
Surgery USMLE (301-400)

301. A 62-year-old woman presents to the physician’s office with complaints of constipation. She has had constipation for the last 6 months, which has worsened over the last month, associated with mild bloating. She noted that her stool has become “pencil thin” in the last month, with occasional blood, but she continues to have bowel movements daily. Past history is unremarkable. Examination reveals normal vital signs and heart and lung examination. Abdominal examination reveals mild fullness, especially in the lower quadrants. Rectal examination shows no rectal masses, but the stool is hematest positive. A barium xray is obtained, and one view is shown in Figure 6-11. Which of the following is the most appropriate next step in management ?
Proctoscopy and passage of a rectal tube
Proctoscopy and biopsy
Colonoscopy
Endoscopic dilation of the stricture
NPO, IV fluids, and antibiotics
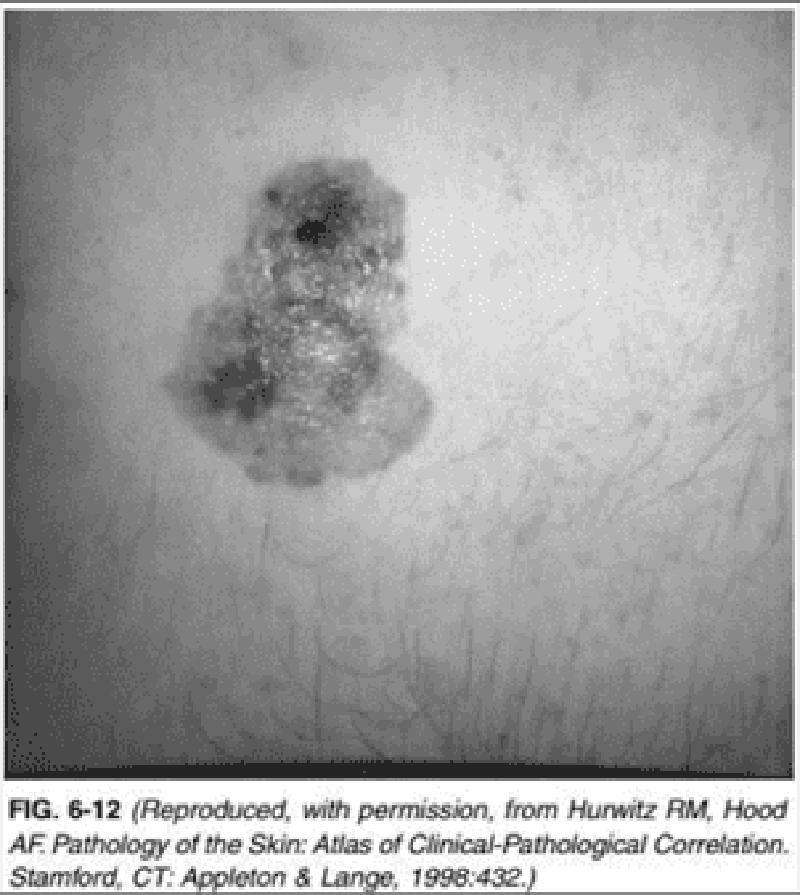
302. A 45-year-old man presents to the physician’s office for evaluation of a skin lesion on his abdomen. He states that the lesion has been present for 1 year, but has recently enlarged over the last 2 months. The mass is nontender, and he is otherwise asymptomatic. Past history is unremarkable. Examination reveals a 3-cm, pigmented, irregular skin lesion located in the left lower quadrant of the abdomen, as shown in Figure 6-12. Heart, lung, and abdominal examination are normal. There are no palpable cervical, axillary, or inguinal lymph nodes. Chest x-ray and liver function tests are normal. Which of the following is the most likely diagnosis?
Squamous cell carcinoma
Basal cell carcinoma
Merkel cell carcinoma
Melanoma
Keratoacanthoma
303. A 55-year-old man with recent onset of atrial fibrillation presents with a cold, numb, pulseless left lower extremity. He is immediately taken to the operating room for an embolectomy of the left popliteal artery. Which additional procedure should be performed along with the embolectomy?
Electromyography (EMG) of the leg
Measurement of anterior compartment pressure in the leg
Fasciotomy of the anterior compartment in the leg
Fasciotomy of all the compartments in the leg
Application of a posterior splint to the leg
304. A 58-year-old man presents with pain in the left leg after walking more than one block that is relieved with rest. On physical examination, distal pulses are not palpable in the left foot and there is dry gangrene on the tip of his left fifth toe. An ankle-brachial index on the same side is 0.5. Which of the patient’s symptoms or signs of arterial insufficiency qualifies him for reconstructive arterial surgery of the left lower extremity?
Ankle-brachial index less than 0.7
Rest pain
Claudication
Absent palpable pulses
Toe gangrene

305. A 62-year-old man comes to the emergency department because of severe abdominal pain. He states that he suddenly felt weak, diaphoretic, and had no energy. He is a smoker and has hypertension. His blood pressure on initial examination was 110/70 mm Hg. Physical examination shows a diffusely tender abdomen. During CT scan he becomes pale and drowsy. CT scan is shown below. Repeat examination shows a man with anxiety and a blood pressure of 80/50 mm Hg and pulse of 110/min. Which of the following is the most appropriate next step in management?
Exploratory abdominal surgery
Obtain ultrasound
Check amylase and lipase
Laparoscopy
Drain fluid from the abdomen
306. An 84-year-old man is brought to the emergency department because of 1 hour of severe back pain. He also had syncope that lasted <1 minute. Before arriving at the hospital, he had an episode of gross hematuria, which he has never had before. He also complains of some shortness of breath. He denies chest pain, cough, nausea, vomiting, headache, and neck pain. His blood pressure is 72/55 mm Hg and pulse is 112/min and regular. His pulse oximetry shows 92% on room air. His ECG shows sinus tachycardia with prominent horizontal ST segment depression in the anterior chest leads. Which of the following is the most likely diagnosis?
Abdominal aortic aneurysm rupture
Acute mesenteric ischemia
Acute myocardial infarction
Massive pulmonary embolism
Nephrolithiasis with renal colic
307. A 23-year-old man known to have neurofibromatosis, type 1 (von Recklinghausen's disease), presents with a left lower quadrant abdominal mass and signs of neurologic deficits in his left leg. In the ensuing workup, it is determined that he has higher than normal values of catabolites of epinephrine and norepinephrine in a 24-hour urinary collection. He is currently normotensive. Before invasive steps are taken to biopsy and eventually remove his left lower quadrant abdominal mass, which of the following is the most appropriate next step in management?
CT scan of the head looking for meningiomas
MRI of his adrenal glands
MRI of the acoustic nerves
Radionuclide scans from the neck to the pelvis looking for extra-adrenal pheochromocytomas
Radiation therapy to the left lower quadrant abdominal mass
308. A car is involved in a head-on collision. The driver, who is sober and wearing his seat belt, explains that he clearly saw his drunk, unrestrained front seat passenger hit the windshield with his face and the dashboard with his knees. Examination of the passenger indeed shows multiple facial lacerations, but because of his intoxication he cannot explain where else he might be hurting. He is neurologically intact, and his cervical spine x-ray films are normal. Additional injury, representing a potential orthopedic emergency, is not obvious but is suspected. Therefore, an x-ray film of which of the following areas should most likely be obtained?
Both patellas
Both hips
The jaw
The lumbar spine
The skull
309. A 35-year-old woman presents to the clinic for a discussion on breast cancer risk. Her family history is pertinent for a grandmother who died of breast cancer at age 53, a mother who died of premenopausal breast cancer, and one of three sisters with breast cancer diagnosed at age 42. The sister with breast cancer underwent genetic testing and was found to have a BRCA1 mutation. Subsequently, the 35-year-old woman underwent genetic testing and was found to be a carrier of the same deleterious BRCA1 mutation. Which of the following ranges represents the lifetime risk for breast cancer that should be quoted for this patient?
0–30%
10–40%
20–50%
50–80%
70–100%
310. A 35-year-old woman presents to the clinic for a discussion on breast cancer risk. Her family history is pertinent for a grandmother who died of breast cancer at age 53, a mother who died of premenopausal breast cancer, and one of three sisters with breast cancer diagnosed at age 42. The sister with breast cancer underwent genetic testing and was found to have a BRCA1 mutation. Subsequently, the 35-year-old woman underwent genetic testing and was found to be a carrier of the same deleterious BRCA1 mutation. For this patient, which of the following strategies represent an accepted management option for her high-risk status?
Yearly self-breast examinations
Semiannual mammography
Bilateral breast irradiation
Prophylactic unilateral mastectomy
Chemoprevention with tamoxifen
308. A 38-year-old woman presents to the physician because of right upper quadrant pain associated with nausea and vomiting for the past 12 hours. She has had similar pain previously, usually precipitated after the ingestion of fatty foods. However, past episodes have always resolved within one to two hours. She has type 2 diabetes mellitus, hypertriglyceridemia, and hypercholesterolemia. Her current medications include metformin, fenofibrate, and a statin. Her temperature is 38.3° C (101° F), blood pressure is 130/70 mm Hg, pulse is 98/min, and respirations are 20/min. Her BMI is 32 kg/m2. Examination shows right upper quadrant tenderness. Abdominal ultrasound reveals gallstones, a thickened gallbladder wall with edema, and a normal common bile duct. Her alkaline phosphatase level is normal. Which of the following is the most appropriate next step in the management of this patient?
Cholecystectomy within 72 hours
Endoscopic retrograde cholangiography
Delayed cholecystectomy
HIDA scan
Percutaneous trans-hepatic drainage
312. A 54-year-old man comes to the physician because of edema of his right ankle. He reports heaviness and cramping in the same leg that is worse after a long day at work. The swelling is usually reduced significantly when he wakes up in the morning and worsens progressively throughout the day. He denies any other symptoms. He has no significant medical problems except hypertension, for which he takes atenoloL His temperature is 36.7° C (98° F), blood pressure is 120/76 mm Hg, pulse is 80/min and respirations are 16/min. JVP is normaL Lungs are clear to auscultation. There are no murmurs. There is no hepatosplenomegaly. Examination shows edema of the right ankle. Doppler examination of the leg shows no evidence of thrombosis. Which of the following is the most likely cause of his edema?
Lymphatic obstruction
Impaired cardiac contraction
Reduced diastolic filling of the heart
Increased urinary loss of protein
Venous valve incompetence
313. A 40-year-old, obese, white woman, mother of five children, gives a history of repeated episodes of right upper quadrant abdominal pain. The pain is brought about by the ingestion of fatty foods and is relieved by the administration of anticholinergic medications. The pain is colicky, radiates to the right shoulder and around to the back, and is accompanied by nausea and occasional vomiting. The patient has no pain at this time, but is anxious to avoid further episodes. She is afebrile, and physical examination is unremarkable. Which of the following is the most appropriate next step in management?
Sonogram of the biliary tract and gallbladder
Upper gastrointestinal series with barium
Antibiotics, IV fluids, and nothing by mouth
Endoscopic retrograde cholangiopancreatogram (ERCP)
Exploratory surgery
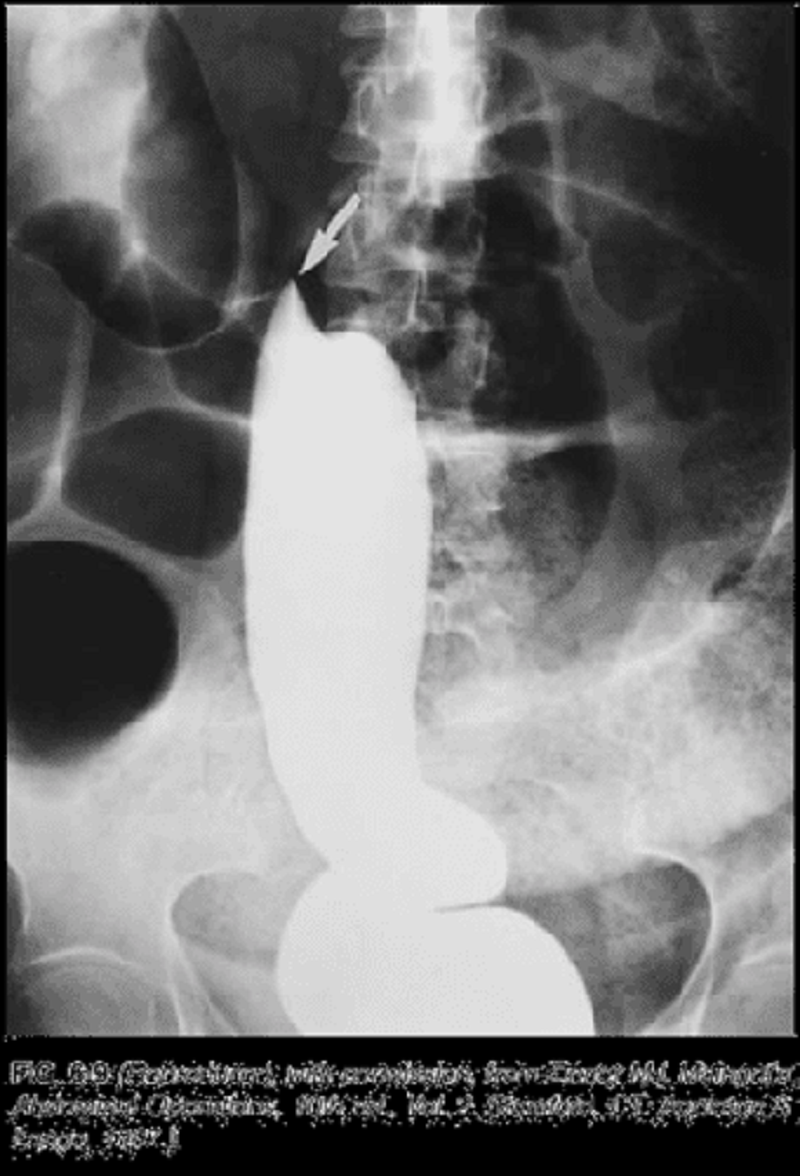
314. A 68-year-old man presents to the physician’s office complaining of progressive dysphagia over the last 3 months associated with mild chest discomfort. He reports a 15-lb weight loss, a 30 pack-year smoking history, and occasional alcohol intake. The physical examination, including vital signs, is unremarkable. A chest x-ray was normal, and a barium esophagogram shows an irregular filling defect in the distal third of the esophagus with distortion and narrowing of the lumen. Which of the following is the most likely diagnosis?
Esophagitis with stricture
Esophageal carcinoma
Lung carcinoma with invasion into the esophagus
Lymphoma
Achalasia
315. A 68-year-old man presents to the physician’s office complaining of progressive dysphagia over the last 3 months associated with mild chest discomfort. He reports a 15-lb weight loss, a 30 pack-year smoking history, and occasional alcohol intake. The physical examination, including vital signs, is unremarkable. A chest x-ray was normal, and a barium esophagogram shows an irregular filling defect in the distal third of the esophagus with distortion and narrowing of the lumen. Which of the following is the most appropriate next step in management?
CT scan
Esophagoscopy
MRI scan
Surgical resection
Bronchoscopy
316. In this patient, a benign gastric ulcer was found, and he was placed on a proton-pump inhibitor and triple antibiotics for Helicobacter pylori. He returns to the physician’s office 3 months later with similar complaints and, on re-evaluation, the gastric ulcer was found to persist. Which of the following is the most appropriate next step in management?
A second trial of proton-pump inhibitors with triple antibiotics and re-evaluation in 2 months
A trial of H2 blockers with triple antibiotics and re-evaluation in 2 months
A trial of sucralfate and re-evaluation in 2 months
Surgical management
A trial of prostaglandins and re-evaluation in 2 months

317. In a 6-month-old previously healthy male infant, an abnormality is revealed during a routine diaper change, as illustrated in Figure 6-19. The parents have noted this finding on and off on several occasions over the last month. On each occasion, the child has been feeding well, and is content and playful. We decided to do surgical repair. Several weeks later, the child presents to the emergency department with a 4-hour history of irritability. He has had one episode of nonbilious vomiting and has refused to breast-feed. In the emergency department, the infant appears inconsolable. He is afebrile, and his abdomen is mildly distended but soft. On removal of his diaper, the same abnormality is documented (see Figure 6-19). Which of the following is the most appropriate management at this time?
Urgent surgical exploration
Systemic antibiotics
Elective surgical repair
Sedation with manual reduction and arrangements for elective surgical repair
Sedation with manual reduction, admission, rehydration, and surgical repair within 24–48 hours
318. A 29-year-old man presents with a 2-day history of severe left-sided scrotal pain and swelling. He is sexually active and has had "many" sexual partners. His temperature is 38.2 C (100.8 F), blood pressure is 120/70 mm Hg, and pulse is 80/min. Examination shows unilateral intrascrotal tenderness and swelling. Testicular support makes the pain less intense. Which of the following is the most likely diagnosis?
Epididymitis
Prostatitis
Testicular torsion
Urethritis
Varicocele
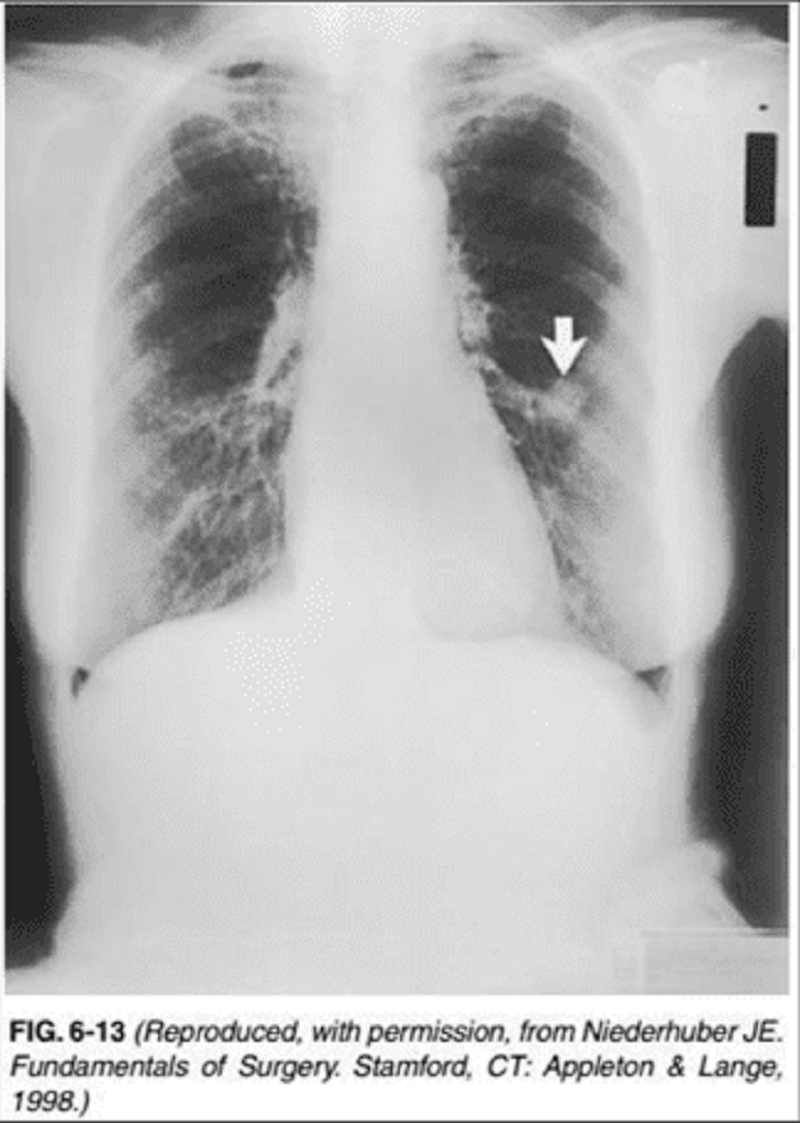
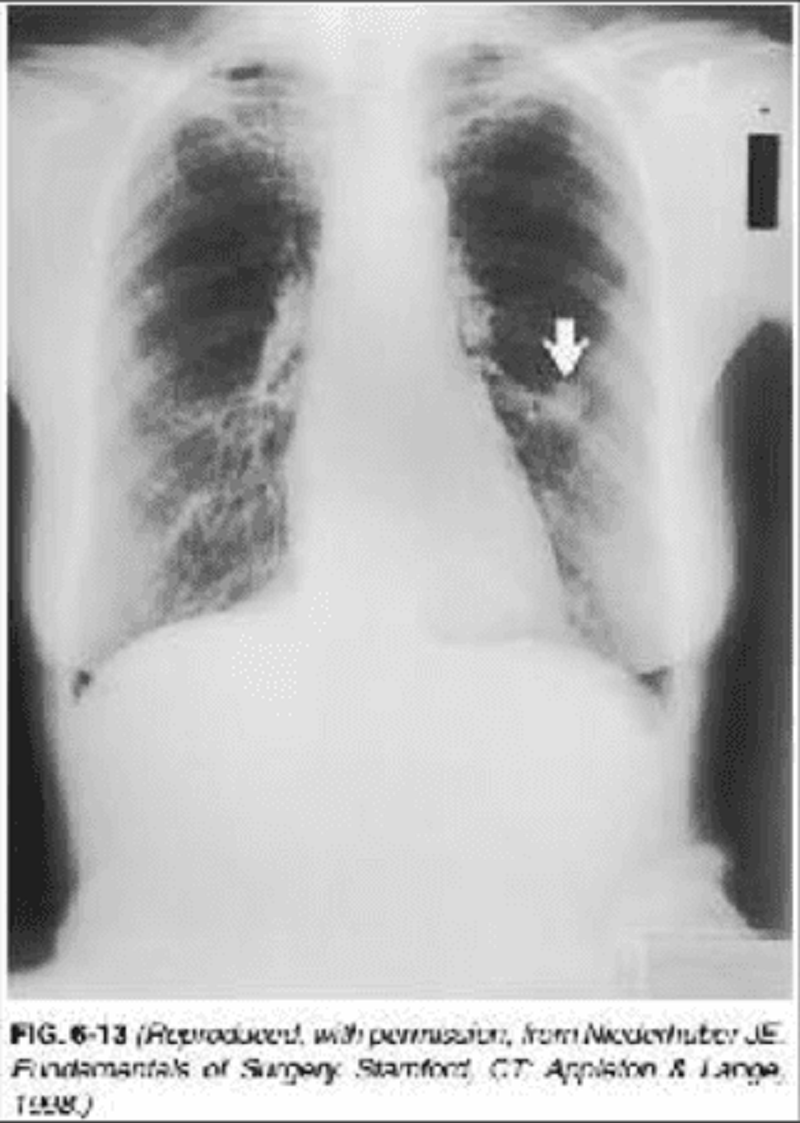
319. A 65-year-old woman presents to the physician’s office for her yearly physical examination. She has no complaints except for a recent 10-lb weight loss. Past history is pertinent for a 40 pack-year smoking history, hypertension, asthma, and hypothyroidism. Examination reveals a thin woman with normal vital signs and unremarkable heart and abdominal examinations. Lung examination reveals mild wheezing and a few bibasilar rales. A chest x-ray is obtained and is shown in Figure 6-13. A chest x-ray obtained 3 years ago was normal. Yearly laboratory tests including a CBC, electrolytes, and lipid panels are normal. Which of the following is the most likely diagnosis?
Small cell lung cancer
Tuberculosis
Nonsmall cell lung cancer
Hamartoma
Abscess
320. A 65-year-old woman presents to the physician’s office for her yearly physical examination. She has no complaints except for a recent 10-lb weight loss. Past history is pertinent for a 40 pack-year smoking history, hypertension, asthma, and hypothyroidism. Examination reveals a thin woman with normal vital signs and unremarkable heart and abdominal examinations. Lung examination reveals mild wheezing and a few bibasilar rales. A chest x-ray is obtained and is shown in Figure 6-13. A chest x-ray obtained 3 years ago was normal. Yearly laboratory tests including a CBC, electrolytes, and lipid panels are normal.
Percutaneous needle biopsy
CT scan
Pulmonary function tests
Mediastinoscopy
Bronchoscopy
321. A 75-year-old woman with history of angina is admitted to the hospital for syncope. Examination of the patient reveals a systolic murmur best heard at the base of the heart that radiates into the carotid arteries. Electrocardiogram (ECG) is notable for left ventricular hypertrophy with evidence of left atrial enlargement. ECG reveals an aortic valve area of 0.7 cm2. What is the most appropriate next step in her management?
Medical management with a nitrate and an angiotensin-converting enzyme inhibitor
Bilateral carotid endarterectomies
Percutaneous coronary artery angioplasty and stenting
Coronary artery bypass surgery
Aortic valve replacement
322. A 68-year-old man is diagnosed with lung cancer. In preparation for pulmonary resection he undergoes pulmonary function tests. Which of the following results indicate a favorable prognosis?
Elevated PCO2
Forced expiratory volume in 1 second (FEV1) more than 60% of predicted
Carbon monoxide diffusing capacity (DLCO) less than 40%
Low FEV1/FVC (forced vital capacity)
Normal FEV1/FVC
323. A 24-year-old man comes to the physician because of 1 week of abdominal pain. It is localized in the right lower quadrant and somewhat exacerbated by motion. Over the past 2 days, it has radiated to the back. He initially had two episodes of vomiting but now just has decreased appetite. He had one episode of diarrhea 1 day ago. He denies urinary frequency. His other medical problems include mild intermittent asthma and gastroesophageal reflux disease. He traveled to Mexico for 5 days 1 month ago and did not have any gastrointestinal symptoms during his stay there. His mother was diagnosed with colon cancer at the age of 49 years. His temperature is 38.2°C (100.8°F), blood pressure is 122/77 mm Hg, and pulse is 109/min and regular. Physical examination reveals prominent tenderness in the right lower quadrant, without rebound. Flexion of the right hip against resistance elicits significant abdominal pain. Laboratory results show: WBC count 16,000/mm' Hemoglobin 14.2 g/dl Platelet count 620,000/mm' Potassium 4.5 mEq/L Creatinine 1.0 mg/dl Which of the following is the most likely diagnosis?
Appendiceal perforation
Colonic malignancy
Complicated pyelonephritis
Inflammatory bowel disease
Parasitic colitis
324. A pediatrician's office gets a phone call from a frantic mother. Her 7-year-old daughter was playing under the sink and accidentally spilled Liquid Plumber (a strong, corrosive alkaline drain cleaner) all over her arms and legs. The nurse on the phone can hear the girl screaming in the background. Which of the following are the most appropriate instructions to give the mother?
Cover the burned areas with triple antibiotic ointment until the girl can be seen at the office
Get the girl into the shower right away and keep the water running over her for 30 minutes before bringing her to the emergency department
Get the girl to the emergency department as soon as possible
Wash the burned areas with diluted vinegar and bring the girl to the office
Wrap the burned areas in sterile dressings before bringing the girl to the emergency department
325. A 59-year-old man sustains blunt trauma in an automobile accident, resulting in multiple intra-abdominal injuries. Surgery for the repair of these injuries takes several hours and requires multiple blood transfusions and infusions of Ringer's lactate. Before all the operative steps are completed, the patient develops a significant coagulopathy, a core body temperature less than 34 C (93.2 F), and refractory acidosis. The anesthesiologists are administering fresh frozen plasma and platelet packs. Which of the following is the most appropriate next step in management for the surgeon?
Provide hemostasis by liberal use of electrocoagulation
Wash the abdomen with warm saline and continue to operate
Complete the operation as soon as possible and do a formal abdominal closure
Pack the bleeding surfaces and close the abdomen temporarily with towel clips
Abort the operation and leave the abdomen open, covering the bowel with mesh
326. A previously healthy 19-year-old man presents to the emergency department with a penetrating wound to the right neck. There were reports of bleeding at the scene. The patient is talking, complaining of pain at the injury site and pain with swallowing. On examination, he has a normal respiratory rate, clear air entry on auscultation, blood pressure of 120/70 mmHg, and heart rate of 95 beats/min. There is a penetrating right neck wound in zone 2 (between the clavicle and the lower part of the mandible), with a surrounding hematoma. On probing, there is violation of the platysma. Which of the following is the best next step in the management of this patient?
Intubation and observation in the ICU
Admission to the ICU for close observation without intubation
Observation in the ICU only if carotid angiogram is normal
Observation in the ICU only if carotidangiogram, contrast esophagram, and bronchoscopy are normal
Neck exploration
327. A 45-year-old man is brought to the emergency department after being involved in an automobile crash. He is alert and oriented, with a normal neurologic examination. His respiratory rate is 20/min, with clear lungs, pulse rate of 120/min, and blood pressure of 80/40 mmHg. On examination, he is noted to have a distended abdomen, with decreased bowel sounds, and a fracture of the right ankle. IV access is established, and the patient receives a rapid infusion of 2 L of saline, without changes to pulse rate or blood pressure. Which of the following is the most appropriate next step in his management?
Abdominal CT scan
Insertion of a Swan-Ganz catheter
Exploratory laparotomy
Focused abdominal sonography for trauma (FAST)
Diagnostic peritoneal lavage

328. A 56-year-old woman presents to her primary care physician for a routine checkup. She states that she was recently hospitalized for surgery and was told she had some metal placed in a large blood vessel to prevent blood clots from moving to her lungs. An abdominal x-ray is shown here. Which of the following is the most appropriate indication for placement of this device?
Recurrent pulmonary embolus despite adequate anticoagulation therapy
Axillary vein thrombosis
Pulmonary embolus due to DVT of the lower extremity that occurs 2 weeks postoperatively
DVT in a patient with patient with metastatic carcinoma
Pulmonary embolus in a patient with metastatic carcinoma
329. A 55-year-old man presents to the emergency department at 5 a.m. Complaining of vomiting blood. After binge drinking last night, the patient began to vomit repeatedly. After a number of episodes, the patient noted blood in the vomitus, followed by a melanotic stool 5 hours later. His past history is pertinent for ethanol abuse and a 40 pack-year smoking history. Vital signs reveal a BP of 100/60 mmHg, pulse rate of 95/min, respiratory rate of 12/min, and temperature of 97°F. Examination reveals a thin man with normal chest, cardiac, and abdominal findings. Rectal examination reveals heme-positive stool. Laboratory data show normal electrolytes and a hematocrit of 30. A chest x-ray is unremarkable. Volume resuscitation, gastric lavage, and NG tube decompression are initiated. Which of the following is the most appropriate diagnostic test?
Barium esophagogram
Water-soluble contrast esophagogram
Esophagoscopy
CT scan
Angiogram
330. A 70-year-old man with a 50 pack-year history of smoking presents with a 6-week history of intermittent, painless, gross hematuria and urinary frequency. There are no masses palpable on abdominal examination, and rectal examination is normal. Urinalysis confirms the presence of hematuria, and urine culture is negative. Which of the following is the most appropriate initial diagnostic evaluation of this patient?
Plain abdominal radiographs and an intravenous pyelogram (IVP)
Voiding cystourethrogram
Cystourethroscopy
Abdominal ultrasound
Urine for cytology
331. A 70-year-old man with a 50 pack-year history of smoking presents with a 6-week history of intermittent, painless, gross hematuria and urinary frequency. There are no masses palpable on abdominal examination, and rectal examination is normal. Urinalysis confirms the presence of hematuria, and urine culture is negative. The initial diagnostic evaluation does not reveal any abnormalities. Which of the following is the best next step in the diagnostic workup?
An abdominal CT scan
Cystourethroscopy and urinary cytology
A transrectal ultrasound
Exploratory laparoscopy
Re-evaluation in 2–4 weeks, with repeat urinalysis and urine culture
331. A 7-week-old, breast-fed, term infant presents with increasing jaundice, abdominal distention, and abnormal stools (Figure 6-20). Liver function tests demonstrate a conjugated hyperbilirubinemia, mildly elevated transaminases, and an elevated gamma-glutamyl transpeptidase. TORCH (congenital infection complex, including toxoplasmosis, rubella, cytomegalovirus, and hepatitis) serology and screening for inborn errors of metabolism are negative. As part of the diagnostic evaluation, the most sensitive imaging study in this clinical setting would be which of the following?
Radioisotope scanning
Radioisotope scanning with pre-imaging phenobarbital administration
Abdominal ultrasound
CT scan of the abdomen
MRI scan of the abdomen
333. Two days after admission to the hospital for a myocardial infarction, a 65-year-old man complains of severe, unremitting midabdominal pain. His cardiac index is 1.6. Physical examination is remarkable for an absence of peritoneal irritation or distention despite the patient’s persistent complaint of severe pain. Serum lactate is 9 mmol/L (normal is < 3 mmol/L). Which of the following is the most appropriate next step in this patient’s management? a. Perform computed tomography.
Perform computed tomography.
Perform mesenteric angiography.
Perform laparoscopy.
Perform flexible sigmoidoscopy to assess the distal colon and rectum.
Defer decision to explore the abdomen until the arterial lactate is greater than 10 mmol/L.
334. A 55-year-old man comes to the emergency department because of severe retrosternal chest pain that suddenly started a few hours ago. He has been having some chest pain and epigastric burning for the past few days but says that the current pain is different. His other medical problems include nonischemic cardiomyopathy for which he takes furosemide, carvedilol, spironolactone, lisinopril, and potassium chloride. He also has HIV infection but has chosen not to take any medication related to this diagnosis. His temperature is 38.9° C (102° F), blood pressure is 110/65 mm Hg, pulse is 110/min, and respirations are 22/min. Examination shows that he is in obvious distress secondary to pain. His lungs are clear to auscultation. The remainder of the examination shows no abnormalities. His ECG is within normal limits. Chest x-ray shows a widened mediastinum and some mediastinal air. Which of the following is the most appropriate next step in the management of this patient?
Aspirin, clopidogrel, and repeat ECG in 30 minutes
Contrast esophagography
Oral omeprazole and antacids
Transesophageal echocardiography
Upper gastrointestinal endoscopy
335. A 36-year-old woman presents with palpitations, anxiety, and hypertension. Workup reveals a pheochromocytoma. Which of the following is the best approach to optimizing the patient preoperatively?
Fluid restriction 24 hours preoperatively to prevent intraoperative congestive heart failure
Initiation of an α-blocker 24 hours prior to surgery
Initiation of an α-blocker at 1 to 3 weeks prior to surgery
Initiation of a β-blocker 1 to 3 weeks prior to surgery
Escalating antihypertensive drug therapy with β-blockade followed by α-blockade starting at least 1 week prior to surgery
336. A 35-year-old woman is involved in a motor vehicle crash, sustaining a severe pelvic fracture, with disruption of the pelvic ring. In the trauma resuscitation room, she is confused and tachypneic, with a blood pressure of 90 mmHg systolic and a heart rate of 130/min. Laboratory investigations include serum electrolyte analysis, revealing a sodium of 139, a chloride of 103, and a bicarbonate of 14 meq/L. This patient demonstrates which of the following?
Nonanion gap metabolic acidosis
Anion gap metabolic acidosis
Metabolic alkalosis
Respiratory acidosis
Normal serum electrolytes
337. A 35-year-old woman is involved in a motor vehicle crash, sustaining a severe pelvic fracture, with disruption of the pelvic ring. In the trauma resuscitation room, she is confused and tachypneic, with a blood pressure of 90 mmHg systolic and a heart rate of 130/min. Laboratory investigations include serum electrolyte analysis, revealing a sodium of 139, a chloride of 103, and a bicarbonate of 14 meq/L. Which of the following is the most appropriate management of this acid-based derangement?
Administration of sodium bicarbonate to correct the base deficit
Restoration of blood volume with aggressive IV fluid resuscitation
IV hydrochloric acid
Intubation and hyperventilation
This patient has no acid-based abnormality.

338. A 1-day-old infant with Down syndrome, feeding intolerance, bilious vomiting, and a double bubble on plain radiographs (Figure 6-18). Which one is the most likely diagnostic?
Congenital hypertrophic pyloric stenosis
Annular pancreas
Duodenal atresia
Midgut volvulus
Intussusception
339. A 33-year-old pregnant woman notices a persistent, painless lump in the left breast. On examination the left breast has a single mobile mass without evidence of skin changes or lymphadenopathy in the neck or axilla. An ultrasound demonstrates a solid, 1-cm mass in the upper outer quadrant of the breast. A core-needle biopsy shows invasive ductal carcinoma. The patient is in her first trimester of pregnancy. Which of the following is the most appropriate management of this patient?
Termination of the pregnancy followed by modified radical mastectomy
Immediate administration of chemotherapy followed by modified radical mastectomy after delivery of the baby
Administration of radiation in the third trimester followed by modified radical mastectomy after delivery of the baby
Total mastectomy with sentinel lymph node biopsy
Modified radical mastectomy
340. A 40-year-old woman presents with a rash involving the nipple-areola complex for the last month with associated itching. On physical examination there is crusting and ulceration of the nipple with surrounding erythema involving the areola and surrounding skin, no palpable breast masses, and no cervical or axillary lymphadenopathy. Which of the following is the most appropriate next step in the management of this patient?
Reexamine the patient in 1 month
Corticosteroid cream to the affected area
Administration of oral antibiotics
Mammogram and biopsy of the affected area
Modified radical mastectomy
341. A 54-year-old woman presents to her physician for an opinion regarding additional therapy following curative resection of recently diagnosed colon cancer. She underwent uncomplicated sigmoid resection for invasive colon cancer 4 weeks ago. The pathology revealed carcinoma invading into, but not through, the muscularis propria, with one of eight positive mesenteric nodes. There was no evidence of liver metastases at the time of operation. Preoperative chest x-ray and CT scan of the abdomen showed no evidence of distant disease. Preoperative carcinoembryonic antigen (CEA) level was normal. Past history is positive for diabetes and mild hypertension. Examination is unremarkable except for a healing abdominal incision. Which of the following is the correct stage of this patient’s colon cancer?
Stage 0
Stage I
Stage II
Stage III
Stage IV
342. A 54-year-old woman presents to her physician for an opinion regarding additional therapy following curative resection of recently diagnosed colon cancer. She underwent uncomplicated sigmoid resection for invasive colon cancer 4 weeks ago. The pathology revealed carcinoma invading into, but not through, the muscularis propria, with one of eight positive mesenteric nodes. There was no evidence of liver metastases at the time of operation. Preoperative chest x-ray and CT scan of the abdomen showed no evidence of distant disease. Preoperative carcinoembryonic antigen (CEA) level was normal. Past history is positive for diabetes and mild hypertension. Examination is unremarkable except for a healing abdominal incision. Which of the following is the most appropriate recommendation regarding adjuvant therapy?
No therapy indicated
5-fluorouracil chemotherapy
5-fluorouracil chemotherapy with leucovorin
Doxorubicin (Adriamycin) chemotherapy
Adriamycin chemotherapy with methotrexate and Cytoxan
343. A 43-year-old man develops excruciating abdominal pain at 8:23 PM (he looked at his watch when the pain "hit him"). When seen in the emergency department about 30 minutes later, he has a rigid abdomen, lies motionless on the examination table, has no bowel sounds, and is obviously in great pain, which he describes as constant and encompassing the entire abdomen. There is very severe pain when deep palpation of the abdomen is attempted in any of the four quadrants. However, the examining hand cannot make much of an indentation because of the impressive muscle guarding. When the attempt is aborted, he manifests severe rebound tenderness. X-ray films show free air under both diaphragms. Which of the following does this man most likely have?
Acute abdomen, the nature of which cannot yet be defined
Acute inflammatory process affecting an intra-abdominal viscera
Acute obstruction of an intra-abdominal viscera
Ischemic process affecting intra-abdominal organs
Perforation of the gastrointestinal tract
344. On the 5th postoperative day after abdominal surgery, a patient has been draining copious amounts of clear pink fluid from his midline laparotomy wound. A medical student removes the dressing, confirms that it is soaked, and sees a normal-appearing fresh wound with a row of skin staples in place. The student asks the patient to sit up so he can get out of bed and be helped to the treatment room for a more thorough examination. When the patient complies, the wound opens widely, and a handful of small bowel suddenly rushes out. Which of the following is the most appropriate management at this time?
Cover the bowel with dry sterile dressings and schedule urgent surgical closure
Cover the bowel with sterile dressings soaked in warm saline and rush the patient to the operating room
Irrigate the bowel with cold antiseptic solutions while awaiting urgent surgical closure
Take the patient to the treatment room and suture the skin edges together
Wearing sterile gloves, push the bowel back in and tape the wound securely
345. Several days following esophagectomy, a patient complains of dyspnea and chest tightness. A large pleural effusion is noted on chest radiograph, and thoracentesis yields milky fluid consistent with chyle. Which of the following is the most appropriate initial management of this patient?
Immediate operation to repair the thoracic duct
Immediate operation to ligate the thoracic duct
Tube thoracostomy and low-fat diet
Observation and low-fat diet
Observation and antibiotics
346. A 56-year-old woman presents for evaluation of a murmur suggestive of mitral stenosis and is noted on echocardiography to have a lesion attached to the fossa ovalis of the left atrial septum. The mass is causing obstruction of the mitral valve. Which of the following is the most likely diagnosis?
Endocarditis
Lymphoma
Cardiac sarcoma
Cardiac myxoma
Metastatic cancer to the heart
347. A 54-year-old man presents to the emergency department on transfer from another hospital at the request of the family. He was admitted to the outside hospital 2 weeks ago with abdominal pain, nausea, vomiting, and fever. He was treated with antibiotics, NG tube decompression, and TPN without significant improvement. He developed jaundice 2 days ago. His past history is pertinent for a 40 pack-year smoking history, chronic alcohol abuse, and diabetes. Examination reveals a mildly jaundiced patient with vital signs of temperature 100°F, pulse rate 95/min, and BP 110/60 mmHg. Cardiac examination is unremarkable, lung examination reveals decreased breath sounds at the bases bilaterally, and abdominal examination reveals fullness in the epigastrium with tenderness and voluntary guarding. Which one is the most likely diagnosis?
Hepatitis A
Hemolysis
Pancreatitis
Liver metastases
Cirrhosis
348. A 56-year-old woman presents to the physician’s office with complaints of a new left breast mass. She denies any pain, nipple discharge, or skin dimpling. She has a prior history of breast cysts 5 years ago, treated by aspiration at that time. Her last mammogram was at age 53. Past history is pertinent for a 30 pack-year smoking history, prior total abdominal hysterectomy bilateral salpingo-oophorectomy (TAH-BSO) at age 54 for leiomyomas, and current use of hormone replacement therapy (HRT). Family history is negative for breast disease. Examination reveals a firm, welldefined, mobile, 1.5-cm nodule in the upper outer quadrant of the left breast without any regional lymphadenopathy. Which of the following is the most appropriate next step in management?
Fine-needle aspiration (FNA) biopsy
Discontinuation of HRT and reexamination in 4–6 weeks
Breast imaging
Open surgical biopsy
Core needle biopsy
349. A 54-year-old African American man, with a history of smoking and drinking, describes progressive dysphagia that began 3 months ago. He first noticed difficulty swallowing meat; it then progressed to other solid foods, then to soft foods, and now to liquids as well. He locates the place where the food "sticks" at the lower end of the sternum. He has lost 30 pounds. Which of the following is the most appropriate first step in diagnosis?
Barium swallow
Gastrografin swallow
Esophageal manometry
Esophageal pH monitoring
Esophagoscopy

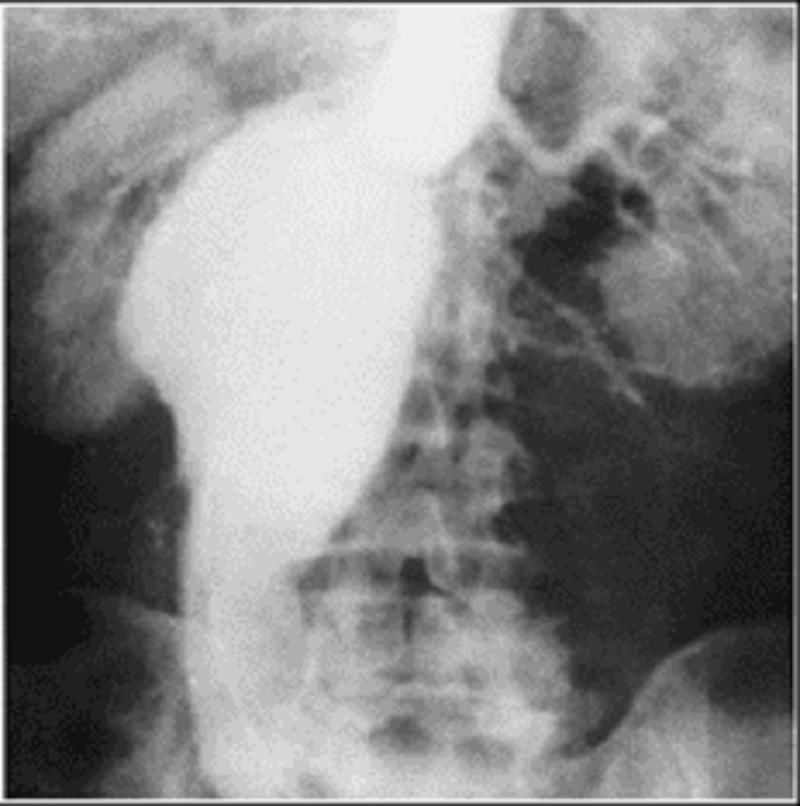
348. A 65-year-old woman presents to the physician’s office with a 6-month history of epigastric discomfort, poor appetite, and 10-lb weight loss. Past history is pertinent for hypertension, diabetes, a 30 pack-year smoking history, and occasional alcohol intake. Examination is unremarkable except for mild epigastric tenderness to deep palpation. An abdominal ultrasound reveals cholelithiasis, and one view of a UGI x-ray series is shown in Figure 6-8. Which of the following is the most appropriate next step in management?
H2 blockers with re-evaluation by UGI in 6 month
Vagotomy and pyloroplasty
Total gastrectomy
Endoscopy
CT scan
351. A 55-year-old man presents to the physician’s office for his yearly physical examination. He is asymptomatic. Past history is pertinent for hypertension. Family history is positive for breast cancer in his mother at age 70 and colon cancer in his father at age 65. His examination is unremarkable except for guiac positive stool. Barium enema shows a sigmoid colon polyp. Colonoscopy confirms a 3-cm pedunculated polyp in the sigmoid colon, and snare polypectomy is performed. Pathologic examination reveals an adenomatous polyp with a focus of invasive carcinoma in the head, with a 4-mm resection margin and no tumor noted in the stalk. Which of the following is the most appropriate next step in management?
CT scan
Magnetic resonance imaging (MRI) scan
Surgical resection of sigmoid
Observation
Regular use of nonsteroidal antiinflammatory drugs (NSAIDs)
352. A 65-year-old male cigarette smoker reports onset of claudication of his right lower extremity approximately 3 weeks previously. He can walk 3 blocks before the onset of claudication. Physical examination reveals palpable pulses in the entire left lower extremity, but no pulses are palpable below the right groin level. Non-invasive flow studies are obtained and are pictured here. What is the level of the occlusive process in this patient?
Right anterior tibial artery
Right superficial femoral artery
Right profunda femoris artery
Right external iliac artery
Right internal iliac artery
353. An elderly woman with osteoporosis falls on her outstretched hand. She comes in with a deformed and painful wrist that looks like a dinner fork. X-ray films show a dorsally displaced, dorsally angulated fracture of the distal radius. There is also an associated fracture of the ulnar styloid. A neurologic examination is normal. Which of the following is the most appropriate management?
Closed reduction and short arm cast
Closed reduction and long arm cast
Skeletal traction
Intramedullary rod
Open reduction and internal fixation
354. A 5-week-old infant presents with a 1-week history of progressive nonbilious emesis, associated with a 24-hour history of decreased urine output. The infant continues to be active and eager to feed. On examination, the infant has a sunken fontanelle and decreased skin turgor. The abdomen is scaphoid, and with a test feed, there is a visible peristaltic wave in the epigastrium. Which of the following is the most likely diagnosis?
Viral gastroenteritis
Gastroesophageal reflux
Urinary tract sepsis
Pyloric stenosis
Milk protein allergy
355. A 5-week-old infant presents with a 1-week history of progressive nonbilious emesis, associated with a 24-hour history of decreased urine output. The infant continues to be active and eager to feed. On examination, the infant has a sunken fontanels and decreased skin turgor. The abdomen is scaphoid, and with a test feed, there is a visible peristaltic wave in the epigastrium. The diagnosis is best confirmed by which of the following?
Abdominal ultrasound
Careful clinical examination with palpation of an epigastric mass
UGI contrast study
Surgical exploration
Endoscopy
356. An 80-year-old man is found to have an asymptomatic pulsatile abdominal mass. An arteriogram is obtained (shown below). Which of the following is the most frequent and lethal complication of this condition?
Rupture
Acute thromboembolism
Dissection
High-output congestive heart failure
Myocardial infarction
357. A 75-year-old man is found by his internist to have an asymptomatic carotid bruit. Which of the following is the most appropriate next test?
Transcranial Doppler studies
Doppler ultrasonography (duplex)
Spiral CT angiography
Arch aortogram with selective carotid artery injections
Magnetic resonance arteriogram (MRA)
358. An older, overweight man complains of disabling, sharp heel pain every time his foot strikes the ground. The pain is worse in the mornings, preventing him from putting any weight on the heel. X-ray films show a bony spur matching the location of his pain, and physical examination shows exquisite tenderness to direct palpation right over that heel spur. Furthermore, when the ankle is dorsiflexed, the entire inner border of the fascia is tender to palpation. Which of the following is the most likely diagnosis?
Epiphysitis of the calcaneus
Fracture of the posterolateral talar tubercle
Plantar fasciitis
Posterior Achilles tendon bursitis
Posterior tibial nerve neuralgia

A 65-year-old woman presents to the physician’s office with a 6-month history of epigastric discomfort, poor appetite, and 10-lb weight loss. Past history is pertinent for hypertension, diabetes, a 30 pack-year smoking history, and occasional alcohol intake. Examination is unremarkable except for mild epigastric tenderness to deep palpation. An abdominal ultrasound reveals cholelithiasis, and one view of a UGI x-ray series is shown in Figure 6-8. Which of the following is the most likely diagnosis?
Cholecystoenteric fistula
Duodenal ulcer
Gastric ulcer
Gastric diverticulum
Duodenal diverticulum
360. A 75-year-old woman is brought to the emergency department from a nursing home for abdominal pain, distention, and obstipation over the last 2 days. Past history is pertinent for stroke, diabetes, atrial fibrillation, and chronic constipation. Examination reveals a temperature of 98.6°F, pulse rate 90/min and irregularly irregular, and BP 160/90 mmHg. Heart examination reveals irregularly irregular rhythm with no murmurs; lung examination reveals few bibasilar rales; and abdominal examination reveals a distended, tympanic abdomen with mild tenderness and no rebound tenderness. Plain abdominal x-rays reveal dilated loops of bowel, and a barium enema is obtained and shown in Figure 6-9. Which of the following is the most likely diagnosis?
Ischemic colitis with stricture
Diverticulitis with obstruction
Cecal volvulus
Sigmoid volvulus
Colon cancer with obstruction
361. A 63-year-old man is seen because of facial swelling and cyanosis, especially when he bends over. There are large, dilated subcutaneous veins on his upper chest. His jugular veins are prominent even while he is upright. Which of the following conditions is the most likely cause of these findings?
Histoplasmosis (sclerosing mediastinitis)
Substernal thyroid
Thoracic aortic aneurysm
Constrictive pericarditis
Bronchogenic carcinoma
362. During endoscopic biopsy of a distal esophageal cancer, perforation of the esophagus is suspected when the patient complains of significant new substernal pain. An immediate chest film reveals air in the mediastinum. Which of the following is the most appropriate management of this patient?
Placement of a nasogastric tube to the level of perforation, antibiotics, and close observation
Spit fistula (cervical pharyngostomy) and gastrostomy
Left thoracotomy, pleural patch oversewing of the perforation, and drainage of the mediastinum
Left thoracotomy with esophagectomy
Thoracotomy with chest tube drainage and esophageal exclusion
363. In preparation for an inguinal hernia repair, a 22-year-old man has a spinal anesthetic placed. The level of sensory block turns out to be much higher than had been planned, and shortly thereafter his blood pressure drops to 75/20 mm Hg. He looks warm and flushed, and his central venous pressure is near zero. Which of the following should be included in his therapy?
Diuretics and fluid restriction
Whole blood and clotting factors
Inotropic agents and cardiac assist pump
Vasoconstrictors and IV fluids
Vasodilators and IV fluids
364. A 55-year-old woman presents with a 6-month history of weight loss, abdominal cramps, and intermittent nonbloody diarrhea. On examination, her abdomen is mildly distended and there is a palpable mass in the right lower quadrant. Stool cultures yield normal fecal flora. CT scan with oral contrast demonstrates an inflammatory mass in the right lower quadrant, with thickening of the terminal ileum and ileocecal valve. Which of the following is the most likely diagnosis?
Ulcerative colitis
Appendicitis
Crohn’s disease
Irritable bowel syndrome
Lactose intolerance
365. A 55-year-old woman presents with a 6-month history of weight loss, abdominal cramps, and intermittent nonbloody diarrhea. On examination, her abdomen is mildly distended and there is a palpable mass in the right lower quadrant. Stool cultures yield normal fecal flora. CT scan with oral contrast demonstrates an inflammatory mass in the right lower quadrant, with thickening of the terminal ileum and ileocecal valve.Which of the following is the best diagnostic test to confirm the diagnosis?
Repeat CT scan with delayed imaging
Ultrasonography
Sigmoidoscopy
Colonoscopy
Small-bowel radiography
366. A 27-year-old woman seeks your advice regarding pain and numbness in the right arm and hand. She reports that it is exacerbated by raising her arm over her head. On examination, the right radial pulse disappears when the patient takes a deep breath and turns her head to the left. A provisional diagnosis is made. Which of the following is the most appropriate initial treatment for this patient?
Physical rehabilitation
Gabapentin to treat neuropathic pain
Right first rib resection
Thoracoscopic sympathectomy
Upper thoracic discectomy
367. A 35-year-old man with a history of melanoma status post wide local excision with negative margins and lymph node dissection presents with 2, peripherallylocated pulmonary lesions seen on chest CT scan. Percutaneous biopsy of the lesion is consistent with metastatic melanoma. He has no evidence of recurrence or extrathoracic disease and is in good general health. Which of the following is the most appropriate management of this patient?
Chemotherapy
Radiation therapy
Pulmonary metastasectomy
Pulmonary metastasectomy followed by radiation therapy
Neoadjuvant radiation therapy followed by pulmonary metastasectomy
368. A 65-year-old woman has had pain in her right shoulder and has been treated with analgesics without relief. The CXR reveals a mass in the apex of the right chest. A transthoracic needle biopsy documents carcinoma. Superior pulmonary sulcus carcinomas (Pancoast tumors) are bronchogenic carcinomas that typically produce which of the following clinical features?
Atelectasis of the involved apical segment
Horner syndrome
Pain in the T4 and T5 dermatomes
Nonproductive cough
Hemoptysis
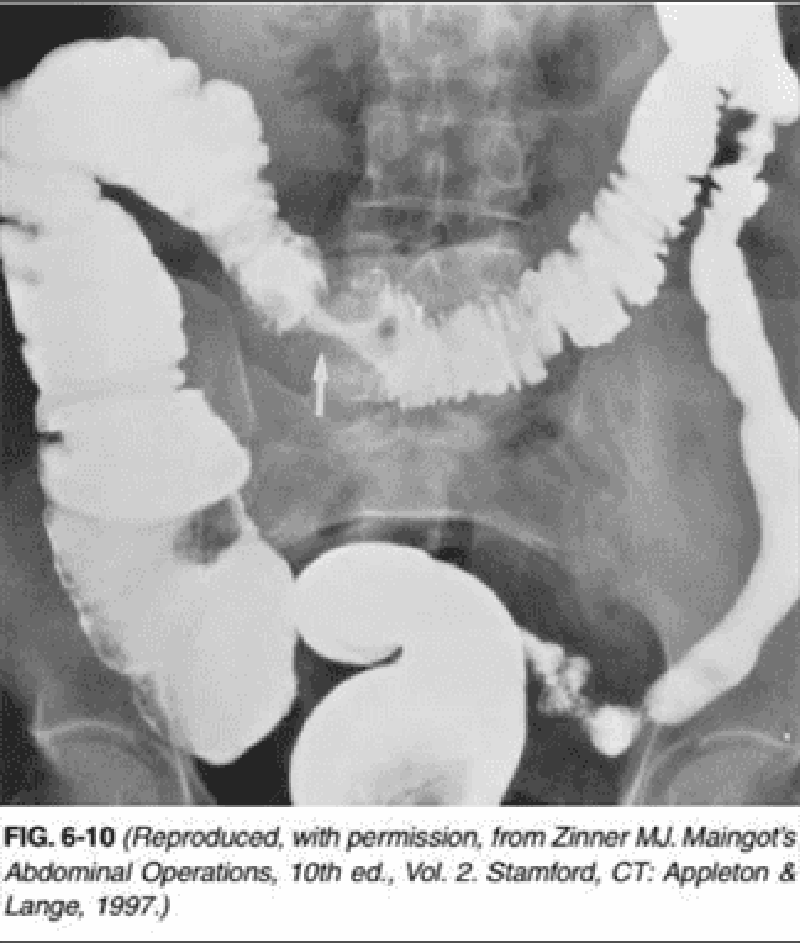
369. A 65-year-old man presents to the physician’s office for his yearly physical examination. His only complaint relates to early fatigue while playing golf. Past history is pertinent for mild hypertension. Examination is unremarkable except for trace hematest-positive stool. Blood tests are normal except for a hematocrit of 32. A UGI series is performed and is normal. A barium enema is performed, and one view is shown in Figure 6-10. Which of the following is the most appropriate therapy following colonoscopy?
Proximal colostomy with mucous fistula
Radiation therapy
Chemotherapy
Surgical resection and primary anastomosis
Surgical bypass (colocolostomy)
370. A 65-year-old man presents to the emergency department with sudden onset of pain and weakness of the left lower extremity of 2-hour duration. Past history reveals chronic atrial fibrillation following a myocardial infarction 12 months ago. On examination, he is found to have a cool, pale left lower extremity with decreased strength and absent popliteal and pedal pulses. The opposite leg has a normal appearance with palpable pulses. Which of the following is the treatment of choice for this patient?
R-TPA (tissue plasminogen activator) infusion following anticoagulation
Administration of vasodilators
Four-compartment fasciotomy
Thromboembolectomy
Anticoagulation and close observation
371. A 53-year-old woman presents with complaints of weakness, anorexia, malaise, constipation, and back pain. While being evaluated, she becomes somewhat lethargic. Laboratory studies include a normal chest x-ray, serum albumin 3.2 mg/dL, serum calcium 14 mg/dL, serum phosphorus 2.6 mg/dL, serum chloride 108 mg/dL, blood urea nitrogen (BUN) 32 mg/dL, and creatinine 2.0 mg/dL. Which of the following is the most appropriate initial management?
Intravenous normal saline infusion
Administration of thiazide diuretics
Administration of intravenous phosphorus
Use of mithramycin
Neck exploration and parathyroidectomy
372. Which of the following patients with primary hyperparathyroidism should undergo parathyroidectomy?
A 62-year-old asymptomatic woman
A 54-year-old woman with fatigue and depression
A 42-year-old woman with a history of kidney stones
A 59-year-old woman with mildly elevated 24-hour urinary calcium excretion
A 60-year-old woman with mildly decreased bone mineral density measured at the hip of less than 2 standard deviations below peak bone density
373. A 45-year-old woman presents with hypertension, development of facial hair, and a 7-cm suprarenal mass. Which of the following is the most likely diagnosis?
Myelolipoma
Cushing disease
Adrenocortical carcinoma
Pheochromocytoma
Carcinoid
374. A 44-year-old homeless woman presents to the emergency department because she is "bleeding from the breast." Physical examination shows a huge, fungating, ulcerated mass that occupies the entire right breast and is firmly attached to the chest wall. The right axilla is full of hard masses that are not movable either. Core biopsies of the breast are read as highly undifferentiated infiltrating ductal carcinoma, and assay for estrogen and progesterone receptors are negative. Which of the following is the most appropriate next step in management?
Local wound care, but no specific antineoplastic therapy
Tamoxifen therapy
Radiation and chemotherapy
Palliative mastectomy
Radical mastectomy with extended lymph node dissection
375. A 64-year-old woman complains of right calf pain and swelling. She recently underwent an uncomplicated left hemicolectomy for diverticular disease. A duplex ultrasound confirms the presence of deep vein thrombosis (DVT) of the calf. Which of the following is the most appropriate initial management of this patient?
Pneumatic compression stockings
Warfarin
Thrombolysis
Inferior vena cava filter
Heparin
376. For the first 6 hours following a long and difficult surgical repair of a 7-cm abdominal aortic aneurysm, a 70-year-old man has a total urinary output of 25 mL since the operation. Which of the following is the most appropriate diagnostic test to evaluate the cause of his oliguria?
Renal scan
Aortogram
Left heart preload pressures
Urinary sodium concentration
Creatinine clearance
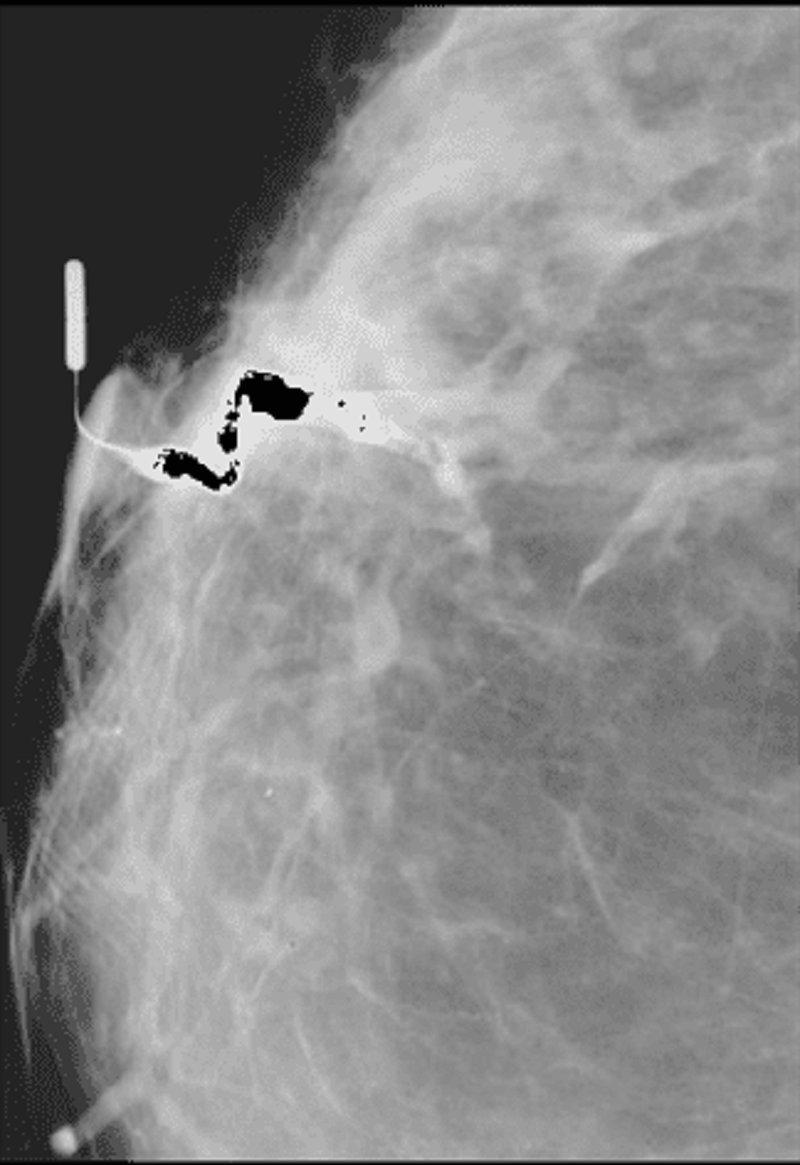
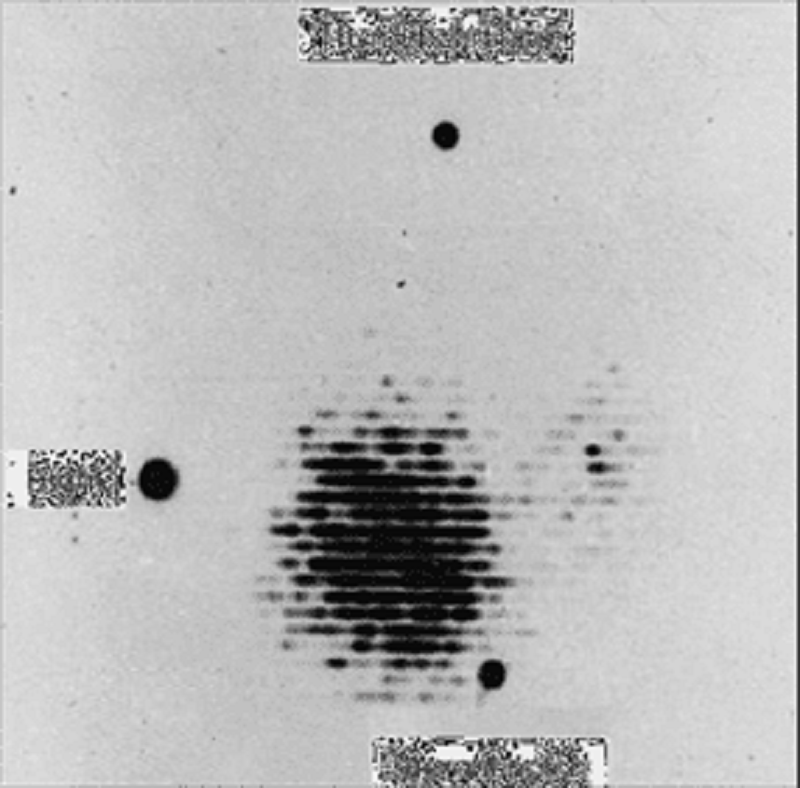
377. A 51-year-old woman presents to the physician’s office with a 2-month history of a right breast blood tinged nipple discharge. Past history is unremarkable. Family history is positive for postmenopausal breast cancer in a maternal grandmother. Examination reveals no palpable masses or regional adenopathy, but a serous discharge is easily elicited from a single duct in the right breast. Bilateral mammograms show no abnormalities. Cytology from the discharge was not diagnostic. A ductogram was ordered, and the results are shown: Which of the following is the most appropriate next step in management?
Collection of discharge for repeat cytologic analysis
Observation, with repeat examination and imaging studies in 3–6 months
Modified radical mastectomy
Central lumpectomy (including removal of the nipple/areolar complex
Terminal duct excision (microdochectomy)
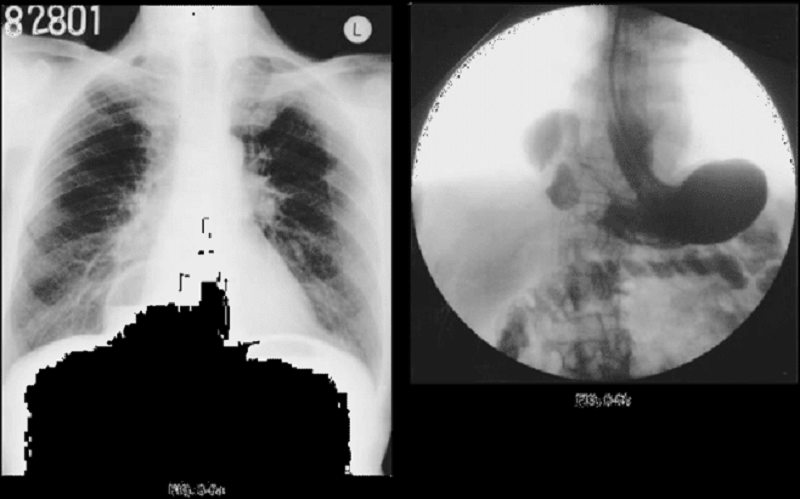
378. An 85-year-old man presents to the emergency room with an acute onset of midepigastric pain, nausea, vomiting, and hiccups starting 2 days ago. He is unable to keep any food down. Past history is pertinent for a long-standing hiatal hernia, hypertension, and diet-controlled diabetes. Examination reveals vital signs of pulse rate 82/min, BP 100/52 mmHg, respiratory rate 16/min, and temperature 97.2°F. The patient is in no acute distress, but has epigastric tenderness without guarding. Laboratory analysis revealed a hematocrit of 46 and a normal white blood cell (WBC) count. A chest x-ray is shown in Figure 6-5a. A fluoroscopically guided NG tube was placed using contrast, and his stomach was decompressed. After adequate fluid and electrolyte resuscitation, an upper gastrointestinal (UGI) contrast study was obtained and is shown in 6-5b. Which of the following is the most likely diagnosis?
Sliding hiatal hernia
Hernia of Bochdalek (posterorlateral congenital diaphragmatic hernia)
Hernia of Morgagni (parasternal congenital diaphragmatic hernia)
Paraesophageal hernia
Eventration of the diaphragm (central diaphragm)
379. A 66-year-old man presents with progressive jaundice, which he first noticed 6 weeks ago. He has a total bilirubin of 22 mg/dL, with a direct (conjugated) bilirubin of 16 mg/dL. His transaminases are minimally elevated, whereas his alkaline phosphatase is about six times the upper limit of normal. A sonogram shows dilated intrahepatic ducts, dilated extrahepatic ducts, and a very distended, thin-walled gallbladder without stones. Which of the following is the most appropriate next step in diagnosis?
CT scan of the upper abdomen
Endoscopic retrograde cholangiopancreatography (ERCP)
Exploratory laparotomy
Percutaneous transhepatic cholangiogram (PTC)
Serologies to define the type of hepatitis
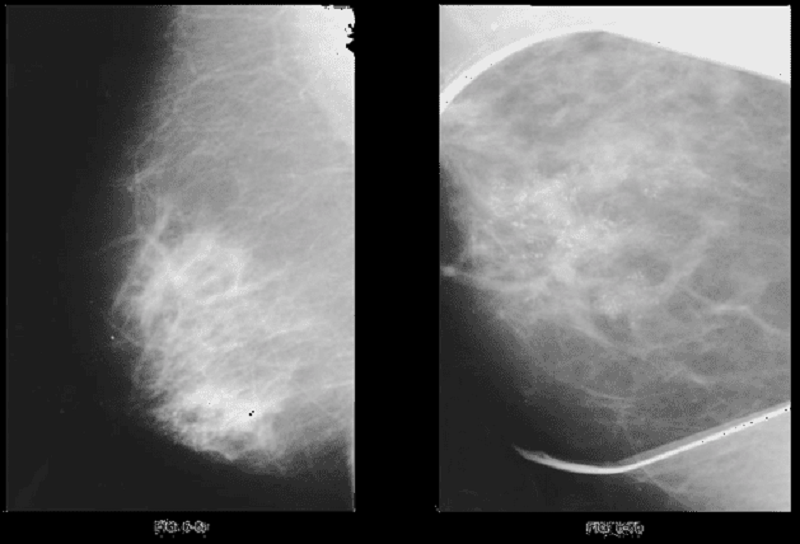
380. A 65-year-old woman presents to the physician’s office for evaluation of an abnormal screening mammogram. She denies any breast masses, nipple discharge, pain, or skin changes. Past history is pertinent for hypertension. Family history is positive for postmenopausal breast cancer in a sister. She has a normal breast examination and no axillary adenopathy. The remainder of her examination is unremarkable. An MLO view of the right breast is shown in Figure 6-6a along with a magnification view of the craniocaudal (CC) film (Figure 6-6b). Which of the following is the most appropriate next step in management?
Observation, with repeat mammogram in 6 months
Observation, with repeat mammogram on an annual basis
Biopsy
Lumpectomy, radiation therapy, and SLN biopsy
Total mastectomy
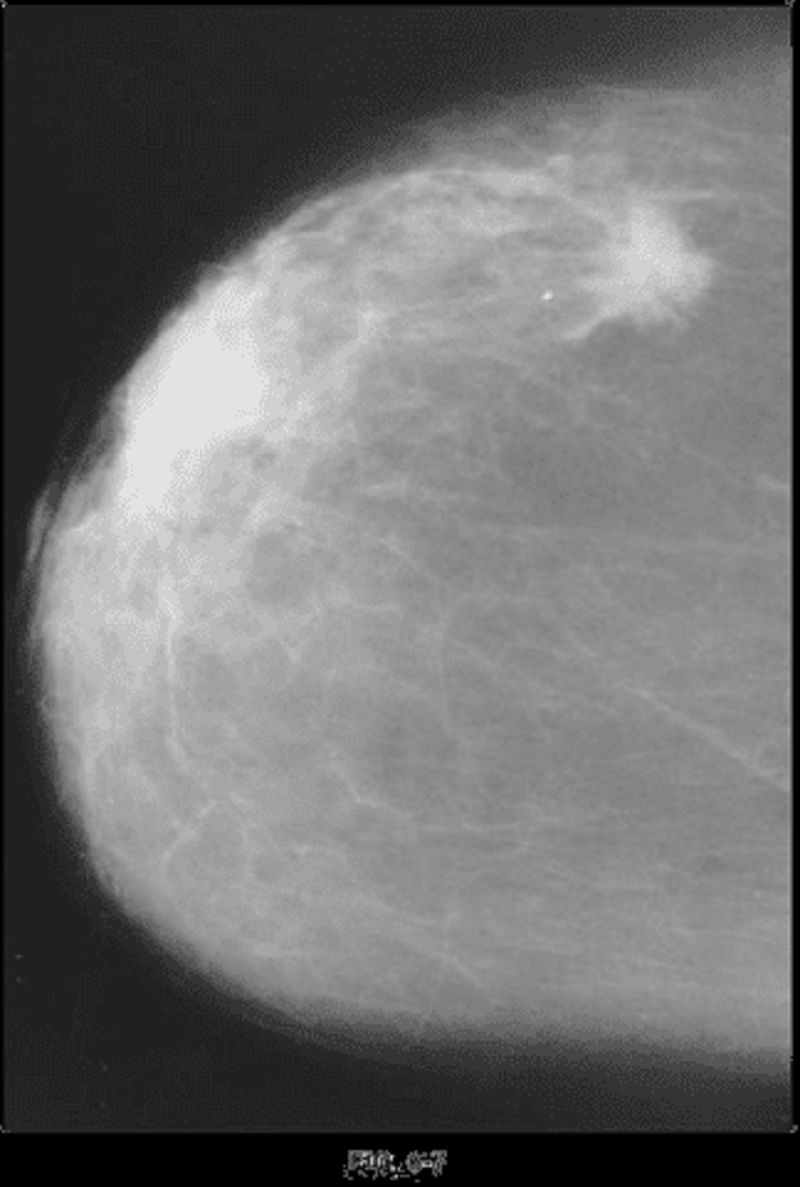
381. An 83-year-old woman presents to a mammographic facility for a screening mammogram. The technician notices a mass in the lateral right breast. The patient denies any breast pain, nipple discharge, skin changes, or breast trauma. A right breast CC view is shown in Figure 6-7. Which of the following is the most likely diagnosis?
Papilloma
Invasive carcinoma
Cystosarcoma phyllodes
DCIS
Fat necrosis
382. A 45-year-old woman presents with a 7-cm renal cell carcinoma with radiologic evidence of abdominal lymph node involvement with no distant metastases. Which of the following is the most appropriate management of this patient?
Radical nephrectomy
Radiation
Chemotherapy
Radiation followed by nephrectomy
Chemotherapy followed by nephrectomy
383. A 58-year-old man is found to have high serum prostate–specific antigen (PSA) concentration with a normal prostate examination. A biopsy of the prostate confirms low-grade carcinoma. The patient wishes to avoid therapy involving any risk for impotence. Which of the following is the most appropriate management of this patient?
Observation
Chemotherapy
Prostatectomy
Radiation therapy
Hormonal therapy
384. A 56-year-old man develops slow, progressive paralysis of the facial nerve on one side. It took several weeks for the full-blown paralysis to become obvious, and it has been present now for 3 months. It affects both the forehead and the lower face. He has no pain anywhere, and no palpable masses by physical examination. Which of the following is the most likely diagnosis?
Bell's palsy
Facial nerve tumor
Hemorrhagic stroke
Parotid gland cancer
Pleomorphic adenoma of the parotid gland
385. A 28-year-old man with a past history of bilateral orchiopexy for cryptorchidism presents with a painless, unilateral right scrotal enlargement. On examination, there is a palpable right testicular mass and enlarged inguinal nodes. Scrotal ultrasonography demonstrates heterogeneity of the testis, with an associated hydrocele. A CT scan of the abdomen and pelvis demonstrated right-sided retroperitoneal adenopathy. CT scan of the chest is normal. Which of the following would help confirm the diagnosis?
Transscrotal needle biopsy
Transscrotal aspiration of the hydrocele for cytology
Radical orchiectomy through an inguinal incision
Transscrotal exploration and orchiectomy
Laparotomy with pelvic and retroperitoneal node dissection
386. A 28-year-old man with a past history of bilateral orchiopexy for cryptorchidism presents with a painless, unilateral right scrotal enlargement. On examination, there is a palpable right testicular mass and enlarged inguinal nodes. Scrotal ultrasonography demonstrates heterogeneity of the testis, with an associated hydrocele. A CT scan of the abdomen and pelvis demonstrated right-sided retroperitoneal adenopathy. CT scan of the chest is normal. Staging workup and surgery reveal a seminoma of the testicle, with positive inguinal and retroperitoneal nodes. Therapeutic management for this patient is which of the following?
External beam radiotherapy
Multidrug combination chemotherapy
Combination radiotherapy and multidrug chemotherapy
Clinical surveillance
Laparotomy with pelvic and retroperitoneal node dissection
387. A 45-year-old woman complains to her primary care physician of nervousness, sweating, tremulousness, and weight loss. The thyroid scan shown here exhibits a pattern that is most consistent with which of the following disorders?
Hypersecreting adenoma
Graves disease
Lateral aberrant thyroid
Papillary carcinoma of thyroid
Medullary carcinoma of thyroid
388. A patient with mild skin pigmentation is admitted emergently to your service because of sudden abdominal pain, fever, and a rigid abdomen. Her blood work indicates a marked leukocytosis, a blood sugar of 55 mg/dL, a sodium value of 119 mEq/dL, and a potassium value of 6.2 mEq/dL. Her blood pressure is 88/58-mmHg. She undergoes an exploratory laparotomy. Which of the following is the definitive treatment for her primary condition?
10% dextrose infusion
Bicarbonate
Hypertonic saline
Corticosteroids
Vasopressors
389. The unrestrained front-seat passenger in a car that crashes sustains closed comminuted fractures of both femoral shafts. Shortly after admission, he develops a blood pressure of 80/50 mm Hg, a pulse rate of 110/min, and a venous pressure of zero. He becomes pale, cold, and clammy, but the rest of his physical examination and x-ray films of the chest and pelvis are unremarkable. A sonogram of the abdomen done in the emergency department is likewise negative. Which of the following is the most likely reason for the low blood pressure?
Blood loss at the fracture sites
Fat embolism
Neurogenic shock from pain
Unrecognized intracranial bleeding
Unrecognized pericardial tamponade

390. A 10-month-old infant presents to the emergency department with a 24-hour history of low-grade fever and anorexia. The parents report several episodes in which the child has been suddenly inconsolable and crying, followed by periods of lethargy. He has had nonbilious vomiting and several loose stools. On examination, the infant is pale and mildly dehydrated. His abdomen is soft and nondistended, with fullness to palpation in the right upper quadrant. The child passed another stool in the emergency department (see Figure 6-14). Which of the following is the most appropriate next step in the diagnostic evaluation and management of this patient?
Proctoscopy
Oral rehydration and stool cultures
IV fluid rehydration and a hydrostatic barium enema
Technetium scan
IV fluid rehydration, NG decompression, and a UGI contrast study
391. A 24-year-old patient with known neurofibromatosis type 2 undergoes an MRI for ringing in his ears. The MRI demonstrates lesions in bilateral auditory canals. Which of the following is the most likely diagnosis?
Gangioneuroma
Schwannoma
Ependymoma
Meningioma
Pituitary adenoma
392. A40-year-old man with a history of alcohol abuse presents after an episode of binge drinking. He is complaining of epigastric pain, radiating to the back, associated with nausea and vomiting. On examination, he has marked tenderness in the epigastrium, with guarding, decreased bowel sounds, and moderate abdominal distention. Laboratory findings include leukocytosis and increased serum amylase and lipase. Abdominal roentgenograms demonstrate several dilated bowel loops in the upper abdomen. Select the most likely diagnosis.
Gastroenteritis
Acute appendicitis
Sigmoid diverticulitis
Acute pancreatitis
Acute cholecystitis
393. A 65-year-old man presents with a 4-day history of worsening lower abdominal pain and constipation. On examination, he is febrile (38.5°C) and has lower abdominal tenderness that is most intense in the midline and left lower quadrant associated with a palpable fullness. Laboratory findings demonstrate a moderate leukocytosis and abdominal roentgenograms show an ileus pattern. Select the most likely diagnosis.
Gastroenteritis
Regional enteritis
Acute appendicitis
Perforated peptic ulcer
Sigmoid diverticulitis
394. A 65-year-old man presents to the physician’s office with complaints of abdominal discomfort and jaundice for the past 3 weeks. Past history is pertinent for 30 pack-year smoking history, occasional alcohol intake, and a 5.5-mm ulcerating melanoma removed from his back 21/ 2 years ago. Examination reveals a mildly jaundiced patient with normal vital signs and a slightly distended abdomen with mild right upper quadrant tenderness and significant hepatomegaly. Which one is the most likely diagnosis?
Hepatitis A
Hemolysis
Choledocholithiasis
Liver metastases
Cirrhosis
395. A 45-year-old woman presents with left-sided weakness. A CT scan of the head demonstrates a well-circumscribed mass abutting the skull in the right hemisphere. Workup of the mass reveals a meningioma. Which of the following is the best next step in treatment?
Cerebral angiography with tumor embolization
Preoperative radiation therapy followed by surgical excision
Surgical excision
Chemotherapy with adriamycin
Chemoradiation
396. A 30-year-old man presents to the emergency department with sudden onset of severe epigastric pain and vomiting 3 hours ago. He reports a 6-month history of chronic epigastric pain occurring nearly every day and relieved by antacids. On examination, he appears sweaty and avoids movement. Vital signs reveal a temperature of 100°F, BP of 100/60 mmHg, pulse rate of 110/min, and respiratory rate of 12/min. The remainder of his examination reveals diminished bowel sounds and a markedly tender and rigid abdomen. A chest x-ray and abdominal films reveal pneumoperitoneum. Which of the following is the most likely diagnosis?
Small-bowel obstruction
Dead bowel
Perforated colon carcinoma
Perforated duodenal ulcer
Perforated gastric ulcer
397. A 15-year-old otherwise healthy female high school student begins to notice galactorrhea. A pregnancy test is negative. Which of the following is a frequently associated physical finding?
Gonadal atrophy
Bitemporal hemianopsia
Exophthalmos and lid lag
Episodic hypertension
Buffalo hump
398. A 52-year-old woman sees her physician with complaints of fatigue, headache, flank pain, hematuria, and abdominal pain. She undergoes a sestamibi scan that demonstrates persistent uptake in the right superior parathyroid gland at 2 hours. Which of the following laboratory values is most suggestive of her diagnosis?
Serum acid phosphatase above 120 IU/L
Serum alkaline phosphatase above 120 IU/L
Serum calcium above 11 mg/dL
Urinary calcium below 100 mg/day
Parathyroid hormone levels below 5 µmol/L
399. A 30-year-old man presents to the emergency department with sudden onset of severe epigastric pain and vomiting 3 hours ago. He reports a 6-month history of chronic epigastric pain occurring nearly every day and relieved by antacids. On examination, he appears sweaty and avoids movement. Vital signs reveal a temperature of 100°F, BP of 100/60 mmHg, pulse rate of 110/min, and respiratory rate of 12/min. The remainder of his examination reveals diminished bowel sounds and a markedly tender and rigid abdomen. A chest x-ray and abdominal films reveal pneumoperitoneum. Which of the following is the most appropriate next step in management?
Immediate laparotomy
Nonoperative management with NG decompression and antibiotics
Fluid resuscitation
Administration of H2 blockers
Placement of a central venous line
400. A 55-year-old man presents to the physician’s office complaining of upper abdominal pain of 2 months’ duration. The pain is described as gnawing, localized to the upper midline, and associated with nausea. The pain is exacerbated by food, and there is an associated 20-lb weight loss over 2 months. His past history is pertinent for a 30 pack-year smoking history, occasional alcohol intake, and a prior history of a benign gastric ulcer 5 years ago. Physical examination reveals normal vital signs, mild epigastric pain with deep palpation, and mildly hemepositive stool. An evaluation for recurrence of a gastric ulcer is recommended. Which of the following tests is the most reliable method for diagnosing a gastric ulcer?
UGI barium x-rays
Fiberoptic upper endoscopy
CT scan
Endoscopic ultrasound
MRI
{"name":"Surgery USMLE (301-400)", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"301. A 62-year-old woman presents to the physician’s office with complaints of constipation. She has had constipation for the last 6 months, which has worsened over the last month, associated with mild bloating. She noted that her stool has become “pencil thin” in the last month, with occasional blood, but she continues to have bowel movements daily. Past history is unremarkable. Examination reveals normal vital signs and heart and lung examination. Abdominal examination reveals mild fullness, especially in the lower quadrants. Rectal examination shows no rectal masses, but the stool is hematest positive. A barium xray is obtained, and one view is shown in Figure 6-11. Which of the following is the most appropriate next step in management ?, 302. A 45-year-old man presents to the physician’s office for evaluation of a skin lesion on his abdomen. He states that the lesion has been present for 1 year, but has recently enlarged over the last 2 months. The mass is nontender, and he is otherwise asymptomatic. Past history is unremarkable. Examination reveals a 3-cm, pigmented, irregular skin lesion located in the left lower quadrant of the abdomen, as shown in Figure 6-12. Heart, lung, and abdominal examination are normal. There are no palpable cervical, axillary, or inguinal lymph nodes. Chest x-ray and liver function tests are normal. Which of the following is the most likely diagnosis?, 303. A 55-year-old man with recent onset of atrial fibrillation presents with a cold, numb, pulseless left lower extremity. He is immediately taken to the operating room for an embolectomy of the left popliteal artery. Which additional procedure should be performed along with the embolectomy?","img":"https://cdn.poll-maker.com/17-692534/untitled.png?sz=1200"}
More Quizzes
Week 5
1470
Bichon Frise
840
Coral reefs
100
Cap. 6 Nuestro GPS interno
10523
What Unnatural Color Should I Dye My Hair? - Free
201018502
Which Transformers: Rise of the Beasts Character Are You?
201019319
Divergent Personality Test: Find Your Faction (Free)
201022356
Social Work - Introductory Practice Questions (Free)
15816717
Bollywood Actors - Icons of Hindi Cinema
201023406
Mental Health Nursing Questions - Free Practice
201031074
Am I Okay - Free Mental Wellbeing Self‑Assessment
201021169
Funny Username Generator - Get Your Hilarious Handle
201020027