
DES 2016. Final (Paer 33)
124) A 70-year-old man presents with a complaint of fatigue. There is no history of alcohol abuse or liver disease; the patient is taking no medications. Scleral icterus is noted on physical examination; the liver and spleen are nonpalpable. The patient has a normocytic, normochromic anemia. Urinalysis shows bilirubinuria with absent urine urobilinogen. Serum bilirubin is 12 mg/dL, AST and ALT are normal, and alkaline phosphatase is 300 U/L (three times normal). Which of the following is the best next step in evaluation?
. Ultrasound or CT scan of the abdomen
. Viral hepatitis profile
. Reticulocyte count
. Serum ferritin
. Antimitochondrial antibodies
125) A 45-year-old woman presents with a 1-week history of jaundice, anorexia, and right upper quadrant discomfort. On examination she is icteric, with a tender right upper quadrant and liver span of 14 cm. There is no shifting dullness or pedal edema and the heart and lungs are normal. On further inquiry, she reports consuming one bottle of wine a day for the past 6 months. Which of the following laboratory tests are most likely to be characteristic of a patient with jaundice secondary to alcoholic hepatitis?
. Ratio of AST: ALT is 3:1 and the AST is 500 U/L
. Ratio of AST: ALT is 2:1 and the AST is 250 U/L
. Ratio of AST: ALT is 1:1 and the AST is 500 U/L
. Ratio of AST: ALT is 1:1 and the AST is 250 U/L
. Ratio of AST: ALT is 1:3 and the AST is 750
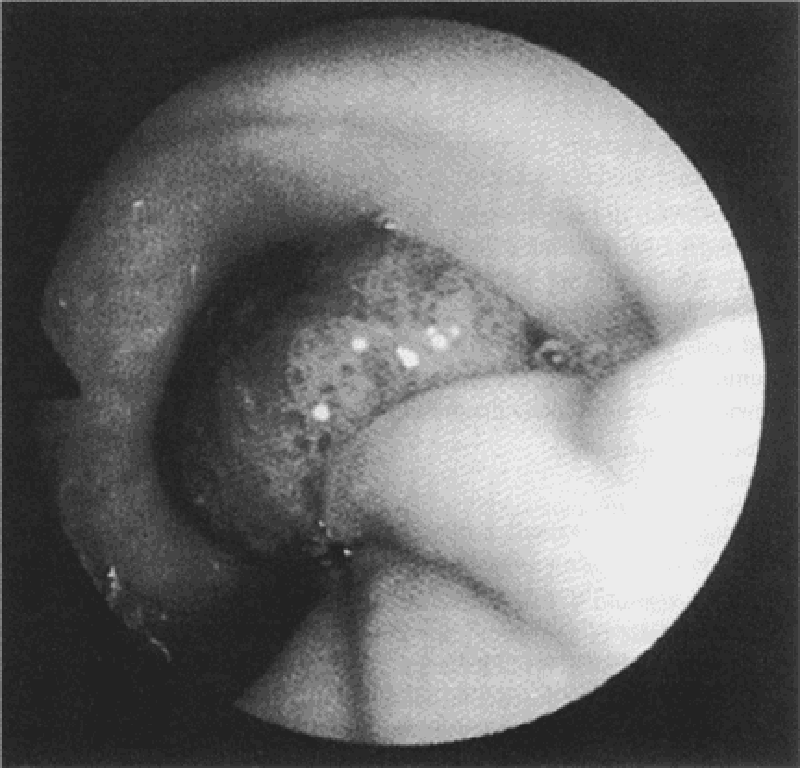
126) A 60-year-old man with a history of alcohol abuse presents to the ED with hematemesis for 1 day. He denies abdominal or chest pain. On physical examination, his eyes appear reddened which he attributes to having drunken heavily the night before (he also reveals vomiting several times after this recent binge). Vital signs are HR 115 beats per minute, BP 130/85 mm Hg, RR 18 breaths per minute, and temperature 99.5°F. Chest radiograph is unremarkable. Laboratory results reveal a WBC 10,000/μL, haemoglobin 14 mg/dL, hematocrit 40%, and platelets 210/μL. Which diagnosis is endoscopic evaluation most likely to confirm?
. Esophageal varices
. Boerhaave syndrome
. Curling ulcer
. Perforated gastric ulcer
. Mallory-Weiss tear
127) A 73-year-old man comes to his primary care physician for his yearly check-up. His medical history is significant for obesity, new onset diabetes mellitus, and a remote history of tobacco use. The patient has noticed that his stool has been darker for the past 3 months, although he has only seen gross blood in his stool once, a week ago. He also complains of recent fatigue and occasional light-headedness when standing up from sitting. On examination the patient has fecal occult blood and a hematocrit of 32%. Colonoscopy and upper gastrointestinal endoscopy reveal no obvious pathology. Which of the following is the best diagnostic test to locate this patient’s hemorrhage?
Angiography
Barium enema
Colonoscopy
CT scan with contrast
Tagged RBC scan
128) A 70-year-old woman with a history of hypertension, congestive heart failure, and atrial fibrillation presents to the ED with several hours of acute onset diffuse abdominal pain. She denies any nausea or vomiting. The pain is constant, but she is unable to localize it. She was diagnosed with a renal artery thrombosis several years ago. Vital signs include HR of 95 beats per minute, BP of 110/70 mm Hg, and temperature of 98°F. Her abdomen is soft and mildly tender, despite her reported severe abdominal pain. Her WBC count is 12,000/μL, hematocrit 38%, platelets 250/μL, and lactate 8 mg/dL. The stool is traced heme-positive. You are concerned for acute mesenteric ischemia. What is the best way to diagnose this condition?
. Serum lactate levels
. Abdominal radiograph (supine and upright)
. CT scan
. Angiography
. Barium contrast study
129) As you palpate the right upper quadrant (RUQ) of a 38-year-old woman’s abdomen, you notice that she stops her inspiration for a brief moment. During the history, the patient states that over the last 2 days she gets pain in her RUQ that radiates to her back shortly after eating. Her vitals include a temperature of 100.4°F, HR of 95 beats per minute, BP of 130/75 mm Hg, and RR of 16 breaths per minute. What is the initial diagnostic modality of choice for this disorder?
. Plain film radiograph
. Computed tomography (CT) scan
. Magnetic resonance imaging (MRI)
. Radioisotope cholescintigraphy (HIDA scan)
. Ultrasonography
130) A 23-year-old woman presents to the ED complaining of lower abdominal pain and vaginal spotting for 2 days. Her menstrual cycle is irregular. She has a history of ovarian cysts and is sexually active but always uses condoms. Her BP is 115/75 mm Hg, HR is 75 beats per minute, temperature is 98.9°F, and RR is 16 breaths per minute. Which of the following tests should be obtained next?
. Chlamydia antigen test
. β-Human chorionic gonadotropin (β-hCG)
. Transvaginal ultrasound
. Abdominal radiograph
. Observe her abdominal pain, if it resolves discharge her with a diagnosis of menstruation
131) For which of the following patients is an abdominal CT scan contraindicated?
. A 52-year-old man with abdominal pain after blunt trauma, negative focused assessment with sonography for trauma (FAST) examination, BP 125/78 mm Hg, and HR 109 beats per minute
. A 22-year-old woman with RLQ pain, negative β-hCG, temperature 100.6 F
. A 45-year-old man with abdominal pain, temperature 100.5 F, WBC 11,200/μL, BP 110/70 mm Hg, HR 110 beats per minute, and lipase 250 IU
. A 70-year-old man with abdominal pain, an 11-cm pulsatile mass in the epigastrium, BP of 70/50 mm Hg, and HR of 110 beats per minute
. A 65-year-old woman with right flank pain that radiates to her groin, microhematuria, BP 165/85 mm Hg, and HR 105 beats per minute
132) A 59-year-old man presents for his routine colonoscopy and during his visit he has numerous large adenomas removed from his colon. Which of the following is the most effective strategy for follow-up of this patient?
Elective colectomy
Repeat colonoscopy in 10 years
Repeat colonoscopy in 3 years
Sigmoidoscopy in 10 years
Urgent colectomy
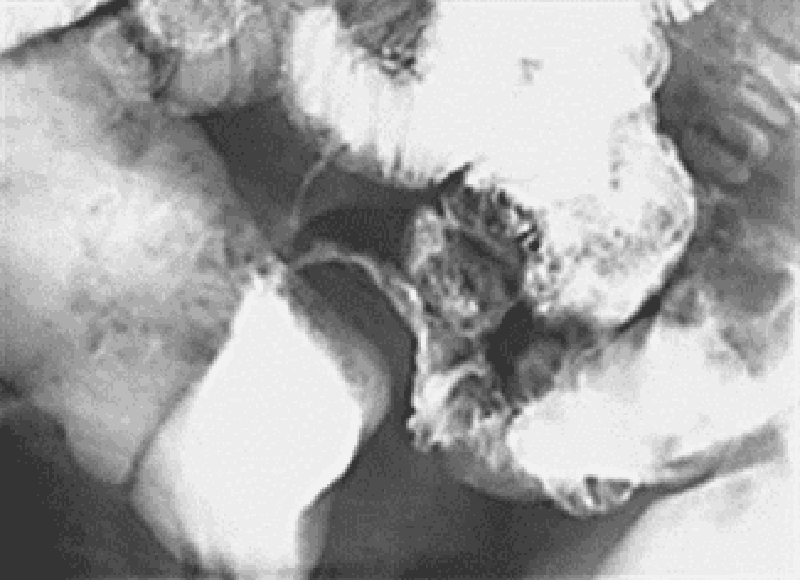
133) A 58-year-old white man complains of intermittent rectal bleeding and, at the time of colonoscopy, is found to have internal hemorrhoids and the lesion shown at the splenic flexure. Pathology shows tubulovillous changes. Repeat colonoscopy should be recommended at what interval?
. In 1 to 2 months
. In 1 year
. In 3 years
. In 10 years
. Repeat colonoscopy is not necessary
134) A 68-year-old man presents to the ED 4 hours after an upper endoscopy was performed for 5 months of progressive dysphagia. During the procedure, a 1-cm ulcerated lesion was found and biopsied. Now, the patient complains of severe neck and chest pain. His vitals are as follows: BP 135/80 mm Hg, HR 123 beats per minute, RR 26 breaths per minute, and temperature 101°F. On physical examination, he appears diaphoretic and in moderate distress with crepitus in the neck and a crunching sound over the heart. You obtain an electrocardiogram (ECG), which is notable for sinus tachycardia. After obtaining a surgical consult, which of the following is the next best step in management?
. Perform an immediate bronchoscopy
. Give aspirin 325 mg and obtain a cardiology consult for possible cardiac catheterization
. Repeat the endoscopy to evaluate the biopsy site
. Perform an immediate thoracotomy
. Order an immediate esophagram with water-soluble agent
135) A 24-year-old man woke up from sleep 1 hour ago with severe pain in his right testicle. He states that he is sexually active with multiple partners. On examination, the right scrotum is swollen, tender, and firm. You cannot elicit a cremasteric reflex. His BP is 145/75 mm Hg, HR is 103 beats per minute, RR is 14 breaths per minute, temperature is 98.9°F, and oxygen saturation is 99% on room air. Which of the following is the most appropriate next step in management?
. Administer one dose of ceftriaxone and doxycycline for 10 days and have him follow-up with a urologist
. Swab his urethra, send a culture for gonorrhea and Chlamydia, and treat if positive
. Send a urinalysis and treat for a urinary tract infection (UTI) if positive
. Treat the patient for epididymitis and have him return if symptoms persist
. Order a statim (STAT) color Doppler ultrasound and urologic consultation
136) A 59-year-old man presents to the ED complaining of vomiting and sharp abdominal pain in the epigastric area that began abruptly this afternoon. He describes feeling nauseated and has no appetite. Laboratory results reveal WBC 18,000/μL, hematocrit 48%, platelets 110/μL, AST 275 U/L, ALT 125 U/L, alkaline phosphatase 75 U/L, amylase 1150 U/L, lipase 1450 IU, LDH 400 U/L, sodium 135 mEq/L, potassium 3.5 mEq/L, chloride 110 mEq/L, bicarbonate 20 mEq/L, BUN 20 mg/dL, creatinine 1.5 mg/dL, and glucose 250 mg/dL. Which of the following laboratory results correlate with the poorest prognosis?
. Amylase 950, lipase 1250, LDH 400
. Lipase 1250, LDH 400, bicarbonate 20
. Lipase 1250, creatinine 1.5, potassium 3.5
. WBC 18,000, LDH 400, glucose 250
. WBC 18,000, amylase 950, lipase 1250
137) A 27-year-old man is seen in the ED for a leak around a surgical G-tube that was placed 2 weeks ago and has been used for enteral feeding for 1 week. Inspection reveals the tube is pulled out from the stoma, but is still in the cutaneous tissue. The abdomen is soft and nondistended and there are no signs of skin infection. Which of the following is the most appropriate next step in management?
. Insert a Foley catheter into the tract and aspirate. If gastric contents are aspirated the tube can be used for feeding
. Insert a Foley catheter into the tract, instill water-soluble contrast, and obtain an abdominal radiograph prior to using for feeding
. Remove the tube and admit the patient for observation
. Remove the tube and immediately obtain a CT scan of the abdomen
. Return to the OR for closure of gastrotomy and placement of a new tube
138) A 23-year-old woman presents with weight loss and chronic diarrhea. She appears unwell and cachectic. Routine laboratory tests reveal a low hemoglobin level and an increased international normalized ratio (INR) even though she is not taking any anticoagulants. The liver enzymes are normal, but the albumin and calcium levels are low, suggesting generalized malnutrition. Which of the following is the most appropriate initial diagnostic test for malabsorption?
. Xylose absorption
. Schilling test
. x-ray studies
. Stool fat quantitation
. Small intestinal biopsy
139) A 50-year-old man with a history of alcohol and tobacco abuse has complained of difficulty swallowing solid food for the past 2 months. More recently, swallowing fluids has also become a problem. He has noted black, tarry stools on occasion. The patient has lost 10 lb. Which of the following statements is correct?
. A CT scan of the abdomen and pelvis is the best next test
. Barium contrast esophagram will likely establish a diagnosis
. The most likely diagnosis is peptic ulcer disease
. The patient has achalasia
. Herpes simplex virus infection of the esophagus is likely
140) A 48-year-old woman presents with a change in bowel habit and 10-lb weight loss over the past 2 months despite preservation of appetite. She notices increased abdominal gas, particularly after fatty meals. The stools are malodorous and occur 2 to 3 times per day; no rectal bleeding is noticed. The symptoms are less prominent when she follows a clear liquid diet. Which of the following is the most likely histological abnormality associated with this patient’s symptoms?
. Signet ring cells on gastric biopsy
. Mucosal inflammation and crypt abscesses on sigmoidoscopy
. Villous atrophy and increased lymphocytes in the lamina propria on small bowel biopsy
. Small, curved gram-negative bacteria in areas of intestinal metaplasia on gastric biopsy
. Periportal inflammation on liver biopsy
141) A 62-year-old woman is transferred to the medical service with an appendiceal mass serendipitously picked up at the edge of an x-ray taken of a broken femur in the emergency department. Otherwise, the patient has no significant past medical history and no current symptoms. Which of the following studies is most likely to be useful?
Arterial blood gas
CT of the chest and abdomen
Immediate ECG
MRI of the chest and abdomen
Room air oxygen saturation
142) A 60-year-old woman complains of fever and constant left lower quadrant pain of 2 days duration. She has not had vomiting or rectal bleeding. She has a history of hypertension but is otherwise healthy. She has never had similar abdominal pain, and has had no previous surgeries. Her only regular medication is lisinopril. On examination blood pressure is 150/80, pulse 110, and temperature 38.9°C (102°F). She has normal bowel sounds and left lower quadrant abdominal tenderness with rebound. A complete blood count reveals WBC = 28,000. Serum electrolytes, BUN, creatinine and liver function tests are normal. What is the next best step in evaluating this patient’s problem?
. Colonoscopy
. Barium enema
. Exploratory laparotomy
. Ultrasound of the abdomen
. CT scan of the abdomen and pelvis
143) A 37-year-old woman presents for evaluation of abnormal liver chemistries. She has long-standing obesity (current BMI 38) and has previously taken anorectic medications but not for the past several years. She takes no other medications and has not used parenteral drugs or had high risk sexual exposure. On examination, her liver span is 13 cm; she has no spider angiomas or splenomegaly. Several sets of liver enzymes have shown transaminases two to three times normal. Bilirubin and alkaline phosphatase are normal. Hepatitis B surface antigen and hepatitis C antibody are normal, as are serum iron and total iron-binding capacity. Which of the following is the likely pathology on liver biopsy?
. Macrovesicular fatty liver
. Microvesicular fatty liver
. Portal triaditis with piecemeal necrosis
. Cirrhosis
. Copper deposition
144) A 55-year-old man from China is known to have chronic liver disease, secondary to hepatitis B infection. He has recently felt unwell, and his hemoglobin level has increased from 130 g/L, 1 year ago, to 195 g/L. Which of the following is the most appropriate initial diagnostic test?
. Alkaline phosphatase
. alpha-fetoprotein (AFP)
. Aspartate transaminase (AST)
. Alanine transaminase (ALT)
. Unconjugated bilirubin
145) A 42-year-old previously well woman presents with pruritus. She is not taking any medications, and only drinks alcohol on a social basis. Her physical examination is entirely normal with no signs of chronic liver disease or jaundice. Laboratory evaluation reveals an alkaline phosphatase level of three times normal, and an ultrasound of the liver and gallbladder is normal. Which of the following is the most appropriate next step in diagnosis?
. INR or prothrombin time
. Antinuclear antibodies
. Protein immunoelectrophoresis
. Abdominal ultrasound
. Antimitochondrial antibodies
146) A 22-year-old man with inflammatory bowel disease is noted to have a “string sign” in the ileal area on barium enema. In which of the following conditions is this sign most often seen?
. In the stenotic or nonstenotic phase of the disease
. In the stenotic phase only
. As a rigid, nondistensible phenomenon
. With gastric involvement
147) A 55-year-old white man with a 20-year history of gastroesophageal reflux visits the clinic for worsening reflux symptoms over the past 18 months. His last visit was 7 years ago and he claims to be otherwise in good health. He has been compliant with his antireflux medications, including an H2-blocker and a proton pump inhibitor. Which of the following is the best next step in management?
Double the dose of his H2-blocker and schedule him for follow-up in 4 weeks
Double the dose of his proton pumps inhibitor and schedule him for follow-up in 4 weeks
Perform an esophagoscopy
Schedule him for elective esophagectomy
Schedule him for emergent Nissen fundoplication
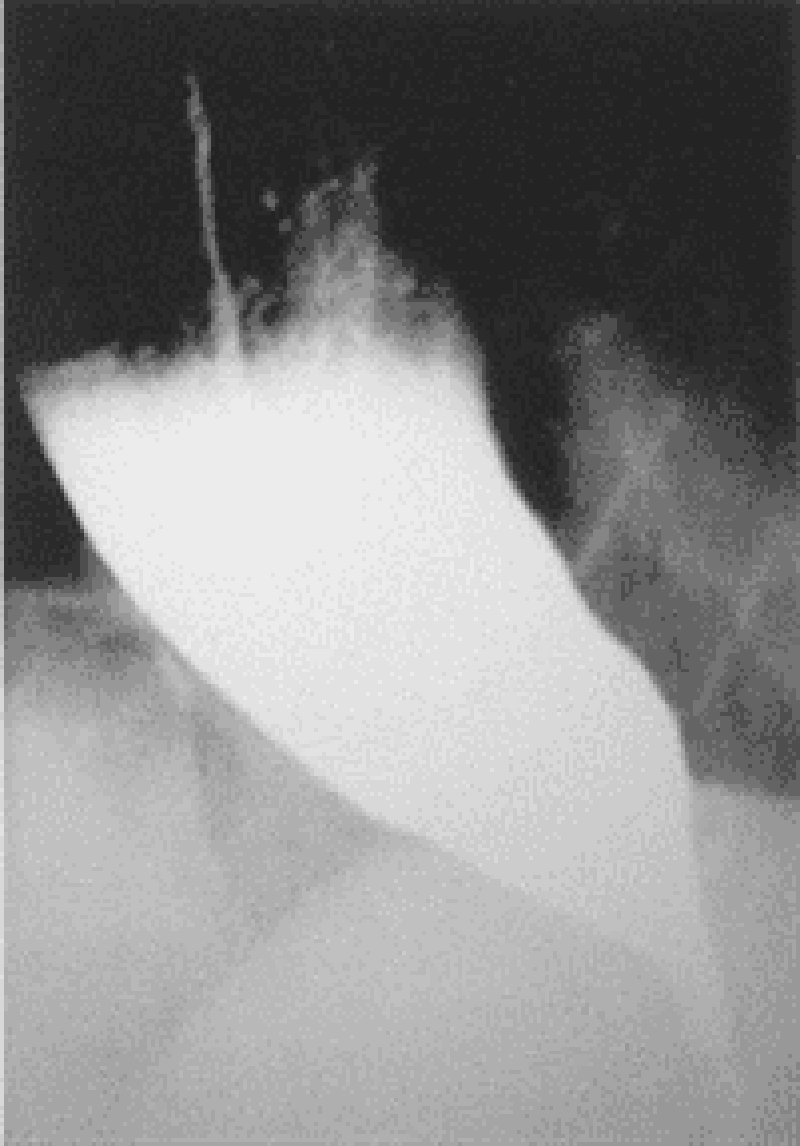
148) A 65-year-old man presents to his physician complaining of difficulty swallowing, occasional chest pain, and regurgitation of food. Over the past 2 months he has lost about 7 kg (15 lb). Results of a barium swallow study are shown in the image. What test should be performed to look for possible causes of his condition?
24-hour pH monitoring
Esophageal manometry
Serum gastrin level measurement
Upper endoscopy
Urease breath test
149) A 63-year-old man with a long history of alcohol abuse presents with ascites. He is experiencing mild abdominal discomfort and nausea. Examination reveals tense ascites and generalized tenderness but no rigidity. A diagnostic paracentesis of the fluid is performed. Which of the following ascitic fluid results is most likely to suggest an uncomplicated ascites due to portal hypertension from cirrhosis?
. hemorrhage
. protein >25 g/L
. Bilirubin level twice that of serum
. Serum to ascites albumin gradient >1.1 g/dL
. More than 1000 white cells/mm3
150) A 21-year-old man presents to the clinic feeling tired and generally unwell. He has fallen several times over the past month and has developed a slight tremor in both hands. Physical examination is significant for scleral icterus, ankle edema, and a distended and tense abdomen. Laboratory studies show: Hemoglobin: 7 g/dL, Reticulocyte count: 7% Total bilirubin: 3.1 mg/dL, Aspartate aminotransferase: 84 U/L Alanine aminotransferase: 92 U/L Ceruloplasmin: 5 mg/dL (normal: 20–45 mg/dL). Results of a Coombs’ test are negative. Which of the following is an appropriate preventive management step after chelation therapy?
Blood protein electrophoresis
Colonoscopy
ECG
Schilling test
Upper endoscopy
151) A 35-year-old alcoholic man is admitted with nausea, vomiting, and abdominal pain that radiates to the back. He has had several previous episodes of pancreatitis presenting with the same symptoms. Which of the following laboratory values suggests a poor prognosis in this patient?
. Elevated serum lipase
. Elevated serum amylase
. Leukocytosis of 20,000/μm
. Diastolic blood pressure greater than 90 mm Hg
. Heart rate of 100 beats/minute
152) A 60-year-old woman with depression and poorly controlled type 2 diabetes mellitus complains of episodic vomiting over the last three months. She has constant nausea and early satiety. She vomits once or twice almost every day. In addition, she reports several months of mild abdominal discomfort that is localized to the upper abdomen and that sometimes awakens her at night. She has lost 5 lb of weight. Her diabetes has been poorly controlled (glycosylated hemoglobin recently was 9.5). Current medications are glyburide, metformin, and amitriptyline. Her physical examination is normal except for mild abdominal distention and evidence of a peripheral sensory neuropathy. Complete blood count, serum electrolytes, BUN, creatinine, and liver function tests are all normal. Gallbladder sonogram is negative for gallstones. Upper GI series and CT scan of the abdomen are normal. What is the best next step in the evaluation of this patient’s symptoms?
. Barium esophagram
. Scintigraphic gastric emptying study
. Colonoscopy
. Liver biopsy
. Small bowel biopsy
153) A 63-year-old man with diabetes is called by his primary care physician because of abnormal liver function test results, as follows: Aspartate aminotransferase: 85 U/L Alanine aminotransferase: 102 U/L Alkaline phosphatases: 180 U/L Total bilirubin: 1.9 mg/dL. On physical examination his liver is enlarged. His skin has a slightly yellow hue, especially on his face. The review of symptoms is significant for some weight loss, weakness, arthritis in his hands, and inability to achieve an erection. What test would generate the most likely diagnosis and should be done first?
Blood smear
CT scan of the abdomen
Endoscopic retrograde cholangiopancreatography
Fasting transferrin saturation levels
Liver biopsy
154) A 28-year-old man presents to the ED complaining of constant vague, diffuse epigastric pain. He describes having a poor appetite and feeling nauseated ever since eating sushi last night. His BP is 125/75 mm Hg, HR is 96 beats per minute, temperature is 100.5°F, and his RR is 16 breaths per minute. On examination, his abdomen is soft and moderately tender in the right lower quadrant (RLQ). Laboratory results reveal a WBC of 12,000/ μL. Urinalysis shows 1+ leukocyte esterase. The patient is convinced that this is food poisoning from the sushi and asks for some antacid. Which of the following is the most appropriate next step in management?
. Order a plain radiograph to look for dilated bowel loops
. Administer 40 cc of Maalox and observe for 1 hour
. Send the patient for an abdominal ultrasound
. Order an abdominal CT scan
. Discharge the patient home with ciprofloxacin
155) A 23-year-old woman presents to the ED in moderate pain in her left lower quadrant (LLQ). She states that the pain began suddenly and is associated with nausea and vomiting. She had a bout of diarrhea yesterday. This is the second time this month that she experienced pain in this location, however, never with this severity. Her BP is 120/75 mm Hg, HR is 101 beats per minute, temperature is 99.5°F, and RR is 18 breaths per minute. She has a tender LLQ on abdominal examination and a tender adnexa on pelvic examination. Which of the following is the most appropriate diagnostic test for the patient?
. CT scan
. MRI
. X-ray
. Doppler ultrasound
. Laparoscopy
156) A 75-year-old woman comes to the emergency department with complaints of nausea and nonbilious, nonbloody vomiting over the past 4 days. The patient reports that both the nausea and vomiting come in “waves”; that is, several hours will pass during which she feels well before the vomiting suddenly recurs. A detailed history reveals that the woman was told several months ago that she “has stones in her gall-bladder,” but she has been too frightened to undergo surgery. She has not had a bowel movement for 7 days. Her temperature is 38.4°C (101.1°F) and the abdomen is distended with high-pitched bowel sounds. Which of the following is the most appropriate initial test for a patient with suspected gallstone ileus?
Abdominal ultrasound
Diagnostic laparoscopy
Endoscopic retrograde cholangiopancreatography
Hepatic iminodiacetic acid scan
Plain X-ray of the abdomen
157) An 82-year-old woman is in the surgical intensive care unit after a carotid endarterectomy. She has been taking clindamycin and ciprofloxacin for the past 13 days. On postoperative day 2 the patient is febrile and tachycardic with a high WBC count and a low RBC count. She is also noted to be dehydrated and hypotensive. On physical examination she is distended and has abdominal tenderness with rebound and guarding. Barium enema reveals colonic dilatation of 8 cm. Stool is sent for Gram stain and analysis for fecal leukocytes, fecal occult blood, and Clostridium difficile toxin. Which of the following is most likely present in the stool sample?
Clostridium difficile toxin
Gram-negative rods
Gram-positive cocci
No fecal occult blood
Spores and hyphae
158) A 51-year-old man presents to the ED complaining of epigastric pain that radiates to his back. He states that he drinks six packs of beer daily. You suspect he has pancreatitis. His BP is 135/75 mm Hg, HR is 90 beats per minute, temperature is 100.1°F, and his RR is 17 breaths per minute. Laboratory results reveal WBC 13,000/μL, hematocrit 48%, platelets 110/μL, amylase 1150 U/L, lipase 1450 IU, lactate dehydrogenase (LDH) 150 U/L, sodium 135 mEq/L, potassium 3.5 mEq/L, chloride 105 mEq/L, bicarbonate 23 mEq/L, BUN 15 mg/dL, creatinine 1.1 mg/dL, and glucose 125 mg/dL. Which of the following laboratory values are most specific for pancreatitis?
. Elevated amylase
. Hyperglycemia
. Elevated lipase
. Elevated LDH
. Leukocytosis
159) A 25-year-old G3P1011 presents to the ED with a 6-hour history of worsening lower abdominal pain, mostly in the RLQ. She also noticed some vaginal spotting this morning. She is nauseated, but did not vomit. Her last menstrual period was 2 months ago, but her cycles are irregular. She is sexually active and has a history of pelvic inflammatory disease. Her BP is 120/75 mm Hg, HR is 95 beats per minute, temperature is 99.2°F, and RR is 16 breaths per minute. Her abdomen is tender in the RLQ. Pelvic examination reveals right adnexal tenderness. Her WBC count is slightly elevated and her β-hCG is positive. After establishing IV access, which of the following is the most appropriate next step in management?
. Call the OR to prepare for laparoscopy
. Order an emergent CT scan of the abdomen
. Perform a transvaginal ultrasound
. Order a urinalysis
. Swab her cervix and treat for gonorrhea and Chlamydia
160) A 40-year-old Asian woman presents to the emergency department complaining of intermittent epigastric pain. The pain is severe, lasts for a few hours, and is sometimes accompanied by nausea and vomiting. Her bowel movements have been normal. Her temperature is 38.3°C (100.9°F), pulse is 100/min, blood pressure is 150/80 mm Hg, and respiratory rate is 22/min. Physical examination reveals moderate obesity and mildly icteric sclerae. Bowel sounds are normal, with an abrupt halt of inspiration upon palpation of the RUQ, and guarding is noted. Laboratory values reveal a WBC count of 13,000/mm³, total bilirubin of 3.3 mg/dL, and normal liver enzymes and alkaline phosphatase levels. Which of the following is the first diagnostic imaging study that should be performed?
CT
Flat and upright plain x-rays of the abdomen
Hepatobiliary iminodiacetic acid scan
MRI
Ultrasound of the RUQ
161) A 45-year-old white man is brought to the emergency department by ambulance. He is waving wildly, trying to hit the “flying bats” that are all around him. He is very agitated and smells strongly of alcohol. The ambulance crew said they found the patient bleeding from the mouth outside a bar. They could not find any laceration on his mouth or lips and believe that the bleeding is internal. The patient screams that he will not stand for this maltreatment any longer and tries to stand up, at which point he begins to vomit. Blood pours out of his mouth, and the patient says, “Here we go again.” The ambulance crew tells the physician that there was also a lot of vomit at the bar where he was found. The physician is able to subdue the patient to obtain his vital signs. His blood pressure is 118/78 mm Hg, pulse is 98/ min, respiratory rate is 22/min, and temperature is 37.2°C (98.9°F). The physician is unable to obtain a history on the patient or con- tact any relatives or friends. No signs of obvious trauma are observed. Which of the following is the best next step in diagnosis?
Barium swallow
Electrocardiogram
Endoscopy
Esophageal manometry
X-ray of the chest
162) A 53-year-old man presents to the emergency department with severe epigastric abdominal pain. His temperature is 37.2°C, blood pressure 110/70 mm Hg, pulse 110/min, and respirations 20/min. Examination of the heart and lungs is normal, and his abdomen is tender in the epigastric region. His white count is 15,000/mL and amylase is 450 U/L (25–125 U/L). Which of the following laboratory abnormalities is also most likely to be present?
. hypoglycemia
. hypercholesterolemia
. hyperglycemia
. hypercalcemia
. hypercarbia
163) A 34-year-old white woman is treated for a UTI with amoxicillin. Initially she improves, but 5 days after beginning treatment, she develops recurrent fever, abdominal bloating, and diarrhea with six to eight loose stools per day. What is the best diagnostic test to confirm your diagnosis?
. Identification of Clostridium difficile toxin in the stool
. Isolation of C difficile in stool culture
. Stool positive for white blood cells (fecal leukocytes)
. Detection of IgG antibodies against C difficile in the serum
. Visualization of clue cells on microscopic examination of stool
164) Her son brings a 50-year-old female to the emergency room because she is confused and sweating a lot. She does not have any medical problems, except hypertension for which she takes hydrochlorothiazide. She is not taking any other medication. He tells you that his mother complained of profound weakness, and inability to stand, because of lightheadedness 3 hours ago. On examination, the patient is drowsy, confused, and appears sick. Her temperature 36.8°C (98.2° F) BP 153/83mm Hg PR 128/min. Her clothes are damp from perspiration. No other abnormalities are noted on physical examination. Initial laboratory studies show: Sodium 144 mEq/L, Potassium 3.6 mEq/L, Bicarbonate 26 mEq/L, Blood urea nitrogen: 12 mg/dl, Creatinine 0.6 mg/dl. You order a few more tests and on the basis of which you diagnose insulinoma. What set of following results leads to this diagnosis? (Serum Glucose, Insulin, C-Protein)
. Increased, Decreased, Increased
. Increased, Increased, Increased
. Decreased, Increased, Increased
. Decreased, Increased, Decreased
. Normal,Normal,Normal
165) A 65-year-old male is brought by his wife to the emergency department because of a very high fever. He has also had a cough productive of greenish, nonbloody sputum for the past two days. He is diabetic, and had pneumonia 3 months ago. He has been smoking one pack of cigarettes daily for 27 years. His temperature is 38.4° C (101.2°F), blood pressure is 118/74 mm Hg, pulse is 98/min, and respirations are 24/min. Physical examination reveals cervical lymphadenopathy, and some scattered rales are heard on the right lung base. Chest-x ray shows a right lower lobe infiltrate. Laboratory studies reveal: Hb 12.6 gm/dL, WBC 40,000/cmm, Platelets 190,000/cmm. Peripheral smear: Segmented neutrophils 10%, Bands 4%, Lymphocytes 85%, Monocytes 1%. Some variant lymphocytes, and smudge cells are seen on the peripheral smear. What is the most appropriate way to confirm the diagnosis of this patient?
. Epstein Barr virus serology
. Bone marrow biopsy
. Lymph node biopsy
. Cytogenetic analysis
. Lung biopsy
166) A father brings his 7-year-old boy to the office because "his eyes are getting yellow". The boy has no other complaints. However, he is feeling tired and does not feel like going to the next Steelers game. There is a history of diabetes and lung cancer in the family. His vitals are stable, but he has pallor, jaundice, and splenomegaly. His labs revel: WBC 10,000/cmm, Hemoglobin 10 gm/dl, Hematocrit 28%, RBC count 3.5 million, Platelets 240,000/cmm, Reticulocyte count 4%. RBC indices were as follows:MCV 90 fl, MCHC 38%, MCH 28 pg. Peripheral smear revealed anisocytosis, some spherocytosis, and polychromatophilia. Coomb's test was negative. LFTs showed: Albumin 5.2 g/dl, AST 47U/L, ALT 52U/L, Alkaline phosphatase 120 U/L, Total bilirubin 3.0 mg/dl, Direct bilirubin 0.2 mg/dl. What is the next step?
. Bone marrow biopsy
. Osmotic fragility test
. Sugar water test
. Hemoglobin electrophoresis
. Serum B 12 level
167) A 50-year-old pale man comes to the office and says, "For the past year, I've been feeling very weak. I get tired early, and I feel that I've lost my sense of humor. I find it difficult to remember things now." When asked about his social history, he says, "I'm jobless and am living on social security benefits. I don't drink or smoke anymore, but I was charged with driving under the influence three times before." His parents died of old age. He shares his room with four friends. His vital signs are normal. CBC reveals: WBC 5,500 /mm3, Hemoglobin 7.0 mg/dl, Hematocrit 22%, Platelets 196,000/mm3, RBC count 1.7 million, MCV 119 fl, MCH 36, MCHC 28%, Reticulocyte count 04%. Peripheral smear shows anisocytosis, poikilocytosis, and basophilic stippling. What is the best next step in the management of this patient?
. Iron studies
. Osmotic fragility test .
. Serum B12 and folate levels
. Sugar water test
. Bone marrow biopsy with prussian blue staining
168) A 45-year-old white male presented to his primary care physician due to easy fatigability. He is a pure vegetarian and a known alcoholic. Physical examination revealed significant pallor. His hemoglobin level was 10.8gm/dl, and serum iron studies were within normal limits. His physician placed him on folic acid (1 mg daily), and his hemoglobin level increased to 13gm/dl over a period of several months. The patient continued to take folic acid for the next two years. On his next follow-up visit, he complained of gradual memory loss and difficulty in maintaining his balance for the past six months. Which of the following is the most likely thing to consider at this point?
. He has been treated with subtherapeutic doses of folic acid
. He should be referred for CT of the abdomen with and without contrast
. The physician should have checked his vitamin B12 levels
. Order FTA-ABS to rule out syphilis
. The patient should have been started on pyridoxine
169) A 39-year-old woman comes to the office and complains of double vision. She feels "weak all over," especially at the end of the day. She had the same complaints 8 months ago that persisted for several weeks, but she didn't see a doctor because she had no insurance then. She has no past medical history. Her mother has rheumatoid arthritis, and her brother has type 1 diabetes mellitus. Her vital signs are normal. She has diplopia and mild ptosis. Her blood profile, CBC and thyroid tests are within normal limits. Electromyography and repetitive nerve stimulation reveals a decremental response in compound action potentials. Her acetylcholine receptor antibody test is positive. Which of the following tests should be ordered next?
. Muscle biopsy
. Edrophonium (Tensilon) test
. Anti-Jo antibodies
. Anti-RNP antibodies
. CT scan of chest
170) A 51-year-old man comes to you complaining of increased itching, especially after bathing. He also has occasional headaches and dizziness. There is no history of smoking or alcohol use. His sister has psychiatric problems and both parents died in a car accident, many years ago. His vitals are; Temperature: 36.7°C (98.2°F); BP 148/90 mm Hg; PR 77/min; RR 12/min. On examination, his spleen is enlarged and he appears plethoric. CBC was ordered and came back as: WBC 14,500/mm3, Hemoglobin 21.5, Hematocrit 64%, Platelets 521,000/mm3, RBC count 7.6 million, MCH 30, MCHC 36, MCV 92, ROW 15.1 (n=10.3-14.1). Which of the following is expected on further work up?
. Absence of measurable erythropoetin in urine
. Elevated ESR
. Markedly elevated serum cortisol level
. Elevated brain natriureteric peptide level
. Hyponatremia and hyperkalemia
171) A 35-year-old white female slipped and fell on her side 2 days ago while she was going down the stairs from her house. Since that time, she has been having pain in her right shoulder. She describes this as an ache, which has been about the same over the last couple of days. She has tried ibuprofen, with only slight relief. She denies smoking and alcohol use. Examination suggests a shoulder sprain. You order an x-ray and see a normal shoulder but incidentally a 1.5cm coin-shaped lesion, in the outer side of right lung with well-aerated surrounding lung. She denies any respiratory complaints. What is the next best step regarding her lung lesion?
. Ask for an old X-ray
. CT scan chest
. Fine needle aspiration
. Bronchoscopy
. Open lung biopsy
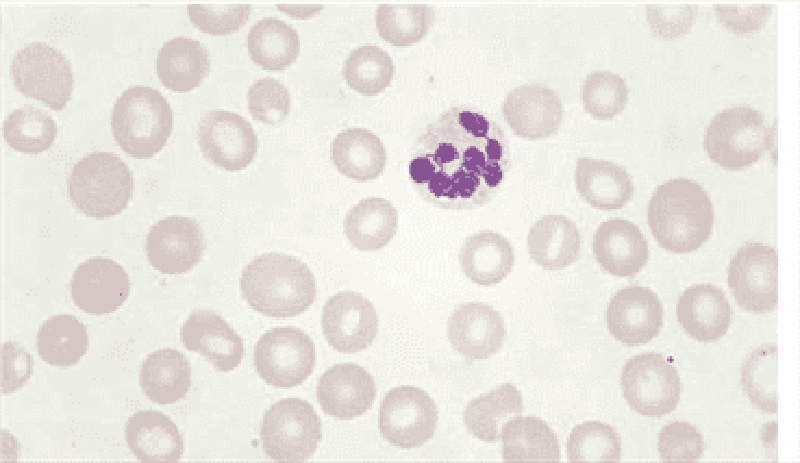
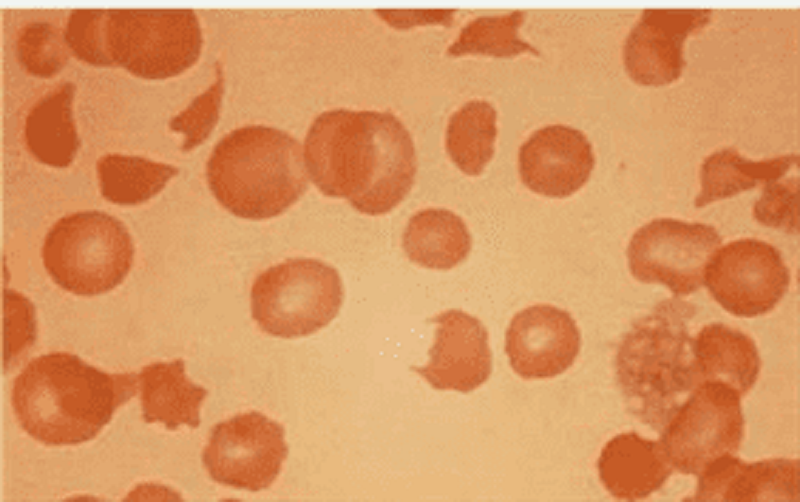
172) A 74-year -old Caucasian man is evaluated for occasional palpitations and poor exercise tolerance. He has been living alone since his wife died two years ago. His diet consists mainly of precooked food that he heats up in the microwave oven. He has a history of degenerative joint disease and hypertension. He takes a daily aspirin, hydrochlorothiazide, and glucosamine. He quit smoking 20 years ago and occasionally drinks alcohol. His peripheral blood smear is shown below. Which of the following substances is most likely elevated in this patient's blood?
. Ferritin
. Methionine
. Haptoglobin
. Homocysteine
. Cobalamin
173) A 45-year-old male with Burkitt's lymphoma is being treated with combination chemotherapy and allopurinol. On the 3rd day of treatment, he is noted to have decreased urine output and increased levels of BUN and creatinine. The patient is started on vigorous hydration. EKG reveals prolonged QT intervals. The suspected diagnosis is tumor lysis syndrome. Complete metabolic profile is ordered. Which of the following sets of results are expected in this patient? (Calcium, Phosphate, Potassium, Uric Acid)
. Increased, Increased, Increased, Increased
. Decreased, Decreased, Decreased, Decreased
. Decreased, Decreased, Increased, Increased
. Decreased, Increased, Increased, Increased
Decreased, Increased, Decreased, Decreased
174) A 55-year-old woman comes with complaints of episodes of night sweats and fever, for the last 6 weeks. She denies any cough or other respiratory complaints. She has lost 201b (9kg) and does not feel like eating anything. She denies smoking or alcohol use. Her brother was recently diagnosed with polycythemia vera. Physical examination reveals pallor and splenomegaly. Chest-X ray is within normal limits. Blood work is ordered and results are: WBC 66,100/cmm, Hemoglobin 8.70, Hematocrit 30%, Platelets 610,000/cmm. The leukocyte distribution on differential smear was: Promyelocyte 1%, Myelocyte 8%, Metamyelocyte 15%, Bands 35%, Segmented Neutrophils 25%, Lymphocytes 14%, Monocytes 2%. Further tests are ordered. Which one of the following is expected in this patient?
. Elevated leukocyte alkaline phosphatase
. Increased bone marrow iron
. Absence of measurable erythropoetin in urine
. Presence of auer rods
. Decreased leukocyte alkaline phosphatase
175) A 62-year-old man comes to the office and complains of increasing fatigue and weakness for the last 4 months. He also describes a dull pain in his back and arms, which gets worse with walking. He denies any numbness or paresthesia. On examination, he appears pale. There is tenderness around the lumbar spine. CBC reveals: WBC 8,600 mm3 with normal differential, Hemoglobin 8.6 g/dl, Hematocrit 27%, Platelets 164,000 mm3. The RBC morphology is significant for a rouleaux appearance. The ESR is 55mm/hr. Bence Jones proteins are identified in the urine. Which of the following is expected in this patient's bone marrow examination?
. Over proliferation of plasma cells
. Increased marrow cellularity with megakaryocytic hyperplasia
. Hypoplastic fat- filled marrow with no abnormal cells
. Normocellular bone marrow
. Hypocellular and fibrotic bone marrow
176) A 27 year-old African-American woman presents to the emergency room complaining of unilateral leg swelling, pleuritic chest pain and shortness of breath. She reports a rash on her face that worsens in the sun, two previous miscarriages, and complains of recent painful swelling in both knees. A CT angiogram confirms a pulmonary embolus. Which of the following is the most likely laboratory abnormality?
. Decreased prothrombin time (PT)
. Absent Von Willebrand's factor
. Prolonged partial thromboplastin time (PTT)
. Increased bleeding time
. Thrombocytosis
177) A 60-year-old man comes to office with persistent complaints of malaise and easy fatigability, for the past 8 months. On examination, he appears pale. PR 93/min; BP 127/84mm Hg; Temperature 37°C (98.6°F); RR 16/min. Fecal occult blood test is negative. Further testing is ordered that include CBC, serum electrolytes and colonoscopy. The results are: WBC 7,600/mm3, Hemoglobin 8.8 gm/dl, Hematocrit 30%, RBC count 3.6 million, Platelets 211,000/mm3. RBC Indices were:MCV 65 fl, MCH 16.5 pg, MCHC 26%, Reticulocyte count 0.5%. Which one of the following is expected on iron studies in this patient? (Serum Iron, Ferritin, TIBC, Transferrin Saturation)
. Low,High,Low,Lowto normal
. Normal, Normal, Normal, Normal
. High,Normai,High,Normal to High
. Low,Low,High,Low
. Low,Low,Low,Low
1) A 55-year-old woman comes to her primary care physician with complaints of pain, itching and red streaks in her left arm. She feels that her arm is "simply not the same". She had a similar episode in her chest almost 2 weeks ago, but it went away on its own. She has no other complaints, except for heartburn and some upper abdominal pain that has been there for a few months. She takes antacids for it, but has never got over it completely. She thinks that she has lost some weight but she feels happy about it, as she always wanted to lose weight. Her vitals are stable and there is mild epigastric tenderness. She has tender, erythematous, cord like veins palpable over left arm and some over the chest. She smokes 1-2pack/day for 15years and drinks alcohol, only on parties. What is the next best step in this patient?
. Upper GI endoscopy with barium swallows
. Colonoscopy
. Antibiotics and reassurance
. CT scan abdomen
. Spiral CT chest
2) A 51-year-old man comes to the office for his annual examination. He is apparently healthy, and does not have any complaints. His diet is normal, and he exercises regularly. He experiences some stress at work, but says that he is "strong and can fight it out." His father died of a heart attack 4 years ago, and his mother has Alzheimer's disease. His brother has recently been diagnosed with colonic polyps. His vital signs are stable. Hematology and chemistries are within normal limits, but the fecal occult blood test (FOBT) is positive. What is the best next step in the management of this patient?
. Perform screening sigmoidoscopy
. Perform double contrast barium enema
. Do colonoscopy
. Advise him to change his diet and examine him next week
. Order abdomen radiograph for air under the diaphragm
3) A 35-year-old man presents with gastrointestinal complaints for the last 4 months. He currently has fever, bloody diarrhea, nausea, and severe abdominal cramps. He has lost 20 lb (9kg), and has also been feeling fatigued and anorexic. His temperature is 37.3°C (99.1° F), blood pressure is 110/74 mm Hg, pulse is 98/min, and respirations are 22/min. Physical examination reveals tenderness in the right lower quadrant. Digital rectal examination is positive for occult blood. His blood work shows: WBC 11,600 /mm3, Hemoglobin 9.6 g/dl, Hematocrit 30%, Platelets 214,000 /mm3. Flexible sigmoidoscopy reveals larger areas of ulceration within the colon. What is the best next step in the management of this patient?
. Refer him for procto-colectomy
. Dietary modification and reassurance
. Give sulfasalazine
. Perform a biopsy of the colon lesion
. Give a bolus of corticosteroids
4) A 34-year-old man presents to your office for a routine check-up. He has no current complaints except for being "a little stressed out." He works as an executive officer and travels a lot within the country. He does not smoke and consumes alcohol occasionally. He currently takes no medications. His family history is insignificant. His blood pressure is 130/80 mmHg and heart rate is 80/min. Chest examination is unremarkable. The liver span is 8 cm and the spleen is not palpable. There is no cervical lymphadenopathy. Laboratory studies show: Erythrocyte count 5 million/mm3, Hemoglobin 14.0 g/dL, Leukocyte count 8,000/mm3, Platelet count 80,000/mm3. Which of the following is the best initial test for this patient?
. Epstein-Barr virus titers
. HIV antibody test
. Rapid plasma reagin test
. Schilling test
. Blood folate level
5) A 25-year-old female presents to your office complaining of exertional dyspnea and fatigue. Her past medical history is insignificant. She does not smoke or consume alcohol. Her blood pressure is 110/70 mmHg and heart rate is 90/min. Physical examination reveals pale conjunctiva. The laboratory values are: ESR 15 mm/hr, Hemoglobin 7.5 g/dL, MCV 70 fl, MCHC 29%, Leukocyte count 7,000/cmm, Segmented Neutrophils 55%, Bands 3%, Eosinophils 3%, Basophils 0%, Lymphocytes 32%, Monocytes 7%. What is the best next step in the management of this patient?
. Bone marrow sampling
. Iron studies
. Serum folate level
. Schilling test
. HbA2 measurement
6) A 40-year-old male comes to the office because of progressive knee and shoulder pain, which he describes as 5/10 in intensity and started 6 months ago. He has no other medical problems, except for newly diagnosed diabetes. He admits to "chain smoking" for "all his life" and drinks 1-2 bottles of beer a night. He is faithful to his wife. His mother died of "blood cancer" when he was 3-years-old. His father also has diabetes mellitus. His temperature is 37°C (98.6° F), pulse is 86/min, blood pressure is 134/86 mmHg, and respirations are 16/min. Physical examination reveals slightly swollen and tender knee joints. Mild hepatomegaly is present on abdominal examination. What is the best next step in the management of this patient?
. HbA1C level
. Serum iron studies
. Liver biopsy
. X-ray of the shoulder and knee
. Steroid injection of the joint
7) A 42-year-old male presents to your office complaining of fatigue. His past medical history is insignificant. He does not smoke or consume alcohol. His blood pressure is 120/70 mmHg and heart rate is 85/min. Physical examination is insignificant. Laboratory values are: Hemoglobin 7.7 g/dL, MCV 72 fL, MCHC 28%, Leukocyte count 8,000/cmm, ESR 15 mm/hr. Serum iron and ferritin levels are decreased. What is the next best step in the management of this patient?
. Iron supplementation
. Dietary modifications
Test for occult blood in the stool
. Work-up for malabsorption
. Bone marrow sampling
8) A 35-year-old male is brought to the emergency room with headaches and confusion for the past 2 days. He denies any focal weakness or sensory symptoms. His past medical history is significant for HIV and hepatitis C infections for which he is not receiving therapy. The remainder of his medical history is unobtainable due to his mental status. On physical exam, he has a temperature of 37.9°C (100.2°F), a blood pressure of 140/86 mm Hg, a pulse of 96/min, and respirations of 16/min. Mild icterus is present. The patient's oropharynx is clear and his neck is supple and without rigidity. Examination of his chest and abdomen are unremarkable. Neurologic examination reveals no focal deficits. Laboratory studies show: Complete blood count:Hemoglobin 7.6 g/L, MCV 85 fl, Reticulocytes 8.1%, Platelet count 80,000/mm3, Leukocyte count 3,500/mm3. Chemistry panel: Blood urea nitrogen (BUN) 30 mg/dL, Serum creatinine 2.2 mg/dL, Serum calcium 10.0 mg/dL, Blood glucose 98 mg/dL. Liver studies:Total bilirubin 3.6 mg/dL, Direct bilirubin 1.0 mg/dL, Alkaline phosphatase 120 U/L, Aspartate aminotransferase (SGOT) 178 U/L, Alanine aminotransferase (SGPT) 255 U/L. Which of the following is the most appropriate next step in the management of this patient?
. Liver biopsy
. Peripheral blood smear
. Right upper quadrant ultrasound
. Lumbar puncture
. CT scan of the head
9) A 46-year-old woman comes to the office and says, "I can't believe I've lost so much weight in the last 2 months because I seem to be eating much more than ever. I also find it odd that I drink lemonade all the time, and I have to rush to the bathroom regularly. It seems like everything in me is vanishing."Her temperature is 37°C (98.6°F), blood pressure is 110/70mm Hg, pulse is 98/min, and respirations are 14/min .Physical examination reveals a lean woman with an erythematous, scaly plaques on her face, and on her buttocks. The laboratory studies reveal: WBC 6,400 /mm3, Hemoglobin 8.7 g/dL, Hematocrit 29%, Platelets 193,000/mm3, Sodium 144 mEq/L, Potassium 3.6 mEq/L, Bicarbonate 21 mEq/L, Blood urea nitrogen 16 mg/dl, Creatinine 0.6 mg/dL, Glucose 245 mg/dL. Which of the following is expected in this patient?
. Increased thyroxine level
. Decreased insulin level
. Increased glucagon level
. Increased gastrin level
. Increased serotonin level
10) A 56-year-old woman comes to the office for the evaluation of an ulcer on her left elbow. The ulcer is a persistent, scaly red patch with irregular borders, and it sometimes crusts or bleeds. She recalls the time when she badly burned her left elbow while learning how to cook pasta at thirteen years of age. She works as a public relations officer in a large marketing company. She is a social smoker, and does not like drinking alcohol. Physical examination of the left elbow reveals a big scar with a firm, nontender, reddened, non-healing indolent, 3cm ulcer in the center. What is the best next step in the management of this patient?
. Surgical excision
. Punch biopsy
. Observation for 3 weeks with antibiotics
. Chemotherapy
. Local radiation
11) A 56-year-old male is being evaluated for increased fatigability. His past medical history is significant for severe aortic stenosis that required aortic valve replacement, diabetes mellitus, and osteoarthritis. Peripheral blood smear findings are shown on the slide below. Which of the following laboratory findings would you most expect to find in this patient?
. Increased total serum iron level
. Decreased serum haptoglobin level
. Increased mean corpuscular volume
. Decreased reticulocyte count
. Decreased serum albumin level
12) A 64-year-old woman comes to the hospital due to an "irritating sore throat for 3 months." She admits to smoking 1 pack of cigarettes daily for the past 29 years, and continues to smoke. She was jailed twice for driving under the influence of alcohol, and went to Alcohol Rehabilitation last year. She currently denies any alcohol intake. She has no fever or any other complaints. She had a complete hysterectomy several years ago for symptomatic fibroids. Her vital signs are stable. Physical examination reveals a 1.5-cm right cervical lymph node. The rest of the examination is normal. Biopsy of the lymph node reveals metastatic squamous cell carcinoma. The CT scan of the chest is negative. What is the best next step in the management of this patient?
. Empirical chemotherapy
. Pan-endoscopy
. Repeat CT in 3 months
. Screening mammogram
. Radical neck dissection
13) A 45-year-old white male comes to the emergency room with "all sorts of things going wrong with him", for the last few months. He has a severe headache, chest and abdominal pain. He is sweating profusely. He has lost weight recently, has diarrhea and palpitations. He is feeling hot all the time. Vital signs reveal BP: 190/100mm of Hg; PR 124/min; RR 18/min; Temperature 37.7° C (99.8°F). On physical examination he has enlarged cervical lymph nodes. Examination of the thyroid reveals multiple thyroid nodules. FNA biopsy reveals thyroid C-cell hyperplasia. Which of the following can also be found on laboratory results?
. Decreased serum calcitonin
. Increased serum phosphorus
. Decreased serum alkaline phosphatase
. Decreased urine metanephrine
. Increased serum calcium
14) A 24-month-old pale child is brought to the office by his mother, who says, "Doc, I think he is under some weird spell. He acts bizarre and always seems tired. He likes to eat wooden, painted toys." The child and her mother live in a relatively poor neighborhood. CBC reveals:WBC 8,600 /mm3, Hemoglobin 7.1 g/dl, Hematocrit 25%, Platelets 166,000 /mm3. His blood lead levels are elevated. Which of the following is most likely seen in this child's peripheral blood smear?
. Megaloblastic anemia and basophilic stippling
. Tear-drop RBCs and hypochromic, microcytic anemia
. Loss of concavity of the RBC and basophilic stippling
. Basophilic stippling and microcytic, hypochromic anemia
. Normochromic, normocytic anemia and basophilic stippling
15) A 42-year-old white female, who has a long history of dysfunctional uterine bleeding, presented with exertional shortness of breath. On examination, she appears very pale and there is a pulmonic flow murmur heard over the second intercostal space. Her vitals are: BP: 130/80mm of Hg; HR: 80/min and regular; RR: 16/min; Temperature 36.7°C (98°F).Initial evaluation reveals hemoglobin of 8.2 gm/dL. WBC count is within normal limits. You are suspecting an iron deficiency anemia secondary to excessive bleeding. Which one of the following studies is most definite for the diagnosis of iron deficiency anemia?
. A low serum ferritin level
. Increased total iron binding capacity
. A low serum iron concentration
. Bone marrow iron staining
. Total iron content of the gastric epithelial cells
16) A 60-year-old Hispanic laboratory technician presents with increasing fatigue and generalized weakness for the last 2 months. He also has chronic pain in the lower back and legs when he walks. He has been smoking 2-3 packs of cigarettes daily for 30 years, and drinks alcohol almost daily. His mother has diabetes, while his father died of a stroke. Physical examination reveals pallor. There is mild hepatomegaly. The neurological examination is completely normal. Complete work-up reveals: CBC: Hemoglobin 9.8 g/L, MCV 85 fl, Platelets 226,000/mm3, Leukocyte count 6,500/mm3, Neutrophils 60%, Eosinophils 1%, Lymphocytes 29%, Lvlonocytes 10%. Chemistry panel: Serum sodium 138 mEq/L, Serum potassium 4.0 mEq/L, Bicarbonate 24 mEq/L, Blood urea nitrogen (BUN) 28 mg/dL, Serum creatinine 2.1 mg/dL, Calcium 11.2 mg/dL, Blood glucose 98 mg/dL. Liver studies: Albumin 4.0 mg/dL, Total protein, serum 9.5 g/dL, Total bilirubin 1.0 mg/dL, Direct bilirubin 0.8 mg/dL, Alkaline phosphatase 110 U/L, Aspartate aminotransferase (SGOT) 58 U/L, Alanine aminotransferase (SGPT) 25 U/L. ESR is 100 mm/h. What is the best next step in the management of this patient?
. ANA and anti-Smith antibodies
. Serum immunoelectrophoresis
. Bone marrow biopsy
. Kidney biopsy
. Bone scan
17) A 57-year-old man comes to the office and complains of long-standing heartburn and chest pain. He describes the pain as burning in nature, and unrelated to eating. For the past week, his interest in things has decreased, and he has been more tired than usual. He has lost almost 40 lbs (18kg) in the last 6 months. He used to smoke 6-10 cigarettes daily, but he quit 4 years ago. He drinks alcohol occasionally. He takes ranitidine for his heartburn. His father died at the age of 67 from lung cancer. His vital signs are stable. Physical examination is unremarkable. The chest x-ray result is within normal limits. What is the best next step in the management of this patient?
. Bronchoscopy
. CT scan of the chest with and without contrast
. Barium swallow followed by endoscopy
. Give omepra zole and follow-up in 2 months
. Test and eradicate Helicobacter pylori infection
18) A 50-year-old woman comes to the office and complains of right shoulder pain which radiates to her hand. She has had cough for many weeks, and feels "more tired than the usual." In addition, her fingers are always swollen, and she now finds it difficult to walk because her knees give way. She has had rheumatoid arthritis for the past 10 years and is used to having pain in her joints; however, she believes that this pain is not due to her arthritis. She takes celecoxib for rheumatoid arthritis. She admits to smoking one pack of cigarettes daily for the past 25 years and to drinking one odd beer every night. All her family members have crippling rheumatoid arthritis. Her vital signs are stable. She is afebrile. Physical examination reveals drooping of the right eyelid and miosis. What is the best next step in the management of this patient?
. CT scan of head and neck
. X-ray of the shoulder
. Steroid therapy
. Chest x-ray
. Nerve conduction study
19) A 54-year-old patient walks into a blood donation camp at a community hospital. His blood report shows an ELISA positive for HIV and HBsAg. He is notified of this finding, and a subsequent western blot test is also positive for HIV. Considering this new diagnosis of HIV, which of the following is indicated in this patient?
. Hepatitis B vaccine
. PPO skin test and anti-Toxoplasma antibody titer
. Serum transaminases and lipid profile
. Trimethoprim-sulfamethoxazole prophylaxis
. Hepatitis C antigen
20) A 25-year-old female presents to her physician with a painful ulcerative lesion on her labia for the past 2 days. She also complains of dysuria. She admits to having sexual intercourse with multiple partners for the last 6 years. Tzanck preparations of one of her lesions reveal multi-nucleated giant cells. She is encouraged to undergo testing for HIV and other STDs. Which of the following is the most appropriate screening test for HIV infection?
. HIV serology by ELISA
. HIV serology by western blot
. HIV viral load
. Absolute CD4 count
. P 24 antigen assay
21) A 27-year-old, HIV-positive man comes to his physician with a two-day history of fever, profuse watery diarrhea, and abdominal cramps. He has been taking zidovudine, didanosine, and indinavir for the past eight months. His temperature is 37.9°C (100.2°F), pulse is 102/min, respirations are 14/min, and blood pressure is 105/70 mm Hg. He is started on fluid and electrolyte support. What is the most appropriate next step in the management of this patient?
. Stop antiretroviral therapy and send stool for Clostridium difficile toxin assay
. Colonoscopy with biopsy of the colonic mucosa
. Stool examination for ova and parasites
. Start empiric treatment for cytomegalovirus
. Loperamide and lactose-free diet until diarrhea subsides
22) A 49-year-old man presents with a three-week history of fever, weight loss, and anorexia. He also reports muscle aches. He has no cough or shortness of breath. He has a thirty pack-year history of cigarette smoking. His temperature is 38.9°C (102°F), blood pressure is 120/76mm Hg, pulse is 90/min, and respirations are 16/min. Lungs are clear to auscultation. The rest of the physical examination is unremarkable. Blood cultures reveal Streptococcus bovis. Echocardiogram reveals vegetations on the mitral valve. Other than antibiotic treatment, what further step is recommended in this patient?
. Cystoscopy
. Colonoscopy
. Bronchoscopy
. Fecal occult blood testing
. CT scan of the head
23) A 43-year-old male presents to a physician with an ulcer on the shaft of his penis. The ulcer is non-tender, with a raised border and a smooth base. There is bilateral inguinal adenopathy. The rest of the examination is unremarkable. Dark field microscopy of a specimen from the ulcer base reveals spirochetes. Which of the following additional screening studies should be performed on this patient?
. VDRL
. FTA-ABS
. HIV antibodies by ELISA
. Proctosigmoidoscopy
. Serum prostate specific antigen
24) A 19-year-old man presents to your office with a one-week history of fever, fatigue, and sore throat. He denies diarrhea or rash. He has no significant past medical history. His brother died of cystic fibrosis at 14 years of age. He admits to occasional cigarette use and alcohol consumption. He has smoked marijuana several times but has never used injectable drugs. He is sexually active with one partner and uses condoms occasionally. Physical examination reveals enlarged tonsils with a whitish exudate and enlarged, slightly tender lymph nodes deep to the sternocleidomastoid muscle bilaterally. The exam is otherwise unremarkable. Which of the following is the best initial test in this patient?
. Rapid plasma reagin (RPR)
. Heterophile antibody test
. HIV antibody determination
. Lymph node biopsy
. Purified protein derivative
25) A 17-year-old man presents with new symptoms of fatigue, malaise, fever, and a sore throat. He has no significant past medical history and is not on any medications. Physical examination is entirely normal except for enlarged, palpable cervical, lymph nodes. He reports no weight loss or night sweats. Laboratory investigations include a normal chest x-ray, negative throat swab, but abnormal blood film with atypical lymphocytes. The hemoglobin is 15.5 g/dL; hematocrit 42%; platelets 290,000/mL; WBC 10500/mL, with 45% segmented neutrophils, 1% eosinophils, and 54% lymphocytes, of which 36% were atypical. Which of the following is the most appropriate initial diagnostic test?
Lymph node biopsy
Bone marrow
Erythrocyte sedimentation rate (ESR)
Heterophil antibody (sheep cell agglutination) test
Hepatic biopsy
26) A 30-year-old male presents with right upper quadrant pain. He has been well except for an episode of diarrhea that occurred 4 months ago, just after he returned from a missionary trip to Mexico. He has lost 7 pounds. He is not having diarrhea. His blood pressure is 140/70, pulse 80, and temperature 37.5°C (99.5°F). On physical examination there is right upper-quadrant tenderness without rebound. There is some radiation of the pain to the shoulder. The liver is percussed at 14 cm. There is no lower-quadrant tenderness. Bowel sounds are normal and active. Which of the following is the most appropriate next step in evaluation of the patient?
. Serology and ultrasound
. Stool for ova and parasite
. Blood cultures
. Diagnostic aspirate
. Empiric broad-spectrum antibiotic therapy
27) A 30-year-old male with sickle cell anemia is admitted with cough, rusty sputum, and a single shaking chill. Physical examination reveals increased tactile fremitus and bronchial breath sounds in the left posterior chest. The patient is able to expectorate a purulent sample. Which of the following best describes the role of sputum Gram stain and culture?
. Sputum Gram stain and culture lack the sensitivity and specificity to be of value in this setting
. If the sample is a good one, sputum culture is useful in determining the antibiotic sensitivity pattern of the organism, particularly Streptococcus pneumoniae
. Empirical use of antibiotics for pneumonia has made specific diagnosis unnecessary
. There is no characteristic Gram stain in a patient with pneumococcal pneumonia
. Gram-positive cocci in clusters suggest pneumococcal infection
28) A 25-year-old male student presents with the chief complaint of rash. He denies headache, fever, or myalgia. A slightly pruritic maculopapular rash is noted over the abdomen, trunk, palms of the hands, and soles of the feet. Inguinal, occipital, and cervical lymphadenopathy is also noted. Hypertrophic, flat, wartlike lesions are noted around the anal area. Laboratory studies show the following: Hct: 40%, Hgb: 14 g/dL, WBC: 13,000/μL, Diff: 50% segmented neutrophils, 50% lymphocytes. Which of the following is the most useful laboratory test in this patient?
. Weil-Felix titer
. Venereal Disease Research Laboratory (VDRL) test
. Chlamydia titer
. Blood cultures
. Biopsy of perianal lesions
29) A previously healthy 19-year-old female university student develops myalgia, headache, fever, and malaise. Blood tests reveal lymphocytosis, with 20% of the lymphocytes being atypical. She remains tired and unwell for 6 weeks, but repeated tests for heterophil antibody are negative. Which of the following is the most likely diagnosis?
Epstein-Barr virus (EBV) infection
Primary HIV infection
Human herpes virus type 7 (HHV-7)
CMV infection
Toxoplasmosis
30) A 20-year-old female college student presents with a 5-day history of cough, low-grade fever (temperature 37.8°C [100°F]), sore throat, and coryza. On examination, there is mild conjunctivitis and pharyngitis. Tympanic membranes are inflamed, and one bullous lesion is seen. Chest examination shows a few basilar rales. Sputum Gram stain shows white blood cells without organisms. Laboratory findings are as follows: Hct: 31, WBC: 12,000/μL, Lymphocytes: 50%, Mean corpuscular volume (MCV): 94 nL, Reticulocytes: 9% of red cells, CXR: bilateral patchy lower lobe infiltrates. Which of the following is the best method for confirmation of the diagnosis?
. High titers of antibody to adenovirus
. High titers of IgM cold agglutinins or complement fixation test
. Methenamine silver stain
. Blood culture
. Culture of sputum on chocolate media
31) A 20-year-old woman complains of headache and discomfort in both sides of her jaw. Physical examination reveals enlarged parotid glands that are slightly tender on palpation. There is reddening of the orifice of Stensen’s duct on intra oral examination; her temperature is 38.3°C, and the pulse rate is 80/min. Laboratory data show hemoglobin 14 g/dL; hematocrit 40%; WBC 11000/mL, with 33% segmented neutrophils, 7% monocytes, and 60% lymphocytes. Which of the following diagnostic tests will help to confirm the diagnosis of epidemic parotitis?
Single blood sample for a specific immunoglobulin G (IgG)
Blood cell count
Blood culture
Single blood test for a specific immunoglobulin M (IgM)
Serum amylase
32) A 19-year-old male presents with a 1-week history of malaise and anorexia followed by fever and sore throat. On physical examination, the throat is inflamed without exudate. There are a few palatal petechiae. Cervical adenopathy is present. The liver span is 12 cm and the spleen is palpable. Throat culture: negative for group A streptococci, Hgb: 12.5, Hct: 38%, Reticulocytes: 4%, WBC: 14, 000/μL, Segmented: 30%, Lymphocytes: 60%, Monocytes: 10%, Bilirubin total: 2.0 mg/dL (normal 0.2 to 1.2), Lactic dehydrogenase (LDH) serum: 260 IU/L (normal 20 to 220), Aspartate aminotransferase (AST): 40 U/L (normal 8 to 20 U/L), Alanine aminotransferase (ALT): 35 U/L (normal 8 to 20 U/L), Alkaline phosphatase: 40 IU/L (normal 35 to 125). Which of the following is the most important initial test combination to order?
. Liver biopsy and hepatitis antibody
. Streptococcal screen and antistreptolysin O (ASO) titer
. Peripheral blood smear and heterophile antibody
. Toxoplasma IgG and stool sample
. Lymph node biopsy and cytomegalovirus serology
33) A 27-year-old man presents with diarrhea. He returned 3 weeks ago from a trip to rural South America. Over the past few days, he has gradually developed lower abdominal pain and diarrhea. Now the symptoms are much worse with eight stools a day consisting mostly of mucus and blood. He is afebrile, the abdomen is tender in left lower quadrant, and the remaining examination is normal. His stool is mostly comprised of blood and mucus. Which of the following is the most appropriate initial diagnostic test?
Stool culture
Stool toxin assay
Examination of a dried stool specimen
Immunofluorescence of stool specimen
Examination of a wet stool specimen
34) A 60-year-old male complains of low back pain, which has intensified over the past 3 months. He had experienced some fever at the onset of the pain. He was treated for acute pyelonephritis about 4 months ago. Physical examination shows tenderness over the L2-3 vertebra and paraspinal muscle spasm. Laboratory data show an erythrocyte sedimentation rate of 80 mm/h and elevated C-reactive protein. Which of the following statements is correct?
. Hematogenous osteomyelitis rarely involves the vertebra in adults
. The most likely initial focus of infection was soft tissue
. Blood cultures will be positive in most patients with this process
. An MRI scan is both sensitive and specific in defining the process
. Surgery will be necessary if the patient has osteomyelitis
35) A 40-year-old school teacher develops nausea and vomiting at the beginning of the fall semester. Over the summer she had taught preschool children in a small town in Mexico. She is sexually active, but has not used intravenous drugs and has not received blood products. Physical examination reveals scleral icterus, right upper quadrant tenderness, and a palpable liver. Liver function tests show aspartate aminotransferase of 750 U/L (normal < 40) and alanine aminotransferase of 1020 U/L (normal < 45). The bilirubin is 13 mg/dL (normal < 1.4) and the alkaline phosphatase is normal. What further diagnostic test is most likely to be helpful?
. Liver biopsy
. Abdominal ultrasound
. IgM antibody to hepatitis A
. Antibody to hepatitis B surface antigen
. Determination of hepatitis C RNA
36) A 24-year-old woman comes to the physician because of a 24-hour history of right flank pain, burning micturition and high-grade fever with chills. Her temperature is 102°F (38.9°C), blood pressure is 90/60 mm Hg, pulse is 130/min, and respirations are 20/min. Physical examination shows costovertebral angle tenderness. Which of the following is the most likely urine dipstick finding in this patient?
. Positive for nitrites and esterase
. Positive for nitrites only
. Positive for esterase only
. Negative for both esterase and nitrites
. Negative for esterase and positive nitrites
37) A 27-year-old woman complains of fatigue, low-grade fevers, anorexia, headaches and skin rash over the past several weeks. She also notes new exertional dyspnea and an unintentional 5-pound weight gain over the past two weeks. On physical examination, her blood pressure is 190/110 mmHg and her heart rate is 90/min. Which of the following is the most likely finding on this patient's urinary tests?
. High VMA excretion
. High daily cortisol excretion
. Red blood cells
. Glucosuria
. Uric acid crystals
38) A 70-year-old man comes to the physician because of nocturia. He states that over the past two years his urinary frequency has increased and he has to strain while passing urine. He also notes dribbling of a few drops of urine at the end of voiding. Sometimes he has to void again within two hours. He has no other symptoms. He has no history of diabetes mellitus, stroke or trauma. He does not take any medication. His father had surgery of the prostate for benign prostatic hyperplasia. He has a 15-pack-years history of cigarette smoking. Rectal examination shows smooth, firm enlargement of the prostate with no induration. Neurological examination shows no abnormalities. Laboratory study shows a serum creatinine of 0.7 mg/dl. Which of the following studies is indicated at this time?
. Blood urea nitrogen
. Ultrasound of kidney, bladder and ureter
. Urinalysis
. Serum prostate specific antigen
. Cystoscopy
39) A 65-year-old man comes to the physician because of increased urinary frequency and urgency, as well as suprapubic discomfort His temperature is 37C(98.6F), blood pressure is 130/75 mm Hg, pulse is 76/min, and respirations are 14/min. Rectal examination shows prostatic induration; physical examination otherwise shows no abnormalities. Urinalysis shows no abnormalities. Expressed prostatic secretions show a leukocyte count of 20 WBCs/HPF (normal is less than 10 WBCs/HPF). They are sent for culture and sensitivity, and fail to grow any bacteria. Serum prostatic specific antigen is 2 ng/ml (normal value is less than 4ng/ml). A diagnosis of nonbacterial prostatitis is suggested. Which of the following is the most appropriate next step in management?
. Perform urinary cytology and cystoscopy
. Repeat urinalysis
. Repeat culture of prostatic secretions
. Treatment with oral erythromycin
. Treatment with oral trimethoprim-sulphamethoxazole
40) A 33-year-old woman comes to the emergency department due to a 4-day history of left-sided flank pain, nausea, vomiting, fevers and chills. Her temperature is 39°C (102°F) and blood pressure is 100/60 mm Hg. Examination shows significant left costovertebral angle tenderness. Urinalysis shows positive nitrites, many WBC and bacteria. Laboratory studies show a WBC count of 17,000/cmm with 8% bands. Which of the following is the most appropriate next step in management?
. Intravenous pyelogram
. Intravenous antibiotics
. Blood cultures
. CT scan of the abdomen
. Ultrasound of the abdomen
41) A 14-year-old boy comes to the physician because of a 2-day history of fever and nasal discharge. He has also had malaise, fatigue and myalgia. His temperature is 38.8°C (101.9°F), blood pressure is 130/70mm Hg, pulse is 90/min, and respirations are 15/min. Examination shows no abnormalities. Urine dipstick testing shows proteinuria but there is no hematuria or pyuria; urinalysis otherwise shows no abnormalities. Which of the following is the most appropriate next step in management?
. Repeat dipstick testing
. BUN and serum creatinine
. 24-hour urinary collection for protein
. Renal ultrasound
. Reassurance
42) A 57-year-old man comes to the physician because of 2 episodes of hematuria. He also complains of cough fatigue and fever for several days. He has smoked two packs of cigarettes daily for 25 years. He does not use alcohol or drugs. Vital signs are stable. Examination shows a left-sided varicocele which fails to empty when the patient is recumbent; examination otherwise shows no abnormalities. Laboratory studies show Hb of 16.2 g/dl and platelets of 480,000/cmm. Which of the following is the most appropriate diagnostic step in management?
. Chest x-ray
. Abdominal CT scan
. Urinalysis
. Serum alfa-fetoprotien levels
. Ultrasonogram of the testicles
43) A patient with benign prostatic hyperplasia has moderately severe symptoms and is started on finasteride. After six months of treatment with finasteride, his symptoms improve remarkably and his prostate has regressed in size. Which of the following histological patterns was most likely present at the time of initiation of treatment?
. Hyperplasia of prostate with predominance of epithelial components
. Hyperplasia of prostate with predominance of muscular element
. Hyperplasia of prostate with predominance of collagen
. Hyperplasia of prostate with predominance of both collagen and smooth muscles
. Hyperplasia of prostate with predominance of glandular tissue
44) A 65-year-old woman comes to the physician because of a two-month history of fatigue and weight gain. She has rheumatoid arthritis and hypertension. She takes hydrochlorothiazide and naproxen. She does not use tobacco, alcohol, or drugs. Her blood pressure is 120/70 mm Hg, pulse is 80/min, and respirations are 14/min. Physical examination shows generalized edema; liver is palpated 2 cm below the costal margin. Urinalysis shows 4+ proteinuria. Ultrasound of the kidneys shows slight enlargement. Renal biopsy was performed. Which of the following is the most likely finding on renal specimen analysis?
. Crescent formation on light microscopy
. Deposits revealed under polarized light
. Linear immunoglobulin deposits revealed on immunofluorescence microscopy
. Granular immunoglobulin deposits revealed on immunofluorescence microscopy
. Normal light microscopy findings
45) A 73-year-old man comes to the physician because of a one-year history of progressively worsening urinary urgency, hesitancy, nocturia, and weak urinary stream. He has no fever, abdominal pain, hematuria, malaise or weight loss. He takes atenolol for essential hypertension. He has no history of diabetes mellitus or ischemic heart disease. He does not use tobacco, alcohol, or drugs. Rectal examination shows a smooth, firm enlargement of the prostate with no induration or asymmetry. Neurological examination shows no abnormalities. Urinalysis shows no abnormalities. Laboratory studies show serum creatinine of 2.1 mg/dl. Which of the following is the most appropriate next step in management?
. Ultrasound of kidneys, ureters, and bladder
. Watchful waiting
. Transurethral resection of prostate
. Treatment with finasteride
. Treatment with prazosin

46) A 30-year-old woman comes to the office due to the recent onset of fever, chills, and dysuria. Her temperature is 38.3°C (101.0°F), blood pressure is 110/70mm Hg, pulse is 68/min, and respirations are 15/min. Examination shows tenderness at the right costovertebral angle. Laboratory studies show WBC count of 16,000/microl with left shift. Urinalysis shows bacteriuria and pyuria. Her urine and blood is collected for culture and sensitivity. She is prescribed oral ciprofloxacin and sent home. After three days, she returns for a follow-up visit. She is still febrile, and the physical examination is unchanged. The blood cultures have no growth after 72 hours of incubation. Results of the urine culture show. Which of the following is the most appropriate next step in management?
. Start intravenous ampicillin and gentamicin
. Start intravenous ciprofloxacin
. Continue oral ciprofloxacin for another 10 days
. Perform renal ultrasound
. Renal CT scan
{"name":"DES 2016. Final (Paer 33)", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"124) A 70-year-old man presents with a complaint of fatigue. There is no history of alcohol abuse or liver disease; the patient is taking no medications. Scleral icterus is noted on physical examination; the liver and spleen are nonpalpable. The patient has a normocytic, normochromic anemia. Urinalysis shows bilirubinuria with absent urine urobilinogen. Serum bilirubin is 12 mg\/dL, AST and ALT are normal, and alkaline phosphatase is 300 U\/L (three times normal). Which of the following is the best next step in evaluation?, 125) A 45-year-old woman presents with a 1-week history of jaundice, anorexia, and right upper quadrant discomfort. On examination she is icteric, with a tender right upper quadrant and liver span of 14 cm. There is no shifting dullness or pedal edema and the heart and lungs are normal. On further inquiry, she reports consuming one bottle of wine a day for the past 6 months. Which of the following laboratory tests are most likely to be characteristic of a patient with jaundice secondary to alcoholic hepatitis?, 126) A 60-year-old man with a history of alcohol abuse presents to the ED with hematemesis for 1 day. He denies abdominal or chest pain. On physical examination, his eyes appear reddened which he attributes to having drunken heavily the night before (he also reveals vomiting several times after this recent binge). Vital signs are HR 115 beats per minute, BP 130\/85 mm Hg, RR 18 breaths per minute, and temperature 99.5°F. Chest radiograph is unremarkable. Laboratory results reveal a WBC 10,000\/μL, haemoglobin 14 mg\/dL, hematocrit 40%, and platelets 210\/μL. Which diagnosis is endoscopic evaluation most likely to confirm?","img":"https://cdn.poll-maker.com/11-504667/3.png?sz=1200"}
More Quizzes
DSP Orientation Test
122610
Master Your Motion Knowledge
11613
The rock
1059
Учебен Квиз за Пето Одделение
15822
The Crucible Act 3 - Free Knowledge Check
201020593
K-Pop Girl Group Name Generator - Free
201017084
Black Music Trivia - Soul & R&B Classics with Answers
201020490
What Type of Worker Are You? Free Work Style
201017401
Attila the Hun - Test Your Knowledge (Free)
201022563
What Angel Are You? - Discover Your Angel Type
201018461
What Animal Crossing Villager Are You? Free
201017209
Friends Trivia - How Well Do You Know the Show?
201016552