
Part 46
118) A 61-year-old Caucasian male presents with ptosis, diplopia and limb weakness. These symptoms worsen in the evening and with exercise, and improve with rest. He also has fatigue, which is worse in the evening. He denies any tingling or numbness. On examination, he cannot sustain an upward gaze, and his eyelids tend to drift downward. Injection of edrophonium quickly restores power, and allows him to maintain an upward gaze. Which of the following is the best initial treatment for this patient?
Treatment with pyridostigmine
Treatment with edrophonium
Treatment with atropine
Treatment with prednisolone
Treatment with intravenous immunoglobulins
119) A 7-year-old boy is brought to the office by his mother because, "he is always daydreaming." Sometimes, he stares for a few seconds and rolls his eyes for unknown reasons. His teacher has noted a recent decline in his school performance. He has no family history of any seizure disorder, and his psychomotor development is normal. His neurological examination is unremarkable. EEG during hyperventilation shows generalized, symmetrical 3-Hz spike-and-wave activity on a normal background. Which of the following medications is the most appropriate to treat the boy's disorder?
. Phenytoin
. Phenobarbital
. Valproic acid
. Clonazepam
. Lamotrigine
120) A 32-year-old Caucasian male comes to the emergency department due to progressive ascending paralysis, which began 18 hours ago. He initially noticed paresthesias in his lower limbs, followed by a sense of fatigue and weakness. He denies any history of headache, fever, and recent infection or illness. His blood pressure is 120/80 mm Hg, pulse is 80/min, respirations are 16/min, and temperature is 37.3°C (99.2°F). The physical examination reveals intact cranial nerves, absent deep tendon reflexes, and a normal sensory exam. Laboratory studies reveal a normal WBC count. No abnormalities are noted on CSF examination. While evaluating the patient in the hospital, he quickly deteriorates. What is the most appropriate next step in the management of this patient?
IV immunoglobulin and plasmapheresis
Administer botulinum antitoxin
IV methylprednisolone
Meticulous search for a tick
MRI of the spine
121) A 36-year-old Caucasian male is brought to the emergency department due to weakness of his upper and lower extremities. Neurological examination reveals weakness, atrophy, fasciculations, spasticity and hyperreflexia of the involved muscles. His sensory, bowel, bladder and cognitive functions are intact. Serum creatine kinase is normal. Cerebrospinal fluid examination is within normal limits. Electromyography shows chronic partial denervation. The patient is subsequently diagnosed with amyotrophic lateral sclerosis. Which of the following has been approved for use in patients with amyotrophic lateral sclerosis?
. Riluzole
. Corticosteroids
. Intravenous immunoglobulins
. Plasmapheresis
. Donepezil
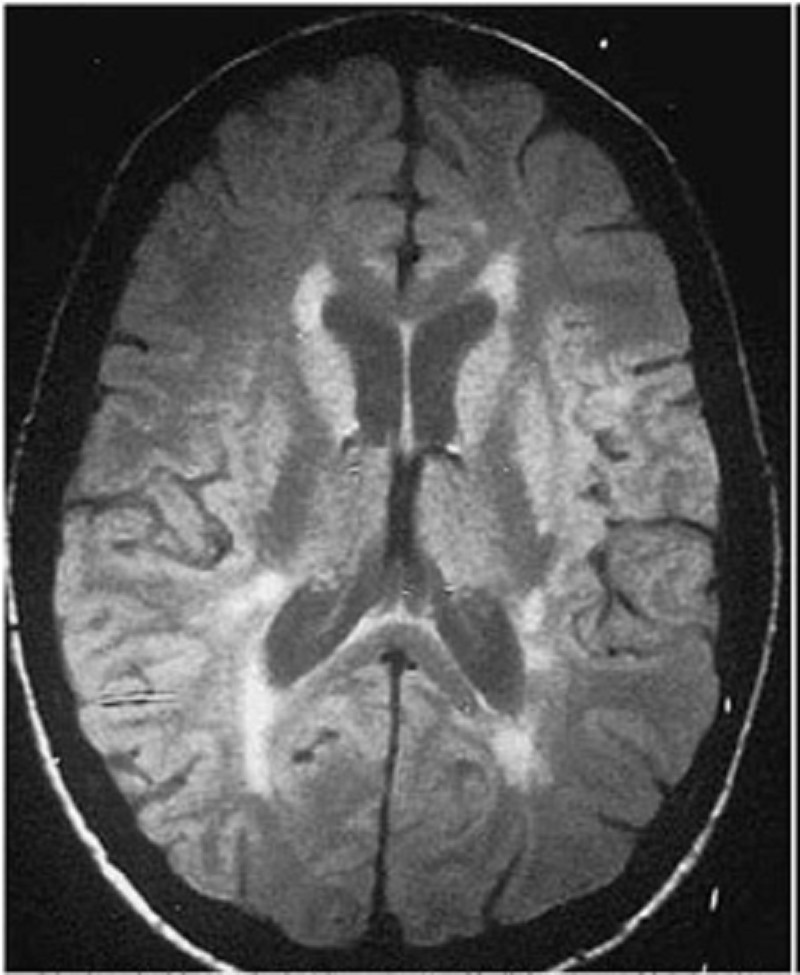
122) A 38-year-old female presents with one week of "shakiness" in her right arm, right leg weakness and unsteady gait. An MRI of her brain is shown below. Which of the following is the best treatment for this patient?
Aspirin and simvastatin
Glatiramer acetate
Argatroban
Tissue plasminogen activator
Broad-spectrum antibiotics
123) A 62-year-old Caucasian man with hypertension and chronic kidney disease complains of poor sleep. He describes a sensation of spiders crawling over both legs about 15-20 minutes after going to bed. Sometimes he has to sit up in bed and massage his legs. His wife's sleep has deteriorated as her husband's leg movements have gotten worse. Pharmacotherapy for this patient's disease is typically directed at which of the following?
. Norepinephrine
. Dopamine
. Serotonin
. Acetylcholine
. GABA
124) A 22-year-old white obese female presents with headache for the last few weeks. Headache is worse at night and wakes her from sleep. Headache is pulsating in quality and is also associated with nausea and vomiting. She denies any weakness, sensory abnormalities or visual problems. She denies any history of trauma. She does not take any medication. Neurological examination is unremarkable. Fundoscopy shows papilledema. CT scan of head does not show any abnormality. Lumbar puncture is performed and CSF examination is normal except increased CSF pressure. Weight loss fails to control her symptoms. Which of the following is the most appropriate next step in the management of this patient?
Treatment with mannitol
Treatment with acetazolamide
Treatment with corticosteroids
Repeated lumbar punctures
Surgery
125) A 52-year-old Caucasian male comes to the office for the evaluation of tremors. He has been having tremors in both hands and head over the past several months. He does not experience any tremors at rest, or any problem with his legs. He has a history of alcohol abuse. He is currently not on any medication. His father had essential tremors, and his paternal uncle has Parkinsonism. The physical examination reveals tremors, which increase in amplitude when he tries to reach for an object. Which of the following is the most appropriate next step in the management of this patient?
. Benztropine
. Propranolol
. Haloperidol
. Valproic acid
. Clonazepam
126) A 32-year-old Caucasian male is admitted to the hospital due to a 1-week history of progressive paralysis of his upper and lower extremities. He had a flu-like illness 3 weeks ago, followed by paresthesias in his fingertips and toes. The weakness initially started in his lower extremities. He denies any changes in bowel and bladder functions. His blood pressure (supine) is 130/70mm Hg, heart rate is 82/min, respirations are 18/min, and temperature is 36.9°C (98.5°F). Physical examination reveals bilateral facial paralysis, orthostatic hypotension, areflexia in all four extremities, and distal paresthesias. His CSF analysis shows: Total WBC 10/cmm, Protein 120 mg/dl, Glucose 70 mg/dl, Gram stains No organisms. What is the most appropriate next step in the management of this patient?
Intravenous methyl prednisolone
Intravenous immunoglobulin therapy
Intravenous acyclovir therapy
Botulinum antitoxin
Intravenous ceftriaxone and ampicillin
127) A 59-year-old white male comes to the office for the evaluation of a brief episode of right arm and leg weakness. The episode lasted for a few minutes, and was followed by a complete recovery. He had a similar episode one month ago. He has a 30 pack-year history of cigarette smoking. He has hypercholesterolemia, which is being treated with diet and exercise. His pulse is 76/min, regular, and blood pressure is 130/80 mmHg. His laboratory test results are: Hb 14.2 g/dl, WBC 7,000/cmm, Platelets 230,000/cmm, Blood Glucose 118 mg/dl, Serum Na 138 mEq/L, Serum K 4.5 mEq/L, BUN 16 mg/dl, Serum Creatinine 1.0 mg/dl. EKG shows normal sinus rhythm. CT scan of the head is unremarkable. MRI angiography of the head and neck fails to show any abnormality. Transesophageal echocardiography (TEE) is unremarkable. Which of the following is the most appropriate next step in management?
Treatment with aspirin
Treatment with heparin followed by warfarin
Treatment with clopidogrel
Treatment with combination of aspirin and dipyridamole
Treatment with ticlopidine
128) A 65-year-old lady comes to the office for the evaluation of her deteriorating memory. She has become increasingly forgetful over the last several months, and now appears very concerned about her memory loss. She used to pride herself for her sharp memory, but has been forgetting the most trivial things and has become "extremely inefficient." She also complains of easy fatigability, poor appetite, and frequent awakening at night. She feels worthless and has lost interest in her favorite hobby, which is gardening. On coughing or laughing, she loses urine involuntarily, and this is adding to her misery. She lives with her husband, who says that she has become very "cranky and irritable" lately. Her medical history is significant for hypercholesterolemia, for which she refuses to take medication. She is presently not on any hormonal therapy. The physical examination is completely normal. Laboratory studies are unremarkable. CT scan of the head is normal. What is the best next step in the management of this patient?
Start hormonal replacement therapy
Treat her with donepezil
Start selective serotonin reuptake inhibitor
Surgical bypass shunting
Reassurance
129) A 27-year-old Caucasian female with multiple sclerosis (MS) comes to the office for a follow-up visit. Six months ago, she experienced monocular vision impairment and clumsiness of the right hand, and both symptoms resolved completely. Three weeks ago, she experienced incoordination, weakness and spasticity in the right extremities. She was admitted in the hospital for treatment of an acute MS flare, and rapidly improved thereafter. Physical examination currently demonstrates slight weakness of the right leg with a hyperactive knee jerk. Which of the following medications may slow the long-term progression of this patient's disease?
High-dose corticosteroids
. Interferon-beta
. Cyclosporine
. Methotrexate
. Mitoxantrone
130) A 45-year-old man is brought to the emergency department following a serious motor vehicle collision. Despite heroic attempts to save him, the physician caring for him believes he is brain dead. Unfortunately, the patient does not have an advanced directive or durable medical power of attorney. What step is necessary in order to remove the patient from the ventilator?
Ask his family members
Ask the hospital ethics committee
Confirm brain death with another physician
Notify the county medical examiner
No further steps are necessary
131) A 32-year-old female is crying as she approaches the office. She has had severe, unbearable pain in her face for the past five days. She describes the pain as knife-like, comes in paroxysms, occurs 10-20 times a day, and lasts a few seconds. She does not know what precipitates the attacks, but she has been unable to sleep, eat or go to work because of her symptoms. She has tried numerous pain medications, but nothing seems to relieve the pain. She denies any history of trauma, medication use or recent surgery. Vital signs are within normal limits. Physical examination is within normal limits. Which of the following agents will best benefit this patient?
. Levodopa
. Methotrexate
. Carbamazepine
. Lithium
. Morphine
132) A 23-year-old white female presents with an acute onset of headache for the last eight hours. Her headache is severe, unilateral, pulsating in quality, associated with photophobia, worsens with physical activity, and does not respond to acetaminophen or ibuprofen. This is her 6th episode of similar headache over the last 2 months, and it is her first time to seek medical attention. Her neurological examination is unremarkable. Which of the following is the most appropriate next step in the management of this patient?
. Propranolol
. Verapamil
. Ergotamine
. Rizatriptan
. Prochlorperazine
133) A 54-year-old male presents to the office with several months history of hand tremors that are unresponsive to over-the-counter medication. The tremors always become worse when he is in public places. Sometimes, the hand tremors are so bad that he is unable to grasp. He denies trauma, fever, loss of muscle function or any prior stroke. His past medical history is significant for vague abdominal pains, the cause of which was never found. He is given some medication. A month later, he comes back and says, "The tremor is gone, but now I have colicky abdominal pain, confusion, headaches, hallucinations and dizziness." What is the drug that caused this patient's new symptoms?
. Alcohol
. Propranolol
. Primidone
. Diazepam
. Lithium
134) A 44-year-old male has been abusing drugs for many years. Recently he started using the agent MPTP and he now presents to you in the ER. He says that he is not feeling well and wonders what is going on. He says he has a persistent tremor in his fingers and his body has become rigid. At times has had difficulty in walking. The CT scan of his brain is normal and all the blood work is within normal limits. You decide to treat him. Two years later you see him and he tells you that his symptoms have improved. He also noticed that he had a significant relief from the recurrent and persistent upper respiratory tract viral infections that he was so prone to. The agent you gave him was?
. Bromocriptine
. Levodopa-Carbidopa
. Amantadine
. Benztropine
. Acyclovir
135) A 5-year-old boy is brought to the office by his frustrated mother because, "he just can't seem to concentrate!" He has episodes that are characterized by frequent blinking and indifference to his surroundings. He does not remember anything after an episode. An episode does not last long, but he usually has 50-80 "daydreaming accidents" daily. His school performance has deteriorated lately, and his teacher has complained about his decreased concentration. Which of the following is the drug of choice for this patient's condition?
. Phenytoin
. Carbamazepine
. Ethosuximide
. Phenobarbital
. Lamotrigine
136) A 27-year-old white female comes to the office and complains of ptosis, diplopia and difficulty in chewing. Her symptoms worsen in the evening. She is asymptomatic when she wakes up in the morning. She denies any sensory complaints or limb weakness. The Tensilon test is positive. Serological testing shows positive acetylcholine receptor antibodies. Which of the following is the best treatment to induce remission and provide long-term benefits in this patient?
. Pyridostigmine
. Prednisolone
. Intravenous immunoglobulins
. Plasmapheresis
. Thymectomy
137) A 62-year-old male is brought to the emergency department with a chief complaint of weakness. He says that he was walking his dog 1 hour ago when he began to limp and noticed some weakness in his left arm. His past medical history is significant for hypertension treated with hydrochlorothiazide, and type II diabetes mellitus managed with metformin. He denies nausea, vomiting, chest pain, fever or chills. He does note occasional palpitations and tension headaches at baseline. On physical examination, his blood pressure is 170/95 mmHg and his heart rate is 76/min and regular. His blood glucose level is 190 mg/dl and his HbA1c is 7.6%. The neurological examination is significant for profound left-sided weakness and an up going Babinski reflex on the left. Non-contrast head CT is negative for any intracranial bleed. Which of the following is most likely to affect his chance of neurological recovery?
. Insulin for tight glucose control
. Labetalol
. Aspirin
. Fibrinolytic
. Heparin
138) A 62-year-old female is brought in by EMS due to a severe right-sided headache, nausea and eye pain. She was fixing a light bulb, when she suddenly felt pain in her right eye. She decided to rest, but the eye pain only got worse. In the next few minutes, she developed loss of vision, photophobia and redness in the same eye. She took medications to relieve the accompanying headache, but the eye pain persisted. She denies any trauma. Her past medical history is significant for diabetes and hypertension. She appears to be in intense pain with bouts of nausea. Her right eye is red, with conjunctival flushing and visual acuity of 20/200. Her right pupil is mid-dilated and non-reactive to light. The same eye feels hard on palpation. The one treatment that should be avoided in this patient is:
. Mannitol
. Acetazolamide
. Pilocarpine
. Timolol
. Atropine
139) A 65-year-old male comes to the emergency department because of a sudden, painless loss of vision in his right eye that occured a half an hour ago. Five hours ago, he experienced a similar but transient loss of vision in the same eye, which lasted for five minutes. He has hypertension, diabetes, hypercholesterolemia, and peripheral vascular disease. He had an anterior wall myocardial infarction six years ago. His medications include glyburide, captopril, atenolol, simvastatin and aspirin. His temperature is 36.7°C (98.0°F), respirations are 16/min, pulse is 88/min, and blood pressure is 146/88 mmHg. Examination of the right eye reveals visual acuity of 20/60 and subtle retinal whitening. A right carotid bruit is heard. Which of the following is the most appropriate next step in the management of this patient?
. Acetazolamide IV
. Ocular massage and high flow oxygen
. Administer systemic steroids
. Instillation of topical beta blocker
. Administer thrombolytics
140) A 33-year-old man presents with a 1-day history of localized, small swelling along the margin of the upper eyelid. He feels pain, which does not seem to come from the conjunctival surface. He has a 10-pack year smoking history. He occasionally drinks alcohol. He is sexually active, and does not use condoms regularly. He is worried about the swelling. What is the best next step in the management of this patient?
. Use warm compresses
. Incision and drainage
. Incision and curettage
. Take biopsy of the lesion
. Oral Penicillin
141) A 72-year-old man presents with right eye pain for 1 day. The patient has a history of diabetes, hypertension, and “some type of eye problem.” He does not recall the name of his eye problem or the name of his ophthalmic medication. However, he does remember that the eye drop has a yellow cap. Which class of ophthalmic medication is the patient taking?
. Antibiotic
. β-Blocker
. Mydriatic/cycloplegic agent
. Miotic
. Anesthetic
142) A 45-year-old woman presents with right eye pain and redness for 1 day. She has photophobia and watery discharge from the eye. She does not wear glasses or contact lenses and has no prior eye problems. On examination, the patient’s visual acuity is 20/20 in the left eye and 20/70 in the right eye. She has conjunctival injection around the cornea and clear watery discharge. On slit-lamp examination, the lids, lashes, and anterior chamber are normal. When fluorescein is applied, a branching, white-colored epithelial defect is seen. The remainder of the head examination is normal and the patient has no cutaneous lesions. Which of the following is the most appropriate treatment for this patient?
Admission for intravenous (IV) antibiotics
Admission for IV antiviral agents
Topical steroids
Topical antiviral medication
Immediate ophthalmology consultation
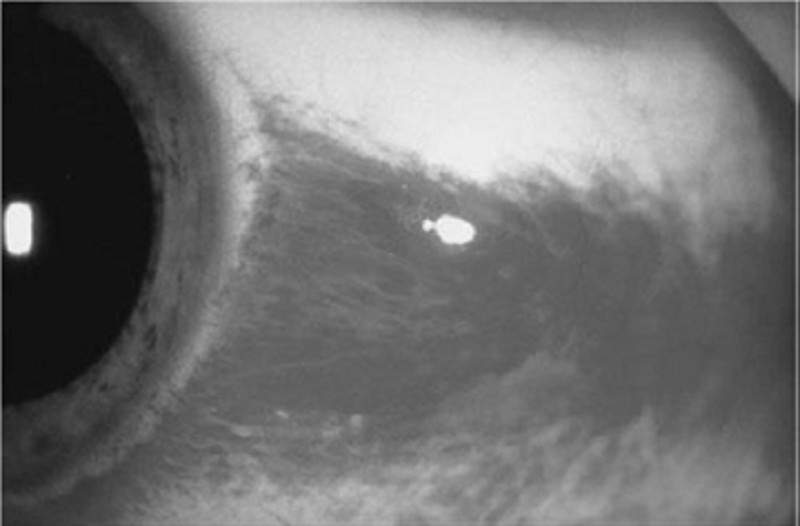
143) A 21-year-old man presents to the ED with a red eye. The patient complains of rhinorrhea and a nonproductive cough but has no eye pain or discharge. He also has no associated ecchymosis, bony tenderness of the orbit, or pain on extraocular eye movement. His vision is normal, extraocular movements are intact, and intraocular pressure (IOP) is 12. A picture of his eye is shown below. What is the most appropriate management of this condition?
Call ophthalmology immediately
Administer 1% atropine
Elevate patient’s head
Administer ophthalmic timolol
Reassurance only
144) A 28-year-old mechanic with no past medical history presents to the ED after a small amount of battery acid was splashed in his right eye. He is complaining of extreme pain and tearing from his eye. Which of the following is the most appropriate next step in management?
Call ophthalmology now
Check visual acuity
Check the pH of the tears
Irrigate with normal saline
Apply erythromycin ointment
145) A 33-year-old white female complains of repeated episodes of fever, malaise, chills, breathlessness and dry cough over the past 6 months. She says that each episode starts suddenly and lasts for several days. She otherwise has no significant past medical history and does not take any medications. There is no family history of lung disorders. She does not smoke cigarettes or drink alcohol. She has never been abroad, and has had no sick contacts. She breeds budgerigars (a small Australian parrot) as a hobby. Chest x-ray shows diffuse generalized haziness in both lower lung fields. Pulmonary function tests reveal reduced lung volumes and an FEV1/FVC ratio of 87%. PPD test is negative. Serology shows antibodies to budgerigar antigens. What is the best treatment for this disease?
Inhaled beclomethasone
Oral prednisolone
Inhaled cromolyn
Avoid exposure to birds
Reassurance
146) A 44-year-old male is involved in a serious motor vehicle accident. He is admitted to the intensive care unit with multiple fractures and internal bleeding, and is placed on mechanical ventilation. Over the next two days, his oxygen saturation repeatedly drops below 90%, requiring gradual increases in the FiO2. On day three of his admission, the patient's chest x-ray, which was initially clear, shows bilateral fluffy infiltrates. He has no prior medical problems and does not take any medications. Skin examination reveals no rashes. Lab studies show: Hemoglobin 10.1 g/L, Platelets 160,000/mm3, Leukocyte count 13,500/mm3. Sputum cultures are negative. The ventilator settings are: FiO2 90%, Tidal volume 400 ml (body weight 60 kg), Respiratory rate 12/min, PEEP 5cmH2O. The patient's oxygenation continues to drop below 90%. Which of the following interventions would be best for improving the patient's oxygenation?
Increase the respiratory rate
Increase the tidal volume
Increase the PEEP
Increase the intravenous fluids
Administer packed red blood cells
147) A 65-year-old white man comes to the Emergency Room complaining of headache, insomnia, palpitations, and vomiting. His past medical history is significant for chronic obstructive pulmonary disease (COPD) treated with theophylline, ipratropium, and occasional albuterol. He had a puncture wound of the foot one week ago, and it is being treated effectively with amoxicillin-clavulanate and ciprofloxacin. For the past three days, his shortness of breath is worsening, and his primary care physician gave oral prednisone. His blood pressure is 150/80 mmHg and heart rate is 105/min with frequent ectopic beats. You suspect that drug toxicity may be responsible for this patient's complaints. Which of the following drugs is most likely responsible for his condition?
. Theophylline
. Ipratropium
. Albuterol
. Ciprofloxacin
. Steroids
148) A 67-year-old woman with a past medical history significant for hypertension, hypercholesterolemia, and type 2 diabetes calls 911 for severe shortness of breath. Her symptoms started 2 hours ago with chest pain and progressed rapidly to orthopnea and shortness of breath. Her blood pressure is 170/ 100 mmHg and heart rate is 120/min and regular. A third heart sound is present. Bilateral crackles are heard on chest auscultation. Her oxygen saturation is 78% with 40% inspired oxygen. She is intubated in the field by paramedics for progressive respiratory failure and is treated with nitrates and diuretics. After the initial resuscitation, breath sounds on the left side are markedly decreased. Which of the following is most likely to restore breath sounds to this hemithorax?
. Left-sided chest tube
. Left-sided needle thoracostomy
. Pericardiocentesis
. Endotracheal tube withdrawal
. Tidal volume increase
149) A 55-year-old chronic smoker comes to you because of worsening shortness of breath. He says that he has had lung problems due to smoking for the past five years. He has hypertension controlled with hydrochlorothiazide, and type 2 diabetes mellitus, controlled with diet. He has smoked two packs of cigarettes daily for 25 years. Physical examination shows bilateral decrease in breath sounds with prolonged expiration and wheezing in both the lung fields. He is hypoxic on room air. An x-ray film of the chest shows hyperinflation of both lung fields. His pulmonary function tests showed moderate obstructive disease, with very little bronchodilator response. The patient is started on bronchodilators. He is being considered for home oxygen therapy. Which of the following is a criterion for initiating home oxygen in such patients?
Worsening of shortness of breath
Patients with SaO2 less than 88% on room air
Patients with PaO2 1ess than 65 mmHg on room air
Patients with SaO2 less than 92% on room air
Development of pulmonary osteoarthropathy

150) A 65-year-old white male who has a history of chronic obstructive pulmonary disease, congestive heart failure, and coronary artery disease presented with a three-day history of worsening shortness of breath, cough with yellowish expectoration, and fever. He is not on steroids and does not use oxygen at home. He takes ipratropium, albuterol, aspirin, digoxin, furosemide, metoprolol, and lisinopril. He lives at home with his wife. His temperature is 39.4°C (103°F), blood pressure is 110/70 mmHg, pulse is 110/min, and respirations are 24/min. He is saturating 88% on room air. He was started on 3-liters of oxygen to keep the saturations above 92%. The chest x-ray of the patient is shown below. What is the most appropriate next step in the management of this patient?
Admit the patient and give ampicillin
Outpatient trimethoprim-sulfamethoxazole
Admit the patient and start levofloxacin
Admit the patient and start ciprofloxacin
Admit the patient and start vancomycin
151) A 76-year-old male nursing home resident is hospitalized with confusion, fever and decreased oral intake. His past medical history is significant for type 2 diabetes mellitus, hypertension, osteoarthritis and gout. Blood cultures are positive for E coli. Despite antibiotic therapy, he slips into respiratory failure. He is intubated and placed on mechanical ventilation with an FiO2 of 70%, tidal volume of 500 ml and respiratory rate of 14/min. His current arterial blood gases are: pH 7.45, pO2 59 mmHg, pCO2 30 mmHg, HCO3 21 mEq/L. Which of the following is the best next step in managing this patient?
Increase tidal volume
Increase respiratory rate
Increase the fraction of inspired oxygen
Add positive end-expiratory pressure
Decrease the fraction of inspired oxygen
152) A 45-year-old male with mild persistent asthma comes to you for a routine checkup. He is taking a low-dose beclomethasone inhaler daily and inhaled albuterol, as needed, for the last year. His past medical history is otherwise not significant. His family history is significant for diabetes mellitus type 2, hypertension and obesity. His blood pressure is 136/90 mmHg and his heart rate is 80/min. His BMI is 26 kg/m2. Which of the following is the most likely complication of chronic beclomethasone use in this patient?
. Cushing's syndrome
. Thrush
. Osteoporosis
. Adrenal suppression
. Purpura
153) A 56-year-old morbidly obese man twisted his ankle five days ago and has been bed-ridden since. Today he presents to the emergency department with acute-onset shortness of breath and chest tightness. His past medical history is significant for diabetes mellitus, hypertension, right knee osteoarthritis, and a deep venous thrombosis. His current medications are lisinopril, metoprolol, and metformin. His blood pressure is 110/60 mmHg and his heart rate is 110/min. A CT scan of the chest with contrast is consistent with pulmonary thromboembolism. Which of the following is the best treatment for this patient?
Start heparin now, and in 5-6 days stop heparin and start warfarin
Start both heparin and warfarin now, and stop heparin in 1-2 days
Start heparin and warfarin now, and stop heparin in 5-6 days
Start heparin now and continue for 3-4 weeks
Start warfarin now and continue for at least 6 months
154) A 35-year old male presents to your office complaining of nocturnal wheezing and chest tightness for the past three months. He has also noticed new hoarseness, particularly in the morning. He has no history of bronchial asthma, hypertension or diabetes. He is a non-smoker but occasionally drinks alcohol. On examination, he is an obese male in no acute distress. His pulse is 84/min, blood pressure is 130/80 mmHg, and respirations are 16/min. His chest is clear to auscultation and percussion. Laryngoscopy reveals a red and inflamed posterior pharynx and larynx. Which of the following pharmacotherapies would be most helpful for this patient?
Bedtime fluticasone inhaler
Bedtime albuterol inhaler
Oral theophylline
Oral omeprazole
Oral prednisone
155) A 38-year-old female comes to your office with a recent episode of hemoptysis. The symptoms started one week ago with malaise, throat pain and dry cough. The cough progressed becoming productive of yellowish sputum. She started noticing speckles of red blood in her sputum as of yesterday. Her past medical history is significant for peptic ulcer disease. She has a 5 pack-year smoking history, but she quit 10 years ago. Her temperature is 98°F (36.7°C), blood pressure is 130/80 mmHg and heart rate is 87/min. Physical examination reveals scattered bilateral wheezes. Chest X-ray shows clear lung fields. Which of the following is the most appropriate next step in management?
CT scan of the chest
Pulmonary function tests
Sputum Gram stain and culture
Observation
Sputum cytology
156) A 34-year-old male presents to his physician's office for a routine health maintenance examination. He has a five-year history of bronchial asthma for which he uses an albuterol inhaler. He says that he uses the inhaler an average of two times per week during the day. In addition, he states that his asthma symptoms wake him from sleep approximately 3-4 times per month. He does not use tobacco, alcohol or illicit drugs. His family history is significant for asthma in his grandfather. Physical examination is unremarkable. Which of the following is the most appropriate next step in his management?
Add long-acting beta-2 agonist inhaler
Add inhaled corticosteroids
Add oral theophylline
Add oral prednisone
Continue current medical regimen
157) A 19-year woman presents to her physician's office for a routine health maintenance examination. She notes experiencing occasional wheezing and breathlessness following aerobic exercise, but has no symptoms at other times of the day or night. Her medical history is otherwise significant for allergic rhinitis and acne, for which she uses topical benzoyl peroxide and erythromycin cream. She does not use tobacco, alcohol or illicit drugs. On physical examination, her vital signs are within normal limits and chest auscultation is unremarkable. Which of the following is the most appropriate next step in her management?
Beta-adrenergic agonists before exercise
Daily oral steroids
Daily steroid inhalers
Daily oral theophylline
Lpratropium inhalers before exercise
158) A 57-year-old male was involved in a motor vehicle accident and was immediately brought to the Emergency Room. He suffered minor head and neck injury, but was found to have a broken tibia. He underwent repair of the tibial fracture the following day. Five days later, he suddenly develops tachycardia and is tachypneic. He complains of increasing chest discomfort and has a syncopal episode. His blood pressure is 80/55 mmHg, pulse is 130/min, and respirations are 24/min. Pulse oximetry showed 82% on room air. Stat echocardiogram reveals obstruction in the main pulmonary artery. Which of the following choices is the most appropriate course of action?
Heparin infusion
Fibrinolytic therapy
Embolectomy
Inferior vena cava filter
A CT scan of the lung
159) A 68-year-old female comes to the Emergency Room with increased shortness of breath and cough for 12 hours. She has a history of chronic obstructive pulmonary disease for the past 14 years and has been oxygen dependent for two years. Twelve hours ago, she felt unable to get her breath. She took two extra nebulizer treatments and used her as-needed inhaler with no relief of symptoms. She denies any fever, chills, sweating, nausea or vomiting, and hemoptysis. She rarely uses alcohol, but had smoked two packs/day for 45 years. She quit smoking about six years ago. Her medications include ipratropium, albuterol, multivitamins, and oxygen 2 liters/min by nasal cannula. She is a thin, frail female in moderate distress. Her temperature is 36.7°C (98°F), blood pressure is 110/65 mmHg, pulse is 110/min, and respirations are 28/min. Pulse oximetry shows 84% on 2 liters oxygen by nasal cannula. The patient is given oxygen, methyl prednisolone, aerosolized ipratropium, and albuterol; however, the patient remains dyspneic and bedridden. ABGs are ordered and the results show: pH 7.32, PCO2 60 mmHg, and PO2 52 mmHg on 4-liters O2. What is the next best step in the management of this patient?
Increase oxygen by nasal cannula
Decrease oxygen
Intubate and mechanically ventilate the patient
Noninvasive positive pressure ventilation
Aminophylline
160) A 68-year-old male is hospitalized following an intracerebral hemorrhage. On hospital day 3, he develops redness, swelling, and tenderness of the left calf. There is no fever. Compression ultrasonography reveals a thrombus in the popliteal vein. Which of the following is the most appropriate next step in the management of this patient?
Anticoagulation with heparin
Thrombolytic therapy
Placement of an inferior vena cava filter
No treatment for his deep vein thrombosis
Compression stockings
161) A 66-year-old man complains of exertional dyspnea that has progressed over the last two years. As a result, he has had to limit his physical activities to avoid becoming short of breath. He denies any significant chest pain, but does note having a recurrent cough productive of whitish sputum. His past medical history is significant for hypertension controlled with hydrochlorothiazide. He has a 40 pack-year smoking history. His family history is significant for a stroke in his mother. His blood pressure is 160/90 mmHg and his heart rate is 80/min. Physical examination reveals a mildly overweight patient in no acute distress. His anteroposterior chest diameter is markedly increased. Breath sounds are decreased bilaterally with scattered expiratory wheezes. Which of the following agents is most likely to reduce this patient's symptoms?
Alpha-adrenergic blocker
Beta-adrenergic blocker
Muscarinic antagonist
Dopamine agonist
Alpha 2-adrenergic agonist
162) A 64-year-old male presents to the physician's office with increasing shortness of breath. He denies orthopnoea, paroxysmal nocturnal dyspnea, or chest pain. He was hospitalized for pneumonia four years ago but has otherwise been healthy. He has smoked one pack of cigarettes daily for the past 30 years. He does not take any medications. His temperature is 37.2°C (98.9°F), blood pressure is 124/76 mm Hg, pulse is 82/min and respirations are 16/min. Pulse oximetry reveals an oxygen saturation of 88%. On chest auscultation, breath sounds are diminished throughout, and the expiratory phase is prolonged. Heart sounds are regular and there are no murmurs or gallops. There is no peripheral edema or jugular venous distention. Laboratory studies show a hematocrit of 56% and WBC count of 6,700/mm3. Which of the following interventions will have the maximum impact on this patient's survival?
Maintenance oral steroids
Prophylactic antibiotics to reduce exacerbations
Influenza and pneumococcal vaccinations
Long-term supplemental oxygen therapy
Long-term beta-blocker therapy
163) A 47-year-old male who has just returned from a cruise to the Bahamas presents to the hospital with a high-grade fever, productive cough and shortness of breath for the past two days. He also complains of frequent vomiting and diarrhea. He has no prior medical problems, does not take any medications, and denies using tobacco, alcohol or drugs. His temperature is 40°C (104°F), blood pressure is 110/65 mm Hg, pulse is 80/min, and respirations are 18/min. Lung examination reveals right lower lobe crackles. The abdomen is soft and non-tender. Chest x-ray demonstrates right lower lobe consolidation. Sputum Gram stain contains many neutrophils with no organisms. Which of the following antibiotics must be given to this patient?
. Vancomycin
. Clindamycin
. Fluconazole
. Amoxicillin
. Azithromycin
164) A 36-year-old female presented to the emergency room with fever and a productive cough. The physician on call suspected community acquired pneumonia and prescribed azithromycin for 5 days. After 5 days of treatment, she comes to your office with no improvement of her symptoms and complains of worsening foul smelling sputum. Further inquiry reveals that she had undergone an upper GI endoscopy 8 days ago for a long history of heartburn and suspected peptic ulcer disease. She also reports a history of manic-type bipolar disorder. In your office she has a blood pressure of 130/80 mm Hg, her pulse is 108/min, temperature is 38.7°C (101.6°F) and respirations are 26/min. Chest x-ray showed a right upper lobe infiltrate. Which of the following additional therapies would be most helpful for this patient's condition?
. Doxycycline
. Ciprofloxacin
. Trimethoprim-sulfamethoxazole
. Clindamycin
. Gentamicin+ ampicillin
165) A 45-year-old male comes to the emergency room complaining of shortness of breath that began 3 hours ago. He also has a nonproductive cough, a low-grade fever and right-sided chest pain that worsen with inspiration. He denies coughing up blood, wheezing, palpitations, leg pain or swelling of his lower extremities. He recently returned home from a trip to Singapore. He has a history of hypertension and diabetes mellitus. His takes fosinopril, metformin and glyburide. He doesn't use tobacco, alcohol or illicit drugs. His temperature is 98.0°F (36.6°C), blood pressure is 115/70 mmHg, pulse is 128/min, respirations are 32/min, and O2 saturation is 84% on room air. Physical examination shows a slightly obese man in acute respiratory distress. He is alert and cooperative without any cyanosis or jaundice. He has a slightly displaced apical impulse with a S4. Chest-x ray shows mild cardiomegaly with no infiltrates. EKG shows sinus tachycardia and left ventricular hypertrophy without ST-T wave changes. His arterial blood gas analysis shows pH 7.52, pCO2 30, pO2 55, HC03 22. What is the next best step in the management of this patient?
Pulmonary angiogram
Lower extremity venous ultrasound
Spiral CT scans of the chest
Initiate heparin weight-based protocol
Broad spectrum antibiotics
166) A 65-year-old male with oxygen-dependent chronic obstructive pulmonary disease, chronic atrial fibrillation, and depression comes into the Emergency Room, with symptoms of increased dyspnea and worsening cough pattern. His recent history had been significant for a gradual worsening of his baseline lung disease over the past month, which had been treated by his outpatient doctor with increased frequency of inhaled beta-agonist and azithromycin. This morning he had a severe shortness of breath that was unresponsive to "stacked" home nebulizer treatments. The ER physician notes that the patient is in moderate severe respiratory distress. His temperature is 37.2°C (99°F), blood pressure is 150/90 mmHg, pulse is 110/min, and respirations are 28/min. Accessory muscle use was noted. Lung exam shows diffuse rhonchi and wheezing. A pulse oximetry revealed an oxygen saturation of 80% on room air. His chest x-ray showed no new infiltrates. His WBC count is 7,000/cmm with normal differential. The ER physician had given nebulization, and the patient is on 5-liters of oxygen. Which of the following should also be considered in this patient?
. Gatifloxacin
. Methylprednisolone
. N-acetylcysteine
. Clarithromycin
. Aminophylline
167) A 32-year-old man presents to the emergency department with pain and swelling in the right leg. He was recently hospitalized for a right lower extremity deep venous thrombosis and discharged on warfarin. Today his INR is 1.12. Ultrasound reveals a right popliteal vein thrombosis extending into the deep femoral vein. What is the best initial management step for this patient?
. Increase warfarin dose for goal INR > 2.0
. Start intravenous unfractionated heparin
. Initiate thrombolytic therapy
. Place inferior vena cava filter
. Discontinue warfarin and reassure
168) A 50-year-old female comes into your office complaining of four-month history of dry cough. She denies dyspnea or hemoptysis. Past medical history is significant for hypertension, diabetes, and gout. Her current medications include enalapril, metformin, hydrochlorothia zide, and allopurinol. She does not smoke or consume alcohol. Her vital signs are BP 130/80 mmHg, HR 80/min, T 36.7°C (98°F) and RR 16/min. Physical examination is within normal limits. The best next step in the management of this patient is:
. Chest radiograph
. Reevaluation of drug therapy
. Pulmonary function testing
. Barium esophagography
. Bronchoscopy
169) A 45-year-old white man presents to your office complaining of daytime somnolence, increased fatigability, and morning headaches. He says that his wife complains that he snores loudly. He is not taking any medications and does not smoke or consume alcohol. His blood pressure is 145/90 mmHg and heart rate is 90/min. Physical examination reveals a well-nourished man with BMI = 31 kg/m2. What is the next best step in the management of this patient?
. A benzodiazepine to improve sleep
. Advise to sleep in supine position
. Weight reduction
. A thiazide diuretic for hypertension
. Tracheostomy
170) A 43-year-old previously healthy male is hospitalized for acute pancreatitis. On day 3 of his admission, he develops respiratory distress. He is transferred to the intensive care unit and intubated. His initial ventilator settings are: FiO2 0.8 (80%), Respiratory rate 10/min, Tidal volume 500 ml, PEEP 5 mm H20. Ten minutes after being intubated, the man's blood pressure is 110/70 mmHg and his heart rate is 90/min. His arterial blood gases are: pH 7.42, pO2 105 mmHg, pCO2 37 mmHg. Which of the following is the best next step in the management of this patient?
. Decrease the positive end expiratory pressure (PEEP)
. Decrease the tidal volume
. Decrease the FiO2
. Decrease the respiratory rate
. Increase the respiratory rate
171) A 35-year-old male was involved in a motor vehicle injury and suffered serious chest trauma. A chest tube was placed for a hemothorax. 800 cc of blood was evacuated from the chest, and, after ten days, the patient was discharged home. He returns again with a low-grade fever and dyspnea. CT scan reveals a complex loculated effusion with a thick surrounding peel. A chest tube is placed; however, after 24 hours, there is little drainage, and the patient continues to have a low-grade fever. What is the next step in his management?
. Surgery
. Streptokinase into the chest tube
. Increase the dose of IV antibiotics
. Place a second chest tube
. Pulmonary consult for bronchoscopy
172) A 40-year-old white male develops a proximal deep vein thrombosis in the left lower extremity. Detailed history, examination and lab testing fail to reveal any obvious cause or risk factor for his deep venous thrombosis. Idiopathic deep vein thrombosis is diagnosed and the patient starts a 6-month course of warfarin anticoagulation. What is the goal INR therapeutic range in this patient?
. 1.0 to 1.5
.1.5to2.0
. 2.0 to 3.0
. 2.5 to 3.5
. Greater than 4
173) An obese 56-year-old female presents to her physician concerned that her asthma is worsening. She describes night-time cough and wheezing that have been increasing over recent months. She also reports feeling tired each morning because she works late hours and has no time to relax after dinner. On review of systems, the patient denies dyspnea on exertion, but acknowledges that her throat has been sore lately. Her past medical history is significant for bronchial asthma, type2 diabetes and hypertension. Her medications include an albuterol inhaler which she uses occasionally, lisinopril and aspirin. Her vital signs are within normal limits, and there are no abnormalities on physical exam. Which of the following is the most appropriate next step in the management of this patient?
. Discontinue lisinopril
. Discontinue aspirin
. Add inhaled fluticasone
. Add pantoprazole
. Add salmeterol

174) A 60-year-old Caucasian female comes to the physician because of progressive shortness of breath for the past month. She has had a 13.6 kg (30 lb) weight loss during this period. She has a history of hypertension and hypothyroidism and takes metoprolol and levothyroxine. She has smoked two packs of cigarettes daily for 35 years. Her temperature is 36.7°C (98°F), blood pressure is 130/70 mmHg, pulse is 80/min, and respirations are 20/min. On examination, decreased breath sounds and dullness to percussion are noted on the right, middle and lower lobes of the lung. Her chest x-ray is shown below. Which of the following is the most appropriate next step in the management?
. Bronchoscopy
. Mediastinoscopy
. Thoracentesis
. Video-assisted thoracoscopy
. Open pleural biopsy
175) A 46-year-old male is hospitalized with severe acute pancreatitis. Because of progressive respiratory difficulty, he is intubated and placed on mechanical ventilation. His weight is 70 kg (152 lb), blood pressure is 110/70 mmHg, and heart rate is 90/min. Chest x-ray shows patchy opacities bilaterally, consistent with pulmonary edema. His current ventilator settings are: assist control mode, respiratory rate of 12/min, tidal volume of 450 ml, FiO2 of 40%, and positive end-expiratory pressure (PEEP) of 5 cm H20. His blood gas readings are: pH 7.51, pCO2 22mmHg, pO2 121mmHg. Which of the following is the best next step in managing this patient?
. Bronchodilator therapy
. Decrease FiO2
. Decrease respiratory rate
. Increase tidal volume
. Incentive spirometry
176) A 69-year-old male presents to the ER with severe shortness of breath for the past 12 hours. He reports that he has used his albuterol inhaler many times without relief. On review of systems he notes having had a mild fever yesterday that resolved with acetaminophen. The patient quit smoking 2 years ago but has a 100 pack year smoking history. On physical examination, his blood pressure is 150/90 mmHg and heart rate is 110/min. The patient is using accessory muscles of respiration. Expirations are prolonged, and there are wheezes bilaterally. Arterial blood gas (ABG) analysis reveals the following: pH 7.36, pO2 64 mmHg, pCO2 57 mmHg, HCO3 32 mEq/L. The patient is treated with ipratropium and albuterol nebulizers and moxifloxacin. Which of the following additional therapies is most likely to benefit this patient?
. Corticosteroids
. Loop diuretic
. Mucolytic agents
. Aminophylline
. Diltiazem
177) A 28-year-old male presents to the physician's office for a routine health maintenance examination. He has a two-year history of bronchial asthma for which he uses an albuterol inhaler. He states that he experiences asthma symptoms an average of 2 times per week, for which his albuterol inhaler provides relief. He has not had nighttime awakenings over the past month. He does not use tobacco, alcohol or illicit drugs. His family history is significant for asthma in his grandfather. Physical examination is unremarkable. Which of the following is the most appropriate next step in his management?
. Add long-acting beta-2 agonist inhaler
. Add inhaled corticosteroids
. Add oral theophylline
. Add oral prednisone
. Continue current medical regimen
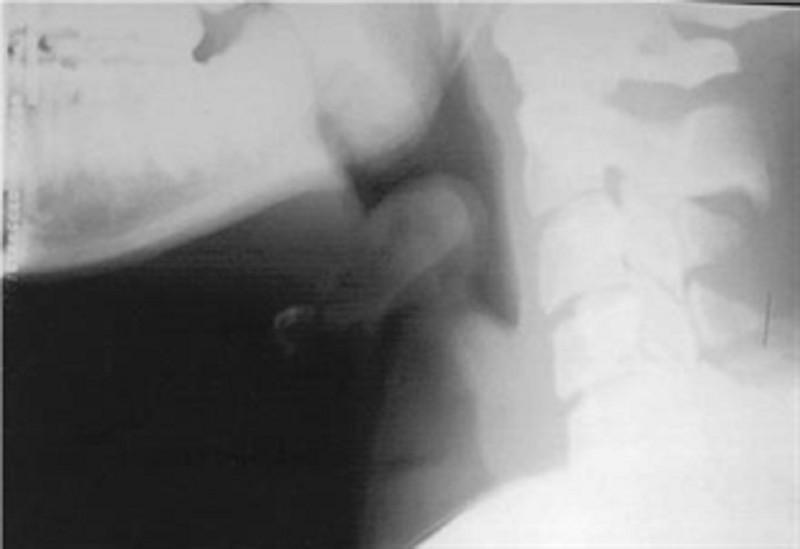
178) A 3-year-old boy presents to the emergency department with a fever and difficulty breathing. He is the product of a normal pregnancy and has been healthy since birth. His immunizations are up to date. This morning he appeared to be in his usual state of health and was dropped off at day care by his father. Later on, his teacher noticed that he had suddenly become fussy and flushed and could not be consoled with toys, rocking, or hearing a story. He also felt warm to the touch and was drooling more than usual. When she took his temperature, it was 39°C (102.2°F). His parents were contacted immediately, and the patient was brought to the emergency department. He appears toxic and anxious, and has loud labored breathing. He is sitting upright, bracing himself on his arms, with his neck hyperextended and mouth open. His temperature is 40°C (104°F), respiratory rate is 50/min, pulse is 140/min, blood pressure is 102/62 mm Hg, and oxygen saturation is 100% on room air. Lateral x-ray of the neck is shown in the image. Laryngoscopy reveals a large cherryred epiglottitis. What is the most appropriate next step in management?
Antibiotic therapy
Corticosteroids
Nasotracheal intubation
Tracheostomy
Observation
179) A 35-year-old homeless man presents to the emergency department with chief complaints of a cough and fever. He is intoxicated. He admits to drinking about a fifth of vodka every day and confirms a history of delirium tremens and blackouts. X-ray of the chest is significant for an air-fluid level in the superior segment of the right lower lobe. Which of the following is the most appropriate first-line agent for treating this patient’s condition?
Azithromycin
Clindamycin
Isoniazid
Moxifloxacin
Piperacillin-tazobactam
180) An agitated and nervous 24-year-old woman has had severe wheezing and shortness of breath for 2 days. After receiving oxygen, steroids, and salbutamol (Ventolin) in the emergency room, her breathing improves. She is still wheezing and now feels tremulous and anxious with a pulse of 110/min and respirations 30/min. Arterial blood gases on oxygen reveal a pH of 7.40, PO2 340 mm Hg, PCO2 40 mm Hg, and bicarbonate of 24 mEq/L. She is hospitalized for further treatment. Which of the following treatments or medications should be avoided in her?
Theophylline
Sedatives
Corticosteroids
Sympathomimetic amines
Intravenous (IV) fluids
181) A 29-year-old woman has a long history of mild asthma. She now has a flare and experiences recurrent episodes of bronchial obstruction, fever, malaise, and expectoration of brownish mucous plug. On examination, there is bilateral wheezing. Infection is suspected and a CXR reveals upper lobe pulmonary infiltrates. The eosinophil count is 2000/mL, and serum precipitating antibodies to Aspergillus are positive. Which of the following is the most appropriate next step in management?
Antihelminthic therapy
A short course of systemic glucocorticoid therapy
Desensitization treatment
High-dose glucocorticoids by puffer
Long-term systemic glucocorticoid therapy
182) A 31-year-old African American man presents with dyspnea on exertion. He also has fever and red tender rash on his shins. Physical examination reveals fine inspiratory crackles in both lower lung lobes and tender erythematous nodules on his legs. CXR shows bilateral hilar adenopathy and reticulonodular changes in both lungs. Transbronchial biopsy reveals noncaseating granulomas. Which of the following is the most appropriate next step in management?
Aspirin
Isoniazid (INH) and streptomycin
Steroids
Nitrogen mustard
No therapy
{"name":"Part 46", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"118) A 61-year-old Caucasian male presents with ptosis, diplopia and limb weakness. These symptoms worsen in the evening and with exercise, and improve with rest. He also has fatigue, which is worse in the evening. He denies any tingling or numbness. On examination, he cannot sustain an upward gaze, and his eyelids tend to drift downward. Injection of edrophonium quickly restores power, and allows him to maintain an upward gaze. Which of the following is the best initial treatment for this patient?, 119) A 7-year-old boy is brought to the office by his mother because, \"he is always daydreaming.\" Sometimes, he stares for a few seconds and rolls his eyes for unknown reasons. His teacher has noted a recent decline in his school performance. He has no family history of any seizure disorder, and his psychomotor development is normal. His neurological examination is unremarkable. EEG during hyperventilation shows generalized, symmetrical 3-Hz spike-and-wave activity on a normal background. Which of the following medications is the most appropriate to treat the boy's disorder?, 120) A 32-year-old Caucasian male comes to the emergency department due to progressive ascending paralysis, which began 18 hours ago. He initially noticed paresthesias in his lower limbs, followed by a sense of fatigue and weakness. He denies any history of headache, fever, and recent infection or illness. His blood pressure is 120\/80 mm Hg, pulse is 80\/min, respirations are 16\/min, and temperature is 37.3°C (99.2°F). The physical examination reveals intact cranial nerves, absent deep tendon reflexes, and a normal sensory exam. Laboratory studies reveal a normal WBC count. No abnormalities are noted on CSF examination. While evaluating the patient in the hospital, he quickly deteriorates. What is the most appropriate next step in the management of this patient?","img":"https://cdn.poll-maker.com/11-487509/for-student-des-2016-2017-last-pdf---adobe-reader.bmp?sz=1200"}
More Quizzes
RBA Awareness
210
The Paw patrol quiz
1166
Discover the Wonders of Harappan Culture
52117
How greedy are you?
630
Fire Doors Help Combat Fires Because... - Free Practice
201018451
How Digital Are You? Free to Find Your Online Persona
201022122
What Golf Irons Should I Buy? Free to Find Your Fit
201018451
East Asia Physical Map - Free Online Practice
201024467
NRP - Free Practice for Certification Exam
201024646
Color by Number Physical & Chemical Changes Answer Key
201020066
Which Primarch Are You? Warhammer 40K Personality
201020282
AFI 10-201 - Test Your Air Force Knowledge
201023781