
Vignette's
Medical Differential Diagnosis Quiz
Test your knowledge with this comprehensive quiz on differential diagnoses, clinical findings, and follow-up procedures for various medical conditions. Designed for healthcare professionals and students, this quiz covers a diverse range of clinical scenarios.
- 102 challenging questions
- Multiple choice format with checkboxes for detailed responses
- Focus on real-world clinical cases

Male 62 years old. CC: Patient presents with LBP and initiating urinary streams. He reports polyuria in the middle of the night. Kemps +. Which labs would you expect to be positive?
PSA
Acid Phosphatase
Alkaline Phosphatase
ESR
CRP
Proteinuria
BUN
Biopsy for Reed Sternberg

Male 62 years old. CC: Patient presents with LBP and initiating urinary streams. He reports polyuria in the middle of the night. Kemps +. What are your differential diagnoses?
Paget's
BPH
Osteomyelitis
Multiple Myeloma
Blastic Mets
Hodgkins
Lytic Mets

Male 62 years old. CC: Patient presents with LBP and initiating urinary streams. He reports polyuria in the middle of the night. Kemps +. List the best follow up procedures?
Oncology
Chiropractor
CT of spine
MRI of prostate
Internist
Endocrinologist
Radionucleotide scan

Male 23 years old. Football player presents with nausea after being hit from behind. He reports feeling dizzy when he is stretching his neck. What are your DDx?
Dens fracture
Hangmans fracture
Os odontodium
Teardrop fracture
Whiplash
Facet Dislocation
Jefferson Burst Fracture
Brown Sequard

Male 23 years old. Football player presents with nausea after being hit from behind. He reports feeling dizzy when he is stretching his neck. What are the findings associated with this condition?
Isthmic spondylolisthesis
Spina Bifida
Congenital block vertebrae
Occipitalization
Atlas hyperplasia
Hypoplastic scapula
Agenesis of atlas
Agenesis of scapula

Male 23 years old. Football player presents with nausea after being hit from behind. He reports feeling dizzy when he is stretching his neck. What other tests are likely to be performed?
Flexion and Extension views
Orthopedic evaluation
Neurologic evaluation
Bone scan
CT scan

Female age 24. Patient presents with headaches and neck pain. She tells you that she has muscle spasms around the suboccipital region. What are your DDx?
Multiple myeloma
Lytic mets of occiput
Agenesis of posterior arch
Occipitalization
Hypertrophy of anterior tubercle

Female age 24. Patient presents with headaches and neck pain. She tells you that she has muscle spasms around the suboccipital region. What else can you see with this condition?
Basilar impression
Spina bifida
Anterior rachischisis
Hemivertebrae
Atlantoaxial instability
Spondylolisthesis
Visceral compromise

Female age 24. Patient presents with headaches and neck pain. She tells you that she has muscle spasms around the suboccipital region. List the best follow up steps.
Flexion and extension views
Low force cervical adjustment
Surgical consult
Traction
Neurological evaluation
Cervical collar
NSAIDs
Avoid adjusting cervical region
Female age 32. Patient presents with bilateral leg weakness, vertigo, and diplopia. Patient reports recently developing a bladder problem. Babinski +. SLR -. Laseague -. Lhermittes +. Normal ROM. List the best follow up procedures?
Cervical spine x-ray
MRI of brain
Lumbar spine x-ray
Refer to neurologist
Electrodiagnosis
Oncologist
Immunoelectrophoresis
Urinary toxicology
Female age 32. Patient presents with bilateral leg weakness, vertigo, and diplopia. Patient reports recently developing a bladder problem. Babinski +. SLR -. Laseague -. Lhermittes +. Normal ROM. List the most likely associated signs.
Visual disturbance
Diplopia
Scissor gait
Festinating gait
+3 DTR
Cortical deficit
Fasciculations
+ Plantar reflex
Female age 32. Patient presents with bilateral leg weakness, vertigo, and diplopia. Patient reports recently developing a bladder problem. Babinski +. SLR -. Laseague -. Lhermittes +. Normal ROM. List the sequelae.
Dementia
Speech impairment
Chorea
Spastic paraplegia
Mask like faces
Clonus
Tonic clonic seizures
Cognitive impairment

Male age 50. Patient presents with hip pain that is a 6/10. Hibbs +. Anvil +. List the radiographic signs that you expect to see.
Ground glass
Osteolytic lesion
Joint destruction
Osteopenia
Metaphyseal lesion
Expansile lesion
Cortical thickening
Sclerosis

Male age 50. Patient presents with hip pain that is a 6/10. Hibbs +. Anvil +. What is the most likely diagnosis?
GCT
Blastic lesion
Primary neoplasm
Paget's
Fibrous dysplasia
Hematopoetic disease
Blastic Mets
Multiple myeloma

Male age 50. Patient presents with hip pain that is a 6/10. Hibbs +. Anvil +. List the possible sequelae.
Anemia
Prostate cancer
Urinary incontinence
Increase in occurrence of infection
Unexplained weight loss
Skin deformities
Increase in PSA
Increase in acid phosphatase

Male age 28. Patient presents with asthma and reports a history of corticosteroid use. Lateral flexion is limited. List associated possibilities with this condition.
Functional scoliosis
Structural scoliosis
Butterfly vertebrae
Blocked vertebrae
Hemivertebrae
Klippel Feil
Omovertebral bone
Primary defect of growth plate

Male age 28. Patient presents with asthma and reports a history of corticosteroid use. Lateral flexion is limited. List the appropriate follow up steps.
Surgical consult
Extension rehab
Strengthen flexors
William's exercises
Milwaukee brace
Adjust
Spinal stretching exercises
Defer adjusting

Male age 28. Patient presents with asthma and reports a history of corticosteroid use. Lateral flexion is limited. What is the likely presentation of the progression of this condition?
Renal disease
Cardiac involvement
DJD
Bone pain
Progressing scoliosis
Neurological defects
Vascular problems
Digestive disorders
Male age 50. Patient presents with right shoulder pain. He reports recently hitting his head on a shelf. Patient played football in college and has a history of skin cancer on his forehead.: Shoulder depression +, Decrease in ROM in cervical spine, Normal reflexes, Babinski +, Weakness in legs, Weak when asked to toe walk. List the best DDx.
IVF encroachment
Canal stenosis
Adhesive nerve tumor
Brown Sequard
Right lateral disc protrusion
Central disc protrusion
Upper motor neuron lesion
Left lateral disc protrusion
Male age 50. Patient presents with right shoulder pain. He reports recently hitting his head on a shelf. Patient played football in college and has a history of skin cancer on his forehead.: Shoulder depression +, Decrease in ROM in cervical spine, Normal reflexes, Babinski +, Weakness in legs, Weak when asked to toe walk. List the symptoms associated with this condition.
Weak wrist extensors
Decrease of sensation in thumb
Clonus
Hyperspasticity
Bowel and bladder incontinence
Cervical rib
Hyperreflexia in lower extremity
Decrease in sensation
Male age 50. Patient presents with right shoulder pain. He reports recently hitting his head on a shelf. Patient played football in college and has a history of skin cancer on his forehead.: Shoulder depression +, Decrease in ROM in cervical spine, Normal reflexes, Babinski +, Weakness in legs, Weak when asked to toe walk. List the complications associated with this condition.
Permanent loss of bowel control
Progressive peripheral neuropathy
Parasthesia
Right hemiplegia
Weakness in lower extremity
Dermatological disorder of pain
Paraplegia
Inability to heel and toe walk

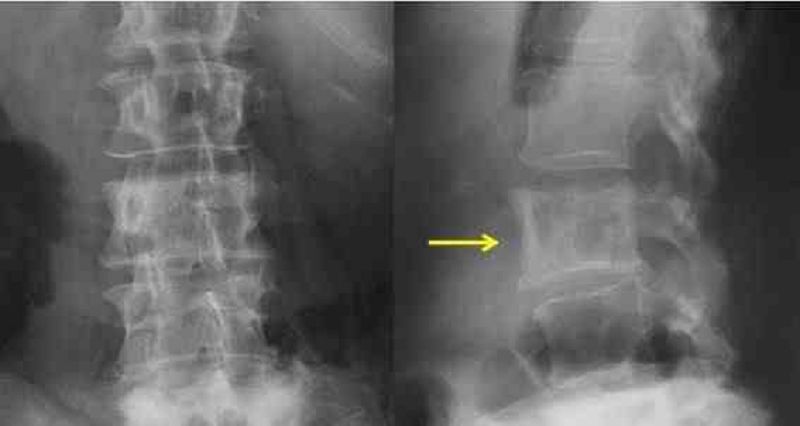
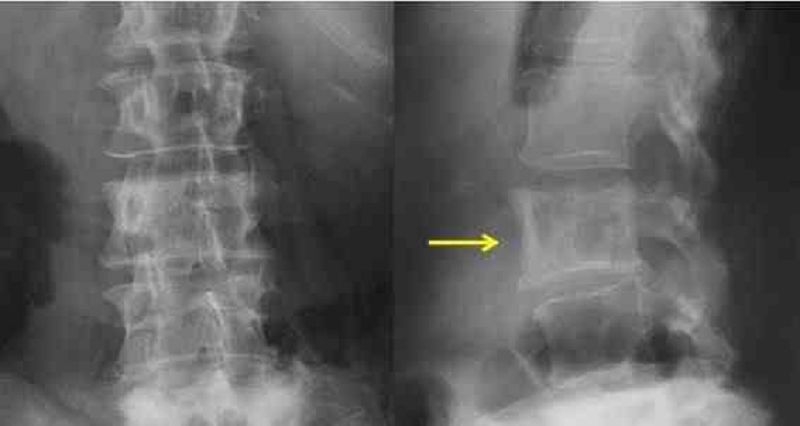
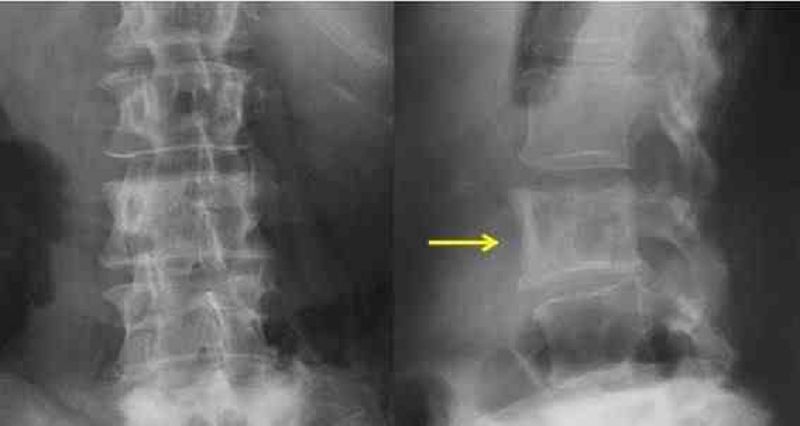
Female age 82. Patient presents with sudden onset of low back pain while gardening. Patient reports feeling a sharp pain with movements and feels better with ice. Pain is rated 8/10. No orthos performed due to pain. List the radiographic signs you expect to see.
Ivory white vertebral body
Synostosis
DDD
Fusiform shape
Atherosclerotic plaquing
Dilation of abdominal aorta
Osteopenia
Anterior wedge deformity

Female age 82. Patient presents with sudden onset of low back pain while gardening. Patient reports feeling a sharp pain with movements and feels better with ice. Pain is rated 8/10. No orthos performed due to pain. What tests would be used to diagnose this condition?
DEXA
MRI
CT
PET
CBC
Angiogram
Abdominal ultrasound
Alkaline phosphatase

Female age 82. Patient presents with sudden onset of low back pain while gardening. Patient reports feeling a sharp pain with movements and feels better with ice. Pain is rated 8/10. No orthos performed due to pain. List the treatments of this condition.
Defer adjusting
Prescribe NSAIDs
Fit for elastic lumbar support
Adjust lumbar
Oncologist
Vascular surgeon
Surgical consult
Limit certain physical activities
Male age 30. Patient presents with LBP. He reports an insidious onset that has gotten progressively worse over the past 3 months. He has pain over his calcaneal tendon, red eyes, and blurred vision. List the DDx.
Reiter's
Poly arthritis
Enteropathic arthritis
Sero +
Psoriatic arthritis
Rheumatoid arthritis
Reactive arthritis
Metabolic arthritis
Male age 30. Patient presents with LBP. He reports an insidious onset that has gotten progressively worse over the past 3 months. He has pain over his calcaneal tendon, red eyes, and blurred vision. List the follow up tests to be performed
HLA B27
RA Latex
ESR
Lewin's supine
Anti DNA antibodies
Chest expansion
Chest evaluation
Chlamydia Culture
Male age 30. Patient presents with LBP. He reports an insidious onset that has gotten progressively worse over the past 3 months. He has pain over his calcaneal tendon, red eyes, and blurred vision. What are the least likely sequelae?
Difficulty breathing
Knee arthritis
Compression fracture
Stomatitis
Postural deformity
Genital lesion
Anterior uveitis
Red and painful nodules on the hands and feet.

Male age 24. Mechanic presents with loss of grip strength. The patient reported having swollen fingers that previous hurt but the pain went away. ROM in hands are decreased, notable swelling of the tissue in his fingers. List the DDx. (Choose 2)
Ollier's
Fibrous dysplasia
Hereditary multiple exostosis
Multiple enchondromas
Scleroderma
Gardner's syndrome

Male age 24. Mechanic presents with loss of grip strength. The patient reported having swollen fingers that previous hurt but the pain went away. ROM in hands are decreased, notable swelling of the tissue in his fingers. What else could be associated with this condition?
CREST sign
Sessile appearance
Geographic lesion
Blister of bone appearance
Periostitis
Cortical thinning
Subchondral cysts
Expansile lesion

Male age 24. Mechanic presents with loss of grip strength. The patient reported having swollen fingers that previous hurt but the pain went away. ROM in hands are decreased, notable swelling of the tissue in his fingers. What are the possible sequelae?
Pathological fracture
Malignant degeneration
Permanent deformity
Reversal of lesion
Hypertrophy of sclera
Self resolving
Skull enlargement
Spinal deformity
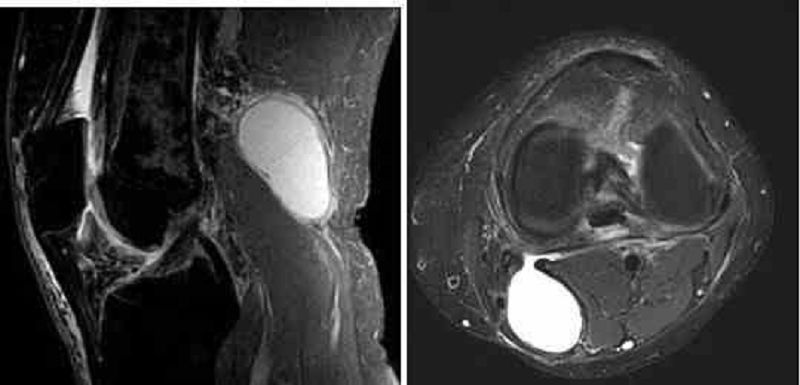
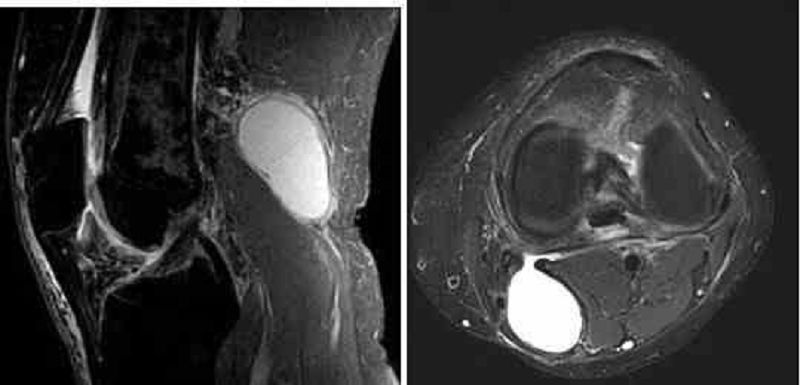
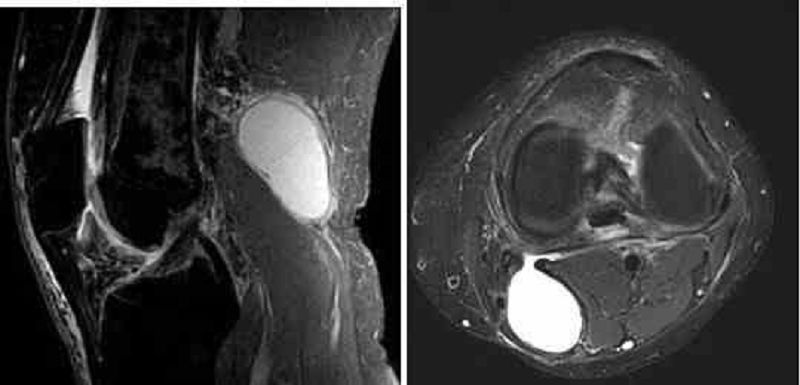
Female age 30. Patient presents with an insidious onset of right knee pain around her popliteal fossa region. The patient reports feeling pain and swelling of the region. She does not recall any trauma or injury. Pain is a 5 out of 10 on the pain scale. Notable swelling, Redness of the metacarpal joints bilaterally, unable to flex the knee past 90˚ due to pain. What are the possible causes of this patients pain?
Lateral meniscus tear
Baker's cyst
Housemaids knee
Jumper's knee
RA
Popliteal bursitis
Runner's knee
Female age 30. Patient presents with an insidious onset of right knee pain around her popliteal fossa region. The patient reports feeling pain and swelling of the region. She does not recall any trauma or injury. Pain is a 5 out of 10 on the pain scale. Notable swelling, Redness of the metacarpal joints bilaterally, unable to flex the knee past 90˚ due to pain. What are additional findings associated with this condition?
Heberden's nodes
Bilateral sacralitis
Symmetrical joint space narrowing
Gull wing deformity
Calcium deposits in the knee
Haygarth's nodes
Asymmetrical joint space narrowing
Increase in joint pain upon rising
Female age 30. Patient presents with an insidious onset of right knee pain around her popliteal fossa region. The patient reports feeling pain and swelling of the region. She does not recall any trauma or injury. Pain is a 5 out of 10 on the pain scale. Notable swelling, Redness of the metacarpal joints bilaterally, unable to flex the knee past 90˚ due to pain. What tests will confirm this condition?
Hand films
Uric acid
ESR
RA latex
Joint aspiration
Bone scan
Ultrasound
HLA B27
Female age 29. Patient presents with low back pain and fatigue. Fatigue is getting progressively worse over a long period of time. Sensitivity to sunlight is reported. Murphy’s punch +, Decreased ROM of wrist, Rebound + (ulnar deviation of phalanges which can be strengthened with hand on the table, Bechterew’s +, Kemps+, Cellular casts, Alopecia, blood and protein in urine. List the tests that are to be found positive.
Insulin resistance test
Uric acid
Serum glucose
ANA
Amylase
Anti-DNA
Thrombocytopenia
HLA B27
Female age 29. Patient presents with low back pain and fatigue. Fatigue is getting progressively worse over a long period of time. Sensitivity to sunlight is reported. Murphy’s punch +, Decreased ROM of wrist, Rebound + (ulnar deviation of phalanges which can be strengthened with hand on the table, Bechterew’s +, Kemps+, Cellular casts, Alopecia, blood and protein in urine. What other findings are to be seen with this condition?
Malar Rash
Optic nerve solarization
Auspitz Sign
Oral ulcers
Discoid lesions
Silver scales
Pitted nails
Linea nigra
Female age 29. Patient presents with low back pain and fatigue. Fatigue is getting progressively worse over a long period of time. Sensitivity to sunlight is reported. Murphy’s punch +, Decreased ROM of wrist, Rebound + (ulnar deviation of phalanges which can be strengthened with hand on the table, Bechterew’s +, Kemps+, Cellular casts, Alopecia, blood and protein in urine. List the management approaches.
Chiropractic care
Blood transfusion
Diathermy
Traction
Avoid sun
Activities to tolerance
Laser surgery
Oncologist
Female age 17. Swimmer presents with shoulder pain present at 90˚- 120˚ abduction. The pain is rated from a 3 to 5 out of 10 on the pain scale with a gradual onset. Irregular hyper pigmented macules (café au lait spots) on her back that have been there her entire life. Insidious onset, patient does not recall any trauma. Empty can +, Yerguson's -, Speed's -. What are the DDx?
Biceps tendonitis
Biceps instability
Fibrous dysplasia
SLAP lesion
Benign bone tumor
Calcium hydroxapetite deposition
Supraspinatus tendonitis
Calcific tendonitis
Female age 17. Swimmer presents with shoulder pain present at 90˚- 120˚ abduction. The pain is rated from a 3 to 5 out of 10 on the pain scale with a gradual onset. Irregular hyper pigmented macules (café au lait spots) on her back that have been there her entire life. Insidious onset, patient does not recall any trauma. Empty can +, Yerguson's -, Speed's -. List the best management options.
Orthopedist
Oncologist
Radiologist
Brace arm
Exercise to strengthen arm muscles
Chiropractic care for shoulder symptoms only
Cast arm
Monitor condition every 6 months
Female age 17. Swimmer presents with shoulder pain present at 90˚- 120˚ abduction. The pain is rated from a 3 to 5 out of 10 on the pain scale with a gradual onset. Irregular hyper pigmented macules (café au lait spots) on her back that have been there her entire life. Insidious onset, patient does not recall any trauma. Empty can +, Yerguson's -, Speed's -. List the possible sequelae.
Adhesive capsulitis
Intervertebral foraminal enlargement
DJD
Osteoporosis
Metastasis
Bone deformity
Skin lesions
Neurological defects
Male age 28. Patient presents with back pain that came on over the past two weeks. The pain is rated a 9 out of 10 on the pain scale. Nothing makes the pain go away or feel better. SLR+ at 20˚and cause ipsilateral SI pain and contralateral leg pain, Bragard’s +. What are possible lab findings?
Increased PSA
Increased WBC
Neutrophilia
Thrombocytopenia
Increased ESR
Eosinophilia
Increase in alkaline phosphatase
Reversal of A:G ratio
Male age 28. Patient presents with back pain that came on over the past two weeks. The pain is rated a 9 out of 10 on the pain scale. Nothing makes the pain go away or feel better. SLR+ at 20˚and cause ipsilateral SI pain and contralateral leg pain, Bragard’s +. What are the most common clinical findings?
Analgesics do not relieve pain
Recurrent UTI
Fever
Decrease in pulse rate
Positive Dejerine's triad
Nocturia
Alteration of urinary stream
Skin changes
Male age 28. Patient presents with back pain that came on over the past two weeks. The pain is rated a 9 out of 10 on the pain scale. Nothing makes the pain go away or feel better. SLR+ at 20˚and cause ipsilateral SI pain and contralateral leg pain, Bragard’s +. List the most likely places in society this condition will be seen.
Sports
Lab technician
Genetic cell mutation
Toxic exposure
Occupational hazard
Radiation therapy
IV drug use
Female age 45. Patient presents with low back pain that started when she bent over to tie her shoe. The severity of the pain ranges from a 2 to a 9 out of 10 on the pain scale. She says it feels better when she is lying on the floor. She also has pain in her left medial knee down into the left medial aspect of her big toe. SLR + with radiation down leg, Kemps +.What would be the initial treatment?
Ab strengthening
Moist heat every 2 hours
Complete bed rest for one week
Extension exercises
Lumbar traction
Core stabilization
Diathermy
Female age 45. Patient presents with low back pain that started when she bent over to tie her shoe. The severity of the pain ranges from a 2 to a 9 out of 10 on the pain scale. She says it feels better when she is lying on the floor. She also has pain in her left medial knee down into the left medial aspect of her big toe. SLR + with radiation down leg, Kemps +. Additional clinical findings?
Decrease in patellar reflex
Hyperreflexia
Weak leg muscles
Myelopathy
Clonus
Diminished hamstring reflex
Diminished achilles reflex
Diminished sensation over the medial malleolus
Female age 45. Patient presents with low back pain that started when she bent over to tie her shoe. The severity of the pain ranges from a 2 to a 9 out of 10 on the pain scale. She says it feels better when she is lying on the floor. She also has pain in her left medial knee down into the left medial aspect of her big toe. SLR + with radiation down leg, Kemps +. If untreated, what could possibly happen?
Atrophy of muscles
Permanent sensation loss
Cauda equina
Gastrocnemius weakness
Medial hamstring reflex diminished
Loss of vibration sense in lower extremity
Loss of pain and temperature sensation in lower extremity

Female age 45. Patient presents with a gradual onset of low back pain. She reports doing light secretarial work that sometimes makes it worse. Rolled shoulders, anterior head carriage, tight lumbar paraspinal muscles. List the DDx.
Hemangioma
Vascular neoplasm
Lytic mets
Benign bone tumor
Osteomyleitis
Osteoporosis
Hyperparathyroidism
Osteoid osteoma

Female age 45. Patient presents with a gradual onset of low back pain. She reports doing light secretarial work that sometimes makes it worse. Rolled shoulders, anterior head carriage, tight lumbar paraspinal muscles. What else could be seen with this condition?
Vertebral body collapse
Pseudo fracture
Vertebral body expansion
Metastasis
Brown's tumor
Spinal stenosis
Gardener's syndrome
Skull enlargement

Female age 45. Patient presents with a gradual onset of low back pain. She reports doing light secretarial work that sometimes makes it worse. Rolled shoulders, anterior head carriage, tight lumbar paraspinal muscles. What is the appropriate treatment approach for this condition?
Oncologist
Orthopedic
Vascular specialist
IV antibiotic therapy
Continue normal ADLs
Send for colonoscopy
Adjust to patient tolerance
Female age 45. Patient presents with tingling in both of her feet, she has problems feeling her feet, has frequent trips and falls. She reports feeling unsteady. Weigh 210 lbs, Height 5’6”, Normal ROM, Normal DTR, Murphy’s punch +, Paraspinal muscle spasm on the left. List the best possible clinical findings.
Ketones in urine
Glucosuria
Hematuria
Papilladema
Polyuria
Urobilinogen in urine
Muscle weakness
Pale optic disc
Female age 45. Patient presents with tingling in both of her feet, she has problems feeling her feet, has frequent trips and falls. She reports feeling unsteady. Weigh 210 lbs, Height 5’6”, Normal ROM, Normal DTR, Murphy’s punch +, Paraspinal muscle spasm on the left. List the most likely presentations of this condition.
Decrease in wound healing
Kidney stones
Increase in vaginal infections
Vitamin B12 deficiency
Gastric distress
Cotton wool exudates
Neovascularization
Macrocytic anemia
Female age 45. Patient presents with tingling in both of her feet, she has problems feeling her feet, has frequent trips and falls. She reports feeling unsteady. Weigh 210 lbs, Height 5’6”, Normal ROM, Normal DTR, Murphy’s punch +, Paraspinal muscle spasm on the left. List the treatment options.
Low glycemic index diet
Capacity of walking to cycling comparison
Increase physical activity
Co-treat with endocrinologist
Send out for NCV/EMG
Decrease in exercise
Suggest swimming instead of walking
Hot packs to relieve leg pain
Male age 13. Young athlete presents with ankle pain and swelling one day after an injury from basketball. Pain feels worse with movement and feels better with rest. Pain is felt in all ranges of motion. Anterior drawer sign +. List the radiographic findings.
Metaphyseal lesion
Diaphyseal lesion
Moth eaten
Permeative
Wide zone
Cortical lesion
Expansile lesion
Laminating periosteal reaction
Male age 13. Young athlete presents with ankle pain and swelling one day after an injury from basketball. Pain feels worse with movement and feels better with rest. Pain is felt in all ranges of motion. Anterior drawer sign +. What are the DDx?
Sprain/Strain
Quasimalignant tumor
SBC
Epiphyseal fracture
Ewing's
ABC
Blood filled lesion
Fluid filled lesion
Male age 13. Young athlete presents with ankle pain and swelling one day after an injury from basketball. Pain feels worse with movement and feels better with rest. Pain is felt in all ranges of motion. Anterior drawer sign +. What are the management options?
Low volt for pain
Orthopedic surgeon
Immobilize for 6 weeks
Ultrasound
Oncologist
Evaluate for splint
Eliminate weight bearing
Chiropractic care
Male age 64. Patient presents with difficulty walking, and no movement of his arms while he is ambulating. Shuffling gait is present. What are additional findings?
Cogwheel rigidity
Hyperreflexia
Weakness
Resting tremors
Bradykinesia
Visual disturbances
Male age 64. Patient presents with difficulty walking, and no movement of his arms while he is ambulating. Shuffling gait is present. What are the possible sequelae?
Tinnitus
Vertigo
Cauda equina
Constipation
Diarrhea
Difficulty swallowing
Respiratory paralysis
Peripheral involvement
Male age 64. Patient presents with difficulty walking, and no movement of his arms while he is ambulating. Shuffling gait is present. List the best follow up options.
Modify home to decrease falls
Refer to opthalmologist
Neurologist
MRI Lumbar
Encourage continuation of ADLs
Upper cervical X-rays
Defer chiropractic care
Refer for hearing evaluation

Male age 22. Patient presents with insidious onset of wrist pain that started one week ago. Father has a history of Hodgkin’s. Distal radius is warm, swollen, and tender, Decrease ROM is all planes with pain, x-ray shows a soap bubbly lesion that is eccentrically located. What are the DDx?
Osteomyelitis
GCT
ABC
Enchondroma
Osteochondroma
Chondroblastoma
Osteosarcoma

Male age 22. Patient presents with insidious onset of wrist pain that started one week ago. Father has a history of Hodgkin’s. Distal radius is warm, swollen, and tender, Decrease ROM is all planes with pain, x-ray shows a soap bubbly lesion that is eccentrically located. What are the possible treatment options/next step?
Oncologist
Surgical consult
MRI
Antibiotics
Curettage
ER
Brace/Stabilize
Refer for biopsy

Male age 22. Patient presents with insidious onset of wrist pain that started one week ago. Father has a history of Hodgkin’s. Distal radius is warm, swollen, and tender, Decrease ROM is all planes with pain, x-ray shows a soap bubbly lesion that is eccentrically located. What are the possible future consequences?
Complete resolution
Septicemia
Vascular compromise
Neurological deficit
Malignant degeneration
Pathological fracture
Lymphedema
Bony fusion
Female age 24. Patient presents with extreme neck pain that she woke up with this morning. She reports being on the phone for two hours last night sitting next to an open window. Head right lateral tilt and left rotation. What are the DDx?
Myoclonus
Spastic torticollis
Cervicogenic cephalgia
Myofascial pain syndrome
Wry neck
Cervical disc lesion
Meningitis
Sprain/Strain
Female age 24. Patient presents with extreme neck pain that she woke up with this morning. She reports being on the phone for two hours last night sitting next to an open window. Head right lateral tilt and left rotation. What are the treatment options?
Myofascial Release
Vapocoolant spray and stretch
Cervical collar
Moist heat
Isokinetic exercise
Trigger point therapy
Hard cervical collar
Cervical Traction
Female age 24. Patient presents with extreme neck pain that she woke up with this morning. She reports being on the phone for two hours last night sitting next to an open window. Head right lateral tilt and left rotation. What are the most likely causes?
Biochemical
Focal muscle dystonia
Cold environment
Brachial plexus syndrome
Genetic
Sprain/Strain
Viral infection
Bacterial infection

Male age 22. Patient presents with insidious onset of low back pain and sacroiliac pain. He also reports having gastrointestinal issues. Forrestier’s sign +, Chest expansion 1.25”. What are the radiographic signs expected?
Shiny corner
Trolley track
Hiatal hernia
Unilateral SI sclerosis
Chondral sclerosis
Overhanging edge sign
Non-marginal syndesmophytes
Dagger sign

Male age 22. Patient presents with insidious onset of low back pain and sacroiliac pain. He also reports having gastrointestinal issues. Forrestier’s sign +, Chest expansion 1.25”. What are the DDx?
AS
Enteropathic arthropathy
Gouty arthritis
Psoriatic arthritis
Psoriatic arthritis
Osteitis condensans ilii
Osteomyleitis
Bilateral sacroiliitis
Reiter's syndrome

Male age 22. Patient presents with insidious onset of low back pain and sacroiliac pain. He also reports having gastrointestinal issues. Forrestier’s sign +, Chest expansion 1.25”. What is seen in the progression of this condition?
Anderson lesion
Carrot stick fracture
Hepatomegaly
Silver scales
Pitted nails
Erosion of joints
Overhanging edge sign
Anterior uveitis

Male age 55. Patient presents with back and abdominal pain. Pain is increased when his grandson sits on his abdomen. Patient has difficulty sitting up. SLR + at 85 degrees. What is most diagnostic in the physical exam of this condition?
Cold feet
Numbness in feet
Weakness in lower extremity
Abnormal auscultation of abdomen
Abnormal pulsation over abdomen
Abdominal pain upon exertion
Difficulty breathing
Ascites

Male age 55. Patient presents with back and abdominal pain. Pain is increased when his grandson sits on his abdomen. Patient has difficulty sitting up. SLR + at 85 degrees. What may be seen in the case history of this patient?
Long history of smoking
Increased cholesterol
Family history of cardiovascular disease
Congenital anomalies of blood vessels
Injury to low back
Prior surgery for cancer
Increased tactile fremitus

Male age 55. Patient presents with back and abdominal pain. Pain is increased when his grandson sits on his abdomen. Patient has difficulty sitting up. SLR + at 85 degrees. What are the management options?
ER
Vascular specialist
Internist
Evaluation with diagnostic ultrasound
Adjust lumbar spine
Check for retinopathy in the spine
Defer chiropractic care
MRI
Female age 24. Patient presents with headaches, blurred vision that lasts for approximately 30 minutes before each episode. Pain is throbbing. A cold cloth is palliative. Distraction produces minor suboccipital pain, Jackson’s -, Decreased ROM in all directions, Normal BP, Normal vitals. What are the clinical findings in this case?
Photophobia
Rhinorrhea
Prodrome/Aura
Papilledema
Anhidrosis
Nausea
Tearing of eyes
Vertigo
Female age 24. Patient presents with headaches, blurred vision that lasts for approximately 30 minutes before each episode. Pain is throbbing. A cold cloth is palliative. Distraction produces minor suboccipital pain, Jackson’s -, Decreased ROM in all directions, Normal BP, Normal vitals. What are the treatment options for this condition?
Adjust
Corticosteroids
Moist heat
Diet log
Doppler ultrasound imaging
Flexion and extension x-rays
Massage therapist
Vascular specialist
Female age 24. Patient presents with headaches, blurred vision that lasts for approximately 30 minutes before each episode. Pain is throbbing. A cold cloth is palliative. Distraction produces minor suboccipital pain, Jackson’s -, Decreased ROM in all directions, Normal BP, Normal vitals. What are the aggravating factors?
Hormone imbalance
Increase protein
Bright light
Allergies
Physical activity
Consumption of red wine
Consumption of beer
Sleep
Female age 37. Patient presents with neck pain and headaches that radiate behind the right eye. The pain is achy and rates a 5 out of 10 on the pain scale. Paraspinal muscle spasms, Suboccipital tension, Decreased ROM, BP 138/80. What are the DDx?
Cluster headache
Common migraine
Cervicogenic headache
Tension Headache
Hypertension headache
TMJ headache
Sinus headache
CVA
Female age 37. Patient presents with neck pain and headaches that radiate behind the right eye. The pain is achy and rates a 5 out of 10 on the pain scale. Paraspinal muscle spasms, Suboccipital tension, Decreased ROM, BP 138/80. What are the likely additional findings?
Drooping eyelid
Vertigo
Nausea
Photophobia
Sensitive to sound
Pain while chewing
Increase serum cholesterol
Scalp sensitivity
Female age 37. Patient presents with neck pain and headaches that radiate behind the right eye. The pain is achy and rates a 5 out of 10 on the pain scale. Paraspinal muscle spasms, Suboccipital tension, Decreased ROM, BP 138/80. What are the management options?
CT
Neurologist
Adjust
Myofascial release technique
CT of brain
Check for seasonal allergies
Evaluate ESR
Suggest relaxation technique

Male age 42. Patient presents after slamming his foot in the door two months ago. He reports burning pain that rates 6 out of 10 on the pain scale. His foot is red swollen and skin appears shiny. Activity provokes pain. What is responsible for the presenting complaints?
Septic arthritis
Cellulitis
Complex regional pain syndrome
Infection
Peripheral vascular compromise
Gonococcal arthritis
Disuse Atrophy

Male age 42. Patient presents after slamming his foot in the door two months ago. He reports burning pain that rates 6 out of 10 on the pain scale. His foot is red swollen and skin appears shiny. Activity provokes pain. What are the indicated approaches?
Ultrasound
Air cast immobilization
Massage
Surgical Fusion
Sympathetic nerve block
TENS
Antibiotics
Corticosteroids

Male age 42. Patient presents after slamming his foot in the door two months ago. He reports burning pain that rates 6 out of 10 on the pain scale. His foot is red swollen and skin appears shiny. Activity provokes pain. What are possible additional symptoms that may occur?
Osteonecrosis
Joint destruction
Fever
Hyperesthesia
Anhidrosis
Hypertrichosis
Muscle weakness
Ulceration of skin

Female age 71. Patient presents with sudden onset of low back pain 18 hours ago. Ice makes it feel better. The pain is rated and 8 out of 10 on the pain scale. No orthos due to pain. What are the DDx?
Spondylitis
Osteoporotic fracture
Lytic mets
Pathological fracture
Unstable fracture
Step defect
Pars fracture
Facet arthrosis

Female age 71. Patient presents with sudden onset of low back pain 18 hours ago. Ice makes it feel better. The pain is rated and 8 out of 10 on the pain scale. No orthos due to pain. What are the best treatment options?
Extension exercises
Orthopedist
Modified ADLs
Strengthen hip flexors
Adjust
Cryotherapy
Oncologist
Bed rest

Female age 71. Patient presents with sudden onset of low back pain 18 hours ago. Ice makes it feel better. The pain is rated and 8 out of 10 on the pain scale. No orthos due to pain. What is seen in the progression of this condition?
Postural changes
Altered biomechanics
Increased rate of degeneration
Metastatic spread
Septicemia
Cachexia
Unrelenting back pain
Disability
Male age 52. Patient presents with mid to low back pain. Pain is felt in every direction. Kemps -, Yeoman’s + in hip, thoracolumbar junction and lumbar spine, coxa vara bilaterally. What are the DDx?
Paget's
Fibrous dysplasia
Burkitt's Lymphoma
Multiple myeloma
Blastic mets
Hodgkins
Lytic mets
Hyperparathyroidism
Male age 52. Patient presents with mid to low back pain. Pain is felt in every direction. Kemps -, Yeoman’s + in hip, thoracolumbar junction and lumbar spine, coxa vara bilaterally. What is also likely to be involved in this condition?
Skull
Colon
Ulna
Liver
Lung
Femur
Pelvis
Heart
Male age 52. Patient presents with mid to low back pain. Pain is felt in every direction. Kemps -, Yeoman’s + in hip, thoracolumbar junction and lumbar spine, coxa vara bilaterally. What is the possible sequelae?
Malignant degeneration
Spinal canal stenosis
Horner's
Dyspnea
Tibial deformity (Saber shin)
Lymph node obstruction
Pathological collapse
Lytic destruction
Female age 19. Patient present with neck pain she woke up with this morning. She has hypertonic cervical extensor muscles. Pain is dull and is 3 out of 10 on the pain scale. Decreased ROM due to pain, Distraction +, Compression +, pain does not radiate. What are the DDx?
Bilateral dystonia of SCM
Hypertonic paraspinals
Nerve root compression
TOS
Space occupying lesion
Myofascitis
Sprain/Strain
Adhesions
Female age 19. Patient present with neck pain she woke up with this morning. She has hypertonic cervical extensor muscles. Pain is dull and is 3 out of 10 on the pain scale. Decreased ROM due to pain, Distraction +, Compression +, pain does not radiate. What are the treatment options?
MRI
Nerve block
Myofascial release
Cervical traction
Trigger point therapy
Diathermy
Orthopedist
Adjust to patient tolerance
Female age 19. Patient present with neck pain she woke up with this morning. She has hypertonic cervical extensor muscles. Pain is dull and is 3 out of 10 on the pain scale. Decreased ROM due to pain, Distraction +, Compression +, pain does not radiate. What would you observe if the patient presents further with a headache and fever?
Ketones in urine
Radionucleotide scan
Kernigs +
Increased monocytes
Heterophile +
Increased WBC
+ ESF exam
Plaques seen on MRI
Brudzinki's +
Male age 55. Patient presents with hip pain that is worse in the morning and at night. The pain feels better after 30 minutes of being up. Pain is worse after long distance walking and standing. Father has a history of AVN. ROM of thoracic and lumbar is limited and painful. List the radiographic images you would see.
Uniform loss of joint space
Nonuniform loss of joint space
Subchondral cyst
Osteophytes
Flattened femoral head
Crescent sign
Brim sign
Sagging rope sign
Male age 55. Patient presents with hip pain that is worse in the morning and at night. The pain feels better after 30 minutes of being up. Pain is worse after long distance walking and standing. Father has a history of AVN. ROM of thoracic and lumbar is limited and painful. What is the possible etiology?
Significant trauma
Corticosteroids
Unrealized microtrauma
Cardiac involvement
Genetic
Pathological
Drug abuse
Rheumatic fever as a child
Male age 55. Patient presents with hip pain that is worse in the morning and at night. The pain feels better after 30 minutes of being up. Pain is worse after long distance walking and standing. Father has a history of AVN. ROM of thoracic and lumbar is limited and painful. What are the possible palliative factors?
Heat
Passive ROM exercises
Drug therapy
Non-weight bearing exercises
Cryotherapy
Bed rest
Immobilization
Weight gain
Female age 32. Patient presents bilateral finger and hand pain with numbness and tingling. Patients report pain at night and rates a 3 to 5 out of 10 on the pain scale. Spends most of her time typing as a secretary. Phalens+, Wrights-, Adsons-. What are the DDx?
Median nerve entrapment
Ulnar nerve entrapment
Radial nerve entrapment
Pronator teres syndrome
Carpal tunnel syndrome
Tunnel of guyon
Dequervain's Disease
Female age 32. Patient presents bilateral finger and hand pain with numbness and tingling. Patients report pain at night and rates a 3 to 5 out of 10 on the pain scale. Spends most of her time typing as a secretary. Phalens+, Wrights-, Adsons-. How would you monitor if the condition is getting worse?
Decrease dynamometer readings
Numbness in medial hand
Inability to perform pinch grip
Hands turn blue
Hypothenar atrophy
Finklesteins +
Swelling over first metacarpophalangeal joint
Thenar atrophy
Female age 32. Patient presents bilateral finger and hand pain with numbness and tingling. Patients report pain at night and rates a 3 to 5 out of 10 on the pain scale. Spends most of her time typing as a secretary. Phalens+, Wrights-, Adsons-. What are the treatment options?
Adjust carpal bones
Transverse friction massage of pronator teres
Evaluate work station ergonomics
Refer for surgery
Strengthen wrist flexors
Cast wrist
Adjust C spine
B5 supplement
Female age 19. Patient presents with a drooping eyelid on one side and ipsilateral inability to raise her eyebrow. Loss of taste to the anterior 2/3rd of her tongue. What are the DDx?
Lower motor neuron lesion
Trigeminal neuralgia
Stroke
Bell's Palsy
Tic douloureaux
CN V
CN VII
Grave's disease
Patient presents with a drooping eyelid on one side and ipsilateral inability to raise her eyebrow. Loss of taste to the anterior 2/3rd of her tongue. What are the possible sequelae if the condition does not resolve?
Flaccid paralysis
Dental orbital pain
Decrease corneal reflex
Constant unremitting pain
Decreased jaw jerk reflex
Tendency towards herpes zoster
No control of saliva while eating
Anosmia
Patient presents with a drooping eyelid on one side and ipsilateral inability to raise her eyebrow. Loss of taste to the anterior 2/3rd of her tongue. What is the proper treatment?
Eye patch
Neurologist
Adjust
Hospital
Diathermy
Artifical tears
Infrared
Ultrasound
Female age 17. Cheerleader presents with bouts of low back pain. Deep dull ache that rates a 4 to 6 out of 10 on the pain scale. Stork test +. What are the possible clinical findings?
Increased lumbar lordosis
Decreased lumbar lordosis
Hypertonic hamstrings and quads
Hypertonic quads
Inhibited psoas
Inhibited quads
Hypertonic lumbar erectors
Inhibited abdominals and psoas
Female age 17. Cheerleader presents with bouts of low back pain. Deep dull ache that rates a 4 to 6 out of 10 on the pain scale. Stork test +. What is the best initial treatment?
Prone adjusting
Side posture
Continue normal activities
Suspend normal activities
Anti lordotic bracing
Cryotherapy
Take stress films
TENS
Female age 17. Cheerleader presents with bouts of low back pain. Deep dull ache that rates a 4 to 6 out of 10 on the pain scale. Stork test +. What muscles should be strengthened?
Psoas
Hamstrings
Quad
Lumbar erectors
Piriformis
Vastus lateralis
Transverse abdominals
Gluteus maximus
Female age 35. Bank teller of 13 years presents with bilateral numbness of her arms and hands and has severe neck pain. Shaking her hands makes her hands feel better but nothing relieves her neck pain. Decreased ROM Cervicals, Wrights+, Adsons+. What is the etiology?
Cervical rib
Spinal stenosis
OA
Hypertonic scalenes
Apical lung tumor
Neurovascular compromise
Costoclavicular impingement
DJD
Female age 35. Bank teller of 13 years presents with bilateral numbness of her arms and hands and has severe neck pain. Shaking her hands makes her hands feel better but nothing relieves her neck pain. Decreased ROM Cervicals, Wrights+, Adsons+. What are the possible management options?
Cock up splint
Strengthen pecs
Stretch mid traps
Strengthen scalenes
Cross friction massage of pronator teres
Stretch pecs
Neck retraction exercises
Stretch scalenes
Female age 35. Bank teller of 13 years presents with bilateral numbness of her arms and hands and has severe neck pain. Shaking her hands makes her hands feel better but nothing relieves her neck pain. Decreased ROM Cervicals, Wrights+, Adsons+. What advice would you give the patient if there is no improvement?
Ultrasound
Angiogram
Surgical consult
Radionucleotide scan
Neurodiagnostic
AP and lateral chest films
NCV
Doppler
{"name":"Vignette's", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"Test your knowledge with this comprehensive quiz on differential diagnoses, clinical findings, and follow-up procedures for various medical conditions. Designed for healthcare professionals and students, this quiz covers a diverse range of clinical scenarios.102 challenging questionsMultiple choice format with checkboxes for detailed responsesFocus on real-world clinical cases","img":"https:/images/course6.png"}
More Quizzes
Neurogenic and Myopathic Dysfunction
10511
Pathophysiology 6
10514
Who would you choose
15814
DCMS FBP quiz (2)
940
Does He Like Me Over Text? Middle School
201021045
Beyblade Burst - Which Character Are You?
201018500
Bridge to Terabithia - Test Your Book Knowledge
201025734
Limits & Continuity - Free AP Calculus Practice
201021939
Vermont Trivia - Test Your Green Mountain Knowledge
201025534
Singular and Plural Verb Agreement - Collective Nouns
201029563
Plant Trivia - Test Your Botany Knowledge Online
201019128
JROTC Rank - Which Army Rank Are You?
201022075