
VIII. NEPHROLOGY & ELECTROLYTE

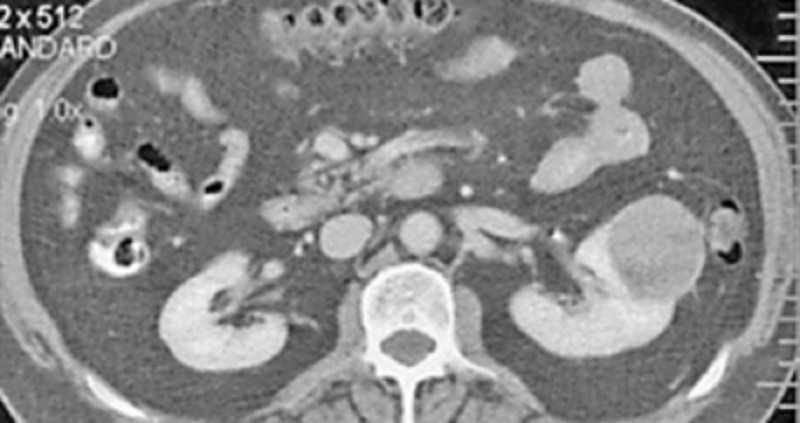
61. A healthy 54-year-old man comes to the physician for a routine health maintenance examination. He has no complaints, but he is requesting for a CT scan of the abdomen. His father died at the age of 60 due to the sudden rupture of an undiagnosed abdominal aortic aneurysm. He has a history of hypertension and gouty arthritis. His social history is not significant. His vital signs are stable. Physical examination shows no abnormalities. ACT scan of the abdomen is shown below. Which of the following is the most appropriate next step in management?
A. Reassurance
B. Surgery
C. CT guided biopsy
D. Antibiotics
E. Repeat CT scan in 3 months
62. A 30-year-old woman comes to the office due to the recent onset of fever, chills, and dysuria. Her temperature is 38.3C (101.0F), blood pressure is 110/70mm Hg, pulse is 68/min, and respirations are 15/min. Examination shows tenderness at the right costovertebral angle. Laboratory studies show WBC count of 16,000/microl with left shift. Urinalysis shows bacteriuria and pyuria. Her urine and blood is collected for culture and sensitivity. She is prescribed oral ciprofloxacin and sent home. After three days, she returns for a follow-up visit. She is still febrile, and the physical examination is unchanged. The blood cultures have no growth after 72 hours of incubation. Results of the urine culture show: Which of the following is the most appropriate next step in management?
A. Start intravenous ampicillin and gentamicin
B. Start intravenous ciprofloxacin
C. Continue oral ciprofloxacin for another 10 days
D. Perform renal ultrasound
E. Renal CT scan
63. A 62-year-old woman presents to your office complaining of urinary frequency and burning during urination. She denies fever, chills, nausea, back pain or abdominal pain. Her past medical history is significant for a long history of diabetes mellitus and hypertension. She does not use tobacco or consume alcohol. Her blood pressure is 160/100 mmHg and her heart rate is 70/min. Her hematocrit is 43% and her WBC count is 8,500/mm3 Urinalysis reveals the following: Glucose negative Ketones negative Nitrates positive Protein 2+ WBC 20-25/hpf RBC 3-5/hpf She is given a three-day course of levofloxacin. Urinalysis two weeks later reveals 2+ protein but no nitrates, WBCs, or RBCs. Which of the following is most likely responsible for her persistent urinalysis abnormality?
A. Atherosclerotic narrowing of the renal arteries
B. Glomerular basement membrane changes
C. Cystic transformation of the renal parenchyma
D. Parenchymal atrophy due to calyceal dilation
E. Insoluble crystal precipitation in the tubular lumen
64. A 72-year-old woman with poorly controlled type 2 diabetes mellitus presents to your clinic one week after being discharged from the hospital. She had been admitted with pyelonephritis secondary to a multi-drug resistant organism, and received several days of intravenous antibiotics. Her serum creatinine on admission had been 2.1 mg/dl. Today it is found to be 4.9 mg/dl. Urinalysis reveals rare epithelial casts and no white blood cells. FENa is greater than 2%. What antibiotic did she most likely receive during her hospitalization?
A Nafcillin
B. Vancomycin
C. Levofloxacin
D. Amikacin
E. Doxycycline
65. A 58-year-old man comes to the physician and complains of "problems with erection." He has recurrent and persistently painful erections. His other medical problems include ulcerative colitis, kidney stones, insomnia, depression, hypertension, drug-induced diabetes, obesity and hypercholesterolemia. He does not use tobacco, alcohol, or drugs. He takes prednisone, mesalamine, insulin, 6-mercaptopurine, simvastatin, glyburide, enalapril, trazodone, and fluoxetine. He has no known drug allergies. His vital signs are stable. The general physical examination is unremarkable. Avoidance of which of the following medications could have prevented his condition?
A. Fluoxetine
B. Trazodone
C. Enalapril
D. Glyburide
E. Simvastatin
66. A 60-year-old man comes to the physician because of a 2-day history of fever and left-sided scrotal pain. The pain has progressed in severity and it radiates to the flank. His has also had increased urinary frequency and urgency along with dysuria. His temperature is 38.1C (100.8F), blood pressure is 130/75mm Hg, pulse is 86/min, and respirations are 15/min. Physical examination shows left scrotal swelling and a tender scrotal mass; there is no urethral discharge. Rectal examination shows a tender prostate. Laboratory studies show a WBC count of 14,000/microl with a left shift. Urinalysis shows bacteriuria and pyuria. Which of the following is the most likely organism responsible for this patient's findings?
A. Escherichia coli
B. Pseudomonas
C. Chlamydia trachomatis
D. Gonococcus
E. Staphylococcus aureus
67. A 40-year-old man comes to the physician because of increasing urinary frequency and urgency. He has had these symptoms in the past, but they are more troublesome now. He has also had urinary hesitancy and interruption of flow. His temperature is 37C(98.6F), blood pressure is 130/75mm Hg, pulse is 76/min, and respirations are 15/min. Physical examination shows no abnormalities except increased tone of the anal sphincter and mild periprostatic tenderness. Urinalysis and urine culture shows no abnormalities and expressed prostatic secretions show a leukocyte count of four WBCs/HPF (normal is less than 10 WBCs/HPF). Serum prostate-specific antigen is 2 ng/ml (normal value is less than 4ng/ml). Which of the following is the most likely diagnosis?
A. Chronic bacterial prostatitis
B. Inflammatory chronic prostatitis
C. Non-inflammatory chronic prostatitis
D. Prostatic cancer
E. Acute bacterial prostatitis
68. A 16-year-old girl presents with a 2-day history of lower abdominal discomfort, burning micturition and increased frequency of urination. She had her first sexual intercourse last week. Her vital signs are stable. Examination shows suprapubic tenderness. Urinalysis shows positive nitrites, positive esterase, 50+ WBC, and many bacteria. Which of the following is the most likely mechanism responsible for her clinical condition?
A. Sexual transmission
B. Hematogenous spread of infection
C. Lymphatic spread of infection
D. Poor genital hygiene
E. Ascending infection
69. A 68-year-old Caucasian man is admitted with a diagnosis of left lower lobe pneumonia, and is started on gatifloxacin. He has a long history of diabetes, hypothyroidism, hypercholesterolemia, and hypertension. He also has diabetic retinopathy, peripheral neuropathy, and nephropathy. He has an arterio-venous fistula placed for a possible dialysis. His medications are insulin, furosemide, atorvastatin, metoprolol and levothyroxine. After having his blood drawn for some laboratory studies today, he bleeds persistently. Laboratory studies show: Hb 11.5 g/dl Platelets 160,000/cmm Blood glucose 178 mg/dl BUN 56 mg/dl Serum creatinine 3.5 mg/dl His baseline creatinine level is between 3.2-3.5 mg/dl. Which of the following is the most likely cause of his bleeding?
A. Disseminated intravascular coagulation
B. Platelet dysfunction
C. Factor VIII deficiency
D. Consumptive coagulopathy
E. Thrombocytopenia
70. A 64-year-old man is scheduled for hemodialysis due to end stage renal disease. He has a several year history of hypertension, diabetes, coronary artery disease, hypercholesterolemia, peripheral vascular disease, gout, and diverticulosis. Six months ago, he was admitted for urosepsis. Recently, his haemoglobin has ranged between 8.5 to 9.5 g/dl. He has already been on iron therapy, and now you are considering erythropoietin injections twice weekly. Which of the following is most likely to be seen following erythropoietin therapy?
A. Worsening of his hypertension
B. Increase in insulin requirement
C. Increased susceptibility to infections
D. Deterioration in renal function
E. Flare-up of gout
71. A 70-year-old man is brought to the hospital by his son because of worsening fatigue. His son states that his father does not like seeing doctors and has not seen a physician in the past 20 years. He has no medical problems. Physical examination of the prostate shows no abnormalities. Laboratory studies show: Hb 10.5 g/dl WBC 7,400/cmm Platelets 160,000/cmm Serum Na 135 mEq/L Serum K 5.0 mEq/L BUN 50 mg/dl Serum creatinine 3.0 mg/dl Ultrasonogram of the abdomen shows bilateral small kidneys and no evidence of hydronephrosis. Kidney biopsy shows intimal thickening and luminal narrowing of renal arterioles with evidence of sclerosis. Which of the following is the most likely cause of this patient's findings?
A. Hypertension
B. Diabetes mellitus
C. Multiple myeloma
D. Analgesic abuse
E. Renal lithiasis
72. A 30-year-old woman comes to the physician due to the recent onset of occipital headaches. She has taken acetaminophen several times, but the pain returns. She has no fever or visual problems. She has not had similar episodes in the past. She has no history of serious illness. Her temperature is 36.1C (98F), blood pressure is 160/90 mm Hg, pulse is 88/min, and respirations are 16/min. Physical examination shows a rightsided renal bruit Which of the following is the most appropriate treatment for this patient's condition?
A. ACE inhibitors
B. Furosemide
C. Angioplasty with stent placement
D. Surgery
E. Oral prednisone
73. A 45-year-old man with known cirrhosis due to hepatitis C is admitted to the hospital for abdominal discomfort and confusion. Physical examination reveals a distended abdomen, leg edema, and deep yellow discoloration of the skin and sclerae. Bibasilar crackles are heard on chest auscultation. His serum sodium level is 127 mEq/L, potassium level is 2.9 mEq/L, and creatinine level is 1.3 mg/dl. On day 3 of his hospitalization, the serum creatinine is 4.2mg/dl. A urinalysis reveals: Protein negative Glucose negative WBC 4-5/hpf RBC 0-1/hpf Renal ultrasound is normal and the post-void residual urinary volume is less than 50 ml. He is given 2 L of normal saline intravenously with no change in his serum creatinine concentration. This patient's kidney dysfunction can be best corrected by which of the following?
A. High-dose spironolactone
B. ACE inhibitors
C. Liver transplantation
D. Broad spectrum antibiotics
E. Pegylated interferon
74. A 35-year-old woman who recently emigrated from Russia comes to the physician because of hematuria. She has a history of frequent headaches. Extensive evaluation did not reveal the cause of her headaches. They occur almost every day, and she tried various analgesics to relieve them. Her family history is significant for hypertension and diabetes mellitus. She does not use tobacco, alcohol, or drugs. Her blood pressure is 120/70 mm Hg and heart rate is 80/min. Physical examination shows no abnormalities. Urinalysis shows numerous unchanged red blood cells/hpf. Which of the following is the most likely cause of this patient's condition?
A Malignancy
B. Glomerular injury
C. Papillary necrosis
D. Infection
E. Nephrolithiasis
75. A 73-year-old man presents to the emergency department complaining of lower abdominal pain and nausea. He denies any vomiting or diarrhea, and his last bowel movement was two days ago. The patient also notes that several days ago he began taking amitriptyline for chronic neck pain. He does not smoke or consume alcohol. On physical examination, his blood pressure is 160/70 mmHg and his heart rate is 100/min. His lung fields are clear to auscultation. Palpation of the abdomen reveals fullness and tenderness along the midline below the umbilicus. Which of the following is the best initial management for this patient?
A. Abdominal CT scan
B. Upright abdominal x-ray
C. Barium enema
D. Broad spectrum antibiotics
E. Urinary catheterization
76. A 55-year-old woman comes to the physician for an annual physical examination. She has no new complaints, except fatigue. She has an 8-year history of chronic low back pain; severe degenerative joint disease has been documented on MRI. She had an anterior wall myocardial infarction four years ago. Her current medications include naproxen, acetaminophen, oxycodone, aspirin, atenolol, and simvastatin. Her blood pressure is 130/80 mm Hg and pulse is 72/min. Laboratory studies show: Hb 10 g/dl WBC 6,000/cmm Blood sugar 82 mg/dl BUN 36 mg/dl Serum creatinine 2.0 mg/dl Urinalysis : Protein 2+ Glucose Absent RBC Absent WBC 10-15/HPF Nitrite Negative Esterase Negative Sediment WBC casts Serum protein electrophoresis is negative for monoclonal gammopathy. Two years ago, her BUN level was 22 mg/dl, and creatinine level was 1.6 mg/dl. Which of the following is the most likely pathology involved in this patient's renal failure?
A. Acute tubular necrosis
B. Chronic glomerulonephritis
C. Tubulointerstitial nephritis
D. Recurrent pyelonephritis
E. Renal tuberculosis
77. A 56-year-old man develops oliguria three days after having a kidney transplantation. His postoperative course was uncomplicated. His blood pressure is 160/100 mm Hg and heart rate is 90/min. Palpation of the transplant reveals mild tenderness. Laboratory studies show: Serum sodium 145 mEq/L Serum potassium 5.5 mEq/L Serum calcium 8.6 mg/dl Serum creatinine 3.2 mg/dl BUN 30 mg/dl His serum cyclosporine level is normal. Renal ultrasonography does not detect dilatation of the calyces. Biopsy of the transplant shows heavy lymphocyte infiltration and vascular involvement with swelling of the intima. Which of the following is the most appropriate next step in management?
A. Decrease the dose of cyclosporine
B. Give IV steroids
C. Order ureterography
D. Administer IV diuretics
E. Prepare for surgery
78. A 50-year-old man comes to the physician for a routine follow-up visit. He has hypertension, diabetes mellitus, secondary hyperparathyroidism, and end-stage renal disease. He has been on hemodialysis for the past three years. He was admitted three months ago for line sepsis, which was treated with antibiotics. He had a right below-the-knee amputation two years ago following a non-healing foot ulcer. Physical examination shows a right carotid bruit. If this patient dies within the next five years, what would be the most likely cause of his death?
A. Cardiovascular disease
B. Stroke
C. Infection
D. Cancer
E. Withdrawal from dialysis
79. A 15-year-old boy comes to the physician because of hematuria and lower abdominal pain. This is his third episode of hematuria in the past 2 years. He has a family history of renal disease. His temperature is 37.1 C (98.9F), blood pressure is 140/90 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows mild sensorineural deafness bilaterally. Urinalysis shows hematuria and proteinuria. Laboratory studies show BUN of 50 mg/dl and serum creatinine of 3.1 mg/dL; serum complement levels are normal. Renal biopsy shows foam cells, and immunofluorescence shows no immunoglobulins or complement. Electron microscopy shows alternating areas of thinned and thickened capillary loops with splitting of GBM. Which of the following is the most likely diagnosis?
A. Alport's syndrome
B. Acute interstitial nephritis
C. Acute post infectious glomerulonephritis
D. Anti-glomerular basement membrane disease
E. Benign recurrent hematuria
80. A 25-year-old woman comes to the physician because of a 3-day history of burning micturition and increased urinary frequency. She has suprapubic discomfort. She denies having unusual vaginal discharge. She has been sexually active and monogamous for the past 4 years with her husband. Her temperature is 37.1 C (98.9F), blood pressure is 110/70 mm Hg, pulse is 68/min, and respirations are 15/min. Examination shows suprapubic tenderness without flank tenderness. The rest of the examination is normal. Urinalysis shows: Specific gravity 1.020 Blood Trace Glucose Negative Ketones Negative Leukocyte esterase Positive Nitrites Positive WBC 40-50/hpf RBC 6-10/hpf Bacteria 50+ Which of the following is the most appropriate next step in management?
A. Urine culture
B. Oral trimethoprim-sulfamethoxazole
C. Oral ciprofloxacin
D. Oral nitrofurantoin
E. Intravenous trimethoprim-sulfamethoxazole
81. A 57 -year-old woman is admitted to the ICU after being involved in a highway motor vehicle accident. She was hypotensive at the scene and received 7 litters of fluids, which included crystalloids, blood, and fresh frozen plasma. She apparently had significant external blood loss from multiple fractures and skin loss. She undergoes surgery, after which she is transferred to the ICU and receives continuous IV fluids and vasopressors. Her laboratory studies 24 hours after the accident show the following: Hb 9.5 g/dl WBC 15,000/cmm Platelets 130,000/cmm BUN 34 mg/dl Serum Creatinine 2.2 mg/dl Which of the following is the most likely microscopic finding on urinalysis?
A. Broad cast
B. Muddy brown cast
C. RBC casts
D. WBC casts
E. Fatty casts
82. A 56-year-old male with a long history of diabetes mellitus complains of nocturnal urinary frequency, occasional dribbling and difficulty completing his stream. His past medical history is significant for a myocardial infarction two years ago and moderately decreased visual acuity. On physical examination, his blood pressure is 160/100 mmHg and his heart rate is 70/min. There is a carotid bruit auscultated on the left side as well as trace ankle edema. Post-void bladder catheterization yields 60 ml of urine. Dipstick urinalysis reveals 2+ protein and 3-4 WBC/hpf. The patient's serum creatinine level is 2.4 mg/dl. Which of the following is the most likely cause of his renal dysfunction?
A. Ascending infection
B. Obstructive uropathy
C. Microangiopathy
D. Renal hypoperfusion
E. Cystic kidney disease
83. A 34-year-old man is being evaluated for possible end-stage renal disease. He has a long history of diabetes, type 1. He previously developed chronic renal insufficiency despite being on enalapril and insulin. His renal function is getting worse day by day. A nephrologist is currently managing his renal condition. Which of the following long-term treatments would give the best survival rate for this patient?
A. Hemodialysis
B. Peritoneal dialysis
C. Renal transplantation from a cadaver
D. Renal transplantation from a living related donor
E. Renal transplantation from a living unrelated donor
84. A 17-year-old African American man comes to the physician after an episode of gross hematuria that resolved spontaneously. He has no other complaints. His past medical history is insignificant. He takes no medications. He smokes occasionally. He does not use drugs or alcohol. His temperature is 36.7C (98F), blood pressure is 120/70 mm Hg, pulse is 70/min, and respirations are 14/min. Physical examination shows no abnormalities. Urinalysis shows many unchanged red blood cells/HPF, but is otherwise normal. Laboratory studies show a creatinine level of 0.9 mg/dl. Which of the following is the most likely diagnosis?
A. Acute glomerulonephritis
B. Acute interstitial nephritis
C. Sickle cell trait
D. Coagulopathy
E. Acute cystitis
85. A 34-year-old woman comes to the physician's office because of occasional headaches and palpitations. She has no other medical problems. She takes no medications. She smokes one and a half packs of cigarettes daily. Her blood pressure is 170/100 mm Hg in both arms, and heart rate is 80/min. Physical examination shows bilateral flank masses. Laboratory studies show: Serum sodium 140 mEq/L Serum potassium 4.4 mEq/L BUN 26 mg/dL Serum creatinine 1.3 mg/dL Urinalysis shows 10-12 red blood cells/hpf, but otherwise shows no abnormalities. The most likely complication that can occur in this patient is which of the following?
A. Liver necrosis
B. Intracranial aneurysms
C. Restrictive cardiomyopathy
D. Pancreatic cancer
E. Aortic dissection
86. A 30-year-old woman comes to the physician due to several weeks history of generalized edema, fatigue, and decreased appetite. She has no other medical problems. She takes no medications. She does not use tobacco, alcohol, or drugs. Her temperature is 36.7C (98F), blood pressure is 110/70 mm Hg, pulse is 80/min, and respirations are 18/min. Physical examination shows generalized edema. Laboratory studies show a low serum albumin level. HBsAg is positive, and liver function tests are abnormal. Urinalysis shows +4 proteinuria and microhematuria. Which of the following is the most likely diagnosis?
A. Membranoproliferative glomerulonephritis
B. Minimal change disease
C. Focal segmental glomerulosclerosis
D. Diffuse proliferative glomerulonephritis
E. Membranous glomerulonephritis
87. A 62-year-old man presents to the emergency department with severe back pain that began suddenly after he attempted to lift a heavy box. He says the pain radiates down his right thigh and leg and that coughing and moving make the pain “unbearable” The patient also complains of an inability to urinate since the pain started. On physical examination, he has no focal lower extremity weakness or numbness, and pinprick testing in the perianal area elicits a quick spasm of the anal sphincter. Rectal exam reveals an enlarged, smooth, nontender prostate. Which of the following best explains this patient's urinary retention?
A. Severe pain
B. Nerve root injury
C. Detrusor instability
D. Hypertonic bladder
E. Urethral injury
88. A 46-year-old man comes to the physician because of a 2-day history of fever and chills. His fever was gradual in onset. He also complains of perineal and back pain, which is worse towards the sacral area. He has repeated urges to urinate, along with pain on micturition. Rectal examination shows a boggy, exquisitely tender prostate. Laboratory studies show: Hb 13 gldl Hct 40% WBC 12,000/cmm Platelets 329,000/cmm Dipstick urinalysis: Esterase +++ PH 5.0 Nitrite +++ WBC 50+ Protein + Blood ++ Which of the following is the most appropriate next step in management?
A. Send culture of post-prostatic massage sample
B. Send culture of mid-stream urine sample
C. Administer alpha blocking agents
D. Start empirical treatment on an outpatient basis
E. Urethral catheterization
89. A 25-year-old woman presents with nausea and vomiting of 2 days duration. She is not on any medications and was previously well until now. Her physical examination is normal except for a postural drop in her blood pressure from 110/80 mm Hg supine to 90/80 mm Hg standing. Her serum electrolytes are sodium 130 mEq/L, potassium 3 mEq/L, chloride 90 mEq/L, bicarbonate 30 mEq/L, urea 50 mg/dL, and creatinine 0.8 mg/dL. Which of the following electrolytes is most likely to be filtered through the glomerulus but unaffected by tubular secretion?
(A) potassium
(B) sodium
(C) bicarbonate
(D) urea
(E) creatinine
90. A 19-year-old man presents with malaise, nausea, and decreased urine output. He was previously well, and his physical examination is normal except for an elevated jugular venous pressure (JVP) and a pericardial rub. His electrolytes reveal acute renal failure (ARF). Which of the following findings on the urinalysis is most likely in keeping with acute glomerulonephritis (GN)?
(A) proteinuria
(B) white blood cell casts
(C) granular casts
(D) erythrocyte casts
(E) hyaline casts
91. A 50-year-old diabetic woman presents for follow-up of her hypertension. Her blood pressure is 152/96 in the office today and she brings in readings from home that are consistently in the same range over the past month. Her current medications are amlodipine 5 mg daily and hydrochlorothiazide 25 mg daily. The diuretic was added when she developed peripheral edema on the amlodipine; now she has only trace peripheral edema. A spot urine specimen shows 280 μg of albumin per mg creatinine (microalbuminuria is present if this value is between 30 and 300 μg/mg). What would be the best next therapeutic step in this patient?91. A 50-year-old diabetic woman presents for follow-up of her hypertension. Her blood pressure is 152/96 in the office today and she brings in readings from home that are consistently in the same range over the past month. Her current medications are amlodipine 5 mg daily and hydrochlorothiazide 25 mg daily. The diuretic was added when she developed peripheral edema on the amlodipine; now she has only trace peripheral edema. A spot urine specimen shows 280 μg of albumin per mg creatinine (microalbuminuria is present if this value is between 30 and 300 μg/mg). What would be the best next therapeutic step in this patient?
A. Add clonidine.
B. Add a beta-blocker.
C. Increase the thiazide diuretic dose.
D. Add an alpha-blocker.
E. Add angiotensin-converting enzyme inhibitor or angiotensin receptor blocker.
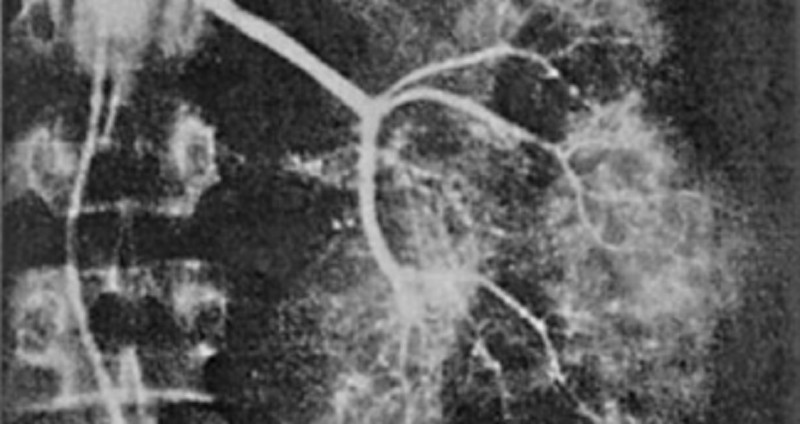
92. A 64-year-old man is admitted for hematuria after slipping on an icy pavement. His physical examination is normal. A selective angiogram of the left kidney is shown in Fig. Which of the following is the most likely diagnosis?
(A) renal cell carcinoma
(B) kidney contusion and laceration
(C) transitional cell carcinoma
(D) renal hamartoma
(E) renal hemangioma
93. A 29-year-old man with HIV, on a highly active antiretroviral therapy (HAART) regimen including the protease inhibitor indinavir, presents with severe edema and a serum creatinine of 2.0 mg/dL. He has had bone pain for 5 years and takes large amounts of acetaminophen with codeine, aspirin, and ibuprofen. He is on prophylactic trimethoprim-sulfamethoxazole. Blood pressure is 170/110; urinalysis shows 4+ protein, 5 to 10 RBC, 0 WBC; 24-hour urine protein is 6.2 g. The serum albumin is 1.9 g/L (normal above 3.7). Which of the following is the most likely cause of his renal disease?
A. Indinavir toxicity
B. Analgesic nephropathy
C. Trimethoprim-sulfamethoxazole–induced interstitial nephritis
D. Focal glomerulosclerosis
E. Renal artery stenosis
94. A 24-year-old woman presents with nausea, vomiting, anorexia, and gross hematuria. She had a sore throat 2 weeks ago that resolved on its own. On examination, her blood pressure is 160/90 mm Hg, pulse 90/min, JVP is 7 cm, heart sounds are normal, there is 1+ pedal edema, and the lungs are clear. She has a renal biopsy. Which of the following electron microscopy findings on the renal biopsy is most likely in keeping with poststreptococcal GN?
(A) diffuse mesangial deposits
(B) no deposits
(C) electron-dense endothelial deposits
(D) closed capillary lumen
(E) subepithelial humps
95. A 74-year-old man is brought to hospital because of urinary retention. He has a Foley catheter inserted to relieve the obstruction, and 1500 cc of urine is emptied from his bladder. Over the next few hours, he has 200cc/h of urine output. Which of the following urine electrolyte values is most likely in keeping with his diagnosis?
(A) high sodium
(B) low potassium
(C) high specific gravity
(D) low pH
(E) osmolality >500 mOsm/kg
96. A 64-year-old woman develops severe diarrhea 2 weeks after finishing antibiotics for pneumonia. She has also noticed decreased urine output despite drinking lots of fluids. On examination, she has a postural drop in her blood pressure, the JVP is low, and the abdomen is soft but diffusely tender. Despite giving 4 L of normal saline, her urine output remains low. The urinalysis is positive for heme-granular casts and the urine sodium is 42mEq/L. Which of the following medications should be held during the recovery phase of this woman’s ARF?
(A) acetaminophen
(B) digoxin
(C) lorazepam
(D) enalapril
(E) simvastatin
97. A 64-year-old man presents with weight gain, shortness of breath, easy bruising, and leg swelling. On examination, his blood pressure is 140/80 mm Hg, pulse 100/min, JVP 4 cm, heart sounds normal, and lungs are clear. There is a 3+ pedal and some periorbital edema. Investigations include a normal chest x-ray (CXR), electrocardiogram (ECG) with low voltages, anemia, high urea and creatinine, and 4 g/day of protein in the urine. A renal biopsy, which shows nodular deposits that have an apple-green birefringence under polarized light when stained with Congo red. Which of the following is the most likely diagnosis?
(A) amyloidosis
(B) multiple myeloma
(C) diabetic nephropathy
(D) minimal change disease
(E) immunoglobulin A (IgA) nephropathy
98. A 67-year-old man with a history of gout presents with intense pain in his right great toe. He has a complex past medical history, including hypertension, coronary artery disease, congestive heart failure, myelodysplasia, and chronic kidney disease with a baseline creatinine of 3.2 mg/dL and a uric acid level of 10 mg/dL. His medications include aspirin, simvastatin, clopidogrel, furosemide, amlodipine, and metoprolol. What is the best therapy in this situation?
A. Colchicine 1.2 mg po initially, followed by 0.6 mg 1 hour later
B. Allopurinol 100 mg po daily and titrate to uric acid less than 6 mg/dL
C. Prednisone 40 mg po daily@
D. Naproxen 750 mg po once followed by 250 mg po tid
E. Probenecid 250 mg po bid
99. A 60-year-old diabetic woman develops angina and will need a coronary angiogram for evaluation of coronary artery disease. She has a creatinine of 2.2. Which of the following is the most effective in reducing the risk of contrast induced nephropathy?
A. Administer mannitol immediately after the contrast is given.
B. Perform prophylactic hemodialysis after the procedure.
C. Give IV hydration with normal saline or sodium bicarbonate prior to and following the procedure.
D. Indomethacin 25 mg the morning of the procedure.
E. Dopamine infusion before and after the procedure.
100. A 47-year-old HIV-positive man is brought to the emergency room because of weakness. The patient has HIV nephropathy and adrenal insufficiency. He takes trimethoprim-sulfamethoxazole for PCP prophylaxis and is on triple-agent antiretroviral treatment. He was recently started on spironolactone for ascites due to alcoholic liver disease. Physical examination reveals normal vital signs, but his muscles are diffusely weak. Frequent extrasystoles are noted. He has mild ascites and 1+ peripheral edema. Laboratory studies show a serum creatinine of 2.5 with a potassium value of 7.3 mEq/L. An EKG shows peaking of the T waves and QRS duration of 0.14. What is the most important immediate treatment?
A. Sodium polystyrene sulfonate (Kayexalate)
B. Acute hemodialysis
D. IV calcium gluconate
E. IV furosemide 80 mg stat
C. IV normal saline
101. An 85-year-old man who resides in a nursing home presents with a 3-day history of lower abdominal pain and increasing fatigue and lethargy. He is afebrile, his BP is 160/92, and RR 16. His lungs are clear and his heart examination normal. There is diffuse abdominal tenderness on palpation and a large area of fullness and dullness to percussion starting just below the umbilicus and extending to the suprapubic area. His serum sodium is 130 mEq/L, potassium 4.9 mEq/L, BUN 75 mg/dL, and creatinine is 3.5 mg/dL. His baseline BUN and creatinine were 25 and 1.3 respectively as recently as 1 month ago. A Foley catheter is placed and 1200 cc of urine is obtained. What will be the likely clinical course for this patient with regard to his renal function?
A. His creatinine will continue to rise slowly for 2 to 3 more days.
B. His creatinine will return to 1.3 over the next week.
C. He will require dialysis within 24 hours.
D. He will produce minimal urinary output for at least 3 days.
E. His renal function is unlikely to show any improvement in the future and 3.5 will be his new baseline.
102. A 74-year-old man presents with fatigue, shortness of breath on exertion, and back and rib pain, which is made worse with movement. Investigations reveal he is anemic, calcium, urea, and creatinine are elevated. X-rays reveal multiple lytic lesions in the long bones and ribs, and protein electrophoresis is positive for an immunoglobulin G (IgG) paraprotein. Which of the following is the most likely mechanism for the renal injury?
(A) plasma cell infiltrate
(C) glomerular injury
(B) tubular damage by light chains
(D) vascular injury by light chains
(E) uric acid crystals
103. 25-year-old man is referred to you because of hematuria. He noticed brief reddening of the urine with a recent respiratory infection. The gross hematuria resolved, but his physician found microscopic hematuria on two subsequent first-voided morning urine specimens. The patient is otherwise healthy; he does not smoke. His blood pressure is 114/72 and the physical examination is normal. The urinalysis shows 2+ protein and 10 to 15 RBC/hpf, with some dysmorphic erythrocytes. No WBC or casts are seen. What is the most likely cause of his hematuria?
A. Kidney stone
B. Renal cell carcinoma
C. Acute poststreptococcal glomerulonephritis
D. Chronic prostatitis
E. IgA nephropathy (Berger disease)
104. A 17-year-old man is brought to the emergency room with confusion and incoordination. He is uncooperative and refuses to provide further history. Physical examination reveals an RR of 30; the vital signs are otherwise normal as is the general physical examination. Laboratory values are as follows: Na: 135 mEq/L K: 2.7 mEq/L HCO3: 15 mEq/L Cl: 110 mEq/L Arterial blood gases: PO2 92, PCO2 30, pH 7.28 Urine: pH 7.5, glucose—negative Ca: 9.7 mg/dL PO4: 4.0 mg/dL Which of the following is the most likely cause of the acid base disorder?
A. GI loss owing to diarrhea
B. Proximal renal tubular acidosis
C. Disorder of the renin-angiotensin system
D. Distal renal tubular acidosis
E. Respiratory acidosis
105. A 56-year-old man presents with hypertension and peripheral edema. He is otherwise healthy and takes no medications. Family history reveals that his father and a brother have kidney disease. His father was on hemo-dialysis before his death at age 68 of a stroke. Physical examination reveals BP 174/96 and AV nicking on funduscopic examination. He has a soft S4 gallop. Bilateral flank masses measuring 16 cm in length are palpable. Urinalysis shows 15 to 20 RBC/hpf and trace protein but is otherwise normal; his serum creatinine is 2.4 mg/dL. Which is the most likely long-term complication of his condition?
A. End-stage renal disease requiring dialysis or transplantation
B. Malignancy
C. Ruptured cerebral aneurysm
D. Biliary obstruction owing to cystic disease of the pancreas
E. Dementia
106. A 64-year-old man presents with symptoms of malaise, shortness of breath, edema, and no urine output for 24 hours. His past medical history is not significant, and his only medication is daily aspirin. On examination his JVP is 4 cm, heart sounds are normal, lungs are clear, and the abdomen is soft. A Foley catheter is inserted into his bladder for 200 cc of urine, which is sent for urinalysis. His urine output still remains low. Which of the following is the most appropriate initial diagnostic test?
(A) renal ultrasound
(B) blood cultures
(C) urine cultures
(D) inferior vena cavagram with selective renal venogram
(E) blood urea nitrogen (BUN)/creatinine ratio
107. 28-year-old woman presents with a recent episode of coughing up some blood, frequent nosebleeds, and now decreased urine output. A nasal mucosa ulcer was seen on inspection. Her urinalysis is positive for protein and red cells consistent with a GN. The CXR shows two cavitary lesions and her serology is positive for antineutrophil cytoplasmic antibodies (ANCA). Which of the following is the most likely diagnosis?
(A) Wegener’s granulomatosis
(B) bacterial endocarditis
(C) Goodpasture’s syndrome
(D) lupus erythematosus
(E) poststreptococcal disease
108. 74-year-old woman develops acute sepsis from pneumonia and is admitted to the intensive care unit because of hypotension. She is started on antibiotics, and her blood pressure is supported with intravenous normal saline. Despite this she remains oliguric and develops ARF. Her urinalysis has heme-granular casts and the urine sodium is 56 mEq/L. Which of the following is the most likely cause of her ARF?
(A) nephrotoxic antibiotics
(B) acute infectious GN
(C) acute tubular necrosis (ATN)
(D) contrast nephropathy
(E) cholesterol emboli
109. A 46-year-old woman with nausea and vomiting presents to hospital because of light- headedness when standing and decreased urine output. She looks unwell; the blood pressure supine is 90/60 mm Hg and 80/60 mm Hg when standing. Her abdominal, heart, and lung examinations are normal. Which of the following laboratory values suggests prerenal azotemia in this patient?
(A) markedly elevated urea, unchanged creatinine
(B) unchanged urea, elevated creatinine
(C) little change in either creatinine or urea for several days after oliguria develops
(D) urea/creatinine ratio of 10
(E) urea/creatinine ratio of 25
110. A 76-year-old man presents to the emergency room. He had influenza and now presents with diffuse muscle pain and weakness. His past medical history is remarkable for osteoarthritis for which he takes ibuprofen, and hypercholesterolemia for which he takes lovastatin. Physical examination reveals blood pressure of 130/90 with no orthostatic change. The only other finding is diffuse muscle tenderness. Laboratory data include BUN: 30 mg/dL Creatinine: 6 mg/dL K: 6.0 mEq/L Uric acid: 18 mg/dL Ca: 6.5 mg/dL PO4: 7.5 mg/dL UA: large blood, 2+ protein. Microscopic study shows muddy brown casts and 0 to 2 rbc/hpf (red blood cells/high power field). Which of the following is the most likely diagnosis?
A. Nonsteroidal anti-inflammatory drug-induced acute kidney injury (AKI)
B. Volume depletion
C. Rhabdomyolysis-induced acute kidney injury
D. Urinary tract obstruction
E. Hypertensive nephrosclerosis
111. A 20-year-old man presents with obtundation. Past medical history is unobtainable. Blood pressure is 120/70 without orthostatic change, and he is well perfused peripherally. The neurological examination is nonfocal. His laboratory values are as follows: Na: 138 mEq/L K: 4.2 mEq/L HCO3: 5 mEq/L Cl: 104 mEq/L Creatinine: 1.0 mg/dL BUN: 14 mg/dL Ca: 10 mg/dL Arterial blood gas on room air: PO2 96, PCO2 15, pH 7.02 Blood glucose: 90 mg/dL Urinalysis: normal, without blood, protein, or crystals. Which of the following is the most likely acid-base disorder?
A. Pure normal anion-gap metabolic acidosis
B. Respiratory acidosis
C. Pure high anion-gap metabolic acidosis
D. Combined high anion-gap metabolic acidosis and respiratory alkalosis
E. Combined high anion-gap metabolic acidosis and respiratory acidosis
112. A 23-year-old woman with no other past medical history was diagnosed with hypertension 6 months ago. She was initially treated with hydrochlorothiazide, followed by the addition of lisinopril, followed by high doses of a beta-blocker, but her blood pressure has not been well controlled. She assures the provider that she is taking all of her medicines. On examination her blood pressure is 165/105 in each arm, and 168/105 when checked by large cuff in the lower extremities. Her pulse is 60. Cardiac examination reveals an S4 gallop but no murmurs. She has a soft mid-abdominal bruit. Distal pulses are intact and equal. She does not have hyperpigmentation, hirsutism, genital abnormalities, or unusual distribution of fat. Her sodium is 140, potassium 4.0, HCO3 22, BUN 15, and creatinine 1.5. Which of the following is the most likely cause of her difficult-to-control hypertension?
A. Primary hyperaldosteronism (Conn syndrome)
B. Cushing syndrome
C. Congenital adrenal hyperplasia
D. Fibromuscular dysplasia
E. Coarctation of the aorta
113. A 73-year-old man undergoes abdominal aortic aneurysm repair. The patient develops hypotension to 80/50 for approximately 20 minutes during the procedure according to the anesthesia record. He received 4 units of packed red blood cells. Postoperatively, his blood pressure is 110/70, heart rate is 110, surgical wound is clean, and a Foley catheter is in place. Over the next 2 days his urine output slowly decreases. His creatinine on post-op day 3 is 3.5 mg/dL (baseline 1.2). His sodium is 140 mEq/L, K 4.6 mEq/L, and BUN 50 mg/dL. Hemoglobin and hematocrit are stable. Urinalysis shows occasional granular casts but otherwise is normal. Urine sodium is 50 mEq/L, urine osmolality is 290 mosmol/L, and urine creatinine is 35 mg/dL. The FeNa (fractional excretion of sodium) based on these data is 3.5. What is the most likely cause of this patient’s acute renal failure?
A. Acute interstitial nephritis
B. Acute glomerulonephritis
C. Acute tubular necrosis
D. Prerenal azotemia
E. Contrast induced nephropathy
114. A 73-year-old woman with arthritis presents with confusion. Neurologic examination is nonfocal, and CT of the head is normal. Laboratory data include Na: 140 mEq/L K: 3.0 mEq/L Cl: 107 mEq/L HCO3: 12 mEq/L Arterial blood gases: PO2 62, PCO2 24, pH 7.40. What is the acid-base disturbance?
A. Respiratory alkalosis with appropriate metabolic compensation
B. High anion-gap metabolic acidosis with appropriate respiratory compensation
C. Combined metabolic acidosis and respiratory alkalosis
D. No acid-base disorder
E. Hyperchloremic (normal anion gap) metabolic acidosis with appropriate respiratory compensation
115. A 17-year-old woman presents with peripheral and periorbital edema. She has previously been healthy and takes no medications. Her blood pressure is 146/92; she is afebrile. The patient has mild basilar dullness on lung examination; her cardiac examination is normal. She has periorbital edema and soft, doughy 3+ edema in her legs. Her serum creatinine is 0.6 mg/dL and her serum albumin is 2.1 g/L. Urinalysis shows 3+ protein, no RBC or WBC, and some oval fat bodies. What is the next best step to take in evaluating this patient?
A. Order serum and urine protein electrophoresis.
B. Request a nuclear medicine renal scan.
C. Measure plasma aldosterone and renin activity.
D. Order a 24-hour urine collection to quantitate the degree of proteinuria.
E. Ask a nephrologist or radiologist to perform a renal biopsy.
116. A 63-year-old man alcoholic with a 50-pack-year history of smoking presents to the emergency room with fatigue and confusion. Physical examination reveals a blood pressure of 110/70 with no orthostatic change. Heart, lung, and abdominal examinations are normal and there is no pedal edema. Laboratory data are as follows: Na: 110 mEq/L K: 3.7 mEq/L Cl: 82 mEq/L HCO3: 20 mEq/L Glucose : 100 mg/dL BUN : 5 mg/dL Creatinine: 0.7 mg/dL Urinalysis: normal Specific gravity: 1.016 Which of the following is the most likely diagnosis?
A. Volume depletion
B. Inappropriate secretion of antidiuretic hormone
C. Psychogenic polydipsia
D. Cirrhosis
E. Congestive heart failure
117. A 63-year-old woman has Type II diabetes mellitus, which is well-controlled. Her physical examination is positive for peripheral neuropathy in the feet and nonproliferative retinopathy. A urinalysis is positive for proteinuria. Which of the following treatments is most likely to attenuate the course of renal disease?
(A) calcium channel blockers
(B) ACE inhibitors
(C) hepatic hydroxymethylglutaryl- coenzyme A (HMG-CoA) inhibitors
(D) dietary carbohydrate restriction
(E) weight reduction
118. A 56-year-old man is involved in a severe motor vehicle accident. He develops ARF after admission to hospital. One of the possibilities for his ARF is posttraumatic renal vein thrombosis. Which of the following findings is most likely to suggest renal vein thrombosis?
(A) white cell casts on urinalysis
(B) heme-granular casts
(C) heavy proteinuria
(D) urine supernatant pink and tests positive for heme
(E) specific gravity >1.020
119. A 69-year-old woman presents with left flank pain and hematuria. Physical examination suggests a left-sided abdominal mass. Computerized tomography (CT) scan of the abdomen reveals a 5-cm mass in the left kidney. Which of the following laboratory abnormalities might also be present? (See Fig.)
(A) polycythemia
(B) thrombocytopenia
(C) hypocalcemia
(D) leukocytosis
(E) high renin hypertension
120. A 60-year-old woman with heart failure and normal renal function is started on furosemide (Lasix) 80 mg/day. She notices a good diuretic response every time she takes the medication. A few weeks later, she is feeling unwell because of fatigue and muscle weakness, but her heart failure symptoms are better. Which of the following is the most likely explanation for her muscle weakness?
(A) hyponatremia
(B) hypernatremia
(C) hypokalemia
(D) hyperkalemia
(E) anemia
{"name":"VIII. NEPHROLOGY & ELECTROLYTE", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"61. A healthy 54-year-old man comes to the physician for a routine health maintenance examination. He has no complaints, but he is requesting for a CT scan of the abdomen. His father died at the age of 60 due to the sudden rupture of an undiagnosed abdominal aortic aneurysm. He has a history of hypertension and gouty arthritis. His social history is not significant. His vital signs are stable. Physical examination shows no abnormalities. ACT scan of the abdomen is shown below. Which of the following is the most appropriate next step in management?, 62. A 30-year-old woman comes to the office due to the recent onset of fever, chills, and dysuria. Her temperature is 38.3C (101.0F), blood pressure is 110\/70mm Hg, pulse is 68\/min, and respirations are 15\/min. Examination shows tenderness at the right costovertebral angle. Laboratory studies show WBC count of 16,000\/microl with left shift. Urinalysis shows bacteriuria and pyuria. Her urine and blood is collected for culture and sensitivity. She is prescribed oral ciprofloxacin and sent home. After three days, she returns for a follow-up visit. She is still febrile, and the physical examination is unchanged. The blood cultures have no growth after 72 hours of incubation. Results of the urine culture show: Which of the following is the most appropriate next step in management?, 63. A 62-year-old woman presents to your office complaining of urinary frequency and burning during urination. She denies fever, chills, nausea, back pain or abdominal pain. Her past medical history is significant for a long history of diabetes mellitus and hypertension. She does not use tobacco or consume alcohol. Her blood pressure is 160\/100 mmHg and her heart rate is 70\/min. Her hematocrit is 43% and her WBC count is 8,500\/mm3 Urinalysis reveals the following: Glucose negative Ketones negative Nitrates positive Protein 2+ WBC 20-25\/hpf RBC 3-5\/hpf She is given a three-day course of levofloxacin. Urinalysis two weeks later reveals 2+ protein but no nitrates, WBCs, or RBCs. Which of the following is most likely responsible for her persistent urinalysis abnormality?","img":"https://cdn.poll-maker.com/10-468769/8-nephrology-electrolyte-pdf---adobe-reader.bmp?sz=1200-000013100053"}
More Quizzes
Choose the correct future form of the verb.
11614
L to J 6th Grade
10529
Lash Technician Training Insights Quiz
1160
Fox Quiz
1050
Milady Chapter 16 Haircutting - Free Practice
201018124
Warm or Cold Personality Test - Find Out Your Type
201018735
What Country Should I Visit - Free Destination Match
201018735
Culinary Skills Test - Check Your Cooking Knowledge
201018347
NASCAR Trivia - Free Racing Knowledge Test
201016578
West Side Story Trivia - Wise Trivia
201021186
About Me: Discover Your Personality Type - Free
201017838
General Safety - OHS Questions and Answers (Free)
201020649