
DES 3 ep 7
67) A 27-year-old Caucasian male is diagnosed with medullary thyroid carcinoma that is non-resectable. His past medical history is insignificant. He does not smoke or consume alcohol. His family history is significant for thyroid cancer and pheochromocytoma in his father. Which of the following tests could have been most effective in preventing this patient's non-resectable cancer?
. Annual physical examination
. Frequent self-examination of the neck
. Periodic serum calcium measurement
. Periodic stimulated serum calcitonin measurement
. DNA testing
68) A 35-year-old Caucasian male presents with weakness, fatigue, and weight loss over the past year. He is anorexic and has lost interest in all his activities. His temperature is 37.1°C (99°F), pulse is 84/min, blood pressure is 101/72 mmHg, and respirations are 14/min. On physical examination, he does not appear to be in acute distress. Dark brown pigmentation is present on his skin creases and oral cavity mucous membranes. Laboratory studies show: Hemoglobin 10.3 g/dL, WBC count 3,000/micro-L, Neutrophils 60%, Monocytes 5%,Eosinophils 10%, Basophils 1%, Lymphocytes 24%, Serum sodium 130 meq/L, Serum potassium 5.5 meq/L. Chest x-ray and PPD tests are normal. What is the most appropriate next step in the management of this patient?
. 24-hour urinary free cortisol
. Measure plasma ACTH level
. Low-dose overnight dexamethasone suppression test
. Begin intravenous hydrocortisone
. Cosyntropin stimulation test
69) A 56-year-old female comes to the office and complains of general malaise and headaches. Her other symptoms are episodic palpitations, throbbing headaches and diaphoresis. She feels "very anxious all the time." Her past medical history is unremarkable. Her deceased sister had very high blood pressure. Her blood pressure is 230/110 mmHg and pulse is 110/min. Initial laboratory studies reveal: WBC 7,000/cmm, Hb 11.2 g/L, Platelets 325,000/cmm, Calcium 11.9 mg/dl. What is the best next step in the evaluation of this patient?
. Serum calcitonin levels
. Nuclear renal scan
. CT scan of the head
. Endoscopy to look for ulcer disease
. Echography of liver
70) A 23-year-old man presents to your office complaining of occasional headaches, muscle weakness and fatigue. He also describes periodic numbness of his extremities. The symptoms started 6 months ago and have gradually progressed. His past medical history is insignificant. He is not taking any medication. His blood pressure is 165/104 mmHg and heart rate is 80/min. His physical examination is within normal limits. Which of the following laboratory findings is the most specific for the patient's condition?
. Metabolic alkalosis
. Low serum potassium level
. Low plasma renin activity
. High serum sodium level
. High aldosterone/renin ratio
71) A 58-year-old Caucasian male presents with polyuria and polydipsia for the past 4 months. He also reports easy bruising and difficulty in climbing stairs. He weighs 180 lbs (81.6kg) and is 5'7"(170cm) tall. His temperature is 37°C (98.6°F), pulse is 76/min, blood pressure is 155/100 mmHg, and respirations are 15/min. Physical examination reveals significant proximal muscle weakness of all the extremities. Skin examination reveals significant pigmentation on the exposed areas. Lab studies show: Sodium 145 meq/L, Potassium 2.9 meq/L, Bicarbonate 30 meq/L, Fasting blood glucose 240 mg/dL, Hemoglobin 13 g/dL, WBC 14,000/micro-L, Neutrophils 70%, Lymphocytes 23%, Monocytes 5%, Basophils 1%,Eosinophils 1%, 24hr urinary free cortisol 1100 microgram, Plasma ACTH 250 pg/mL (Normal 9-52 pg/mL). High dose dexamethasone suppression test did not decrease the 24 hr urinary cortisol excretion. Which of the following is consistent with this patient's findings?
. Adrenal adenoma
. Cushing's disease
. Bilateral adrenal hyperplasia
. Exogenous glucocorticoids
. Ectopic ACTH production
72) A 60-year-old white male is hospitalized due to an acute myocardial infarction. His other medical problems include type 2 diabetes mellitus, hypertension, chronic obstructive pulmonary disease, and degenerative joint disease. He admits to smoking 2 packs of cigarettes daily for the past 20 years, as well as drinking 2 bottles of beer daily for the past 15 years. His medications include aspirin, glyburide, metoprolol, enalapril, heparin, and albuterol and ipratropium inhalers. His blood pressure is 140/80 mmHg, pulse is 80/min, respirations are 16/min, and temperature is 36.7°C (98.0°F). During his stay in the hospital, a number of blood tests were ordered. Which of the following lab abnormalities is an indication for thyroid function testing?
. Unexplained hypernatremia
. Hyperlipidemia
. Thrombocytopenia
. Unexplained hypocalcemia
. Neutropenia
73) A 45-year-old unconscious male is brought to the emergency room. His airway is secured, oxygen is administered, and his vitals are as follows Temperature 36.4°C (97.8°F); PR 102/min; BP 90/65 mmHg; RR 27/min. An IV line is secured and blood and urine samples are drawn. Lab results are as follows: Blood urea nitrogen 40 mg/dl, Calcium 9.1 mg/dl, ALT 50 U/L, AST 60 U/L, Ammonia 15 micro-mol/1 (Normal is 9-33 micro-mol/1), PT 13 sec, APTT 30 sec, Amylase 100 U/L, Glucose 400 mg/dl, Sodium 134 meq/L, Potassium 5.2 meq/L, Chloride 97 meq/L, Bicarbonate 12 meq/L. Arterial Blood Gases: PH 7.19, PaCO2 25 mm Hg, PaO2 80 mm Hg. Blood and urine are positive for ketones. A diagnosis of diabetic ketoacidosis (DKA) is made and IV infusion of normal saline and regular insulin are started. What will be a most reliable index for monitoring the response to treatment?
. Serum osmolality
. Urine glucose
. Urine ketones
. Serum ketones
. Serum anion gap
74) A 27-year-old woman presents to the office due to a significant amount of hair on her cheeks, chin and upper lips. This symptom developed over the past two months. Her last menstrual period was 12 weeks ago, but she did not seek medical help because her home pregnancy test was negative. Her medical history is unremarkable. She denies taking any medications other than oral contraceptive pills. Physical examination reveals acne on the forehead and cheeks; there is terminal hair on the upper lip, cheeks, chin, upper chest and lower abdomen. Examination of the genitals shows clitoromegaly. The abdominal exam is normal; the uterus is normal in size. Ultrasound reveals a normal uterus and ovaries, but there is a left adrenal mass. Which of the following measurements is most specific for this patient's condition?
. Testosterone
. Luteinizing hormone (LH)
. Dehydroepiandrosterone-sulfate
. Adrenocorticotropic hormone (ACTH)
. Dihydrotestosterone
75) A 16-year-old female presents to the office with her mother and complains of changes in her physical appearance over the past year. She first noted the appearance of dark hair on the cheeks, upper lips, around the nipples and umbilicus. Her menstrual cycles have always been irregular since her menarche at age 14. Her medical history is otherwise unremarkable. She denies taking any medications. She has a boyfriend, but claims that she is still not sexually active. Her blood pressure is 115/65 mmHg, pulse is 80/min, respirations are 16/min, and temperature is 37°C (98°F). Pelvic examination could not be performed, and abdominal examination is normal. Ultrasound is normal. Results of the initial work-up are as follows: Serum Na+ 140mEq/L, Serum K+ 4.0mEq/L, Serum Cl- 98 mEq/L, Bicarbonate 25 mEq/L, 1,7-alpha-hydroxyprogesterone elevated. According to these findings, which of the following hormone deficiencies does this patient most likely have?
. 17 -alpha-hydroxylase-deficiency
. 21-hydroxylase-deficiency
. 11-beta-hydroxylase-deficiency
. 3-beta-hydroxysteroid-dehydrogenase deficiency
. Cystathionine synthase deficiency
76) A 6-year-old boy presents to his pediatrician for a routine physical examination. His mother reports no problems over the past year except that he seems to be shorter than the other boys in his class. His mother is 163 cm (5'4") tall and experienced menarche at age 12 years, and his father is 178 cm (5'10") tall and went through puberty at approximately age 14 years. On his growth curve, the boy’s height was at the 10th percentile at birth, at the sixth percentile by age 3 years, and at the third percentile now. His weight is currently at the 25th percentile. Which of the following is most important in this patient’s evaluation?
Colonoscopy
Chromosomal analysis
Insulin-like growth factor-1 level
Growth hormone level
No further evaluation is necessary
77) A 16-year-old obese Hispanic girl presents to her physician’s office complaining of ugly skin around my neck‖ and having to wear turtlenecks. On examination the physician notes darkening and thickening of the skin, which has a velvety appearance. Which of the following is the most appropriate course of action?
Obtain a serum glucose test
Obtain a CT scan of the abdomen
Obtain a shave biopsy of the affected skin
Obtain a punch biopsy of the affected skin
Obtain liver function tests
78) A 30-year-old female complains of palpitations, fatigue, and insomnia. On physical examination, her extremities are warm and she is tachycardic. There is diffuse thyroid gland enlargement and proptosis. There is thickening of the skin in the pretibial area. Mild clubbing of digits is present. Which of the following laboratory values would you expect in this patient?

nn

. Increased free thyroxine (free T4), increased TSH
Increased free thyroxine, decreased TSH
. Increased free thyroxine, normal TSH
. Normal free thyroxine, elevated triiodothyronine (T3), normal TSH
. Normal free thyroxine, decreased TSH
79) A 45-year-old woman with chronic alcohol abuse admitted 3 days ago for nausea and severe diarrhea now complains of perioral and finger tingling. She was admitted for hydration after 1 week of severe watery diarrhea. She has been receiving intravenous hydration and dextrose but has not been able to take oral nutrition secondary to continued nausea. Her blood pressure is 130/74 mmHg, pulse is 68/min, and respiratory rate is 16/min. She is afebrile. Physical examination is significant for facial twitching on percussion of her facial nerve just anterior to the ear, as well as the induction of carpal spasm after the inflation of a blood pressure cuff on her arm. Which of the following is most likely to have caused these findings?
Azotemia
Hypernatremia
Hypophosphatemia
Hypomagnesemia
Hypouricemia
80) A 17-year-old girl has never had a menstrual period. On physical examination, she has minimal breast development and no axillary or pubic hair. She is color blind and has had a diminished sense of smell since birth. Laboratory evaluation would most likely reveal which of the following?
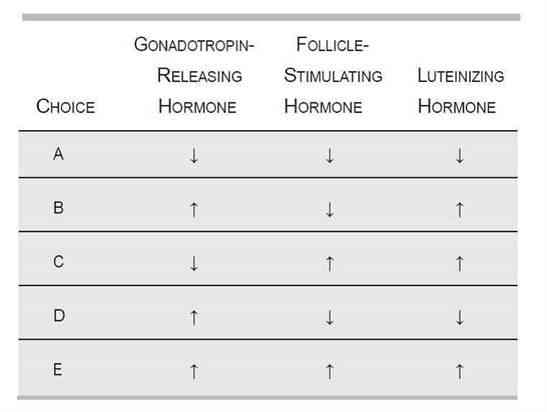
mm

A
B
C
D
E
81) A 65-year-old black female presents for an annual examination. Physical examination is unremarkable for her age. In completing the appropriate screening tests, you order a dual x-ray absorptiometry (DXA) to evaluate whether the patient has osteoporosis. DXA results reveal a T-score of -3.0 at the total hip and −2.7 at the spine, consistent with a diagnosis of osteoporosis. Since her Z-score is -2.0, you proceed with an initial evaluation of secondary osteoporosis. Laboratory evaluation reveals: Calcium: 9.7 mg/dL, Cr: 1.0 mg/dL, Bun: 19 mg/d, Glucose: 98 mg/dL, 25, OH vitamin D: 12 ng/mL (optimal > 25), WBC: 7700/μL, Hg: 12 g/dL, HCT: 38 g/dL, PLT: 255,000/μL. Based on the above information, additional laboratory would most likely reveal which of the following?
. Normal iPTH, normal ionized calcium, elevated alkaline phosphatase
. Elevated iPTH (intact parathormone), low ionized calcium, normal alkaline phosphatase
. Normal iPTH, low ionized calcium, elevated alkaline phosphatase
. Elevated iPTH, normal ionized calcium, elevated alkaline phosphatase
. Elevated iPTH, low ionized calcium, normal alkaline phosphatase
82) A 58-year-old male is referred to your office after evaluation in the emergency room for abdominal pain. The patient was diagnosed with gastritis but a CT scan with contrast performed during the workup of his pain revealed a 2-cm adrenal mass. The patient has no history of malignancy and denies erectile dysfunction. Physical examination reveals a BP of 122/78 mmHg with no gynecomastia or evidence of Cushing syndrome. His serum potassium is normal. What is the next step in determining whether this patient’s adrenal mass should be resected?
. Estradiol level
. Plasma aldosterone/renin ratio
. Testosterone level
. Plasma metanephrines and dexamethasone-suppressed cortisol level
. Repeat CT scan in 6 months
83) A 36-year-old white female comes to the office due to swelling in front of her neck. She denies any hoarseness, dysphagia, fever, chills, diarrhea, constipation, heat or cold intolerance, and changes in appetite or weight. Her menstrual cycles are regular. She does not have any history of head and neck irradiation. Her family history is negative for thyroid problems. Her blood pressure is 130/80 mmHg, pulse is 80/min, respirations are 16/min, and temperature is 36.7°C (98.0°F). Examination of the neck shows a 2 x 2 cm, discrete, non-tender, firm, mobile nodule in the left thyroid lobe. There is no cervical lymphadenopathy. The rest of the examination is normal. Which of the following is the most appropriate next step in the evaluation of this patient?
. Measurement of free T4 and anti-thyroid antibodies
. Measurement of TSH
. Fine needle aspiration biopsy
. Radionuclide scan with iodine 131
. Ultrasound of the thyroid gland
84) A 40-year-old African American female comes to you for her routine medical check-up. She admits to smoking one pack of cigarettes daily for the last 20 years. Her mother and one maternal uncle have diabetes. Her height is five feet six inches, and weight is 130 lbs. Her blood pressure is 122/80 mmHg, pulse is 80/min, respirations are 16/min, and temperature is 37°C (98°F). What is the most appropriate screening test for diabetes mellitus?
. 50 g glucose tolerance test
. Random blood glucose measurement
. 75 g glucose tolerance test
. Blood glucose measurement after an 8 hour fast
. 100 g glucose tolerance test
85) A 41-year-old woman presents to the emergency department with palpitations. On questioning she notes heat intolerance, nervousness, and insomnia. On physical examination the physician notes a fine tremor, diffuse non-pitting edema of the anterior lower leg, and bulging of both of her eyes. What finding on blood test would confirm the diagnosis?
Increased creatine kinase-myocardial bound
Anti-thyroid-stimulating hormone receptor antibodies
Increased thyroid-stimulating hormone levels
Decreased thyroid-stimulating hormone levels
Positive antinuclear antibody
86) A 4-year-old boy is brought to the pediatrician by his worried mother. She notes that he urinates 10 times a day and is always drinking water. She also reports that despite eating more than either of his brothers did at the same age, he is not gaining any weight. Which of the following human leukocyte antigen (HLA) types is associated with the most likely diagnosis for this child?
HLA-B27
HLA-B51
HLA-DR2
HLA-D11
HLA-DR3
87) A 40-year-old alcoholic male is being treated for tuberculosis, but he has not been compliant with his medications. He complains of increasing weakness, fatigue, weight loss, and nausea over the preceding three weeks. He appears thin, and his blood pressure is 80/50 mmHg. There is increased pigmentation over the elbows and in the palmar creases. Cardiac examination is normal. Which of the following is the best next step in evaluation?
. Early morning serum cortisol and cosyntropin stimulation
. CBC with iron and iron-binding capacity
. Blood cultures
Erythrocyte sedimentation rate
. Esophagogastroduodenoscopy (EGD)
88) A 58-year-old postmenopausal female presents to your office on suggestion from a urologist. She has passed 3 kidney stones within the past 3 years. She is taking no medications. Her basic laboratory work shows the following: Na: 139 mEq/L, K: 4.2 mEq/L, HCO3: 25 mEq/L, Cl: 101 mEq/L, BUN: 19 mg/dL, Creatinine: 1.1 mg/dL, Ca: 11.2 mg/dL. A repeat calcium level is 11.4 mg/dL; PO4 is 2.3 mmol/L (normal above 2.5). Which of the following tests will confirm the most likely diagnosis?
. Thyroid function profile
. Serum ionized calcium
. Liver function tests
. Intact parathormone (iPTH) level
. 24-hour urine calcium
89) A 14-year-old boy presents at the pediatric clinic for a routine check-up. The patient had developed end-stage renal disease over the previous 2 years, and was successfully treated with a renal transplant 6 months prior. Since his operation, he has developed purple striae on his back and arms, central obesity, and an increasingly round face. During the subsequent blood analysis, which of the following results would be most likely?

A
B
D
C
E
90) A 64-year-old man presents to the emergency department after a motor vehicle crash and receives a CT of the abdomen that shows a finding of a unilateral mass in the left adrenal gland. He is unharmed from the accident, feels well, and has never smoked. His blood pressure is 155/90 mmHg, deep tendon reflexes are 3/4, and muscle strength is 4/5. Laboratory studies show: Na+: 150 mEq/L, K+: 3.0 mEq/L, Cl−: 105 mEq/L, HCO −: 36 mEq/L. Plasma renin activity is also decreased. Which of the following is most likely to be increased?
Carcinoembryonic antigen
Aldosterone
Prostate-specific antigen
Anion gap
Troponin
91) A 19-year-old man with insulin-dependent diabetes mellitus is taking 30 units of NPH insulin each morning and 15 units at night. Because of persistent morning glycosuria with some ketonuria, the evening dose is increased to 20 units. This worsens the morning glycosuria, and now moderate ketones are noted in urine. The patient complains of sweats and headaches at night. Which of the following is the most appropriate next step in management?
. Increase the evening dose of NPH insulin further
. Measure blood glucose levels at bedtime
. Obtain blood sugar levels between 2:00 and 5:00 AM
. Add regular insulin to NPH at a ratio of 2/3 NPH to 1/3 regular
. Add lispro via a calculated scale to each meal; continue NPH
92) A 48-year-old high school teacher with no prior medical history presents to his primary care physician after feeling extremely fatigued for > 1 month. Previously an avid runner, he has recently experienced dyspnea on moderate exertion. Although he denies vomiting, he admits to intermittent episodes of diarrhea. His blood pressure is 73/37 mmHg and he is afebrile. On physical examination his skin is warm and erythematous, and his jugular venous pressure is elevated. Cardiac examination reveals a systolic murmur near the right border of the sternum that is accentuated with inspiration. Which of the following is most consistent with these findings?
Peaked T waves on ECG
Elevated urinary excretion of 5-hydroxyin- doleacetic acid
Pseudomonas species grown from blood cultures
Elevated urinary excretion of vanillylman- delic acid
Severe pulmonary congestion on x-ray of the chest
93) A 3010-g (6.6-lb) boy was born to a 37-year-old primagravida by spontaneous vaginal delivery after an uncomplicated pregnancy. On examination he has cyanotic extremities and a significant right precordial heave, a single S2, and a harsh systolic ejection murmur along the sternal border. He also has a prominent squared nose and cleft palate. An echocardiogram is subsequently performed and demonstrates tetralogy of Fallot. Corrective surgery is performed without complications. At 2 months of age the infant is diagnosed with Pneumocystis jiroveci pneumonia, and at 3 months he is diagnosed with fungal septicemia. Additional work-up of this child should include which of the following tests?
Quantitative immunoglobulin levels
Hemoglobin electrophoresis
Renal ultrasound
Nitroblue tetrazolium
Serum calcium
94) A 50-year-old female is evaluated for hypertension. Her blood pressure is 130/98 mmHg. She complains of polyuria and mild muscle weakness. She is on no blood pressure medication. On physical examination, the PMI is displaced to the sixth intercostal space. There is no sign of congestive heart failure and no edema. Laboratory values are as follows: Na+: 147 mEq/dL, K +: 2.3 mEq/dL, Cl−: 112 mEq/dL, HCO3: 27 mEq/dL. The patient denies the use of diuretics or over-the-counter agents to decrease fluid retention or promote weight loss. She does not eat licorice. Which of the following tests is most useful in establishing a diagnosis?
. 24-hour urine for cortisol
. Urinary metanephrine
. Renal angiogram
. Plasma renin activity
. Ratio of serum aldosterone to plasma renin activity
95) A 36-year-old female complains of inability to lose weight despite low-calorie diet and daily exercise. She has also noticed that she is cold intolerant. She is wearing a jacket even though it is summer. She also reports constipation and hair loss. These symptoms have been worsening over the past 2 to 3 months. An elevated TSH and low total and free T4 confirm your suspicion of hypothyroidism. You suspect the etiology of this patient’s hypothyroidism to be autoimmune thyroiditis. What is the best test to confirm the diagnosis of autoimmune thyroiditis?
. 24-hour radioactive iodine uptake
. Thyroid peroxidase antibody (TPOAb)
. Thyroid ultrasound
Antinuclear antibody
. Thyroid aspiration
96) A 72-year-old man with end stage renal disease secondary to hypertension presents with several months of back pain. He denies fever, weight loss, difficulty walking, altered sensation in his legs, or incontinence. He was diagnosed with renal disease 20 years ago and was managed medically for many years. However, 2 years ago he began hemodialysis because of a progressive decline in renal function. There is no family history of renal disease or malignancy. Physical examination is unremarkable. X-ray of the chest shows ill-defined bands of increased bone density adjacent to the vertebral endplates. What laboratory abnormalities is most likely in this patient?
Decreased parathyroid hormone
Elevated parathyroid hormone
Elevated bone-specific alkaline phosphatase
Bence-Jones protein in urine
Decreased phosphate
97) An 82-year-old woman presents 1-hour after the sudden onset of moderate-to-severe epigastric pain. The pain radiates to her back, both scapulae, and both arms. She has been nauseated and vomited three times in the past hour. Her past medical history is remarkable for peptic ulcer disease 10-years ago, cholelithiasis for the past 6-years, and stable angina pectoris for the past 3-years. She has had occasional episodes of biliary colic and two bouts of acute cholecystitis which were treated conservatively. Her temperature is 36.8°C (98.2°F), blood pressure is 120/70 mmHg, pulse is 90/min, and respirations are 14/min. The lungs are clear to auscultation. Abdominal examination shows a soft abdomen with mild tenderness to palpation in the epigastrium. Murphy's sign is negative. Which of the following studies should be done first?
. Electrocardiogram
. Abdominal ultrasound
. Upright abdominal x-ray
. Upper GI endoscopy
. Serum amylase and lipase
98) A 65-year-old woman presents with a 2-month history of fatigue and dyspnea on exertion. She takes no medication. Her temperature is 36.7°C (98°F), blood pressure is 162/83 mmHg, pulse is 100/min, and respirations are 21/min. Auscultation shows a 2/6 systolic murmur in the 2nd right intercostal space. No peripheral edema is noted. Rectal examination shows no abnormalities. Test of the stool for occult blood is negative. EKG shows sinus tachycardia and non-specific ST-T changes. Laboratory studies show: Hemoglobin 8.1 g/L, MCV 73 fl, Platelets 360,000/mm3, Leukocyte count 4,500/mm3, Neutrophils 56%, Eosinophils 1%, Lymphocytes 33%, Monocytes 10%. Which of the following is the most appropriate next step in management?
. Bone marrow biopsy
. Echocardiography
. Colonoscopy
. Gastro-duodenoscopy
. Isotope-labeled erythrocytes scintigraphy
99) A 45-year-old Mexican male presents with a 2-day history of traces of blood on the tissue paper after he wipes. He does not have gross blood mixed with stool, but on one occasion there were drops of blood in the toilet after defecation. He has no past medical history or family history of cancer or other significant disease. Which of the following is the most appropriate next step in management?
. Anoscopy
. Colonoscopy
. Sigmoidoscopy
. Fecal occult blood test
. Barium enema
100) A 26-year-old man presents with a 1-week history of intermittent, crampy, lower abdominal pain accompanied by rectal urgency, bloody diarrhea, nausea and vomiting. His symptoms have become more severe over the past 24 hours. His past medical history is unremarkable. He denies any recent travel or antibiotic use. His temperature is 38.5°C (102.0°F), blood pressure is 120/80 mmHg, pulse is 95/min, and respirations are 15/min. Abdominal examination reveals distension and tenderness to palpation without rebound or guarding. The bowel sounds are decreased. Rectal examination shows marked rectal tenderness and mucus mixed with blood in the vault. An x-ray film of the abdomen shows distended colon filled with gas. Laboratory studies show: Hb 10.8 g/dl, WBC 19,600/cmm, Platelet count 459,000/cmm, ESR 54/hr. Which of the following is the most appropriate next step in management?
. Stool for ova, parasites and culture
. Barium enema
. Serology for Entamoeba histolytica
Proctosigmoidoscopy and biopsy
. CT scan of the abdomen
101) A 34-year-old woman complains of occasional diarrhea and crampy lower abdominal pain. She says that at times her symptoms hamper her performance in important business meetings. The pain sometimes occurs after meals but is not always preceded by eating. The pain is often accompanied by diarrhea with small amounts of stool and mucus. Her past medical history is significant for bleeding hemorrhoids. Her mother died of colon cancer. Which of the following findings is most likely in this patient?
. Folic acid deficiency
. Normal colonic mucosa
. Duodenal ulcer
. Crypt abscesses
. Intestinal villous atrophy
102) A 40-year-old female presents with abdominal discomfort. The discomfort is localized to the center of the upper abdomen and is not related to meals or fatty food. She has a history of similar symptoms. She has not had gastrointestinal bleeding, fatigue, dysphagia, or weight loss. Her mother has a history of gastric ulcer. Her vital signs are within normal limits. Complete physical examination is unremarkable. Stool for heme occult is negative. Complete blood count and serum chemistries are within normal limits. Which of the following is the most appropriate next step in management?
. Endoscopy
. Barium swallow
. Empiric trial of H2 blockers
. H. Pylori breathe test
. Empirical antibiotic trial
103) A 30-year-old woman presents with a 5-month history of episodic retrosternal pain that radiates to the interscapular region. The pain episodes typically last 15 minutes, and are precipitated by emotional stress and hot or cold food. Her relative gave her sublingual nitroglycerine tablets, which alleviated the pain. Her past medical history is unremarkable, and she does not take any other medications. There is no family history of coronary artery disease. Her vital signs are within normal limits. Physical examination shows no abnormalities. A lipid profile is within normal limits. An EKG shows a normal sinus rhythm. A stress test fails to reproduce the symptoms or to induce ST/T wave changes. Chest x-ray, upper GI endoscopy, and echocardiography show no abnormalities. Which of the following is the most appropriate next step in diagnosis?
. Esophageal motility studies (manometric recordings)
. CT scan of the chest with contrast
. Acid perfusion (Bernstein) test
. Coronary angiogram
. Pulmonary perfusion/ventilation scintigraphy
104) A 45-year-old male comes to the physician for epigastric pain and diarrhea. His past medical history is significant for chronic duodenal ulcers. He has been smoking 2 packs of cigarettes daily for the past 10 years. He occasionally drinks alcohol. He denies illegal drug use or multiple sexual partners. Physical examination shows abdominal tenderness without rebound or rigidity. Endoscopy shows prominent gastric folds, chronic duodenal ulcer, and upper jejunal ulceration. Which of the following is the most appropriate next step in the diagnosis of this patient?
. Serum chromogranin A
. Secretin stimulation test
. Calcium infusion study
. Gastric acid secretion study
. Serum gastrin concentration
105) A 32-year-old female from South America presents with a 3-month history of progressive difficulty with swallowing for both liquids and solids. At night she has a bitter taste in her mouth. Over the past two months, she has had a 10 lb (4.54 kg) weight loss. She has not had any previous illnesses, and does not take any medication. Physical examination is unremarkable. A lateral x-ray film of the chest shows extreme dilatation of the esophagus with an air fluid level. Which of the following is the diagnostic test for this patient's condition?
. Endoscopy
. Barium swallow
. PH monitoring
. Manometry
. CTscan
106) A 50-year-old man presents with a 3-hour history of right arm pain. Two weeks ago, he was treated for superficial thrombophlebitis of the right cephalic and right saphenous veins. For the past two months, he has had significant back pain, which is being treated with NSAIDs. His temperature is 37.0°C (98.6°F), blood pressure is 140/80 mmHg, pulse is 70/min, and respirations are 10/min. Physical examination shows a swollen, ruddy and warm right arm, but is otherwise unremarkable. Cervical and chest x-ray films show no abnormalities. Laboratory studies show: Hct 50%, Platelets 120,000/cmm, WBC 9,600/cmm, Neutrophils 60%, Eosinophils 2%, Basophils 0%, Lymphocytes 31%, Monocytes 7%, PT 25 sec, PTT 39 sec, Fibrinogen 300 mg/dL, Fibrin split products positive. Which of the following is the most appropriate next step in management?
Venography of right brachial, axillary and subclavian veins
. Protein C, S and antithrombin III levels
. CT of the chest abdomen and pelvis
. Perfusion scintigraphy of the lungs
. CT of the thoracic outlet
107) A 45-year-old Asian-American female comes to the physician due to bloating, flatulence, abdominal cramps and explosive watery diarrhea. These symptoms occur after ingesting dairy products. She has not had any weight loss. She has not had bone pain or easy bruising. Physical examination shows abdominal distention and borborygmi. You decide to investigate the patient further. Which of the following test results is most likely to be observed?
. Positive urine test for reducing substances
. Decreased stool osmotic gap
. Alkaline stool pH
. Positive hydrogen breath test
. Positive acid steatocrit test
108) A 50-year-old male undergoes vagotomy and pyloroplasty for a peptic ulcer perforation. His early postoperative course is complicated by fever and hypotension, which are treated with broad-spectrum antibiotics and IV fluid support. He then recovers well; however, on post-operative day 6 he develops nausea, vomiting, abdominal pain, and profuse, watery diarrhea. His temperature is 38.9°C (102° F), blood pressure is 110/70 mmHg, pulse is 120/min, and respirations are 18/min. Abdominal examination shows tenderness in the sigmoidal area. Test of the stool for occult blood is negative. Laboratory studies show: Hb 11.5g/dL, Platelet count 180, 000/cmm, Leukocyte count 17, 500/cmm, segmented neutrophils 75%, Bands 10%, Eosinophils 1%, Lymphocytes 14%. Which of the following is the most appropriate next step in management?
. Blood cultures
. Colonoscopy
. Cytotoxin assay in the stool
. Stool cultures
. Observation
109) A 68-year-old woman with a history of heavy alcohol use and chronic pancreatitis presents with a several month history of recurrent epigastric pain. The pain is occasionally associated with nausea and vomiting. She has lost 15 lbs (6.8 kg) over the past 3 months. She is afebrile. Physical examination shows scleral icterus. Laboratory studies show: Albumin 3.0 mgldl, Total bilirubin 3.5 mgldl, Direct bilirubin 24 mgldl, Alkaline phosphatase 220 U/L, Aspartate aminotransferase (SGOT) 28 U/L, Alanine aminotransferase (SGPT) 25 U/L, Amylase 145 U/L, Lipase 100 U/L. Which of the following is the most appropriate next step in management?
. ERCP
. CT scan of the abdomen
. Plain abdominal radiography
. MRI of the abdomen
. Upper GI endoscopy
110) A 56-year-old man comes to the emergency department due to a one day history of abdominal pain and increasing distension. He has not passed flatus during this time. He has had nausea without vomiting. He has a history of cirrhosis secondary to chronic alcoholism. He is taking spironolactone and furosemide. His temperature is 38.0°C (101.3°F), blood pressure is 120/70 mm Hg, pulse is 100/min, and respirations are 24/min. Physical examination shows a slightly confused man with a flapping tremor. Breathing is labored and lungs are clear to auscultation. Abdominal examination shows distension, tenderness to palpation with rebound, and no guarding; a fluctuating wave and shifting dullness are present. Abdominal auscultation shows splashing and markedly decreased bowel sounds. An x-ray film of the chest shows no abnormalities. An x-ray film of the abdomen shows gas in the small and large bowels without air-fluid levels. Which of the following is the most appropriate next step in management?
. Barium enema
. Sigmoidoscopy
. Diagnostic peritoneal lavage
. Ultrasound of abdomen
. Diagnostic paracentesis
111) A 42-year-old male presents with a 2-year history of heartburn. The heartburn occurs after heavy meals and while supine. Over time, his symptoms have been increasing in severity and frequency. His symptoms used to be alleviated with the use of over-the-counter antacids, but these have become ineffective in the past two months. He also complains of epigastric pain and occasional vomiting, both of recent onset, especially in the morning. He denies dysphagia or odynophagia. He eats junk food and drinks two cups of coffee daily. He regularly drinks grape brandy and smokes 1 pack of cigarettes/day. Abdominal examination shows epigastric tenderness. Abdominal ultrasound is unremarkable. Test of the stool for occult blood is negative. Which of the following is the most appropriate next step in management?
. Treatment with ranitidine
. Upper GI endoscopy
. Manometric studies
. Barium swallow
. Reassurance
112) A 66-year-old man returns to the emergency department (ED) for a second time because of persistent left lower quadrant pain and developing fever, despite 48 hours of oral antibiotics. He had presented to the ED 2 days ago because of left lower quadrant pain. He was able to tolerate a diet and had no fever; he was then sent home on antibiotics, and instructed to return if there was no improvement. He has a 2-week history of constipation without regular bowel movements. Laxatives have not relieved his symptoms. His diet consists of meat with very few vegetables. His vital signs are within normal limits, except for a low-grade fever. Abdominal examination shows left lower quadrant tenderness and guarding. Rectal examination shows no abnormalities. Laboratory studies show a WBC of 16,400/cmm. He is admitted and started on IV antibiotics. Forty-eight hours later, his symptoms persist without any improvement. Which of the following is the most appropriate next step in management?
. Abdominal x-rays
. Flexible sigmoidoscopy
. CT scan
. Colonoscopy
. Barium enema
113) A 58-year-old woman presents to the emergency department with right subcostal heaviness, intermittent pain, food intolerance, and 13.2 lbs-weight loss (6kg) over the past 2 months. Her pain has been worsening for the past 2 days; it was initially localized to the right upper quadrant, but has now shifted to her back. Her past medical history is remarkable for appendicitis, which was complicated by perforation and peritonitis 20 years ago. Abdominal examination shows epigastric tenderness. There is a palpable mass below the right costal margin. Murphy's sign is negative. Abdominal ultrasound shows an enlarged gallbladder and dilation of the hepatic ducts. Laboratory studies show: WBC 11,000/cmm, Total bilirubin 24 mg/dl, Direct bilirubin 1.6 mg/dl, Alkaline phosphatase 310 U/L, Aspartate aminotransferase (SGOT) 87 U/L, Alanine aminotransferase (SGPT) 56 U/L, Amylase 140 U/L. Which of the following is the most appropriate next step in management?
. Plain abdominal film
. Endoscopic retrograde cholangiopancreatography
. CT scan of the abdomen
. Percutaneous transhepatic cholangiography
. HIDA scan for cystic duct obstruction
114) A 50-year-old white male presents with complaints of bitter taste and central chest pain. He further describes he pain as moderate-to-severe, occurring during or after meals, non-radiating, and burning. The pain is relieved with antacids, and worsened by lying supine. He has lost 10 lbs (4.5kg) over the past 5-months (unintentional). He has smoked 2 packs of cigarettes daily for 20 years. His vital signs are stable, and he is afebrile. The physical examination is unremarkable. Chest x-ray and EKG show no abnormalities. Which of the following is the most appropriate next step in management?
. Treatment with omeprazole
. Treatment with antacids
. Esophagoscopy
. Treatment with famotidine
. Esophageal pH monitoring
115) A 63-year-old man presents with a 2-month history of dysphagia for both solids and liquids. He has had a 6.6 lb (3kg) weight loss over this time. His past medical history is remarkable for a transient ischemic attack 6 months ago, two bouts of pneumonia in the past 3 months, and chronic heartburn treated with over-the-counter antacids. Physical examination shows a supple neck without masses. Abdominal examination shows mild epigastric tenderness to deep palpation. Chest x-ray is normal for his age. Which of the following is the most appropriate next step in diagnosis?
. Barium swallow
. Endoscopy
. Video fluoroscopy
. Motility studies
. 24-hour pH monitoring
116) A 47 -year-old male comes to the emergency department complaining of an intense burning pain in his abdomen. The pain started a couple of hours ago and is getting worse. He also has nausea and vomited twice. The vomitus is described as dark red-brown in color. He drank "quite a bit of alcohol' last night. He has had several episodes of this type of pain before, and was diagnosed with peptic ulcer disease five years ago. Several courses of H. Pylori eradication therapy have been prescribed in the past, but the patient admits to being non-compliant. He admits to smoking and drinking heavily. His temperature is 36.8° C (98.2° F), blood pressure is 126/88 mm Hg, pulse is 98/min, and oxygen saturation is 96% on room air. The physical examination is remarkable for marked epigastric tenderness. No masses or rebound tenderness are appreciated. IV fluids are administered, blood tests are taken, and upper Gl endoscopy is being arranged. Which of the following serum markers is most likely to be elevated in this patient?
. Platelet count
. Blood urea nitrogen
. Potassium
. Prothrombin time
. Creatinine
117) A 65-year-old Asian male presents to the physician with a four-week history of weakness and vague postprandial epigastric pain. His past medical history is insignificant. He does not take any medications. He smokes 1½packs of cigarettes daily and drinks alcohol occasionally. The fecal occult blood test is positive. Gastroduodenoscopy shows an antral ulcer. Four of seven biopsies taken from the margins of the ulcer are consistent with adenocarcinoma. Which of the following is the most appropriate next step in management?
. Serologic markers
. Helicobacter pylori testing
. A CT scan
. Laparoscopy
. Exploratory laparotomy
118) A 45-year-old male presents to the office with complaints of progressive difficulty in swallowing both solids and liquids. His other complaints include occasional regurgitation of undigested food, and a nighttime cough which disturbs his sleep. The physical examination is unremarkable. Barium studies show a dilated esophagus, loss of esophageal peristalsis, and smooth tapering of the distal esophagus. Which of the following is the most appropriate next step in management?
. Esophagoscopy
. Esophageal manometry
. Botulinum toxin injection
. Esophageal pH monitoring
. Pneumatic dilation
119) A 76-year-old man with multi-infarct dementia is brought to the emergency department because of lethargy. For the past 6 months, he has had difficulties with feeding and occasionally regurgitates undigested food. In recent days, his condition has deteriorated, and he has become lethargic. He has a history of hypertension for 15 years, chronic atrial fibrillation for 7 years, dementia for 5 years, and frequent respiratory tract infections for the past year. His temperature is 37.8°C (101.5°F), blood pressure is 150/95 mm Hg, pulse is 120/min, and respirations are 26/min. Physical examination shows foul-smelling breath; there is a fluctuating mass in the left side of his neck. Auscultation shows crackles in the right lung base. An x-ray film of the chest shows multiple infiltrates without cavitation in the right lower lung field. The patient is admitted, sputum and blood cultures are sent, and antibiotics are started. Which of the following is the most appropriate next step in management?
. Puncture of the neck mass
.Esophagoscopy
. Bronchoscopy
. Esophagography
. CT of the neck
120) A 69-year-old man has had pain in left lower quadrant (LLQ) for 3 days. The pain was intermittent, but since yesterday it has been constant. He also had sweating and chills for the last 2 days. He hasn't had a bowel movement for 4 days, but has passed flatus. He vomited once and still has nausea. His past medical history is remarkable for constipation and nephrolithiasis. His vital signs are: PR: 110/min; BP: 122/80mm Hg; RR: 24/min; Temperature: 38.6°C (101.3°F). His abdomen is soft and tender to palpation in the left lower quadrant. Deep palpation is difficult but reveals no masses or organomegaly. Bowel sounds are decreased. Rectal exam is positive for enlarged prostate. Costovertebral angle tenderness is absent. Ultrasound shows bilateral hydronephrosis and stones in the kidneys. His laboratory test results are: WBC 14,500/cmm, Hb 11.7gm/dl, Hct 34%, ESR 40/hour, BUN43 mg/dl, Creatinine 2.0 mg/dl. Urinalysis RBC 4-10/hpf; WBC 3/hpf; few hyaline casts; many oxalate crystals. The next step should be?
. Sigmoidoscopy
Intravenous pyelography
CT of abdomen
. Contrast enema
Upright abdominal film
121) A 46-year-old white male presents with chronic diarrhea, abdominal distention, flatulence, and weight loss. He also has arthralgias and bulky, frothy stools. He has never had blood transfusions, tattooing or highrisk sexual behaviors. His temperature is 38.3°C (101°F), blood pressure is 130/90 mm Hg, pulse is 84/min, and respirations are 16/min. Physical examination shows generalized lymphadenopathy and skin hyperpigmentation. Which of the following is the most appropriate diagnostic test?
. Serum TSH
. Antinuclear antibody (ANA) titer
. ELISA for anti-HIV antibodies
. Gamma-glutamyl transpeptidase levels
. Endoscopy with small bowel biopsy
122) A 40-year-old male comes to the physician complaining of diarrhea with pale, voluminous, foul-smelling stools that are difficult to flush. He has had this problem sporadically for years, but has neglected medical care. He also has severe, intermittent, epigastric pain lasting 15 to 30 minutes after eating. He admits to chronic alcohol consumption. Physical examination shows no abnormalities. Which of the following is the best test to confirm fat malabsorption in this patient?
. Acid steatocrit
. Sudan III stain
. D-xylose test
. 72-hour fecal fat collection
. Lactose tolerance test
123) A 40-year-old man with long-standing alcohol abuse complains of abdominal swelling, which has been progressive over several months. He has a history of gastrointestinal bleeding. On physical examination, there are spider angiomas and palmar erythema. Abdominal collateral vessels are seen around the umbilicus. There is shifting dullness, and bulging flanks are noted. Which of the following is the most important first step in the patient’s evaluation?
. Diagnostic paracentesis
. Upper GI series
. CT scan of the abdomen
. Ethanol level
. Examination of peripheral blood smear
124) A 70-year-old man presents with a complaint of fatigue. There is no history of alcohol abuse or liver disease; the patient is taking no medications. Scleral icterus is noted on physical examination; the liver and spleen are nonpalpable. The patient has a normocytic, normochromic anemia. Urinalysis shows bilirubinuria with absent urine urobilinogen. Serum bilirubin is 12 mg/dL, AST and ALT are normal, and alkaline phosphatase is 300 U/L (three times normal). Which of the following is the best next step in evaluation?
. Viral hepatitis profile
. Ultrasound or CT scan of the abdomen
. Serum ferritin
Reticulocyte count
. Antimitochondrial antibodies
125) A 45-year-old woman presents with a 1-week history of jaundice, anorexia, and right upper quadrant discomfort. On examination she is icteric, with a tender right upper quadrant and liver span of 14 cm. There is no shifting dullness or pedal edema and the heart and lungs are normal. On further inquiry, she reports consuming one bottle of wine a day for the past 6 months. Which of the following laboratory tests are most likely to be characteristic of a patient with jaundice secondary to alcoholic hepatitis?
. Ratio of AST: ALT is 3:1 and the AST is 500 U/L
. Ratio of AST: ALT is 2:1 and the AST is 250 U/L
. Ratio of AST: ALT is 1:1 and the AST is 250 U/L
. Ratio of AST: ALT is 1:1 and the AST is 500 U/L
. Ratio of AST: ALT is 1:3 and the AST is 750
126) A 60-year-old man with a history of alcohol abuse presents to the ED with hematemesis for 1 day. He denies abdominal or chest pain. On physical examination, his eyes appear reddened which he attributes to having drunken heavily the night before (he also reveals vomiting several times after this recent binge). Vital signs are HR 115 beats per minute, BP 130/85 mm Hg, RR 18 breaths per minute, and temperature 99.5°F. Chest radiograph is unremarkable. Laboratory results reveal a WBC 10,000/μL, haemoglobin 14 mg/dL, hematocrit 40%, and platelets 210/μL. Which diagnosis is endoscopic evaluation most likely to confirm?
. Curling ulcer
. Esophageal varices
. Perforated gastric ulcer
. Boerhaave syndrome
. Mallory-Weiss tear
127) A 73-year-old man comes to his primary care physician for his yearly check-up. His medical history is significant for obesity, new onset diabetes mellitus, and a remote history of tobacco use. The patient has noticed that his stool has been darker for the past 3 months, although he has only seen gross blood in his stool once, a week ago. He also complains of recent fatigue and occasional light-headedness when standing up from sitting. On examination the patient has fecal occult blood and a hematocrit of 32%. Colonoscopy and upper gastrointestinal endoscopy reveal no obvious pathology. Which of the following is the best diagnostic test to locate this patient’s hemorrhage?
Angiography
Barium enema
CT scan with contrast
Colonoscopy
Tagged RBC scan
128) A 70-year-old woman with a history of hypertension, congestive heart failure, and atrial fibrillation presents to the ED with several hours of acute onset diffuse abdominal pain. She denies any nausea or vomiting. The pain is constant, but she is unable to localize it. She was diagnosed with a renal artery thrombosis several years ago. Vital signs include HR of 95 beats per minute, BP of 110/70 mm Hg, and temperature of 98°F. Her abdomen is soft and mildly tender, despite her reported severe abdominal pain. Her WBC count is 12,000/μL, hematocrit 38%, platelets 250/μL, and lactate 8 mg/dL. The stool is traced heme-positive. You are concerned for acute mesenteric ischemia. What is the best way to diagnose this condition?
. Abdominal radiograph (supine and upright)
. Serum lactate levels
. Angiography
. CT scan
Barium contrast study
129) As you palpate the right upper quadrant (RUQ) of a 38-year-old woman’s abdomen, you notice that she stops her inspiration for a brief moment. During the history, the patient states that over the last 2 days she gets pain in her RUQ that radiates to her back shortly after eating. Her vitals include a temperature of 100.4°F, HR of 95 beats per minute, BP of 130/75 mm Hg, and RR of 16 breaths per minute. What is the initial diagnostic modality of choice for this disorder?
. Computed tomography (CT) scan
Plain film radiograph
Radioisotope cholescintigraphy (HIDA scan)
Magnetic resonance imaging (MRI)
. Ultrasonography
130) A 23-year-old woman presents to the ED complaining of lower abdominal pain and vaginal spotting for 2 days. Her menstrual cycle is irregular. She has a history of ovarian cysts and is sexually active but always uses condoms. Her BP is 115/75 mm Hg, HR is 75 beats per minute, temperature is 98.9°F, and RR is 16 breaths per minute. Which of the following tests should be obtained next?
. β-Human chorionic gonadotropin (β-hCG)
. Chlamydia antigen test
. Abdominal radiograph
. Transvaginal ultrasound
. Observe her abdominal pain, if it resolves discharge her with a diagnosis of menstruation
131) For which of the following patients is an abdominal CT scan contraindicated?
A 52-year-old man with abdominal pain after blunt trauma, negative focused assessment with sonography for trauma (FAST) examination, BP 125/78 mm Hg, and HR 109 beats per minute
. A 22-year-old woman with RLQ pain, negative β-hCG, temperature 100.6 F
A 70-year-old man with abdominal pain, an 11-cm pulsatile mass in the epigastrium, BP of 70/50 mm Hg, and HR of 110 beats per minute
. A 45-year-old man with abdominal pain, temperature 100.5 F, WBC 11,200/μL, BP 110/70 mm Hg, HR 110 beats per minute, and lipase 250 IU
. A 65-year-old woman with right flank pain that radiates to her groin, microhematuria, BP 165/85 mm Hg, and HR 105 beats per minute
132) A 59-year-old man presents for his routine colonoscopy and during his visit he has numerous large adenomas removed from his colon. Which of the following is the most effective strategy for follow-up of this patient?
Repeat colonoscopy in 3 years
Elective colectomy
Sigmoidoscopy in 10 years
Repeat colonoscopy in 10 years
Urgent colectomy
133) A 58-year-old white man complains of intermittent rectal bleeding and, at the time of colonoscopy, is found to have internal hemorrhoids and the lesion shown at the splenic flexure. Pathology shows tubulovillous changes. Repeat colonos
 copy should be recommended at what interval?
copy should be recommended at what interval?
 copy should be recommended at what interval?
copy should be recommended at what interval?. In 1 year
. In 1 to 2 months
. In 10 years
. In 3 years
. Repeat colonoscopy is not necessary
134) A 68-year-old man presents to the ED 4 hours after an upper endoscopy was performed for 5 months of progressive dysphagia. During the procedure, a 1-cm ulcerated lesion was found and biopsied. Now, the patient complains of severe neck and chest pain. His vitals are as follows: BP 135/80 mm Hg, HR 123 beats per minute, RR 26 breaths per minute, and temperature 101°F. On physical examination, he appears diaphoretic and in moderate distress with crepitus in the neck and a crunching sound over the heart. You obtain an electrocardiogram (ECG), which is notable for sinus tachycardia. After obtaining a surgical consult, which of the following is the next best step in management?
Perform an immediate bronchoscopy
. Give aspirin 325 mg and obtain a cardiology consult for possible cardiac catheterization
. Repeat the endoscopy to evaluate the biopsy site
. Perform an immediate thoracotomy
. Order an immediate esophagram with water-soluble agent
135) A 24-year-old man woke up from sleep 1 hour ago with severe pain in his right testicle. He states that he is sexually active with multiple partners. On examination, the right scrotum is swollen, tender, and firm. You cannot elicit a cremasteric reflex. His BP is 145/75 mm Hg, HR is 103 beats per minute, RR is 14 breaths per minute, temperature is 98.9°F, and oxygen saturation is 99% on room air. Which of the following is the most appropriate next step in management?
. Swab his urethra, send a culture for gonorrhea and Chlamydia, and treat if positive
. Administer one dose of ceftriaxone and doxycycline for 10 days and have him follow-up with a urologist
. Treat the patient for epididymitis and have him return if symptoms persist
. Send a urinalysis and treat for a urinary tract infection (UTI) if positive
. Order a statim (STAT) color Doppler ultrasound and urologic consultation
136) A 59-year-old man presents to the ED complaining of vomiting and sharp abdominal pain in the epigastric area that began abruptly this afternoon. He describes feeling nauseated and has no appetite. Laboratory results reveal WBC 18,000/μL, hematocrit 48%, platelets 110/μL, AST 275 U/L, ALT 125 U/L, alkaline phosphatase 75 U/L, amylase 1150 U/L, lipase 1450 IU, LDH 400 U/L, sodium 135 mEq/L, potassium 3.5 mEq/L, chloride 110 mEq/L, bicarbonate 20 mEq/L, BUN 20 mg/dL, creatinine 1.5 mg/dL, and glucose 250 mg/dL. Which of the following laboratory results correlate with the poorest prognosis?
. Lipase 1250, LDH 400, bicarbonate 20
. WBC 18,000, LDH 400, glucose 250
. Amylase 950, lipase 1250, LDH 400
. Lipase 1250, creatinine 1.5, potassium 3.5
. WBC 18,000, amylase 950, lipase 1250
137) A 27-year-old man is seen in the ED for a leak around a surgical G-tube that was placed 2 weeks ago and has been used for enteral feeding for 1 week. Inspection reveals the tube is pulled out from the stoma, but is still in the cutaneous tissue. The abdomen is soft and nondistended and there are no signs of skin infection. Which of the following is the most appropriate next step in management?
. Insert a Foley catheter into the tract and aspirate. If gastric contents are aspirated the tube can be used for feeding
. Insert a Foley catheter into the tract, instill water-soluble contrast, and obtain an abdominal radiograph prior to using for feeding
. Remove the tube and immediately obtain a CT scan of the abdomen
. Remove the tube and admit the patient for observation
. Return to the OR for closure of gastrotomy and placement of a new tube
138) A 23-year-old woman presents with weight loss and chronic diarrhea. She appears unwell and cachectic. Routine laboratory tests reveal a low hemoglobin level and an increased international normalized ratio (INR) even though she is not taking any anticoagulants. The liver enzymes are normal, but the albumin and calcium levels are low, suggesting generalized malnutrition. Which of the following is the most appropriate initial diagnostic test for malabsorption?
. Schilling test
. Xylose absorption
. x-ray studies
. Stool fat quantitation
. Small intestinal biopsy
139) A 50-year-old man with a history of alcohol and tobacco abuse has complained of difficulty swallowing solid food for the past 2 months. More recently, swallowing fluids has also become a problem. He has noted black, tarry stools on occasion. The patient has lost 10 lb. Which of the following statements is correct?
. Barium contrast esophagram will likely establish a diagnosis
. A CT scan of the abdomen and pelvis is the best next test
. The patient has achalasia
. The most likely diagnosis is peptic ulcer disease
. Herpes simplex virus infection of the esophagus is likely
140) A 48-year-old woman presents with a change in bowel habit and 10-lb weight loss over the past 2 months despite preservation of appetite. She notices increased abdominal gas, particularly after fatty meals. The stools are malodorous and occur 2 to 3 times per day; no rectal bleeding is noticed. The symptoms are less prominent when she follows a clear liquid diet. Which of the following is the most likely histological abnormality associated with this patient’s symptoms?
. Villous atrophy and increased lymphocytes in the lamina propria on small bowel biopsy
. Signet ring cells on gastric biopsy
. Small, curved gram-negative bacteria in areas of intestinal metaplasia on gastric biopsy
. Mucosal inflammation and crypt abscesses on sigmoidoscopy
. Periportal inflammation on liver biopsy
141) A 62-year-old woman is transferred to the medical service with an appendiceal mass serendipitously picked up at the edge of an x-ray taken of a broken femur in the emergency department. Otherwise, the patient has no significant past medical history and no current symptoms. Which of the following studies is most likely to be useful?
Immediate ECG
Arterial blood gas
MRI of the chest and abdomen
CT of the chest and abdomen
Room air oxygen saturation
142) A 60-year-old woman complains of fever and constant left lower quadrant pain of 2 days duration. She has not had vomiting or rectal bleeding. She has a history of hypertension but is otherwise healthy. She has never had similar abdominal pain, and has had no previous surgeries. Her only regular medication is lisinopril. On examination blood pressure is 150/80, pulse 110, and temperature 38.9°C (102°F). She has normal bowel sounds and left lower quadrant abdominal tenderness with rebound. A complete blood count reveals WBC = 28,000. Serum electrolytes, BUN, creatinine and liver function tests are normal. What is the next best step in evaluating this patient’s problem?
. Exploratory laparotomy
. Colonoscopy
. Ultrasound of the abdomen
. Barium enema
. CT scan of the abdomen and pelvis
143) A 37-year-old woman presents for evaluation of abnormal liver chemistries. She has long-standing obesity (current BMI 38) and has previously taken anorectic medications but not for the past several years. She takes no other medications and has not used parenteral drugs or had high risk sexual exposure. On examination, her liver span is 13 cm; she has no spider angiomas or splenomegaly. Several sets of liver enzymes have shown transaminases two to three times normal. Bilirubin and alkaline phosphatase are normal. Hepatitis B surface antigen and hepatitis C antibody are normal, as are serum iron and total iron-binding capacity. Which of the following is the likely pathology on liver biopsy?
Portal triaditis with piecemeal necrosis
. Macrovesicular fatty liver
. Cirrhosis
. Microvesicular fatty liver
. Copper deposition
144) A 55-year-old man from China is known to have chronic liver disease, secondary to hepatitis B infection. He has recently felt unwell, and his hemoglobin level has increased from 130 g/L, 1 year ago, to 195 g/L. Which of the following is the most appropriate initial diagnostic test?
. alpha-fetoprotein (AFP)
. Alkaline phosphatase
. Alanine transaminase (ALT)
. Aspartate transaminase (AST)
. Unconjugated bilirubin
145) A 42-year-old previously well woman presents with pruritus. She is not taking any medications, and only drinks alcohol on a social basis. Her physical examination is entirely normal with no signs of chronic liver disease or jaundice. Laboratory evaluation reveals an alkaline phosphatase level of three times normal, and an ultrasound of the liver and gallbladder is normal. Which of the following is the most appropriate next step in diagnosis?
. Antinuclear antibodies
. INR or prothrombin time
. Abdominal ultrasound
. Protein immunoelectrophoresis
. Antimitochondrial antibodies
146) A 22-year-old man with inflammatory bowel disease is noted to have a “string sign” in the ileal area on barium enema. In which of the following conditions is this sign most often seen?

. In the stenotic or nonstenotic phase of the disease
. In the stenotic phase only
. With gastric involvement
. As a rigid, nondistensible phenomenon
. With rectal involvement
147) A 55-year-old white man with a 20-year history of gastroesophageal reflux visits the clinic for worsening reflux symptoms over the past 18 months. His last visit was 7 years ago and he claims to be otherwise in good health. He has been compliant with his antireflux medications, including an H2-blocker and a proton pump inhibitor. Which of the following is the best next step in management?
Double the dose of his proton pumps inhibitor and schedule him for follow-up in 4 weeks
Double the dose of his H2-blocker and schedule him for follow-up in 4 weeks
Schedule him for elective esophagectomy
Perform an esophagoscopy
Schedule him for emergent Nissen fundoplication
148) A 65-year-old man presents to his physician complaining of difficulty swallowing, occasional chest pain, and regurgitation of food. Over the past 2 months he has lost about 7 kg (15 lb). Results of a barium swallow study are shown in the image. What test should be performed to look for possible causes of his condition?
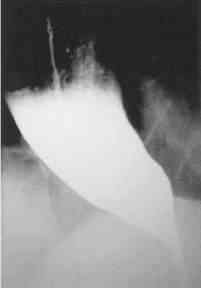
vvvv

Esophageal manometry
24-hour pH monitoring
Upper endoscopy
Serum gastrin level measurement
Urease breath test
149) A 63-year-old man with a long history of alcohol abuse presents with ascites. He is experiencing mild abdominal discomfort and nausea. Examination reveals tense ascites and generalized tenderness but no rigidity. A diagnostic paracentesis of the fluid is performed. Which of the following ascitic fluid results is most likely to suggest an uncomplicated ascites due to portal hypertension from cirrhosis?
. protein >25 g/L
. hemorrhage
. Serum to ascites albumin gradient >1.1 g/dL
. Bilirubin level twice that of serum
. More than 1000 white cells/mm3
150) A 21-year-old man presents to the clinic feeling tired and generally unwell. He has fallen several times over the past month and has developed a slight tremor in both hands. Physical examination is significant for scleral icterus, ankle edema, and a distended and tense abdomen. Laboratory studies show: Hemoglobin: 7 g/dL, Reticulocyte count: 7% Total bilirubin: 3.1 mg/dL, Aspartate aminotransferase: 84 U/L Alanine aminotransferase: 92 U/L Ceruloplasmin: 5 mg/dL (normal: 20–45 mg/dL). Results of a Coombs’ test are negative. Which of the following is an appropriate preventive management step after chelation therapy?
Upper endoscopy
Schilling test
Colonoscopy
ECG
Blood protein electrophoresis
151) A 35-year-old alcoholic man is admitted with nausea, vomiting, and abdominal pain that radiates to the back. He has had several previous episodes of pancreatitis presenting with the same symptoms. Which of the following laboratory values suggests a poor prognosis in this patient?
. Leukocytosis of 20,000/μm
. Elevated serum lipase
. Diastolic blood pressure greater than 90 mm Hg
. Elevated serum amylase
. Heart rate of 100 beats/minute
152) A 60-year-old woman with depression and poorly controlled type 2 diabetes mellitus complains of episodic vomiting over the last three months. She has constant nausea and early satiety. She vomits once or twice almost every day. In addition, she reports several months of mild abdominal discomfort that is localized to the upper abdomen and that sometimes awakens her at night. She has lost 5 lb of weight. Her diabetes has been poorly controlled (glycosylated hemoglobin recently was 9.5). Current medications are glyburide, metformin, and amitriptyline. Her physical examination is normal except for mild abdominal distention and evidence of a peripheral sensory neuropathy. Complete blood count, serum electrolytes, BUN, creatinine, and liver function tests are all normal. Gallbladder sonogram is negative for gallstones. Upper GI series and CT scan of the abdomen are normal. What is the best next step in the evaluation of this patient’s symptoms?
. Colonoscopy
. Barium esophagram
. Liver biopsy
. Scintigraphic gastric emptying study
. Small bowel biopsy
153) A 63-year-old man with diabetes is called by his primary care physician because of abnormal liver function test results, as follows: Aspartate aminotransferase: 85 U/L Alanine aminotransferase: 102 U/L Alkaline phosphatases: 180 U/L Total bilirubin: 1.9 mg/dL. On physical examination his liver is enlarged. His skin has a slightly yellow hue, especially on his face. The review of symptoms is significant for some weight loss, weakness, arthritis in his hands, and inability to achieve an erection. What test would generate the most likely diagnosis and should be done first?
Fasting transferrin saturation levels
Blood smear
Liver biopsy
CT scan of the abdomen
Endoscopic retrograde cholangiopancreatography
154) A 28-year-old man presents to the ED complaining of constant vague, diffuse epigastric pain. He describes having a poor appetite and feeling nauseated ever since eating sushi last night. His BP is 125/75 mm Hg, HR is 96 beats per minute, temperature is 100.5°F, and his RR is 16 breaths per minute. On examination, his abdomen is soft and moderately tender in the right lower quadrant (RLQ). Laboratory results reveal a WBC of 12,000/ μL. Urinalysis shows 1+ leukocyte esterase. The patient is convinced that this is food poisoning from the sushi and asks for some antacid. Which of the following is the most appropriate next step in management?
. Send the patient for an abdominal ultrasound
. Order a plain radiograph to look for dilated bowel loops
. Order an abdominal CT scan
. Administer 40 cc of Maalox and observe for 1 hour
. Discharge the patient home with ciprofloxacin
155) A 23-year-old woman presents to the ED in moderate pain in her left lower quadrant (LLQ). She states that the pain began suddenly and is associated with nausea and vomiting. She had a bout of diarrhea yesterday. This is the second time this month that she experienced pain in this location, however, never with this severity. Her BP is 120/75 mm Hg, HR is 101 beats per minute, temperature is 99.5°F, and RR is 18 breaths per minute. She has a tender LLQ on abdominal examination and a tender adnexa on pelvic examination. Which of the following is the most appropriate diagnostic test for the patient?
. X-ray
. CT scan
. Doppler ultrasound
. MRI
. Laparoscopy
156) A 75-year-old woman comes to the emergency department with complaints of nausea and nonbilious, nonbloody vomiting over the past 4 days. The patient reports that both the nausea and vomiting come in “waves”; that is, several hours will pass during which she feels well before the vomiting suddenly recurs. A detailed history reveals that the woman was told several months ago that she “has stones in her gall-bladder,” but she has been too frightened to undergo surgery. She has not had a bowel movement for 7 days. Her temperature is 38.4°C (101.1°F) and the abdomen is distended with high-pitched bowel sounds. Which of the following is the most appropriate initial test for a patient with suspected gallstone ileus?
Endoscopic retrograde cholangiopancreatography
Abdominal ultrasound
Hepatic iminodiacetic acid scan
Diagnostic laparoscopy
Plain X-ray of the abdomen
157) An 82-year-old woman is in the surgical intensive care unit after a carotid endarterectomy. She has been taking clindamycin and ciprofloxacin for the past 13 days. On postoperative day 2 the patient is febrile and tachycardic with a high WBC count and a low RBC count. She is also noted to be dehydrated and hypotensive. On physical examination she is distended and has abdominal tenderness with rebound and guarding. Barium enema reveals colonic dilatation of 8 cm. Stool is sent for Gram stain and analysis for fecal leukocytes, fecal occult blood, and Clostridium difficile toxin. Which of the following is most likely present in the stool sample?
Gram-positive cocci
Clostridium difficile toxin
No fecal occult blood
Gram-negative rods
Spores and hyphae
158) A 51-year-old man presents to the ED complaining of epigastric pain that radiates to his back. He states that he drinks six packs of beer daily. You suspect he has pancreatitis. His BP is 135/75 mm Hg, HR is 90 beats per minute, temperature is 100.1°F, and his RR is 17 breaths per minute. Laboratory results reveal WBC 13,000/μL, hematocrit 48%, platelets 110/μL, amylase 1150 U/L, lipase 1450 IU, lactate dehydrogenase (LDH) 150 U/L, sodium 135 mEq/L, potassium 3.5 mEq/L, chloride 105 mEq/L, bicarbonate 23 mEq/L, BUN 15 mg/dL, creatinine 1.1 mg/dL, and glucose 125 mg/dL. Which of the following laboratory values are most specific for pancreatitis?
. Elevated lipase
. Elevated amylase
. Elevated LDH
. Hyperglycemia
. Leukocytosis
159) A 25-year-old G3P1011 presents to the ED with a 6-hour history of worsening lower abdominal pain, mostly in the RLQ. She also noticed some vaginal spotting this morning. She is nauseated, but did not vomit. Her last menstrual period was 2 months ago, but her cycles are irregular. She is sexually active and has a history of pelvic inflammatory disease. Her BP is 120/75 mm Hg, HR is 95 beats per minute, temperature is 99.2°F, and RR is 16 breaths per minute. Her abdomen is tender in the RLQ. Pelvic examination reveals right adnexal tenderness. Her WBC count is slightly elevated and her β-hCG is positive. After establishing IV access, which of the following is the most appropriate next step in management?
. Perform a transvaginal ultrasound
Call the OR to prepare for laparoscopy
. Order a urinalysis
. Order an emergent CT scan of the abdomen
. Swab her cervix and treat for gonorrhea and Chlamydia
160) A 40-year-old Asian woman presents to the emergency department complaining of intermittent epigastric pain. The pain is severe, lasts for a few hours, and is sometimes accompanied by nausea and vomiting. Her bowel movements have been normal. Her temperature is 38.3°C (100.9°F), pulse is 100/min, blood pressure is 150/80 mm Hg, and respiratory rate is 22/min. Physical examination reveals moderate obesity and mildly icteric sclerae. Bowel sounds are normal, with an abrupt halt of inspiration upon palpation of the RUQ, and guarding is noted. Laboratory values reveal a WBC count of 13,000/mm³, total bilirubin of 3.3 mg/dL, and normal liver enzymes and alkaline phosphatase levels. Which of the following is the first diagnostic imaging study that should be performed?
Hepatobiliary iminodiacetic acid scan
CT
MRI
Flat and upright plain x-rays of the abdomen
Ultrasound of the RUQ
161) A 45-year-old white man is brought to the emergency department by ambulance. He is waving wildly, trying to hit the “flying bats” that are all around him. He is very agitated and smells strongly of alcohol. The ambulance crew said they found the patient bleeding from the mouth outside a bar. They could not find any laceration on his mouth or lips and believe that the bleeding is internal. The patient screams that he will not stand for this maltreatment any longer and tries to stand up, at which point he begins to vomit. Blood pours out of his mouth, and the patient says, “Here we go again.” The ambulance crew tells the physician that there was also a lot of vomit at the bar where he was found. The physician is able to subdue the patient to obtain his vital signs. His blood pressure is 118/78 mm Hg, pulse is 98/ min, respiratory rate is 22/min, and temperature is 37.2°C (98.9°F). The physician is unable to obtain a history on the patient or con- tact any relatives or friends. No signs of obvious trauma are observed. Which of the following is the best next step in diagnosis?
Endoscopy
Barium swallow
Esophageal manometry
Electrocardiogram
X-ray of the chest
162) A 53-year-old man presents to the emergency department with severe epigastric abdominal pain. His temperature is 37.2°C, blood pressure 110/70 mm Hg, pulse 110/min, and respirations 20/min. Examination of the heart and lungs is normal, and his abdomen is tender in the epigastric region. His white count is 15,000/mL and amylase is 450 U/L (25–125 U/L). Which of the following laboratory abnormalities is also most likely to be present?
. hypercholesterolemia
. hypoglycemia
. hypercalcemia
. hyperglycemia
. hypercarbia
163) A 34-year-old white woman is treated for a UTI with amoxicillin. Initially she improves, but 5 days after beginning treatment, she develops recurrent fever, abdominal bloating, and diarrhea with six to eight loose stools per day. What is the best diagnostic test to confirm your diagnosis?
. Isolation of C difficile in stool culture
. Identification of Clostridium difficile toxin in the stool
. Detection of IgG antibodies against C difficile in the serum
. Stool positive for white blood cells (fecal leukocytes)
. Visualization of clue cells on microscopic examination of stool
164) Her son brings a 50-year-old female to the emergency room because she is confused and sweating a lot. She does not have any medical problems, except hypertension for which she takes hydrochlorothiazide. She is not taking any other medication. He tells you that his mother complained of profound weakness, and inability to stand, because of lightheadedness 3 hours ago. On examination, the patient is drowsy, confused, and appears sick. Her temperature 36.8°C (98.2° F) BP 153/83mm Hg PR 128/min. Her clothes are damp from perspiration. No other abnormalities are noted on physical examination. Initial laboratory studies show: Sodium 144 mEq/L, Potassium 3.6 mEq/L, Bicarbonate 26 mEq/L, Blood urea nitrogen: 12 mg/dl, Creatinine 0.6 mg/dl. You order a few more tests and on the basis of which you diagnose insulinoma. What set of following results leads to this diagnosis? (Serum Glucose, Insulin, C-Protein
. Decreased, Increased, Increased
. Increased, Decreased, Increased
. Decreased, Increased, Decreased
. Increased, Increased, Increased
. Normal,Normal,Normal
165) A 65-year-old male is brought by his wife to the emergency department because of a very high fever. He has also had a cough productive of greenish, nonbloody sputum for the past two days. He is diabetic, and had pneumonia 3 months ago. He has been smoking one pack of cigarettes daily for 27 years. His temperature is 38.4° C (101.2°F), blood pressure is 118/74 mm Hg, pulse is 98/min, and respirations are 24/min. Physical examination reveals cervical lymphadenopathy, and some scattered rales are heard on the right lung base. Chest-x ray shows a right lower lobe infiltrate. Laboratory studies reveal: Hb 12.6 gm/dL, WBC 40,000/cmm, Platelets 190,000/cmm. Peripheral smear: Segmented neutrophils 10%, Bands 4%, Lymphocytes 85%, Monocytes 1%. Some variant lymphocytes, and smudge cells are seen on the peripheral smear. What is the most appropriate way to confirm the diagnosis of this patient?
. Lymph node biopsy
. Epstein Barr virus serology
. Cytogenetic analysis
. Bone marrow biopsy
. Lung biopsy
166) A father brings his 7-year-old boy to the office because "his eyes are getting yellow". The boy has no other complaints. However, he is feeling tired and does not feel like going to the next Steelers game. There is a history of diabetes and lung cancer in the family. His vitals are stable, but he has pallor, jaundice, and splenomegaly. His labs revel: WBC 10,000/cmm, Hemoglobin 10 gm/dl, Hematocrit 28%, RBC count 3.5 million, Platelets 240,000/cmm, Reticulocyte count 4%. RBC indices were as follows:MCV 90 fl, MCHC 38%, MCH 28 pg. Peripheral smear revealed anisocytosis, some spherocytosis, and polychromatophilia. Coomb's test was negative. LFTs showed: Albumin 5.2 g/dl, AST 47U/L, ALT 52U/L, Alkaline phosphatase 120 U/L, Total bilirubin 3.0 mg/dl, Direct bilirubin 0.2 mg/dl. What is the next step?
. Osmotic fragility test
. Bone marrow biopsy
. Sugar water test
. Hemoglobin electrophoresis
. Serum B 12 level
{"name":"DES 3 ep 7", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"67) A 27-year-old Caucasian male is diagnosed with medullary thyroid carcinoma that is non-resectable. His past medical history is insignificant. He does not smoke or consume alcohol. His family history is significant for thyroid cancer and pheochromocytoma in his father. Which of the following tests could have been most effective in preventing this patient's non-resectable cancer?, 68) A 35-year-old Caucasian male presents with weakness, fatigue, and weight loss over the past year. He is anorexic and has lost interest in all his activities. His temperature is 37.1°C (99°F), pulse is 84\/min, blood pressure is 101\/72 mmHg, and respirations are 14\/min. On physical examination, he does not appear to be in acute distress. Dark brown pigmentation is present on his skin creases and oral cavity mucous membranes. Laboratory studies show: Hemoglobin 10.3 g\/dL, WBC count 3,000\/micro-L, Neutrophils 60%, Monocytes 5%,Eosinophils 10%, Basophils 1%, Lymphocytes 24%, Serum sodium 130 meq\/L, Serum potassium 5.5 meq\/L. Chest x-ray and PPD tests are normal. What is the most appropriate next step in the management of this patient?, 69) A 56-year-old female comes to the office and complains of general malaise and headaches. Her other symptoms are episodic palpitations, throbbing headaches and diaphoresis. She feels \"very anxious all the time.\" Her past medical history is unremarkable. Her deceased sister had very high blood pressure. Her blood pressure is 230\/110 mmHg and pulse is 110\/min. Initial laboratory studies reveal: WBC 7,000\/cmm, Hb 11.2 g\/L, Platelets 325,000\/cmm, Calcium 11.9 mg\/dl. What is the best next step in the evaluation of this patient?","img":"https://www.quiz-maker.com/3012/images/ogquiz.png"}
More Quizzes
Franchise FastLane Quiz
10515
Doraemon Fan Quiz
14710
Multiplication
940
Which Vape Suits You Best
940
Babysitting - Check Your Skills Online (Free)
201017983
Social Media Marketing - Free Online Skills Check
201019242
Graph Transformations - Parent Functions (Free)
201018905
Free Relationship Test - How Strong Is Your Bond?
201018742
Civil War - Test Your U.S. History Knowledge
201018428
Which Katseye Member Are You? Free KISS Personality
201018276
TOEIC Part 5 Practice Questions - Free Online
201021905
Which Decade Are You? with Instant Results
201018987