mm3 Platelet count 220,000/mm3 Serum creatinine 0.8 mg/dL\ Fibrinogen 350 mg/dL Prothrombin time 10 sec INR 1.0 Partial thromboplastin time 25 sec Which of the following is the most likely cause of this patient's complaint?
A. Poor platelet adhesion
E. Bone marrow failure
D. Vitamin K deficiency
C. Perivascular connective tissue atrophy
B. Lupus anticoagulant
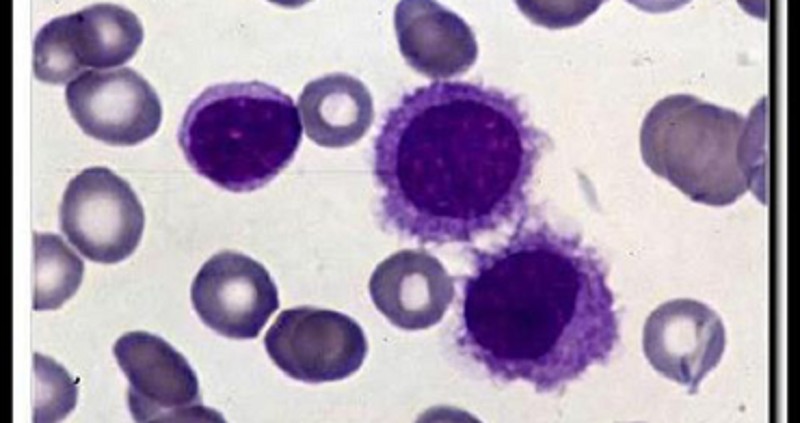
49. A 55-year-old male comes to the physician's office because of fatigue. He denies any other symptoms. His vital signs are stable. Examination shows pallor, massive splenomegaly, and mild hepatomegaly. CBC reveals pancytopenia with striking monocytopenia. His peripheral blood smear is shown below. Bone marrow biopsy shows a dry tap. What is the most appropriate treatment for this patient's condition?
A. Bone marrow transplantation
E. Chlorambucil and prednisone
D. CHOP regimen
C. Cyclophosphamide
B. Cladribine
50. A 36-year-old male comes to your office complaining of progressive fatigability. His past medical history is significant for infiltrative pulmonary tuberculosis diagnosed two months ago. His current treatment includes isoniazid, rifampin, ethambutol, and pyrazinamide. Laboratory values are: Hemoglobin 8 g/dl MCV 77 fl MCHC 30% ESR 17 mm/hr Serum iron 170 micro-g/dl (N 50- 150 micro-g/dl ) Total iron binding capacity (TIBC) 280 micro-g/dl (N 300-360 micro-g/dl) Microscopy reveals two populations of red blood cells (RBC) - hypochromic and normochromic. What is the next best step in the management of this patient?
A. Bone marrow biopsy
E. Pyridoxine
D. Folic acid and vitamin B 12
C. Folic acid
B. Iron preparations
51. A 56-year-old white male comes to the office for a health maintenance visit. He feels healthy, and is "enjoying life as much as possible in a stressed environment." He smokes 2-3 packs of cigarettes daily and drinks socially. His temperature is 37C (98.6F), blood pressure is 160/94 mm Hg, pulse is 78/min, and respirations are 14/min. Physical examination reveals plethora of the face and moderate splenomegaly. Blood tests show the following: WBC 15,600/mm3 Hemoglobin 17 gm/dl Hematocrit 52% Platelets 550,000mm3 RBC count 7.5 million Sodium 141 mEq/L Potassium 3.6 mEq/L Bicarbonate 22 mEq/L Blood urea nitrogen 16 mg/dl Creatinine 0.6 mg/dl Glucose 95 mg/dl The erythrocyte indices are all within normal range. What is the most probable diagnosis?
A. Idiopathic hypertension
E. Primary hyperaldosteronism
D. Congestive heart failure
C. Polycythemia vera
B. Cushing syndrome
A. Idiopathic hypertension B. Cushing syndrome C. Polycythemia vera@ D. Congestive heart failure E. Primary hyperaldosteronism 52. A 51-year-old man comes to you complaining of increased itching, especially after bathing. He also has occasional headaches and dizziness. There is no history of smoking or alcohol use. His sister has psychiatric problems and both parents died in a car accident, many years ago. His vitals are; Temperature: 36.7C (98.2F); BP 148/90 mm Hg; PR 77/min; RR 12/min. On examination, his spleen is enlarged and he appears plethoric. CBC was ordered and came back as: WBC 14,500mm3 Hemoglobin 21.5 Hematocrit 64%, Platelets 521,000mm3 RBC count 7.6 million MCH 30 MCHC 36 MCV 92 ROW 15.1 (n=10.3-14.1) Which of the following is expected on further work up?
A. Absence of measurable erythropoetin in urine
E. Hyponatremia and hyperkalemia
D. Elevated brain natriureteric peptide level
C. Markedly elevated serum cortisol level
B. Elevated ESR
53. A 56-year-old male is admitted to the ICU for the management of hepatic encephalopathy. He is a known alcoholic. He is started on oral neomycin, lactulose, and a low-protein, high-carbohydrate diet. His blood pressure is 116/78 mm Hg, pulse is 78/min, temperature is 37.5C (99.5F), and respirations are 18/min. His labs reveal the following: Hb 10.2 g/dl WBC 7,400/cmm Hct 27% Platelets 4 2,000/mm3 PT 18 sec INR 2.02 PTT 31 sec He has no evidence of active bleeding. Which of the following should be administered to this patient at this time?
A. Fresh frozen plasma
E. Packed RBC
D. Platelets
C. Vitamin K
B. Cryoprecipitate
54. A 35-year-old white female slipped and fell on her side 2 days ago while she was going down the stairs from her house. Since that time, she has been having pain in her right shoulder. She describes this as an ache, which has been about the same over the last couple of days. She has tried ibuprofen, with only slight relief. She denies smoking and alcohol use. Examination suggests a shoulder sprain. You order an x-ray and see a normal shoulder but incidentally a 1.5cm coin-shaped lesion, in the outer side of right lung with well-aerated surrounding lung. She denies any respiratory complaints. What is the next best step regarding her lung lesion?
A. Ask for an old X-ray
E. Open lung biopsy
D. Bronchoscopy
C. Fine needle aspiration
B. CT scan chest
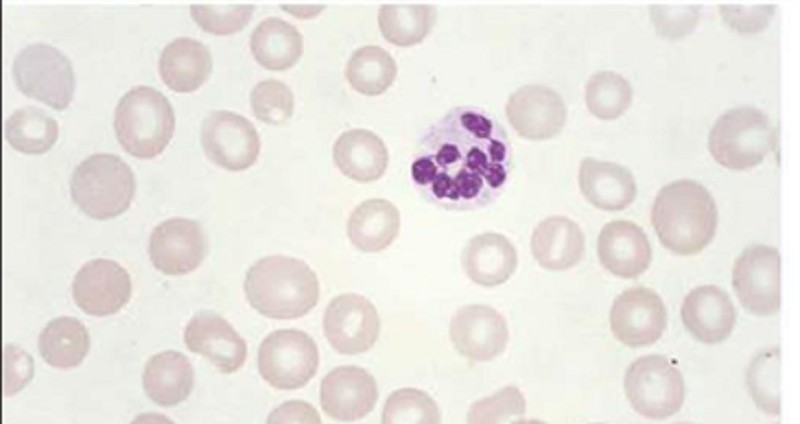
55. A 74-year-old Caucasian man is evaluated for occasional palpitations and poor exercise tolerance. He has been living alone since his wife died two years ago. His diet consists mainly of precooked food that he heats up in the microwave oven. He has a history of degenerative joint disease and hypertension. He takes a daily aspirin, hydrochlorothiazide, and glucosamine. He quit smoking 20 years ago and occasionally drinks alcohol. His peripheral blood smear is shown below. Which of the following substances is most likely elevated in this patient's blood?
A. Ferritin
E. Cobalamin
D. Homocysteine
C. Haptoglobin
B. Methionine
56. A 45-year-old male with Burkitt's lymphoma is being treated with combination chemotherapy and allopurinol. On the 3rd day of treatment, he is noted to have decreased urine output and increased levels of BUN and creatinine. The patient is started on vigorous hydration. EKG reveals prolonged QT intervals. The suspected diagnosis is tumor lysis syndrome. Complete metabolic profile is ordered. Which of the following sets of results are expected in this patient? (Calcium, Phosphate, Potassium, Uric Acid)
A. Increased, Increased, Increased, Increased
E. Decreased, Increased, Decreased, Decreased
D. Decreased, Increased, Increased, Increased
C. Decreased, Decreased, Increased, Increased
B. Decreased, Decreased, Decreased, Decreased
57. A 49-year-old woman comes to the office and complains of a "strange, itchy rash" on her left areola which has been present for the last month. She tried applying various lotions and creams, but the lesion did not resolve. She denies having other skin conditions, except for a poison ivy rash 2 months ago. She does not take any medications and feels "goofy" when she takes penicillin. Physical examination reveals an eczemoid lesion on the left nipple. No abnormality is visible on the mammogram. Biopsy demonstrates large cells surrounded by halo-like areas which invade the epidermis. What is the most likely diagnosis?
A. Adenoma of nipple
E. Lymphocytic carcinoma of breast
D. Phyllodes tumor
C. Scirrhous carcinoma
B. Paget's disease
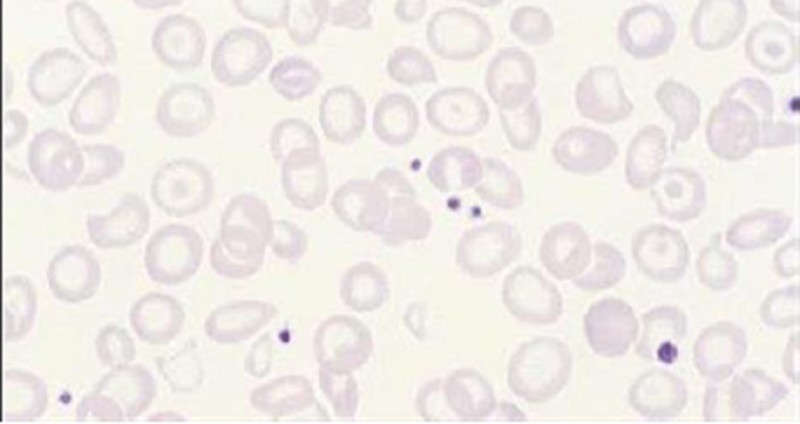
58. A 32-year-old Italian-American man presents to your office for a routine check-up. He works as a business executive and admits to being under a lot of stress recently. He drinks alcohol occasionally and smokes one pack of cigarettes per day. Laboratory analyses reveal: Hemoglobin 10.1 mg/dl RBC count 4.0 x 1012fL MCV 70fl WBC count 5,500/mm3 Platelets 170,000/mm3 Serum calcium 10.1 mg/dl Serum potassium 4.5 meq/L Serum sodium 135 meq/L Serial fecal occult blood tests are negative. A peripheral blood smear reveals the following: Which of the following is the best treatment for this patient?
A. Iron
E. Erythropoietin
D. Reassurance
C. Cobalamin
B. Folic acid
59. A 55-year-old woman comes with complaints of episodes of night sweats and fever, for the last 6 weeks. She denies any cough or other respiratory complaints. She has lost 20 lb (9kg) and does not feel like eating anything. She denies smoking or alcohol use. Her brother was recently diagnosed with polycythemia vera. Physical examination reveals pallor and splenomegaly. Chest-X ray is within normal limits. Blood work is ordered and results are: WBC 66,100/cmm Hemoglobin 8.70 Hematocrit 30%, Platelets 610,000/cmm The leukocyte distribution on differential smear was Promyelocyte 1% Myelocyte 8% Metamyelocyte 15% Bands 35% Segmented Neutrophils 25% Lymphocytes 14% Monocytes 2% Further tests are ordered. Which one of the following is expected in this patient?
A. Elevated leukocyte alkaline phosphatase
E. Decreased leukocyte alkaline phosphatase
D. Presence of auer rods
C. Absence of measurable erythropoetin in urine
B. Increased bone marrow iron
60. A 41-year-old fire-fighter comes to your office and requests for prostate cancer screening. He is concerned because his elder brother was recently diagnosed with prostate cancer, and he read in the paper that "cancers run in families." He requests to be screened urgently, as he "cannot even think of life with such a deadly disease." He has no medical complaints. He has been your patient for the past 6 years, and has no other medical history. He is on a very balanced diet, and adds that he eats a lot of garlic "so that cholesterol remains in check." He takes a low-dose aspirin daily. He does not smoke, and is only a social drinker. He admits using marijuana "once in a while” What is the best next step to address this patient's concerns?
A. Transurethral ultrasonogram
E. Needle biopsy
D. Perform digital rectal examination
C. T ransrectal ultrasonogram
B. Bone scan
61. A 62-year-old man comes to the office and complains of increasing fatigue and weakness for the last 4 months. He also describes a dull pain in his back and arms, which gets worse with walking. He denies any numbness or paresthesia. On examination, he appears pale. There is tenderness around the lumbar spine. CBC reveals: WBC 8,600 mm3 with normal differential Hemoglobin 8.6 g/dl Hematocrit 27% Platelets 164,000 mm3 The RBC morphology is significant for a rouleaux appearance. The ESR is 55mm/hr. Bence Jones proteins are identified in the urine. Which of the following is expected in this patient's bone marrow examination?
A. Over proliferation of plasma cells
E. Hypocellular and fibrotic bone marrow
D. Normocellular bone marrow
C. Hypoplastic fat- filled marrow with no abnormal cells
B. Increased marrow cellularity with megakaryocytic hyperplasia
62. A 27-year-old male presents with dyspnea and fatigue. He has no family history of asthma, heart disease or any blood disorder. His vital signs are stable, and he is afebrile. The only significant findings on examination are pallor and splenomegaly. Lab studies show: Hematocrit 20% WBC count 4,000/micro-L Platelet count 85,000/miro-L Bilirubin 7 mg/dl Direct bilirubin 1 .2 mg/dl Serum LDH 500 U/L (normal value is 80-280 U/L) Serum haptoglobin 20mg/dl (normal value is 30-220 mg/dl) Peripheral blood smear shows microcytic hypochromic cells. Serum ferritin is low while total iron binding capacity (TIBC) is elevated. Reticulocyte count is 5 %. Urine dipstick testing is positive for hematuria and microscopy of urine shows 1 RBC/HPF. Repeated G6PD assays are normal. Coomb's and micro-Coomb's tests are negative. Bone marrow examination shows hypocellular marrow. Based on these findings, what is the most likely diagnosis?
A. Aplastic anemia
E. Paroxysmal nocturnal hemoglobinuria
D. Autoimmune hemolytic anemia
C. Hereditary spherocytosis
B. G6PD deficiency
63. A 44-year-old man who comes to the office because he has had several episodes of hemoptysis for the past two months. He admits to smoking 2-3 packs of cigarettes daily for the last 24 years. Physical examination and chest x-ray are very suggestive of a lung malignancy. Chest CT and bronchoscopy with biopsy are done, and the patient goes on vacation in Aruba. The patient returns to the office after one week, and you are now holding the biopsy result in your hands. It reads, "The tumor has spread to the hilar and mediastinal lymph nodes with bony extension." Which of the following is the most appropriate opening statement?
A. "How much would you like to know about your condition?"
E. "Would you like to have someone else with you as I don't have good news for you?"
D. "Unfortunately, the situation is more serious than what I earlier thought."
C. "What do you think of your symptoms?"
B. "I am sorry to tell you that you have lung cancer and it is fairly advanced."
64. A 47-year-old man comes to the office for the evaluation of a sore over his right ear. His sore bleeds and oozes, and has remained open for 3 weeks. He thinks that it has been growing slowly over the past year. He works for the postal service (USPS), and is usually out all day delivering mail. He admits to smoking approximately 2 packs of cigarettes daily for the last 13 years. Physical examination reveals a punched out 1.5 cm ulcer on his right auricle. There are no enlarged lymph nodes. Full thickness biopsy reveals proliferating malignant cells which arise from the epidermis and extend into the dermis in lobules or strands. What is the best next step in the management of this patient?
A. Surgical excision with 1-2 mm of clear margins
E. Local chemotherapy with anticancer creams
C. Scraping
B. Wide excision with at least 5 em margins
D. Observe for 3 weeks and then examine
65. A 42-year-old woman is evaluated for chronic abdominal pain and fatigue. Her pain is epigastric, crampy, and sometimes awakens her from sleep. She denies any recent weight loss, nausea, or vomiting. Her diet consists mainly of fruits and vegetables. She also complains of a "strange appetite" for paper and ice that she has never had before. Upper gastrointestinal endoscopy reveals an ulcer located on the anterior wall of the duodenal bulb. Her unusual appetite is most directly related to:
A H. Pylori infection
E. Lactose intolerance
D. Oral leukoplakia
C. Chronic bleeding
B. Vitamin deficiency
66. A 27-year-old African-American woman presents to the emergency room complaining of unilateral leg swelling, pleuritic chest pain and shortness of breath. She reports a rash on her face that worsens in the sun, two previous miscarriages, and complains of recent painful swelling in both knees. A CT angiogram confirms a pulmonary embolus. Which of the following is the most likely laboratory abnormality?
A. Decreased prothrombin time (PT)
E. Thrombocytosis
D. Increased bleeding time
C. Prolonged partial thromboplastin time (PTT)
B. Absent Von Willebrand's factor
67. A 60-year-old man comes to office with persistent complaints of malaise and easy fatigability, for the past 8 months. On examination, he appears pale. PR 93/min; BP 127/84mm Hg; Temperature 37C (98.6F); RR 16/min. Fecal occult blood test is negative. Further testing is ordered that include CBC, serum electrolytes and colonoscopy. The results are: WBC 7,600mm3 Hemoglobin 8.8 gm/dl Hematocrit 30%, RBC count 3.6 million Platelets 211,000mm3 RBC Indices were: MCV 65 fl MCH 16.5 pg MCHC 26% Reticulocyte count 0.5% Which one of the following is expected on iron studies in this patient? Serum Iron, Ferritin, TIBC, Transferrin Saturation
A. Low,High,Low,Low to normal
E. Low,Low,Low,Low
D. Low,Low,High,Low
C. High,Normai,High,Normal to High
B. Normal, Normal, Normal, Normal
68. A 25-year-old male presents to his physician with dyspnea and fatigue for the last few weeks. He is a non-smoker. He denies any family history of asthma or blood disorders. He does not take any medications. Examination shows pallor, scleral icterus and splenomegaly. Lab tests show the following: Hematocrit 20% WBC count 1 0,000/micro-L Platelet count 180,000/miro-L Total Bilirubin 7 mg/dl Direct bilirubin 1 A mg/dl BUN 10 mg/dl Serum creatinine 0.7 mg/dl Serum LDH 400 U/L (normal value is 80-280 U/L) Serum haptoglobin 160mg/dl (normal value is 30-220 mg/dl ) Reticulocyte count 8 % Peripheral blood smear shows spherocytes with central pallor. Osmotic fragility and direct Coombs' tests are positive Based on these findings, what is the most likely diagnosis?
A. Hereditary spherocytosis
E. G6PD deficiency
D. Sickle cell anemia
C. Paroxysmal nocturnal hemoglobinuria
B. Autoimmune hemolytic anemia
69. A 56-year-old man complains of fatigue and occasional palpitations. He has a 20-year history of diabetes mellitus and takes daily insulin therapy. He receives hemodialysis three times a week for end-stage renal disease. He was recently started on erythropoietin therapy for anemia (his pretreatment hemoglobin was 8.0 mg/dl). Physical examination at this visit reveals pale conjunctiva. Repeat laboratory studies show: Hemoglobin 9.2 mg/dl MCV 77 fl MCHC 30 g/dl WBC count 7,000/mm3 Platelets 150,000/mm3 Hemoglobin A1c 7.5% ESR 15 mm/hr Which of the following is likely to be helpful in improving this patient's symptoms?
A. Tighter blood glucose control
E. Splenectomy
D. Folic acid supplementation
C. Iron supplementation
B. Higher erythropoietin dose
70. A 48-year-old Caucasian female is undergoing a routine work-up 9 months after radical mastectomy due to right-sided breast cancer. She has no present complaints, and says that she is 'full of energy'. Chest radiograph reveals an isolated pulmonary nodule, 2.0 cm in diameter, in the middle lobe of the right lung. CT confirms that the lesion is solitary with poorly defined margins, but completely within lung parenchyma. Bone scan is negative. CT abdomen and pelvis is normal. Transthoracic biopsy demonstrates adenocarcinoma with positive estrogen receptors (ER) and no HER-2/neu overexpression. Which of the following is the best management strategy for this patient?
A. Surgery
E. Combined chemotherapy and endocrine therapy
D. Pretreatment with monoclonal antibodies against HER-2/neu
C. Hormone therapy
B. Systemic chemotherapy
71. A 22-year-old female presents to the emergency room with a nosebleed. A quick review of her records reveals that she presented with the same problem yesterday, at which time the bleeding was stopped with prolonged local pressure. On review of systems, the patient also reports easy bruising for the past several months. On physical examination, her heart and lungs appear normal. The liver span is 8 cm and the spleen is not palpable. There are scattered ecchymoses over her arms and legs. Laboratory findings include the following: Hematocrit 45% Platelet count 9,000/mm3 Leukocyte count 5,500/mm3 Neutrophils 56% Eosinophils 1% Lymphocytes 33% Monocytes 10% Fibrinogen 250 mg/dL Prothrombin time 13 sec Which of the following is the most likely cause of this patient's condition?
A. Bone marrow infiltration by malignant cells
E. Immune destruction of platelets
D. Platelet sequestration
C. von Willebrand disease
B. Bone marrow aplasia
72. A 55-year-old woman comes to her primary care physician with complaints of pain, itching and red streaks in her left arm. She feels that her arm is "simply not the same". She had a similar episode in her chest almost 2 weeks ago, but it went away on its own. She has no other complaints, except for heartburn and some upper abdominal pain that has been there for a few months. She takes antacids for it, but has never got over it completely. She thinks that she has lost some weight but she feels happy about it, as she always wanted to lose weight. Her vitals are stable and there is mild epigastric tenderness. She has tender, erythematous, cord like veins palpable over left arm and some over the chest. She smokes 1-2pack/day for 15years and drinks alcohol, only on parties. What is the next best step in this patient?
A. Upper Gl endoscopy with barium swallow
E. Spiral CT chest
D. CT scan abdomen
C. Antibiotics and reassurance
B. Colonoscopy
73. A 10-year-old white boy is brought to the office by his foster parents for the evaluation of severe pain in his left knee for the last few days. His left knee has been hurting so bad that he is now unable to play with his peers. The pain is continuous and non-radiating. His knee appears swollen, but he denies any history of trauma. His family history is unknown. His vital signs are stable. Physical examination reveals a pale young boy. The left knee is tender, erythematous and swollen. Blood tests reveal: WBC 12,600mm3 Hemoglobin 9.3 g/dl Hematocrit 29% Platelets 201,000mm3 ESR 40 X-ray of the knee reveals that the lower end of the femur has a central lytic lesion, onion skinning and a moth-eaten appearance with some extension into the soft tissue. What is the most likely diagnosis?
A. Osteomylitis
E. Fibrosarcoma
D. Glomus tumor
C. Chondrosarcoma
B. Ewings sarcoma
74. A 56-year-old white male is being evaluated for having isolated Ig G elevation. The level of serum IgG is 2400 (Normal is 700 to 1500), while the levels of the other paraproteins are within normal limits. The patient was previously admitted with a diagnosis of pneumonia, which resolved completely with levofloxacin. His other laboratory test results are as follows: Hemoglobin 13.0 g/dl Serum Ca 8.0 mg/dl BUN 18 mg/dl Creatinine 1.1 mg/dl Bone marrow biopsy reveals 2% of plasma lesions. What is the most appropriate next step in the management of this patient?
A. Reassurance and regular follow-up
E. Autologus bone marrow transplantation
D. Combination chemotherapy
C. Interferon
B. Melphalan and prednisolone
75. A 55-year-old Caucasian male is hospitalized after a massive hemorrhage from a duodenal ulcer. The hemorrhage was stopped with endoscopic manipulation. Two litters of Ringer lactate were infused and two units of packed red blood cells (RBC) ordered. Ten minutes after the transfusion of packed RBC had been started; the patient was complaining of tremor and feeling 'chilly.' His temperature is 39.4 C (103 F), blood pressure is 120/76 mmHg, pulse is 100/min, and respirations are 24/min. The transfusion was stopped, and acetaminophen was given. Direct antiglobulin test and plasma free hemoglobin level are negative. Urinalysis is normal. The reaction abated three hours after the transfusion had started. Which of the following actions could have prevented the reaction described?
A Warming the blood
E. Washing cells
D. Infusing calcium gluconate
C. Careful cross matching of the blood
B. Using whole blood
76. A 51-year-old man comes to the office for his annual examination. He is apparently healthy, and does not have any complaints. His diet is normal, and he exercises regularly. He experiences some stress at work, but says that he is "strong and can fight it out." His father died of a heart attack 4 years ago, and his mother has Alzheimer's disease. His brother has recently been diagnosed with colonic polyps. His vital signs are stable. Hematology and chemistries are within normal limits, but the fecal occult blood test (FOBT) is positive. What is the best next step in the management of this patient?
A. Perform screening sigmoidoscopy
E. Order abdomen radiograph for air under the diaphragm
D. Advise him to change his diet and examine him next week
C. Do colonoscopy
B. Perform double contrast barium enema
77. A 56-year-old woman is complaining of cough for the past 4 months. The cough was dry initially, but only yesterday she was scared-to-death to see phlegm with blood. She is not feeling well and thinks that she has lost "a lot of weight" recently, despite no apparent change in her diet. She swears that she has never smoked a cigarette in her life. There is no history of night sweats nor contact with any person with similar complaints. She is a housewife who rarely drinks, and can't think of using recreational drugs. She is completely faithful to her husband. Her husband is also a "religious non-smoker". Her vitals are stable and lung examination reveals no significant findings. Her chest x-ray shows 1.5cm lesion in the right peripheral lung field and no evidence of any hilar or mediastinal lymph node enlargement. What is the most probable diagnosis?
A. Tuberculosis
E. Adenocarcinoma of lung
D. Squamous cell carcinoma of lung
C. Small cell carcinoma of lung
B. Sarcoidosis
78. A 35-year-old man presents with gastrointestinal complaints for the last 4 months. He currently has fever, bloody diarrhea, nausea, and severe abdominal cramps. He has lost 20 lb (9kg), and has also been feeling fatigued and anorexic. His temperature is 37.3C (99.1 F), blood pressure is 110/74 mm Hg, pulse is 98/min, and respirations are 22/min. Physical examination reveals tenderness in the right lower quadrant. Digital rectal examination is positive for occult blood. His blood work shows: WBC 11,600 mm3 Hemoglobin 9.6 g/dl Hematocrit 30% Platelets 214,000 mm3 Flexible sigmoidoscopy reveals larger areas of ulceration within the colon. What is the best next step in the management of this patient?
A. Refer him for procto-colectomy
E. Give a bolus of corticosteroids
D. Perform a biopsy of the colon lesion
C. Give sulfasalazine
B. Dietary modification and reassurance
79. A 74-year-old immigrant from Colombia comes to the office and complains of having "all sorts of problems of old age." He has pain all over his body. He often has headaches and feels dizzy. He has visual problems, and finds it difficult to walk. For the last several weeks, he has been feeling weak and numb in his feet. He lives with his son, and is not happy with the way his son treats him; however, he denies receiving any form of physical abuse. His past medical history is unremarkable. His mother had "some blood disease." His vital signs are stable. Physical examination reveals multiple bruises on his body, and sensory deficits in his feet. Other significant findings include lymphadenopathy and hepatosplenomegaly. Ophthalmoscopy shows dilated, segmented, and tortuous retinal veins. Laboratory studies show: WBC 10,200 mm3 Hemoglobin 9.6 g/dl Hematocrit 29% Platelets 94,000 mm3 Sodium 141 mEq/L Potassium 3.6 mEq/L Blood urea nitrogen 18 mg/dl Creatinine 0.8 mg/dl Glucose 115 mg/dl Serum protein electrophoresis reveals an IgM spike. Which of the following is the most likely diagnosis in this patient?
A Multiple myeloma
E. Heavy chain diseas
D. Elderly abuse
C. Monoclonal gammopathy of undetermined significance
B. Waldenstrom's macroglobulinemia
80. A 66-year-old female comes for removal of a lipoma from her elbow. She wants the swelling out because it looks ugly when she wears sleeveless tops. Her only complaints are general malaise and fatigue for the past 8 months, which she attributes to her "being alone all the time." Her vital signs are within normal limits. Physical examination reveals mild pallor and both cervical and supraclavicular lymphadenopathy. Her preoperative blood count reveals the following: Hemoglobin 10.0 g/dL Hematocrit 32% Platelets 126,000/cmm WBC 31,600/cmm Leukocyte distribution Segmented neutrophils 18% Lymphocytes 77% Bands 4% Monocytes 1% The pathologist reports the presence of "leukocytes that have undergone partial breakdown during preparation of a stained smear or tissue section, because of their greater fragility." Lymph node biopsy confirms the diagnosis. What is the correct statement about the above patient?
A. The prognosis is extremely bad.
E. The most common cause of death is renal failure.
D. This is a classic T-cell disease.
C. The presence of thrombocytopenia is a poor prognostic factor.
B. This is a form of plasma cell leukemia.
81. A 25-year-old white female presents to the clinic with persisting pain in her wrists and ankles for the last 3 months. The pain is 3/10 in intensity, and partially relieved by ibuprofen. She also has a rash on her face. She denies smoking, and drinks alcohol occasionally. Her temperature is 37.3C (99.2F), blood pressure is 120/80 mm Hg, pulse is 79/min, and respirations are 18/min. Physical examination reveals swollen joints of the hands and ankle, as well as erythema over the bridge of the nose and the upper cheeks. There is no muscle weakness. Labs show: Hemoglobin 11.0 g/dL Hematocrit 33% Platelets 240,000/mm3 WBC 13,600/mm3 Leukocyte distribution: Segmented neutrophils 76% Lymphocytes 20% Bands 2% Monocytes 2% RF, ANA, and antibodies to double stranded-DNA are positive in high titers. What is the most likely diagnosis?
A. Scleroderma
E. Mixed connective tissue disease
D. Polymyositis
C. Dermatomyositis
B. Systemic lupus erythematosus
82. A 44-year-old white male comes to the office and says, "I have had this persistent, upper abdominal pain for the past 2 months. My wife has peptic ulcer, and I think I also have an ulcer down there, so I take some of her medicines. At first, the medicines made the pain go away, but soon after the pain proved to be too tough for the medicines. I hardly want to eat anything now. Do you think all this is due to some reaction to those medicines?" Physical examination reveals mild tenderness in the epigastric region. Esophagogastroduodenoscopy reveals a mass in the pylorus, which the biopsy identifies as an infiltrating, low-grade, gastric mucosa-associated lymphoid tissue (MALT) lymphoma. Further work-up concludes that there are no regional lymph nodes involved. What is the best next step in the management of this patient?
A. Radical gastrectomy with en bloc resection of spleen and regional nodes
E. Observation and strict surveillance
D. Radiotherapy
C. Give combination chemotherapy.
B. Give a combination of omeprazole, clarithromycin, and amoxicillin.
83. A 48-year-old woman comes to the office because her regular screening mammogram revealed irregular densities. Radiographic-guided needle biopsy shows evidence of invasive lobular carcinoma. The tumor is hormone receptor positive (HR +). Further investigation reveals involvement of the axillary lymph nodes; the other breast seems to be spared. No distant metastasis is detected. She undergoes modified radical mastectomy, along with radiotherapy. She is then prescribed adjuvant chemotherapy and tamoxifen for 5 years. This patient's use of tamoxifen increases her risk for developing which of the following cancers
A. Ovarian cancer
E. Cervical cancer
D. Pancreatic cancer
C. Lung cancer
B. Endometrial cancer
84. A 42-year-old African-American woman presents to your office with bilateral knee pain that severely limits her mobility. She also complains of joint stiffness in the morning that takes several hours to improve. Her hand joints are symmetrically swollen. She has been taking over-the-counter ibuprofen and aspirin with little relief of symptoms. She has no other medical problems and does not use tobacco, alcohol, or illicit drugs. Her vital signs are within normal limits. Physical examination shows pain and swelling of both wrists and knees. Laboratory studies reveal: Hemoglobin 8.4 mg/dl Serum iron 30 μg/dL (normal 50- 150 μg/dL) Total iron binding capacity 230 μg/dL (normal 300-360 μg/dL) Ferritin 300 ng/dl Which of the following is most likely to improve this patient's anemia?
A. Iron supplementation
E. Splenectomy
D. lnfliximab
C. Cyanocobalamin supplementation
B. Folic acid supplementation
85. A 17 -year-old male presents to clinic for routine check-up. He is a long distance runner and has beenachieving outstanding results recently. He is very proud of his athletic achievements, remarking that his effort "pays off." He does not smoke or consume alcohol. His family history is significant for diabetes mellitus in his mother and skin cancer in his father. Chest examination is normal. His liver span is 8 cm and his spleen is not palpable. His current laboratory findings include: Hematocrit 59% WBC count 7,500/mm3 Platelet count 170,000/mm3 ESR 15 mm/hr Which of the following is the most likely explanation for the high hematocrit in this patient?
A. High oxygen affinity hemoglobin
E. Autonomous erythroid precursor proliferation
D. Renal artery stenosis
C. Steroid drug abuse
B. Intensive exercise schedule
86. A 65-year-old Caucasian male had undergone cardiac catheterization followed by aortic valve replacement for severe aortic stenosis and coronary artery bypass grafting for three-vessel disease. His postoperative course was complicated by atrial fibrillation and a urinary tract infection. His other medical problems include hypertension, diabetes, and hypercholesterolemia. He is also receiving heparin, ciprofloxacin, and amiodarone. On postoperative day five, he developed prolonged bleeding from the venipuncture site. His labs show: Hb 11 .5 g/dL MCV88 fl Platelet count 50,000/cmm Leukocyte count 7,500/cmm Segmented neutrophils 68% Bands 1% Eosinophils 1% Lymphocytes 24% Monocytes 6% Prothrombin time 12 sec (INR=1.0) Partial thromboplastin time 65 sec His preoperative labs were unremarkable. What is the most likely cause of these findings in this patient?
A. Thrombotic thrombocytopenic purpura
E. Medication effect
D. Vitamin deficiency
C. Idiopathic thrombocytopenia purpura
B. Hemolytic uremic syndrome
87. A 23-year-old man presents to the emergency room complaining of severe abdominal pain. He has also suffered from nausea and vomiting for several hours. His past medical history is insignificant, but his brother has had similar problems. He denies risky sexual behavior and intravenous drug use. On exam, his temperature is 38.8C (101.8F), heart rate is 102/min, and respirations are 14/min. There is tenderness in the right upper quadrant exacerbated by deep inspiration. The liver span is 7 cm. His spleen is palpated 2 cm below the left costal margin. There are no peritoneal signs. Which of the following is the most likely diagnosis?
A. Acute viral hepatitis
E. Hereditary spherocytosis
D. Hodgkin's lymphoma
C. Gaucher's disease
B. Acute pancreatitis
88. A 34-year-old man presents to your office for a routine check-up. He has no current complaints except for being "a little stressed out." He works as an executive officer and travels a lot within the country. He does not smoke and consumes alcohol occasionally. He currently takes no medications. His family history is insignificant. His blood pressure is 130/80 mmHg and heart rate is 80/min. Chest examination is unremarkable. The liver span is 8 cm and the spleen is not palpable. There is no cervical lymphadenopathy. Laboratory studies show: Erythrocyte count 5 million/mm3 Hemoglobin 14.0 g/dL Leukocyte count 8,000/mm3 Platelet count 80,000/mm3 Which of the following is the best initial test for this patient?
A. Epstein-Barr virus titers
E. Blood folate level
D. Schilling test
C. Rapid plasma reagin test
B. HIV antibody test
89. A 62-year-old woman presents complaining of recurrent cough productive of yellow sputum. She was seen several weeks ago for similar complaints and was effectively treated with a course of azithromycin. Today she expresses frustration that she seems to keep getting sick with the same infection. On review of systems, the patient also reports recent-onset back pain for which she has been taking acetaminophen. Her past medical history is otherwise insignificant. She has never smoked cigarettes, and drinks alcohol only on rare social occasions. Physical examination reveals conjunctival pallor, a few scattered rales in the lungs bilaterally, and tenderness over the lumbar vertebrae. Laboratory analyses reveal: Hemoglobin 8.4 g/dL Leukocyte count 5,500/mm3 Blood urea nitrogen 34 mg/dL Creatinine 2.0 mg/dL Calcium 10.9 mg/dL Albumin 3.8 g/dL Total protein 9.5 g/dL This patient is at increased risk for recurrent infections because of which of the following abnormalities?
A. Defective chemotaxis
E. Inability to produce effective antibodies
D. Impaired granulocyte oxidative metabolism
C. Defective intracellular bacterial lysis
B. Defective complement production
90. A 25-year-old, G3PO white female in her 8th week of gestation comes to the antenatal clinic. Her obstetric history is significant for two second trimester abortions. She is currently taking folic acid and iron supplementation. She does not smoke, but she drinks alcohol on social occasions. She is in a monogamous relationship with her husband. She has never been diagnosed with or treated for any STDs. Laboratory studies reveal the following: VDRL positive FTA-ABS negative Hct 33% WBC 7,000/mico-L Platelets 70,000/micro-L PT 10 sec APTT 40 sec What is the most appropriate next step in the management of this patient?
A. Give heparin and aspirin
E. Three doses of benzathine penicillin
D. Single dose of benzathine penicillin
C. Repeat VDRL
B. Repeat FTA-ABS
91. A 64-year-old male, who rarely sees the doctor and doesn't believe in screening procedures, comes to office with the complaint of severe back pain. He has not felt comfortable for the past 4 months and is having severe pain in the back. He has found it difficult to sleep. He has hypertension, for which he takes hydrochlorothiazides regularly. He thinks that he has lost some weight. On examination, his BP is 165/90mm of Hg, while rest of vitals are stable. On rectal examination you find a rock hard 2 cm nodule in prostate. Biopsy shows poorly differentiated adenocarcinoma. Bone scans shows wide spread metastasis all over his skeleton. What is the most appropriate treatment for his metastatic disease?
E. Complete androgen blockade with Leuprolide and Flutamide
D. Radicle prostatectomy
C. Flutamide
B. Diethylstilbestrol (DES)
A. Leuprolide
92. A 25-year-old female presents to your office complaining of exertional dyspnea and fatigue. Her past medical history is insignificant. She does not smoke or consume alcohol. Her blood pressure is 110/70 mmHg and heart rate is 90/min. Physical examination reveals pale conjunctiva. The laboratory values are: ESR 15 mm/hr Hemoglobin 7.5 g/dL MCV 70 fl MCHC 29% Leukocyte count 7,000/cmm Segmented Neutrophils 55% Bands 3% Eosinophils 3% Basophils 0% Lymphocytes 32% Monocytes 7% What is the best next step in the management of this patient?
A. Bone marrow sampling
E. HbA2 measurement
D. Schilling test
C. Serum folate level
B. Iron studies
93. A 47-year-old man presents to your office complaining of occasional daytime headaches, dizziness and nausea. He has no significant past medical history. He works as a traffic controller in an underground parking lot. He does not smoke cigarettes, and consumes alcohol only on weekends. He is sexually active in a monogamous relationship with his wife and uses condoms for contraception. His cardiac exam is unremarkable. His abdomen is soft and non-tender. The liver span is 8 cm and the spleen is not palpable. Laboratory findings are: Hematocrit 59% WBC count 7,000/mm3 Platelets 200,000/mm3 Which of the following is most likely responsible for this patient's increased hematocrit?
A. Polycythemia vera
E. Carboxyhemoglobinemia
D. Arteriovenous shunting
C. Pulmonary hypertension
B. Plasma volume loss
94. A 60-year-old Vietnam war veteran comes for his annual examination. He does not have any complaints, other than getting tired very quickly. Physical examination reveals pallor and an enlarged spleen. CBC reveals: WBC 14,000/cmm Hemoglobin 9.9 g/dL Hematocrit 30% Platelets 100,000/cmm The lymphocytes have fine, irregular cytoplasmic projections. Cytochemical testing reveals a strong acid phosphatase reaction, which is not inhibited by tartaric acid. What is the most probable diagnosis?
A Lymphoblastic leukemia
E. Hodgkin's disease
D. Chronic myeloid leukemia
C. Chronic lymphocytic leukemia
B. Hairy cell leukemia
95. A 40-year-old male comes to the office because of progressive knee and shoulder pain, which he describes as 5/10 in intensity and started 6 months ago. He has no other medical problems, except for newly diagnosed diabetes. He admits to "chain smoking" for "all his life" and drinks 1-2 bottles of beer a night. He is faithful to his wife. His mother died of "blood cancer" when he was 3-years-old. His father also has diabetes mellitus. His temperature is 37C (98.6 F), pulse is 86/min, blood pressure is 134/86 mmHg, and respirations are 16/min. Physical examination reveals slightly swollen and tender knee joints. Mild hepatomegaly is present on abdominal examination. What is the best next step in the management of this patient?
A. HbA1C level
E. Steroid injection of the joint
D. X-ray of the shoulder and knee
C. Liver biopsy
B. Serum iron studies
96. A 47-year-old woman comes to the office and complains of burning abdominal pain which has been present for the past 3 months, is grade 6/10 in severity, continuous, and relieved by taking antacids. She also complains of some constipation. Her father has a history of "ulcers in his belly." She works as a floor secretary in a surgical ward, and is not happy with her new boss. She denies any weight loss or decreased appetite. Her temperature is 37.1C (98.8F), blood pressure is 130/85 mm Hg, heart rate is 78/min, and respirations are 14/min. She is awake, alert, and oriented. The abdominal examination reveals normoactive bowel sounds and tenderness in the epigastric region, but no palpable mass. Her stools are occult blood positive. ECG reveals increased PR and shortened QT intervals. The laboratory results reveal the following: Sodium 137 mEq/dL Potassium 4.2 mEq/dL Chloride 101 mEq/dL Bicarbonate 27 mEq/dL Calcium 12.0 mg/dl Phosphorus 2.2 mg/dl BUN 37 mg/dl Creatinine 1.8 mg/dl Which of the following is the most likely diagnosis?
A. Glucagonoma
E. Metastatic gastric carcinoma
D. Vitamin-0 toxicity
C. Parathyroid adenoma
B. Stress ulcer
97. A 42-year-old male presents to your office complaining of fatigue. His past medical history is insignificant. He does not smoke or consume alcohol. His blood pressure is 120/70 mmHg and heart rate is 85/min. Physical examination is insignificant. Laboratory values are: Hemoglobin 7.7 g/dL MCV 72 fL MCHC 28% Leukocyte count 8,000/cmm ESR 15 mm/hr Serum iron and ferritin levels are decreased. What is the next best step in the management of this patient?
A. Iron supplementation
E. Bone marrow sampling
D. Work-up for malabsorption
C. Test for occult blood in the stool
B. Dietary modifications
98. A 35-year-old male is brought to the emergency room with headaches and confusion for the past 2 days. He denies any focal weakness or sensory symptoms. His past medical history is significant for HIV and hepatitis C infections for which he is not receiving therapy. The remainder of his medical history is unobtainable due to his mental status. On physical exam, he has a temperature of 37.9°C (100.2F), a blood pressure of 140/86 mm Hg, a pulse of 96/min, and respirations of 16/min. Mild icterus is present. The patient's oropharynx is clear and his neck is supple and without rigidity. Examination of his chest and abdomen are unremarkable. Neurologic examination reveals no focal deficits. Laboratory studies show: Complete blood count: Hemoglobin 7.6 g/L MCV 85 fl Reticulocytes 8.1% Platelet count 80,000/mm3 Leukocyte count 3,500/mm3 Chemistry panel: Blood urea nitrogen (BUN) 30 mg/dL Serum creatinine 2.2 mg/dL Serum calcium 10.0 mg/dL Blood glucose 98 mg/dL Liver studies: Total bilirubin 3.6 mg/dL Direct bilirubin 1.0 mg/dL Alkaline phosphatase 120 U/L Aspartate aminotransferase (SGOT) 178 U/L Alanine aminotransferase (SGPT) 255 U/L Which of the following is the most appropriate next step in the management of this patient?
A Liver biopsy
E. CT scan of the head
D. Lumbar puncture
C. Right upper quadrant ultrasound
B. Peripheral blood smear
99. A 65-year-old woman is very worried because she recently had a close family member and friend die, one after the other. First, her 85-year-old mother died of an ovarian cancer that was diagnosed 3 years ago. Last week, she lost her best friend to lung cancer that metastasized to the liver and brain. Today, her 58-year-old sister learned that she has breast cancer. She has regular pap smears and breast examinations. She has read in the paper that there are a few ways that have proved to be very successful in preventing breast cancer. Which of the following measures has the best evidence of preventing breast cancer in high-risk women?
A. Prophylactic oophorectomy
E. Having mammograms every month
D. Tamoxifen
C. Low-fat diet
B. BRCA screening
100. A 46-year-old woman comes to the office and says, "I can't believe I've lost so much weight in the last 2 months because I seem to be eating much more than ever. I also find it odd that I drink lemonade all the time, and I have to rush to the bathroom regularly. It seems like everything in me is vanishing." Her temperature is 37.C (98.6F), blood pressure is 110/70mm Hg, pulse is 98/min, and respirations are 14/min. Physical examination reveals a lean woman with an erythematous, scaly plaques on her face, and on her buttocks. The laboratory studies reveal: WBC 6,400 mm3 Hemoglobin 8.7 g/dL Hematocrit 29% Platelets 193,000mm3 Sodium 144 mEq/L Potassium 3.6 mEq/L Bicarbonate 21 mEq/L Blood urea nitrogen 16 mg/dl Creatinine 0.6 mg/dL Glucose 245 mg/dL Which of the following is expected in this patient?
A. Increased thyroxine level
E. Increased serotonin level
D. Increased gastrin level
C. Increased glucagon level
B. Decreased insulin level
101. A 16 year-old-girl with hereditary spherocytosis is scheduled for a splenectomy. She was previously managed with folate therapy and occasional blood transfusions, but her anemia became refractory to medical management alone. Before the operation, she is told that she will have an enhanced risk of developing pneumococcal sepsis. She then asks, "How long will these risks last?" What is the best response to her question?
A. 2 weeks
E. More than 10 years
D. Up to 10 years
C. Up to 2 years
B. Up to 6 months
102. A 57 -year-old Caucasian female is diagnosed with deep venous thrombosis of the right leg that was confirmed with Doppler ultrasonography. She was diagnosed with pneumonia and empyema one week earlier, and treated with chest tube, antibiotics and bed rest. On her 6th day of anticoagulation therapy, she develops right hemiparesis and slight motor aphasia. The laboratory findings are: Red blood cells 4.3 million/mm3 Hemoglobin 14.00 g/dL White blood cells 7,000/cmm Platelets 50,000/cmm APTT 60 sec (N<25-40 sec) Fibrin degradation products negative The emergency head CT scan does not reveal blood in the subarachnoid space or brain parenchyma. Which of the following is the most probable cause of this patient's condition?
A. Non-immune platelet degradation
E. Platelet sequestration and redistribution
D. Antibody-mediated platelet activation
C. Disseminated intravascular coagulation
B. Venous thromboembolism
103. A 42-year-old mildly overweight Caucasian male is being worked-up for his second episode of deep venous thrombosis in two years. Both episodes seem to have been unprovoked. He denies any recent prolonged immobility, long-distance travel or lower extremity trauma. He has no past medical history of diabetes, cancer or liver disease. A thrombophilia work-up is ordered for this patient. Use of which of the following drugs is most likely to give a false-positive result for protein S deficiency?
A. Heparin
E. Simvastatin
D. Clopidogrel
C. Aspirin
B. Warfarin
104. A 56-year-old woman comes to the office for the evaluation of an ulcer on her left elbow. The ulcer is a persistent, scaly red patch with irregular borders, and it sometimes crusts or bleeds. She recalls the time when she badly burned her left elbow while learning how to cook pasta at thirteen years of age. She works as a public relations officer in a large marketing company. She is a social smoker, and does not like drinking alcohol. Physical examination of the left elbow reveals a big scar with a firm, nontender, reddened, non-healing indolent, 3cm ulcer in the center. What is the best next step in the management of this patient?
A. Surgical excision
E. Local radiation
D. Chemotherapy
C. Observation for 3 weeks with antibiotics
B. Punch biopsy
105. A 21-year-old Caucasian man bumped into a table in his living room two days ago and now presents to the emergency department with a swollen and tender right thigh. Pulsation is decreased over the right popliteal artery. His uncle suffered from a "blood clotting disease". This patient's history is most likely to reveal which of the following episodes in his past?
A. Occasional tarry stools
E. Red papules over his trunk and lips
D. Cola-colored urine
C. Joint swelling
B. Spontaneous bruises
106. A 54-year-old Caucasian woman presents to your office with fatigue. She also reports dizziness and palpitations after moderate physical activity. Additionally, her feet feel "numb" and are less sensitive to cold than they used to be. She has no significant past medical history. Physical examination reveals pale conjunctivae and a shiny tongue. Ankle reflex is decreased bilaterally. Laboratory findings include: Hemoglobin 7.6 mg/dL MCV 110 fL MCHC 36 g/dL WBC count 3,900/mm3 Platelet count 150,000/mm3 This patient should be monitored for which of the following long-term complications?
A. Acute myelogenous leukemia
E. Liver cirrhosis
D. Gastric cancer
C. Celiac sprue
B. Hodgkin's disease
107. A 25-year-old African American woman presents with a photo distributed skin rash and arthralgias. She is found to have low-range proteinuria and abnormal urinary sediment. Renal biopsy findings are consistent with focal proliferative glomerulonephritis. Her complete blood count shows: Erythrocyte count 3.2 mln/mm3 Platelets 60,000/mm3 Leukocyte count 2,500/mm3 Which of the following is the most likely cause of these hematologic findings?
A. Bone marrow hypoplasia
E. Dilutional pancytopenia
D. Peripheral destruction of blood cells
C. Abnormal pooling of blood cells
B. Ineffective hemopoiesis
108. A 7-year-old Caucasian boy is brought to your office for a routine check-up. He underwent splenectomy one year ago for persistent anemia and jaundice. He has received pneumococcal vaccination and takes penicillin prophylaxis. His uncle underwent splenectomy for "some blood disorder" in his childhood. His blood hemoglobin level is 11.5 mg/dL and MCV is 90 fl. Blood smear demonstrates occasional red blood cells with single, round, blue inclusions on Wright stain. The latter finding is most likely related to:
A. Hemoglobin precipitation
E. Splenectomy
D. Mechanical RBC damage
C. Penicillin therapy
B. Low reticulocyte count
109. A 45-year-old Asian man presents to your office complaining of easy fatigability. He denies abdominal pain, distention, nausea, vomiting, or significant weight loss. His past medical history includes a gastrectomy for a non-healing gastric ulcer. He is not currently taking any medications. He quit smoking several years ago and does not use alcohol or illicit drugs. His vital signs are within normal limits. Physical examination reveals a shiny tongue and pale palmar creases. No lymphadenopathy, hepatomegaly, or splenomegaly is present. His blood hemoglobin level is 7.5 mg/dL and W8C count is 3,800/mm3. Stool tests for occult blood are repeatedly negative. This patient's condition involves which of the following pathophysiologic mechanisms?
A. RBC membrane instability
E. Mechanical R8C injury
D. Impaired glutathione synthesis
C. lmpaired DNA synthesis
B. Impaired hemoglobin synthesis
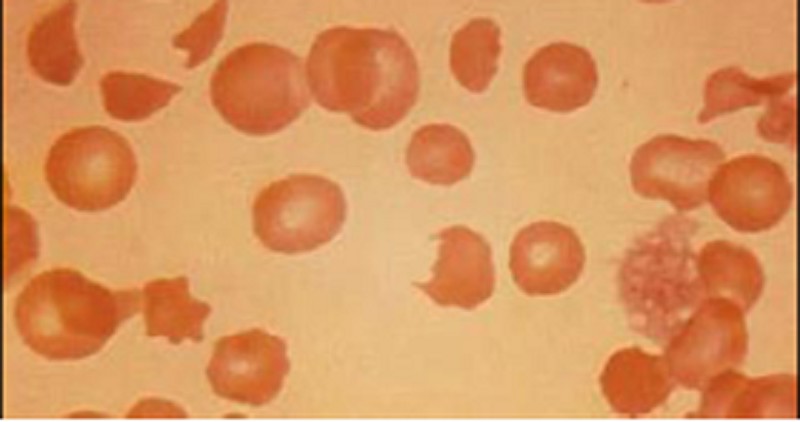
110. A 56-year-old male is being evaluated for increased fatigability. His past medical history is significant for severe aortic stenosis that required aortic valve replacement, diabetes mellitus, and osteoarthritis. Peripheral blood smear findings are shown on the slide below. Which of the following laboratory findings would you most expect to find in this patient?
A. Increased total serum iron level
E. Decreased serum albumin level
D. Decreased reticulocyte count
C. Increased mean corpuscular volume
B. Decreased serum haptoglobin level
111. A 25-year-old white female presents with a 5-day history of sore throat, extreme fatigue, and headaches. She has just returned from a spring break in Jamaica where she had "the time of her life." She smokes 2-3 cigarettes daily and occasionally drinks alcohol. Her vital signs are stable. She is afebrile. Physical examination reveals posterior cervical lymphadenopathy, mild splenomegaly, and exudative pharyngitis. Palatal petechiae are present. CBC shows: WBC 16,000/cmm with 55% lymphocytes Hemoglobin 13 .5gm/dl Hematocrit 4 1% Platelets 216,000/cmm Many variant forms of lymphocytes are seen, including cells with convoluted nuclei and highly vacuolated cytoplasm. Rapid streptococcal throat test, urinalysis, and heterophilic antibody test are all negative. What is the most likely diagnosis?
A. Acute myeloid leukemia
E. Infectious mononucleosis
D. Chronic lymphocytic leukemia
C. Acute lymphoblastic leukemia
B. Chronic myeloid leukemia
112. A 2-year-old boy is brought by his mother to the emergency department because of a high-grade fever which "does not go away" with acetaminophen. For the last four days, the child has been very irritable and is crying a lot. He is also pulling his ear and not eating well. He has been generally well, other than the occasional sore throat this season. His temperature is 38.8C (102.2F), blood pressure is 90/60 mm Hg, pulse is 119/min, and respirations are 24/min. He appears well nourished, but is irritable. Physical examination reveals enlarged cervical lymph nodes and splenomegaly. The tympanic membranes are inflamed. CBC shows: WBC 81,100 mm3 Hemoglobin 8.0 g/dL Hematocrit 25% Platelets 16,000 mm3 Blast forms 80% Prolymphocytes 10% Lymphocytes 10% The blast cells have condensed nuclear chromatin, small nucleoli and scant agranular cytoplasm. Subsequent histochemical staining reveals strongly positive periodic acid Schiff (PAS) reaction. No Auer rods were seen. Which of the following is the most likely diagnosis?
A Burkitt lymphoma
E. Myelodysplastic syndrome
D. Acute lymphoblastic leukemia
C. Prolymphocytic leukemia
B. Acute myelocytic leukemia
113. A mother brings her 7-year-old son in for evaluation of bleeding gums. She reports that he brushes his teeth regularly and visits a dentist twice per year. The boy also complains of easy fatigability and a pounding sensation in his ears. On physical examination, he is at the 5th percentile for height and the 25th percentile for weight for his age. You note several areas of hypopigmentation on his skin. Laboratory findings include: Hemoglobin 7.8 mg/dl RBC count 3.0 x 1012/L MCV 112fl Platelet count 40,000/mm3 This patient's condition is most likely caused by:
A. Chromosomal breaks
E. Thymic tumor
D. Benzene exposure
C. Congenital infection
B. RBC enzyme deficiency
114. A 23-year-old African American man is treated with an antibiotic for an uncomplicated urinary tract infection. Several days later, he presents to your office saying that his initial symptoms have improved but his urine now appears dark. He has no significant past medical history and does not use tobacco, alcohol, or illicit drugs. His temperature is 36.8C (98.2F), pulse is 88/min, respirations are 14/min, and blood pressure is 130/76 mmHg. Physical examination is within normal limits. The urine sample stains positive with Prussian blue and the sediment microscopy is unrevealing. What is the mechanism behind the cell damage responsible for this patient's current complaint?
A. Autoantibody production
E. Inflammatory cytokine production
D. Oxidative stress
B. Spread of the infection
C. Circulating immune complexes
115. A 64-year-old woman comes to the hospital due to an "irritating sore throat for 3 months." She admits to smoking 1 pack of cigarettes daily for the past 29 years, and continues to smoke. She was jailed twice for driving under the influence of alcohol, and went to Alcohol Rehabilitation last year. She currently denies any alcohol intake. She has no fever or any other complaints. She had a complete hysterectomy several years ago for symptomatic fibroids. Her vital signs are stable. Physical examination reveals a 1.5-cm right cervical lymph node. The rest of the examination is normal. Biopsy of the lymph node reveals metastatic squamous cell carcinoma. The CT scan of the chest is negative. What is the best next step in the management of this patient?
A. Empirical chemotherapy
E. Radical neck dissection
D. Screening mammogram
C. Repeat CT in 3 months
B. Panendoscopy
116. A 34-year-old male is brought to the emergency room after being involved in a motor vehicle accident. He suffers blunt abdominal trauma and bilateral femur fractures. He has no significant past medical history. On physical examination, his blood pressure is 80/40 mmHg and his heart rate is 110/min. He receives several units of packed red blood cells. Once stabilized, the patient begins complaining of a tingling sensation in his toes and fingers. His serum calcium level is noted to be 7.2 mg/dL. Which of the following is the most likely cause of this patient's current symptoms?
A. Increased renal tubular secretion of calcium
E. Parathyroid gland suppression due to fluid overload
D. Antibody-mediated red blood cell membrane damage
C. Electrolyte leakage from red blood cells during pre-transfusion storage
B. Calcium chelation by a substance in the transfused blood
117. A 33-year-old computer programmer was diagnosed with ulcerative colitis last year. He had a colonoscopy and biopsy that showed pancolitis, after which no further work-up was done. This is his first visit to a physician in 6 months. He takes aminosalicylates and is in remission, without any symptoms. He is a member of the Ulcerative Colitis Support Group, which recently sent him a letter that said he should be screened for colon cancer. His vital signs are stable. Physical examination reveals mild tenderness on deep palpation of the lower abdomen. What is the best advice for him regarding his concerns?
A. He has an increased risk of colon cancer and he should have prophylactic colectomy.
E. He has an increased risk of colon cancer, and he should have a biopsy.
D. Since he does not have any signs and symptoms, he has no increased risk and doesn't need any surveillance.
C. He has an increased risk of colon cancer and he should have periodic colonoscopy eight years later.
B. He has an increased risk of colon cancer and he should have colonoscopy every year.
118. A 6-year-old Caucasian boy is hospitalized for acute sinusitis that was accompanied with intensive nasal bleeding. Past medical history is significant for recurrent pulmonary infections and several hospitalizations for parenteral antibiotic therapy. The sweat chloride test is positive. The blood tests reveal a prothrombin time (PT) of 20 seconds. Which of the following coagulation factors is most likely to be deficient in this patient?
A Fibrinogen
E. Factor V
D. Factor VII
C. Factor VIII
B. Hageman factor
119. A 72-year-old Hispanic man comes to the clinic with complains of mild headache, and lethargy for the past several days. He complains of cough for the past 12 years, the cough has been bothering him more lately. The cough is mucoid, he has noticed blood in it once in a while. He has smoked 1 pack/day for 29 years. His vitals are, Temperature 37.0C (98.6F); BP 120/84 mm Hg; PR 78/min; RR 24/min. On examination of lungs, adventitious sounds are heard over all the lobes and scant crackles at the base. Laboratory studies show: WBC 7,600mm Hemoglobin 13.6 Hematocrit 40%, Platelets 214,000mm3 Sodium 130 mEq/L Potassium 3.6 mEq/L Bicarbonate 18 mEq/L Blood urea nitrogen 16 mg/dl Creatinine 0.6 mg/dl Glucose 95 mg/dl Serum osmolality 260 mOsm/kg (normal 280) Urine osmolality 310 mOsm/kg A chest x-ray shows a 2-centimeter left upper lobe mass and mediastinal adenopathy. What will be the next best step in management of this patient?
A. Prescribe demeclocycline
E. A CT of head
D. Start furosemide
C. Start an infusion of hypertonic saline
B. Restrict the patient water intake
120. A 34-year-old woman comes to the office for her annual examination. She has been your patient for the last 4 years. She eats a lot of meat, but does not like fruits and vegetables. Her menstrual period began at age 12. She has two children, who are ages 13 and 11. She is in a monogamous relationship with her husband, and uses oral contraceptive pills. She smokes 1/2 pack of cigarettes daily, and drinks alcohol socially. Her mother had breast disease and had an operation, but died 1 month after the surgery due to a heart attack. She has read in "US Health News" that breast cancer is the leading culprit for cancer death among non-smoking women. She now asks you, "What is the most important risk factor for breast cancer?" What is the correct response to this patient's question?
A. Parity of the woman
E. Family history of breast cancer
D. Use of oral contraceptive pills
C. Age of woman
B. Age of menarche
121. A 45-year-old white male comes to the emergency room with "all sorts of things going wrong with him", for the last few months. He has a severe headache, chest and abdominal pain. He is sweating profusely. He has lost weight recently, has diarrhea and palpitations. He is feeling hot all the time. Vital signs reveal BP: 190/100mm of Hg; PR 124/min; RR 18/min; Temperature 37.7 C (99.8F). On physical examination he has enlarged cervical lymph nodes. Examination of the thyroid reveals multiple thyroid nodules. FNA biopsy reveals thyroid C-cell hyperplasia. Which of the following can also be found on laboratory results?
A. Decreased serum calcitonin
E. Increased serum calcium
D. Decreased urine metanephrine
B. Increased serum phosphorus
C. Decreased serum alkaline phosphatase
122. A 54-year-old male had undergone an emergency colonic resection following an extensive ischemic colitis. The surgery was uneventful. The patient has been on peperacillin and tazobactam (Zosyn) for the past five days. He was NPO (nothing by mouth) for the past five days. He has a significant alcoholic history. On postoperative day six, he developed bleeding from the venipuncture site. His temperature is 36.7 C (98 F), blood pressure is 120/76 mmHg, pulse is 80/min, and respirations are 16/min. Lab results are: Hb 11.5g/dL MCV 88 fl Platelet count 160,000/cmm Leukocyte count 7,500/cmm Segmented neutrophils 68% Bands 1% Eosinophils 1% Lymphocytes 24% Monocytes 6% Prothrombin time 20 sec (INR=1.9) Partial thromboplastin time 45 sec His family history is insignificant. Which of the following is the most likely cause of his condition?
A Thrombotic thrombocytopenic purpura
E. Medication effect
D. Vitamin deficiency
C. Idiopathic thrombocytopenic purpura
B. Hemolytic uremic syndrome
123. A 24-month-old pale child is brought to the office by his mother, who says, "Doc, I think he is under some weird spell. He acts bizarre and always seems tired. He likes to eat wooden, painted toys." The child and her mother live in a relatively poor neighborhood. CBC reveals: WBC 8,600 mm3 Hemoglobin 7.1 g/dl Hematocrit 25% Platelets 166,000 mm3 His blood lead levels are elevated. Which of the following is most likely seen in this child's peripheral blood smear?
A. Megaloblastic anemia and basophilic stippling
E. Normochromic, normocytic anemia and basophilic stippling
D. Basophilic stippling and microcytic, hypochromic anemia
C. Loss of concavity of the RBC and basophilic stippling
B. Tear-drop RBCs and hypochromic, microcytic anemia
124. You are called by the hospice nurse to evaluate a 74-year-old man who refuses to eat. He has terminal colon cancer, which was diagnosed 8 months ago and has metastasized to his liver. He has already gone through chemotherapy with 5-Fiourouracil + oxaliplatin. During the past 4 months, his condition has gotten extremely worse. He has lost 501bs (27.6kg), and currently appears totally wasted. As you approach him, he says, "I don't feel like eating anything, and I don't want anymore procedures, but I'll drink any pill that can make me feel better." His abdomen is distended with positive fluid thrills. His liver has several palpable nodules. What is the best pharmacological agent of choice for this patient's anorexia?
A. Megestrol acetate
E. Metoclopramide
D. Ondansetron
C. Dimenhydrinate
B. Dexamethasone
125. A 27-year-old man presents to the emergency department with unremitting nose bleeding. He reports having a similar bleeding episode one year ago that was stopped in the ER. He works as a computer programmer and has a sedentary lifestyle. He drinks alcohol on social occasions but does not smoke or use illicit substances. On physical examination, there are several ruby-colored papules on his lips that blanch partially with pressure. Digital clubbing is also present. His abdomen is soft and non-tender. The liver span is 8 cm and the spleen is not palpable. Laboratory findings are: Hematocrit 60% WBC count 8,000/mm3 Platelets 180,000/mm3 Which of the following is most likely responsible for this patient's increased hematocrit?
A. Polycythemia vera
E. Carboxyhemoglobinemia
D. Arteriovenous shunting
C. Pulmonary hypertension
B. Plasma volume loss
126. A 67 -year-old man presents to your office with a one-month history of progressive fatigue and exertional dyspnea. He has no significant past medical history. Physical examination reveals enlarged, non-tender axillary lymph nodes bilaterally. His abdomen is soft and non-tender and the liver span is 10 cm. Serial fecal occult blood tests are negative. Laboratory values are as follows: Hemoglobin 7.8 mg/dl MCV 90 fl MCHC 33 g/dl Reticulocytes 7% WBC count 22,000/mm3 Platelets 200,000/mm3 Which of the following is most likely to improve this patient's symptoms?
A Folic acid
E. Erythropoietin
D. Pyridoxine
C. Prednisone
B. Iron
127. A 42-year-old white female, who has a long history of dysfunctional uterine bleeding, presented with exertional shortness of breath. On examination, she appears very pale and there is a pulmonic flow murmur heard over the second intercostal space. Her vitals are: BP: 130/80mm of Hg; HR: 80/min and regular; RR: 16/min; Temperature 36.7C (98F). Initial evaluation reveals hemoglobin of 8.2 gm/dL. WBC count is within normal limits. You are suspecting an iron deficiency anemia secondary to excessive bleeding. Which one of the following studies is most definite for the diagnosis of iron deficiency anemia?
A. A low serum ferritin level.
E. Total iron content of the gastric epithelial cells.
D. Bone marrow iron staining.
C. A low serum iron concentration.
B. Increased total iron binding capacity.
127. A 42-year-old white female, who has a long history of dysfunctional uterine bleeding, presented with exertional shortness of breath. On examination, she appears very pale and there is a pulmonic flow murmur heard over the second intercostal space. Her vitals are: BP: 130/80mm of Hg; HR: 80/min and regular; RR: 16/min; Temperature 36.7C (98F). Initial evaluation reveals hemoglobin of 8.2 gm/dL. WBC count is within normal limits. You are suspecting an iron deficiency anemia secondary to excessive bleeding. Which one of the following studies is most definite for the diagnosis of iron deficiency anemia?
A. A low serum ferritin level.
E. Total iron content of the gastric epithelial cells.
D. Bone marrow iron staining.
C. A low serum iron concentration.
B. Increased total iron binding capacity.
128. An 81-year-old man is brought to the hospital due to complaints of very severe pain in his back and thighs. Seven months ago, he was diagnosed with stage IV prostate cancer which reached the spine. He has had palliative radiotherapy of his spine, and is now taking leuprolide. He is restless and very irritable, even after the nursing home staff gave him ibuprofen. He has never received any narcotics. What is the best next step in this patient's pain management?
A Give high dose NSAIDs
E. Repeat radiotherapy
D. Long-acting opiates
C. Start with short-acting morphine
B. T ransdermal fentanyl patch
129. A 16-year-old boy is brought to the office by his basketball coach because, "he is unable to work out with other boys." For the past several weeks, the boy has been complaining of left knee pain which is dull and worsens with running, especially on the court. In addition, he thinks he has lost some weight. He does not smoke or drink alcohol. He is sexually active with many partners, and does not use condoms. His vital signs are stable. On examination, his left knee is swollen and tender. X-ray reveals a sclerotic lesion in the distal femur with periosteum lifted and a "sun burst appearance”. What is the most likely diagnosis?
A. Ewings sarcoma
E. Giant cell tumor
D. Septic arthritis
C. Osteosarcoma
B. Growing pains
130. A 45-year-old previously healthy male is brought to the emergency room because of headaches and confusion for 2 days. He denies any focal weakness or sensory symptoms. He has no significant past medical history and does not use any medications. He does not use tobacco, alcohol or drugs. On physical exam, the patient has a temperature of 37.9°C (100.2F), a blood pressure of 140/86 mm Hg, a pulse of 96/min, and respirations of 16/min. Mild icterus is present. The patient's oropharynx is clear and his neck is supple and without rigidity. Examination of the patient's chest and abdomen is unremarkable. Neurologic examination reveals no focal deficits. Laboratory studies show: Complete blood count: Hemoglobin 84 g/L Platelet count 80,000/mm3 Leukocyte count 5,500/mm3 Chemistry panel Blood urea nitrogen (BUN) 30 mg/dL Serum creatinine 2.2 mg/dL Serum calcium 10.0 mg/dL Blood glucose 98 mg/dL A peripheral blood smear shows many fragmented red blood cells. The prothrombin time is normal. Which of the following is the most appropriate next step in the management of this patient?
A Hemodialysis
E. Platelet transfusion
D. Plasma exchange
C. Electroencephalogram
B. MRI of the brain
131. A 14-year-old boy is brought by his mother because she noticed a change in his voice. He has been having frequent nosebleeds for the last month, and feels that his "left nose" is always congested. There is no history of trauma. He admits to using marijuana, in the absence of his mother. He is otherwise well, and does not take any medications. He actively participates in the school basketball tournaments. Physical examination reveals an intact nasal septum with a visible mass at the back of the left nostril. CT scan reveals an erosion of the adjacent bone. What is the most likely reason of this patient's nosebleeds?
A. Cocaine abuse
E. Chondroma of nasal cartilage
D. Reactive nasal polyps
C. Bleeding disorder
B. Angiofibroma
132. A 60-year-old Hispanic laboratory technician presents with increasing fatigue and generalized weakness for the last 2 months. He also has chronic pain in the lower back and legs when he walks. He has been smoking 2-3 packs of cigarettes daily for 30 years, and drinks alcohol almost daily. His mother has diabetes, while his father died of a stroke. Physical examination reveals pallor. There is mild hepatomegaly. The neurological examination is completely normal. Complete work-up reveals: CBC: Hemoglobin 9.8 g/L MCV 85 fl Platelets 226,000/mm3 Leukocyte count 6,500/mm3 Neutrophils 60% Eosinophils 1% Lymphocytes 29% Lvlonocytes 10% Chemistry panel: Serum sodium 138 mEq/L Serum potassium 4.0 mEq/L Bicarbonate 24 mEq/L Blood urea nitrogen (BUN) 28 mg/dL Serum creatinine 2.1 mg/dL Calcium 11.2 mg/dL Blood glucose 98 mg/dL Liver studies: Albumin 4.0 mg/dL Total protein, serum 9.5 g/dL Total bilirubin 1.0 mg/dL Direct bilirubin 0.8 mg/dL Alkaline phosphatase 110 U/L Aspartate aminotransferase (SGOT) 58 U/L Alanine aminotransferase (SGPT) 25 U/L ESR is 100 mm/h. What is the best next step in the management of this patient?
A. ANA and anti-Smith antibodies
E. Bone scan
D. Kidney biopsy
C. Bone marrow biopsy
B. Serum immunoelectrophoresis
133. A 54-year-old female with megaloblastic anemia and ataxia is given radiolabeled cobalamin by mouth followed by an intramuscular injection of unlabeled cobalamin. The urine radioactivity level measured afterwards is determined to be normal. Which of the following is the most likely cause of this patient's symptoms?
A. Dietary cobalamin deficiency
E. Chronic low-volume Gl bleeding
D. Fish tapeworm infestation
C. Nontropical sprue
B. Atrophic gastritis
134. An 18-year-old boy comes to clinic to discuss an embarrassing problem. For the last 6 weeks he has noticed a painless mass in his right testis. This is not bothering him at all, but it is becoming larger. He is afraid that his girlfriend may notice it and find out about his other partners. He has multiple partners, and does not use condoms. He has no fever and no other medical complaints. His cousin has SLE but otherwise family history is unremarkable. On ultrasound you suspect testicular cancer and order a few tests. Results are as follows: Alpha-fetoprotein (AFP) Increased Beta subunit of the human chorionic gonadotropin (hCG) Normal Placental Alkaline phosphate (PLAP) Normal Carcinoembryonic antigen (CEA) Slightly Increased Lactate Dehydrogenase (LDH) Increased What could be the most likely diagnosis?
A. Seminoma
E. Sertoli cell tumor
D. Teratoma
C. Choriocarcinoma
B. Embryonal carcinoma
135. A 57-year-old man comes to the office and complains of long-standing heartburn and chest pain. He describes the pain as burning in nature, and unrelated to eating. For the past week, his interest in things has decreased, and he has been more tired than usual. He has lost almost 40 lbs (18kg) in the last 6 months. He used to smoke 6-10 cigarettes daily, but he quit 4 years ago. He drinks alcohol occasionally. He takes ranitidine for his heartburn. His father died at the age of 67 from lung cancer. His vital signs are stable. Physical examination is unremarkable. The chest x-ray result is within normal limits. What is the best next step in the management of this patient?
A. Bronchoscopy
E. Test and eradicate Helicobacter pylori infection
D. Give omepra zole and follow-up in 2 months
C. Barium swallow followed by endoscopy
B. CT scan of the chest with and without contrast
136. Elizabeth, a 13-year-old girl, comes with complaints of new onset seizures. She has morning headaches that go away after vomiting. She also has history of colonic polyps, for which she is undergoing work-up. Her family history is significant for her mother having problems with polyps. (She underwent proctocolectomy.) Initial non-contrast T1-weighted MRI shows a large, heterogeneous, hypointense mass in the white matter of the right temporal lobe and extending into the parietal and occipital lobes. The lower signal area within the mass suggests tissue necrosis. What is the most likely diagnosis in this patient?
A. Multiple hamartoma syndrome
E. Cronkhite-Canada syndrome
D. Peutz-Jeghers syndrome
C. Turcot's Syndrome
B. Gardner's Syndrome
137. A 22-year-old woman comes to the office for the evaluation of a breast mass which she discovered while taking a shower 2 months ago. She experiences severe pain in this mass during her menses. She looks very anxious because her 45-year-old friend was diagnosed with breast cancer last year, and who "now has all sorts of medicines that have made her lose her hair." She has no other problems. She has never been pregnant. She is an occasional smoker, and drinks 3-4 beers a week. There is no family history of breast cancer. Her vital signs are stable. Physical examination reveals a 4 x 5 x 6 cm firm, moveable, rubbery mass in her left breast. Ultrasound shows a cystic mass. Needle aspiration yields clear fluid, after which the mass disappears. What is the best approach in the management of this patient?
A Send the fluid for cytology
E. Breath CT scan
D. Order a mammogram to look for other lesions
C. Observe for 4 weeks
B. Perform a core biopsy
138. A 28-year-old male comes for complete physical examination for a new job he is starting next week. He is healthy and has no complaints. He smokes 1 pack/day cigarettes for the last 10 years. He drinks 4 oz of alcohol daily. His mother has hypertension and father has heart problems. Vitals signs are with in normal limits. Physical examination is within normal limits except for a painless, hard mass in left testicle. Ultrasound shows high likelihood of a testicular tumor. What is the next best step in management?
A. Observe and recheck the mass after one month
E. Radical orchiectomy
D. Fine needle aspiration cytology
C. Trans-scrotal biopsy
B. Platinum based chemotherapy
139. A 50-year-old woman comes to the office and complains of right shoulder pain which radiates to her hand. She has had cough for many weeks, and feels "more tired than the usual." In addition, her fingers are always swollen, and she now finds it difficult to walk because her knees give way. She has had rheumatoid arthritis for the past 10 years and is used to having pain in her joints; however, she believes that this pain is not due to her arthritis. She takes celecoxib for rheumatoid arthritis. She admits to smoking one pack of cigarettes daily for the past 25 years and to drinking one odd beer every night. All her family members have crippling rheumatoid arthritis. Her vital signs are stable. She is afebrile. Physical examination reveals drooping of the right eyelid and miosis. What is the best next step in the management of this patient?
A. CT scan of head and neck
E. Nerve conduction study
D. Chest x-ray
C. Steroid therapy
B. X-ray of the shoulder
140. A 54-year-old male comes to the emergency department with complaints of cough and bloody sputum. He used to smoke 2 packs of cigarettes daily for 22 years, but states that he quit last month. He also complains of weight loss, anorexia, constipation, increased thirst, and easy fatigability, which he attributes to depression. He lost his wife 4 months ago and "life never felt the same after that." He is sure that he cannot have cancer because he does not smoke anymore. His vital signs are stable. He appears slim, pale, slightly irritable, and short of breath. The laboratory studies and chest x-ray results are as follows: Sodium 144 mEq/dL Potassium 4.3 mEq/dL Chloride 98 mEq/dL Bicarbonate 21 mEq/dL Calcium 14.5 mg/dl BUN 48 mg/dl Creatinine 2.0 mg/dl Chest x-ray hilar mass in the left lung While in the ED, he becomes more somnolent and vomits twice. What is the best next step in the management of this patient?
A. IV furosemide
E. IV pamidronate
D. Emergency hemodialysis
C. IV normal saline
B. CT scan of the head
141. A 75-year-old Caucasian male who was diagnosed with carcinoma of the prostate presents to ER with worsening back pain for the past 2-3 days. He never had this pain before. He denies any weakness of the legs. On examination, his muscle power in the lower extremities is 4.5/5 and has brisk reflexes. Rectal sphincter tone is weak. He has point tenderness over the L5 and S1 region. His vital signs are, BP: 122/80 mm Hg, PR 80/min, RR 16/min and Temperature 37C (98F). What is the most appropriate next step in management of this patient?
A. Radiotherapy.
E. CT myelogram.
D. Decompression surgery of spine.
C. Immediate MRI of spine
B. Intravenous dexamethasone.
142. A 72-year-old Caucasian man presents to your office complaining of severe fatigue. He says that five months ago he was able to climb four flights of stairs without shortness of breath, but now he has to rest after two. His appetite has decreased, but he denies any abdominal discomfort or black stool. Physical examination reveals firm, enlarged cervical and supraclavicular lymph nodes. A soft I/VI grade systolic murmur is heard along the left sternal border. Abdomen is soft and non-tender. His liver span is 10 cm and the spleen is palpated 4 cm below the left costal margin. His blood hemoglobin level is 7.5 mg/dl. Which of the following is the most likely cause of this patient's anemia?
A. Iron deficiency
E. Red blood cell membrane defect
D. Glucose-6-phosphate dehydrogenase deficiency
C. Bone marrow infiltration
B. Folate deficiency
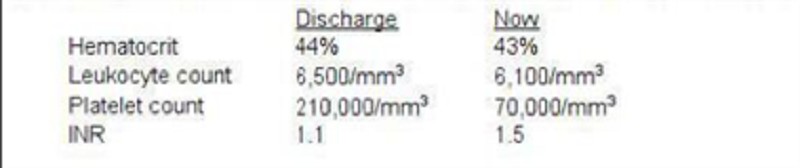
143. A 55-year-old woman complains of right leg swelling and tenderness following an international flight. A venous scan of the right lower extremity showed thrombosis of the right popliteal vein. She is sent home with oral warfarin and subcutaneous enoxaparin. One week later, she returns to the office for a follow-up appointment. Laboratory studies at the time of discharge and now are shown below: This patient's current condition predisposes her to which of the following?
A. Acute interstitial nephritis
E. Fat embolism
D. Pneumothorax
C. Hemarthrosis
B. Arterial thrombosis
144. A 41-year-old woman comes to the office for the evaluation of a lump on her left breast. She feels, "generally well," and denies having any medical problems. She takes a multivitamin and Tums daily. She stopped smoking after getting married 21 years ago. She drinks wine only on weekends. Her only surgery was a bilateral tubal ligation last year, after giving birth to her fourth child. Physical examination of the left breast reveals a 4 cm lump at the 11 o'clock position and two axillary nodes on the left side. Mammography shows irregular micro-calcifications. The result of the FNA is suggestive for infiltrating ductal carcinoma. Which of the following is the single most important prognostic factor in this patient?
A. TNM staging
E. Irregular micro calcifications in mammogram
D. Histological grade of the tumor
C. Her-2/neu oncogene expression
B. Estrogen and progesterone receptor status
145. A 22-year-old African American male suffering from sickle cell anemia presents in the emergency department with a sustained painful penile erection for the last 4 hours. Previously, he had one episode of acute chest syndrome that was treated with oxygenation, hydration and blood transfusion. His pulse is 76/min, respirations are 16/min, blood pressure is 115/76 mm Hg, and temperature is 37C (98.6F). Examination of all his systems is unrevealing. What is the best next step in the management of this patient?
A. Observation
E. Hydroxyurea
D. Surgical intervention
C. Exchange transfusion
B. Hyperbaric oxygen therapy
146. A 29-year-old woman comes to the office of a primary care physician complaining of pain in her right knee for the last 3 months. The pain is getting progressively worse and is not moving anywhere. She has tried ibuprofen but found little comfort. She is a housewife and unable to do household work because of this pain. She does not smoke nor drink and has hypertension well controlled by hydrocholorothiazide. Her vitals are stable and she is afebrile. On examination her right knee is a little swollen and tender with reduced range of motion. On x-ray, there is soap-bubble appearance in the epiphysis of distal femur. What is the next best step in the management of this patient?
A. Refer to an orthopedic surgeon
E. Do rheumatoid factor and anti-nuclear antibody
D. Start antibiotics
C. Order bone scan
B. Perform biopsy in the office
147. A 34-year-old male who recently emigrated from Asia comes to the clinic and complains of a two-month history of exertional shortness of breath and easy fatigability. He has been taking isoniazid and rifampin for his tuberculosis, which was diagnosed four months ago. Due to his religious beliefs, he completely turned into a vegetarian for the last year. Physical examination reveals severe pallor. Peripheral smear shows macrocytosis with hypersegmented polymorphonuclear neutrophils. His WBC and platelet counts are within normal limits. This patient's most likely problem is due to which of the following?
A. B 12 deficiency because of the vegetarian diet
E. Chronic myeloid leukemia
D. Myelodysplastic syndrome
C. Drug-induced 8 12 deficiency
B. B 12 deficiency because of the pernicious anemia
148. A 54-year-old male comes to the physician's office because of chronic cough and recent bloody sputum. He used to smoke 2 packs of cigarettes daily for 22 years, but he quit last month. His other symptoms are weight loss, anorexia, constipation, increased thirst, and easy fatigability. He thinks that he is depressed because his wife died 4 months ago and "life never felt the same after that." On examination, he is a slim man who appears pale. His vital signs are stable, although he appears a little irritable and short of breath. Laboratory and radiologic studies reveal: Sodium 144 mEq/dL Potassium 4.3 mEq/dL Chloride 98 mEq/dL Bicarbonate 21 mEq/dL Calcium 11.5 mg/dl BUN 28 mg/dl Creatinine 0.8 mg/dl Chest x-ray hilar mass in the left lung. Biopsy of the mass would most likely reveal?
A. Tuberculosis
E. Adenocarcinoma of the lung
D. Sarcoidosis
C. Oat cell carcinoma of the lung
B. Squamous cell carcinoma of the lung
{"name":"Hematology& Oncology ( USMLE)", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"Test your knowledge and understanding of hematology and oncology with our comprehensive quiz designed specially for USMLE candidates. This quiz covers a range of clinical scenarios and intricate details that challenge your diagnostic and management skills.Enhance your learning and prepare for your exams with:30 carefully crafted questionsReal-world clinical casesImmediate feedback on your answers","img":"https:/images/course1.png"}
More Quizzes
New Part 5 (1020-1056) nana 1
100500
USMLE_Diagnosis XII
100500
Beer Logos
1050
Where are you in 20 years
210
How Well Do You Know Pink? Take the Pink Trivia
201047493
Modernist Writers: Can You Ace Literary History?
201049576
Discover If You Can Ace the Gifts of the Holy Spirit Test
201023986
Can You Recall the Events of Romeo and Juliet in Order?
201023986
Discover Your Dating Personality - Play Free Now
201033068
Edward Cullen & Jacob Black: Find Your Perfect Match
201033962
Manage Front Office Operations
201037021
Executive Branch: Test Your US Government Knowledge
201034915