
ECN and Teachers' Questions page 345-387 part 9
A 27-year-old man is referred by his GP with progressively painful swelling of his left knee following a minor football injury some weeks ago. The radiograph shows a 5-cm ill-defined lytic lesion within the left distal femoral metaphysis, with a permeative pattern of bone loss and areas of cloud-like ossification. There is an extensive periosteal reaction, predominantly orientated perpendicular to the cortex. What is the most likely diagnosis?
Aneurysmal bone cyst.
Chondrosarcoma.
Ewing’s sarcoma.
Metastasis.
Osteosarcoma.
An 80-year-old woman is admitted to hospital following a fall. The patient had a right mastectomy and axillary dissection 5 years ago to treat an invasive ductal carcinoma. The pelvic radiograph reveals a left hip fracture. Which fracture site would be most suggestive of a pathological fracture?
Greater trochanter fracture
Intertrochanteric fracture of the left proximal femur.
Subcapital fracture of the left neck of femur.
Pertrochanteric fracture of the left proximal femur.
Subtrochanteric fracture of the left proximal femur.
A 19-year-old student returns to the UK following 4 months’ travelling around the world. Radiographs reveal multiple oval areas of calcification, up to 1 cm in long axis, aligned in the direction of muscle fibres. What is the most likely diagnosis?
Cysticercosis.
Dracunculus (guinea worm) infection.
Hydatid disease.
Loiasis.
Schistosomiasis.
A previously well 80-year-old woman sustains a subcapital fracture of the right neck of femur following a fall onto hard ground. The plain film reveals multiple lytic lesions within the pelvic bones and proximal femora, which are highly suspicious for bone metastases. What is the most likely occult primary lesion?
Carcinoma of the breast
Carcinoma of the bladder.
Carcinoma of the colon
Carcinoma of the bronchus
Carcinoma of the stomach
A 34-year-old man with chronic back pain is referred by his GP for thoracic and lumbar spine radiographs. The GP is concerned about the possibility of ankylosing spondylitis. Which radiological feature is atypical for ankylosing spondylitis, and might suggest an alternative diagnosis?
Anterior longitudinal ligament calcification
Ankylosis of the apophyseal joints
Sclerosis of the anterior corners of the vertebrae
Osteophyte formation
Vertebral body squaring
A 50-year-old woman complains of painful swelling of the joints of the hands and wrists. Radiographs show evidence of an erosive arthropathy. Which radiological feature would favour a diagnosis of rheumatoid rather than psoriatic arthritis?
Erosions of the terminal tufts of the distal phalanges
Early reduction in bone mineralisation.
Pencil-in-cup deformities of the middle phalanges
Joint ankylosis
Periosteal reaction
An 18-year-old man attends his general practitioner with a painful right knee. His radiograph shows a well-defined, lobular, lytic lesion within the proximal tibial epiphysis, extending into the metaphysis. There is a faintly sclerotic margin and no matrix calcification. What is the most likely diagnosis?
Chondromyxoid fibroma
Chondroblastoma
Giant cell tumour
Enchondroma
Osteoid osteoma
A young girl is brought to the Emergency Department with a painful right elbow following a fall. The radiograph reveals that the radial head is ossified. Which other structure should be visible?
Internal epicondyle
Capitellum
Lateral epicondyle
Olecranon
Trochlea
A radiograph of the left knee of a 35-year-old man reveals a 3-cm lytic lesion sited eccentrically in the proximal tibia. It has a well-defined non-sclerotic margin, and extends to the tibial articular surface. What is the most likely diagnosis?
Chondroblastoma
Aneurysmal bone cyst.
Non-ossifying fibroma
Giant cell tumour
Osteoid osteoma
A 35-year-old woman is referred to thee Radiology Department following the birth of her first child. The baby was delivered 8 days post-term and was a vaginal delivery following a prolonged labour and episiotomy. Two months later, the patient continues to experience faecal incontinence and an anal sphincter tear is suspected. Which investigation would be most useful to demonstrate anal sphincter damage?
CT with rectal contrast media
Barium evacuation proctogram
Endoanal ultrasound
CT colonography
MRI of the pelvis with a body coil.
A 37-year-old man presents to his GP with increasing right upper quadrant pain. On examination, he is afebrile with right upper quadrant tenderness and fullness. An abdominal ultrasound is performed and demonstrates a 5-cm diameter cystic lesion in the right lobe of liver. The mass contains multiple septations with a large cyst centrally and multiple small cystic spaces peripherally. Echogenic debris is seen within the cystic lesion and alters in position when the patient lies on his side. From the clinical an sonographic details, what is the most likely diagnosis?
Hydatid cyst
Amoebic abscess
Simple liver cyst
Pyogenic liver abscess
Solitary metastasis
A 33-year-old woman presents to her GP with a one year history of intermittent rectal bleeding. She experiences regular episodes of fresh blood per rectum with associated lower abdominal pain, lasting several days at a time. A flexible sigmoidoscopy is normal. A double contrast barium enema is performed and demonstrates an irregular appearance of the anterior wall of the sigmoid colon with mild extrinsic mass effect. What is the most likely diagnosis?
Endometriosis
Carcinoma of the sigmoid colon
Radiation enteritis
Pelvic lipomatosis
Solitary rectal ulcer syndrome
A 56-year-old woman presents with a 4-day history of right upper quadrant pain and vomiting. She describes a previous episode one year ago that resolved after a few day. On examination, she is very tender in the right upper quadrant with guarding on deep palpation during inspiration. Laboratory investigations reveal elevated white cell count and CRP but normal liver function tests and an abdominal ultrasound is performed. What are the most likely ultrasound findings?
Nodular liver surface, mixed reflectivity liver texture and ascites
Hypoechoic mass in the pancreatic head with common bile duct measuring 14 mm and pancreatic duct measuring 6 mm in diameter
Several large gallstones with gallbladder wall measuring 5 mm and a rim of pericholecystic fluid
Severe intrahepatic duct dilatation with no cause identified
Several small gallstones with gallbladder wall thickness of 2 mm
An 82-year-old woman is referred to the on-call surgical team as an emergency admission. The patient lives in a residential care home and has a 48-hour history of generalised abdominal pain and vomiting. On examination, she is dehydrated and tachycardic and an abdominal radiograph demonstrates multiple dilated small bowel loops measuring up to 4.8 cm in diameter. A linear gas-filled structure is present in the right upper quadrant with short branches extending from it. What is the most likely diagnosis?
Emphysematous cholecystitis
Acute mesenteric ischaemia
Obstructed right inguinal hernia
Gallstones ileus
Small bowel obstruction due to adhesions
A 72-year-old man is referred to hospital as an emergency admission by his GP. He has experienced vomiting and abdominal pain for 24 hours following a takeaway meal. There is a past medical history of ischaemic heart disease, chronic obstructive pulmonary disease and hypertension. An abdominal radiograph is performed and demonstrates several gas-filled loops of small bowel centrally measuring up to 2.5 cm diameter. In the left side of the abdomen, multiple round foci of gas are projected over the wall of a loop of large bowel. No free gas or mucosal thickening is identified, what is the most likely explanation for the clinical and radiographic findings?
Emphysematous pyelonephritis with a paralytic ileus
Gastroenteritis with incidental pneumatosis coli
Perforated sigmoid diverticulitis with gas in the retroperitoneum
Ischaemic colitis causing intramural bowel gas
Small bowel obstruction due to a gallstone ileus
A 68-year-old woman presents with a 2month history of generalized abdominal bloating and two episodes of vaginal bleeding. On examination, the abdomen is distended with clinical evidence of ascites. Tumour makers are performed; CA 15-3 is normal, CA 125 and CEA are slightly elevated and CA 19-9 is markedly elevated. An abdominopelvic ultrasound demonstrates a moderate volume of ascites, multiple liver metastases and bilateral mixed solid/cystic adnexal masses. What is the most likely underlying primary tumour?
Gastric adenocarcinoma
Breast cancer
Ovarian cancer
Melanoma
Primary peritoneal carcinoma
A 27-year-old man is referred to the hepatology outpatient clinic with a 3-week history of malaise, lethargy and mild upper abdominal pain. Liver function tests performed by his GP are significantly abnormal. The results of hepatitis serology performed in the clinic are consistent with an acute hepatitis B infection. An abdominal ultrasound is performed. What is the most likely finding on ultrasound?
Increased reflectivity of the liver parenchyma
Decreased reflectivity of the liver parenchyma
Normal ultrasound appearances
Nodular liver surface
Retrograde portal venous flow
A 32-year-old man presents to his GP with increasing pain on swallowing solids and liquids. He has lost 15 kg in weight over the preceding 2 months. After a full history and examination, he is found to be HIV positive with a very low CD4 count. The GP refers him for a barium swallow examination and this demonstrates a single ulcer in the mid-oesophagus. The ulcer has a smooth margin, measures 4 cm in length and is oval in shape. There is no stricture identified. Which diagnosis is most likely?
CMV oesophagitis
Candida oesophagitis
Oesophageal lymphoma
Intramural pseudodiverticulosis
Squamous cell carcinoma of the oesophagus
A 49-year-old woman has experienced increasing difficulty swallowing over the past 6 months, with associated retrosternal discomfort. A barium swallow is performed and demonstrates virtually no peristaltic activity within a dilated oesophagus. The gastro-oesophageal junction appears widened and there is marked reflux of barium when the patient lies supine. An upper GI endoscopy shows moderate reflux oesophagitis. Given these findings, what is the most likely underlying diagnosis?
Oesophageal web
Achalasia
Scleroderma
Presbyoesophagus
Squamous cell carcinoma of oesophagus
A 30-year-old man attends the Emergency Department with a 2-day history of abdominal pain and vomiting. On examination, he is afebrile with a firm mass palpable in the right lower quadrant of the abdomen. A supine abdominal radiograph is performed and demonstrates dilated loops of small bowel with a large soft tissue mass in the right lower quadrant. On ultrasound, the mass has a “pseudotumour” appearance. What is the most likely diagnosis?
Gallstone ileus
Colonic carcinoma
Intussusception
Psoas abscess
Strangulated femoral hernia
A 49-year-old man is involved in a road traffic accident and sustains serious head and chest injuries. He is ventilated on the intensive care unit and his injuries are managed conservatively. Ten days later, he develops a temperature of 39.5°c, becomes tachycardic and requires inotropic support to maintain his blood pressure. An abdominal ultrasound is performed and shows a cystic structure in the right upper quadrant measuring 12 x 8 cm in size. The mass has a 6-mm thick wall, contains a layer of echogenic material and is surrounded by a rim of fluid. What is the most likely diagnosis?
Acute cholangitis
Acalculous cholecystitis
Traumatic hepatic artery pseudoaneurysm
Gallbladder haematoma
Xanthogranulomatous cholecystitis
A 40-year-old male diabetic patient has an intravenous urogram (IVU) for left-sided renal colic. On the IVU, the left kidney shows papillary and calyceal abnormalities that give an “egg in a cup” appearance at some calyces and “tracks and horns” at other calyces. The affected left kidney has preserved renal cortical thickness despite the calyceal/papillary abnormalities. The contralateral kidney appears normal. What is the most likely diagnosis?
Amyloidosis
Acute pyelonephritis
Renal papillary necrosis
Reflux nephropathy
Xanthogranulomatous pyelonephritis
A 40-year-old female diabetic patient has right loin pain, vomiting and a fever. An ultrasound examination is requested to exclude urinary obstruction. This demonstrates no evidence of upper tract dilatation, but features of acute pyelonephritis are present. What are the most likely sonographic findings within the right kidney?
Focal atrophy of segments of the right kidney
Focal areas of reduced reflectivity in the renal parenchyma
Enlarged right kidney and diffusely hyperechoic parenchyma
Increased echogenicity of the renal calyces
Shrunken right kidney and diffusely hyperechoic parenchyma
A 55-year-old HIV-positive man presents with macroscopic haematuria and right-sided renal colic. An IVU does not demonstrate any renal tract calcification, but there is a dense right nephrogram with no excretion of contrast on a delayed film. The urologist performs a retrograde ureteroscopy and retrieves a 9-mm right ureteric calculus. What is the likely composition of the calculus?
Cysteine
Calcium oxalate
Indinavir phosphate
Struvite
Uric acid
A 29-year-old man has an IVU performed following an episode of haematuria. This demonstrates complete right-sided ureteric duplication. Which one of the following statements is true?
The lower moiety ureter usually obstructs at the vesicoureteric junction
If present, an ectopic ureterocoele is usually related to the lower moiety ureter
The upper moiety ureter is prone to ureteric obstruction
The upper moiety calyces are prone to vesicoureteric reflux
The upper moiety ureter usually inserts into the bladder superior to the lower moiety ureter.
A 27-year-old man with membranous glomerulonephritis presents with a 1-day history of right-sided flank pain and haematuria. An abdominal radiograph did not reveal any renal calcification but his renal function has significantly deteriorated over the past 24 hours. On ultrasound there is a large, oedematous right kidney with loss of the corticomedullary differentiation. On a subsequent IVU, there is a faint nephrogram with absent pelvicalyceal filling after 15 minutes. What is the most likely diagnosis?
Acute pyelonephritis
Acute hydronephrosis
Acute renal vein thrombosis
Acute renal infarction
Chronic pyelonephritis
A 24-year-old motorcyclist involved in a traffic accident presents to the Emergency Department with a broken leg and bruising over his left flank. He is found to have microscopic haematuria and fractures of the left 8th and 9th ribs. The patient is haemodynamically stable and clinicians suspect a left renal injury. Which one of the following imaging investigations is the most appropriate?
Contrast-enhanced CT abdomen and pelvis
Abdominal ultrasound
Gadolinium-enhanced renal MRI
Emergency catheter renal angiography
IVU
A 68-year-old man is involved in a traffic accident and sustains a pelvic fracture, head and limb injuries. Attempted urethral catheterisation in the Emergency Department is unsuccessful and a cystourethrogram is requested to exclude urethral injuries. Regarding urethral injuries, which one of the following statements is correct?
Cystography should precede a retrograde urethrogram in a patient with suspected urethral injury
Anterior urethral injury is more commonly due to iatrogenic or penetrating trauma than to blunt trauma.
Urethral injuries occur in 50% of major pelvic fractures.
In men, on digital rectal examination the prostate is lower than normal in patients with urethral trauma
Urethral injury due to blunt trauma more commonly affects the penile urethra
A 42-year-old man is referred for investigation of painless microscopic haematuria. An IVU is performed and demonstrates bilateral small areas of calcification within the kidneys on the control image. On the 5-min postcontrast IVU film, the calcification appears to lie within the collecting system. On ultrasound, there are numerous small hyperechoic rounded areas within the medullary pyramids, many of which cast an acoustic shadow. What is the most likely diagnosis?
Adult polycystic kidney disease
Hyperparathyroidism
Primary hyperoxaluria
Medullary sponge kidney
Sacoidosis
A 32-year-old man involved in a high-speed traffic accident is found to have blood at the urethral meatus and a high riding prostate during the secondary clinical survey. The examining doctor suspects a urethral injury. Which part of the urethra is most likely to be involved?
Membranous urethra
Bulbar urethra
Penoscrotal urethra
Penile urethra
Prostatic urethra
You are the radiologist reviewing the mammograms of a 56-year-old woman. When compared with her previous mammograms, areas of calcification previously seen within the left upper outer quadrant have now disappeared. Which of the following is not a possible explanation?
Chemotherapy
Breast surgery
Radiotherapy
Postmenopausal changes
Spontaneous resolution
A transvaginal ultrasound is performed on a 36-year-old woman with dysfunctional uterine bleeding. This demonstrates an enlarged globular uterus with a heterogeneous appearance of the myometrium. The myometrium contains diffuse echogenic nodules, subendometrial echogenic linear striations and 2- to 6-mm subendometrial cysts. Color Doppler demonstrates a speckled pattern of increased vascularity within the heterogeneous area of myometrium. What is the most likely diagnosis?
Endometrial polyposis
Adenomyosis
Stage 1A endometrial cancer
Gestational trophoblastic disease (GTD)
Uterine fibroid
A 52-year-old postmenopausal woman presents for her first screening mammogram. Within the right upper outer quadrant, there is a 2-cm well-defined, oval mass that has dense “popcorn” calcification within it and is surrounded by a thin radiolucent rim. On ultrasound, the mass is well defined and hyperechoic with areas of acoustic shadowing due to contained calcification. What is the most likely diagnosis?
Fibroadenoma
Fat necrosis
Oil cyst
Hamartoma
Papilloma
A 56-year-old woman is found to have a screen-detected breast cancer on her second screening mammogram. Two breast radiologists both agree that there is no evidence of malignancy on the previous mammograms, even in retrospect. Which one of the following statement best describes this interval cancer?
This is known as a Type 1interval cancer.
An interval cancer has a better prognosis, when compared with other screen-detected cancers.
This is known as a Type 2b interval cancer.
This is known as a Type 2a interval cancer.
This is known as a Type 3interval cancer.
A 42-year-old man with known Wegener’s granulomatosis develops haematuria. He has an abdominal ultrasound which reveals small, smooth kidneys with diffuse thinning of the renal parenchyma. The pelvicalyceal systems appear normal but there is an increased amount of renal sinus fat. What is the most likely diagnosis?
Chronic glomerulonephritis
Bilateral vesicoureteric reflux.
Pyelonephritis.
Medullary sponge kidney
Renal tuberculosis.
A 29-year-old man presents with a 4-hour history of sudden onset right loin pain, radiating to the right groin. The clinicians request an emergency IVU for suspected acute urinary obstruction. Which one of the following IVU features would be most consistent with acute urinary obstruction?
An increasingly dense right nephrogram that remains present after 6 hours
Absent right nephrogram and no evidence of contrast excretion on the right
The right kidney being 10% longer than the left kidney
An initially dense right nephrogram, which then resolves within 30 minutes
The right kidney being small with an irregular cortical surface.
A 35-year-old woman presents with a painless lump in the outer upper quadrant of her left breast. She is referred for an ultrasound examination of the left breast. Which of the following ultrasound findings would suggest a malignant rather than a benign breast mass?
A larger transverse than anterior-to-posterior diameter
Ill-defined echogenic halo around the lesion
Less than 1 cm in greatest diameter
Posterior acoustic enhancement
Uniform hyperechogenicity
An immunosuppressed 24-year-old man presents with left renal colic. He is referred for an IVU. The control film shows a gas containing, round lamellated mass within the urinary bladder. Postcontrast, there are multiple filling defects within the urinary bladder. What is the most likely cause of these appearances?
Bladder calculi
Blood clot
Fungal ball
Cystitis
Schistosomiasis
A 53-year-old woman is invited to attend a mobile breast-screening unit for routine screening mammograms. Which one of the following statements is correct regarding the standard mammographic projections (the mediolateral oblique (MLO) and craniocaudal (CC) views)?
A well-positioned MLO view rarely shows the nipple in profile because of the oblique compression.
A well-positioned CC view usually contains all the breast tissue.
The MLO view is taken with the radiograph beam directed from superomedial to inferolateral.
On a well-positioned MLO the nipple should be at the lower border of the pectoralis minor.
The pectoralis major muscle is demonstrated at the posterior border of a CC view in approximately 70% of individuals.
A 24-year-old man presents to his GP with increased urinary frequency. Physical examination is normal and he is referred for ultrasound. Transabdominal ultrasound demonstrates a cystic structure posterior to the urinary bladder and a TRUS is performed for further evaluation. TRUS reveals a midline anechoic structure in the posterior portion of the prostate gland, superior to the verumontanum. It does not communicate with either the bladder or the seminal vesicles. Which of the following is the most likely diagnosis?
External iliac artery aneurysm
Bladder diverticulum
Seminal vesicle cyst
Mullerian duct cyst
Urethral cyst
A 22-year-old woman presents to her GP with irregular menstrual periods. She is overweight with a body mass index of 32 and has excess body hair. Her LH/FSH ratio is elevated and her GP refers her for a pelvic ultrasound. Which one of the following findings are most likely to be present on ultrasound?
Enlarged ovaries with multiple peripheral cyst
Enlarged, oedematous ovaries with multiple packed follicles and pelvic-free fluid.
Ovarian mass with mixed cystic and solid components
Normal appearances of the ovaries
Ovaries replaced by multiple large cyst
A 5-year-old boy who had a coarctation of his aorta repaired 12 months ago requires follow-up. Which of the following imaging modalities is the gold standard?
CT
Which of the following imaging modalities is the gold standard? Conventional angiography
MRI
Echocardiogram
Plain radiograph
A 6-year-old boy presents with a right-sided limp of a few weeks’ duration. He is apyrexial. Which one of the following is the earliest radiographic sign that would support a diagnosis of Perthers’ disease of the hip?
Fragmentation of the femoral head
A subchondral lucency
Periarticular osteopenia
Hip effusion
Sclerosis of the femoral head
A 2-year-old has an elbow radiograph performed following a fall. Which one of the following epiphyses should be visible?
Medial epicondyle
Capitellum
Olecranon
None
Radial head
On a 20-weeks antenatal ultrasound, unilateral fetal hydronephrosis is detected. Which one of the following findings would confirm the diagnosis of renal pelvic dilatation (RPD)?
During the third trimester, the AP renal pelvis measures greater than 5 mm
During the second trimester, the AP renal pelvis measures more than 3 mm
The AP renal pelvis measures greater than 25% of the longitudinal length of the kidney
Megaureters are present.
The AP renal pelvis measures greater than 50% of the longitudinal length of the kidney
A 2-week-old septic neonate shows worsening renal function and proteinuria. He is currently being monitored on the pediatric ITU. Seven days after his initial illness, an ultrasound is performed which reveals a unilateral enlarged kidney, with loss of corticomedullary differentiation and reversal of end diastolic arterial flow. Associated adrenal haemorrhage is noted. What is the most likely diagnosis?
Acute tubular necrosis
Acute glomerulonephritis
Renal vein thrombosis
Renal artery stenosis
Unilateral obstruction
A 2-year-old child presents to Emergency Department with a greenstick fracture of the ulna. On the radiograph, there is evidence of an old fracture to the same limb and the history given by the parents is inconsistent. Non-accidental injury (NAI) is clinically suspected and a skeletal survey is performed. Which of the following fractures have a high specificity for NAI?
Fracture of the middle third of the clavicle.
Fractures of multiple ages
Linear skull fracture
Fracture of the lateral third of the clavicle.
Spiral humeral fracture.
A 33-year-old HIV-positive woman presents with increasing headache and confusion. On examination she is pyrexial and has left leg and right facial weakness. A CT head demonstrates multiple lesions measuring between 2 and 4 cm, which are predominantly situated at the corticomedullary junction. These lesions have a thin enhancing rim as well as associated oedema and local mass effect. Which one of the following is the most likely diagnosis?
Histiocytosis
Cryptococcosis
Multiple cerebral metastasis
HIV encephalopathy
Toxoplasmosis
A GP requests your advice regarding an 18-month-old girl whose mother has noticed that her left pupil appears white. The GP has performed ophthalmoscopy and is suspicious that there is a retinal mass. Which one of the following is the investigation of choice?
CT orbits
MRI orbits
Repeat ophthalmoscopy by ophthalmologist
Orbital radiographs
Ultrasound
A 19-year-old HIV-positive man is admitted with headache, confusion and disorientation. He is mildly pyrexial. A CT brain reveals multiple hypodensities, particularly in the brainstem and in the periventricular white matter. There is some ependymal enhancement postcontrast. What is the most likely cause for these findings?
Cryptococcosis
CMV encephalitis
Toxoplasmosis
HIV encephalitis
Tuberculosis
A 37-year-old woman is involved in a road traffic accident and sustains a severe head injury. Her CT head shows acute blood within the extradural, subdural and subarachnoid spaces. Which one of the following statements is true regarding extradural haematomas?
They are commonest in the temporoparietal region
They are crescentic is shape
They are usually due to laceration of the middle cerebral artery
They are rarely associated with a skull fracture
They commonly cross the cranial sutures
A 50-year-old man has a CT head after sustaining a head injury during a mechanical fall. The only positive finding is a large low attenuation lesion in the left middle cranial fossa, which is well defined, and of the same attenuation as cerebrospinal fluid (CSF). There is some thinning of the overlying temporal bone. Which one of the following is the most likely diagnosis?
Cerebral infarct
Arachnoid cyst
Dermoid cyst
Colloid cyst
Epidermoid cyst
190) Un patient de 60 ans vient vous voie pour un nodule hépatique sur l’échographie qui évoque un foie d’aspect granuleuse. Quel est votre aptitude pour la démarche diagnostic devant une suspicion de CHC?
Alpha-foetoprotéine, bilan hépatique complet.
Scanner avec infection en 3 temps, Alpha-foetoprotéine, rechercher infection virale.
Bilan de fonction hépatique et Alpha-feotoprotéine.
Ponction biopsie hépatique, bilan pour recherche la possibilité d’origine autre primitive.
Rechercher infection virale, Alpha-foetoprotérine, bilan de fonction hépatique complet.
Chez un patient présentant une fibrillation auriculaire d'installation récente et anticoagulé de manière efficace par anti-vitamine K au long court, quelle situation constitue une contre-indication au choc électrique externe?
Un rétrécissement mitral
Un traitement par Cordarone
Une hyperthyroïdie évolutive
Une mauvaise tolérance hémodynamique
Des antécédents d'infarctus du myocarde
Un patient d’une cinquantaines d’années est vu 1h00 après le début d’une douleur thoracique infarctoïde. A l’ECG, il existe un sus décalage de ST en inférieur. La tension est à 9/6, la fréquence cardiaque à 50/mn, les jugulaires sont turgescentes, il n’y a pas de crépitant à l’auscultation pulmonaire. Les médicaments suivants, sauf un, sont prescrits, selon la voie d’administration appropriée, pendant la phase pré hospitalière:
Aspirine
Héparine
Morphine
Atropine
Trinitrine
Un homme de 60 ans, hypertendu traité de longue date, diabétique et dyslipidémique se présente au SAU suite à une violente douleur transfixiante rétrosternale à irradiation interscapulaire. A son arrivée, le patient souffre toujours et est agité. Vous constatez un coeur rapide à 100/minute, la pression artérielle est à 160/95 mais le reste de votre examen clinique est normal. Son ECG est subnormal, hormis un discret sous-décalage du segment ST en V4-V6. L'examen complémentaire que vous prescrivez en urgence est:
Un dosage des marqueurs biologiques de l'infarctus du myocarde
Une coronarographie
Un scanner thoracique
Un prélèvement pour mesure des gaz du sang
Une échocardiographie trans-thoracique
Lors d'un IDM de topographie inférieure, on observe une chute de la pression artérielle à 80/50 mmHg, une bradycardie sinusale à 40/min, des sueurs et des nausées. L'auscultation pulmonaire est normale. Parmi les mesures thérapeutiques suivantes, laquelle retiendrez-vous en priorité?
Perfusion d'un soluté glucose 10%
Injection d'Isuprel IV
Digoxine IV, 1 ampoule
Atropine 1 mg IV
Mise en place d'une perfusion de TNT
Chez une femme enceinte de 8 mois, vous avez la certitude d'une thrombose veineuse fémorale sans embolie pulmonaire. Quelle thérapeutique préconisez-vous dans l'immédiat?
Héparinothérapie
Antivitamines K avec doses de charge
Traitement thrombolytique
Antiagrégants plaquettaires
Interruption de la veine cave inférieure
Un patient de 60 ans, souffrant de silicose, a par ailleurs des épisodes de palpitations fréquents, prolongés et invalidants, par fibrillation auriculaire paroxystique. L’un des antiarythmiques ci-dessous est contre-indiqué. Lequel?
DISOPYRAMIDE (RYTHMODAN®)
VERAPAMIL (Isoptine®)
HYDRO QUINIDINE « retard » (Sérécor®)
AMIODARONE (Cordarone®)
FLECAINIDE (Flécaïne)
Ms T, 20 year-old, is admitted to the emergency of a nationa hospital. She has DKA. The arguments below are the severity cryteria except one.
Bicarbonate < 10 mmol/l
PH < 7
Conscience normal
K < 2.5 mmol/l or > 7 mmol/l
Coma
Mr B. 65 ans, est adressé aux urgences par son médecin traitant. Il a aimablement joint une lettre: “Cher confère, merci de prendre en charge Mr B., qui présente une hypercalcémie à 3,05 mmol/L, chez qui je suspecte une hyperparathyroïdie primitive. Quelle atteinte met en jeux le prognostic vital?
Rénale
Hépatite
Cardiaque
Cérébrale
Respiratoire
Mr B. 65 ans, est adressé aux urgences par son médecin traitant. Il a aimablement joint une lettre: “Cher confère, merci de prendre en charge Mr B., qui présente une hypercalcémie à 3,05 mmol/L, chez qui je suspecte une hyperparathyroïdie primitive. Quel médicament peut donner d’hypercalcémie?
Anti-inflammatoires
Antibiotiques
Biphosphonates
Litium
Calcitonine
Mr B. 65 ans, est adressé aux urgences par son médecin traitant. Il a aimablement joint une lettre: “Cher confère, merci de prendre en charge Mr B., qui présente une hypercalcémie à 3,05 mmol/L, chez qui je suspecte une hyperparathyroïdie primitive. Quel est le traitement d’une hypercalcémie moderée?
Hydratation IV
Hydratation PO
Corticothérapie PO en cas de cause maligne
Biphosphonate PO
Diurèse forcée au Lasilix
A 50-year-old woman presents to accident and emergency complaining of excessive lethargy. In addition, she mentions that she has been constipated. On examination, there are clinical features of dehydration. Blood tests have revealed corrected calcium of 3.3 mol/L. Her chest x-ray shows bilateral streaky shadowing throughout both lung fields. She is given 3 L of saline in 24 hours after admission. The following day her blood tests are repeated and her corrected calcium level is now 3.0 mmol/L. Results of parathyroid hormone levels and thyroid function tests are still awaited. What is the most appropriate management?
Intravenous saline rehydration and pamidronate
Intravenous saline rehydration
Pamidronate
Calcitonin
Intravenous saline rehydration plus calcitonin
A 66-year-old man with known metastatic squamous cell carcinoma of the esophagus is brought to the emergency room for increasing lethargy and confusion. He is clinically dehydrated, his serum calcium level is 14 mg/dL, and his creatinine level is 2.5 mg/dL but 1 month ago was 0.9 mg/dL. Which therapy for his hypercalcemia should be instituted first?
Intravenous furosemide
Intravenous bisphosphonate
Intravenous normal saline
Glucocorticoids
Chemotherapy for squamous cell carcinoma
Un patient âgé de 66 ans est hospitalisé pour une hématémèse. A l'interrogatoire, vous notez qu'il a de l'hématémèse 3fois. Comme l'antécédent: l'infarctus du myocarde il y a 3mois. A l'examen clinique: TA: 98/72mmHg, FC: 100/mn, absence de marbrure. Quel critère de gravité de ce patient que vous inquiétez le plus?
Co-morbidité du patient
Age du patient
Etat hémodynamique
Nombre de l'hématémèse
Cause de l'hémorragie
Le 16/11/2014, 20h40, Vous êtes interne au service urgence porte d’un hôpital à Phnom Penh. Monsieur C.V, âgé de 53 ans amené par son fils pour une émission de selle noirâtre une fois à 17 heures. 20h45, l'hémorragie digestive est confirmée après votre examen. La tension artérielle est à 80/40mmHg, FC 110/mn, FR 22/mn, SpO2 96% en air ambiant, la température à 370C, Glasgow 15. Vous reprenez votre interrogatoire minutieux, vous avez noté que c’est le premier épisode de méléna. Il n’en a pas de l’antécédent médical, chirurgical ou familial connu. Il n'a jamais pris de médicament. Il n’a pas d’allergie connue. Il fume 1 paquet par jour et il boit du vin du riz 1 litre par jour depuis l’âge de 30 ans. A l'examen clinique, vous avez trouvé des angiomes stellaires, circulation veineuse collatérale avec ictère conjonctival. Quel type de médicament le plus utile prescrivez-vous pour ce patient?
Vaso-actif
Bêtabloquant
Inhibiteur de la pompe à protons
Hémostase systémique
Antifibrinolytique
Le 16/11/2014, 20h40, Vous êtes interne au service urgence porte d’un hôpital à Phnom Penh. Monsieur C.V, âgé de 53 ans amené par son fils pour une émission de selle noirâtre une fois à 17 heures. Le lendemain, le patient allait mieux. Il n'existe pas de désorientation temporo-spatiale. A l'examen clinique vous trouvez de l'ictère, des angiomes stellaires, d'ascite de moyenne abondance avec des circulations veineuses collatérales. Le bilan biologique: Hb: 80g/L, VGM : 84,7 fl, GB : 8,39giga/l, Plaquettes : 85 giga/l. Transaminase: ASAT: 3 fois à la normal et ALAT: 2 fois à la normal. Urée et créatinine sanguine sont normales. L'échographie a confirmé la cirrhose du foie chez ce patient. Votre sénior vous demande de faire le bilan biologique pour calculer le score de Child-Pugh. Quel est la proposition la plus appropriée pour calculer ce score?
Taux de prothrombine, Bilirubine total, Albumine sérique
Alpha foeto-protéine, INR, Albumine
INR, Bilirubine totale, Taux de prothrombine
Alpha foeto-protéine, Taux de prothrombine, Bilirubine totale
Taux de prothrombine, Bilirubine total, Albumine de liquide d'ascite
Vous faite la visite matinale avec votre senior, vous s'occuper d'une dame de 54ans ayant la pancréatite chronique. La patiente a des vomissements répètes, Ceux-ci sont dues aux complications de la pancréatite chronique. Quelle complication la plus probable est responsable de vomissements répétés chez cette patiente?
Destruction de la cellule bêta
Carence de la vitamin
Douleur pancréatique
Destruction de la cellule exocrine
Pseudo-kyste du pancréas
A 73 year old man presents with several episodes of hematemesis. Examination shows signs of orthostatic hypotension and melena. What is the first priority in caring for this patient?
Resuscitation with adequate IV access and appropriate fluid and blood product fusion.
Nasogastric tube placement and gastric lavage.
Urgent upper panendoscopy.
Intravenous infusion of H2-receptor antagonists to stop the bleeding.
Urgent surgical consultation.
A fifty-eight year old female patient presents to the emergency department in Calmette hospital with a 24-hour history of several hematochesia. Physical examination show: hypotension, and anemia. Both the upper endoscopy and colonoscopy are not diagnostic. The patient continues to pass clots per rectum. Resuscitation has normalized her vital signs and maintained her Hct at 32%. What is the most effective management strategy?
Magnetic resonance imaging
Abdominal CT scan with contrast
Emergency surgery with intraoperative enteroscopy
Scintigraphy and angiography
Barium enema
Un home de 50 ans, obèse, vient vous voir en consultation spécialisé pour une vésicule de porcelaine ayant découverte fortuitement sur un bilan de santé. Il est complètement asymptomatique. Son médecin lui demande d’opérer, mais il a peur de l’opération. Il veut savoir votre avis. Quel est le risque s’il n’opère pas ?
Angiocholite lithiasique
Cholécystite aiguë lithiasique
Abcès du foie
Pancréatite aiguë
Cancer de la vésicule biliaire
Chez un malade adulte en état de choc hypovolémique par déshydratation suite à des pertes digestives, quel est le principe de votre expansion volémique initiale ?
10 à à 15 ml/kg de cristalloïdes / 20 minutes
1 à à 1,5 ml/kg de cristalloïdes / 20 minutes
1 à à 1,5 ml/kg de colloïdes / 20 minutes
100 à 150 ml/kg de cristalloïdes / 20 minutes
100 à 150 ml/kg de colloïdes / 20 minutes
Vous réalisez une RCP de base chez un patient en ACC. Dans quel ordre réalisez-vous les gestes ? A = Airways (LVAS) ; B = Breathing = ventilation ; C = Circulation = MCE
B-C-A
A-B-C
C-A-B
B-A-C
C-B-A
Monsieur D, 65 ans, sans antécédents connus, est adressé aux urgences pour somnolence d’apparition progressive depuis 48 h. Les examens sanguins montrent : Na⁺ = 130mmol/L, K⁺ = 7.6mmol/L, Cl = 110mmol/L, Bicarbonates = 18mmol/L, urée = 1.45g/L, créatinine = 1425μmol/L, Hb= 75g/L, GB = 9.2giga/L, plaquettes = 280giga/L, CRP = 45mg/L. Parmi les anomalies métaboliques suivantes, laquelle nécessite le traitement immédiat ?
Hyperkaliémie
Hyponatrémie
Insuffisance rénale
Acidose métabolique
Anémie
Un homme de 55 ans aux antécédents de diabète de type 2 et HTA sous biguanides et IEC est admis en urgence pour détresse respiratoire aiguë. Constantes : PA = 170/100mmHg, FC = 98/min, T = 37°C, FR = 30/min et SpO2 = 90% en air ambiant. Le bilan biologique montre une insuffisance rénale aiguë : urée = 1.5 g/L, Créatinine = 780 μmol/L, Ca = 80 mg/L (2 mmol/L), HCO3 = 18 mmol/L, K = 7.5 mmol/L, diurèse = 400 ml/24h. Parmi les complications cliniques et biologiques ci-dessus, laquelle nécessite l’indication d’épuration extra-rénale en urgence ?
Hypocalcémie
Hypertension artérielle
Hyperkaliémie
Acidose métabolique
Oligo-anurie
Mademoiselle D, 18 ans, sans ATCD connu, est amenée aux urgences pour état confus. L’examen clinique retrouve : PA = 115/85 mmHg, T= 38,9°C, fréquence cardiaque à 110/min et fréquence respiratoire à 25/min. Pas de signe de localisation en examen neurologique. L’auscultation cardio-respiratoire est sans particularité. Le gaz du sang montre : Na = 132 mmol/L, K = 5,5 mmol/L, chlore = 102 mmol/L, Bicarbonates = 8 mmol/L, pH artériel = 7, pCO2 = 18 mmHg, pO2 = 110 mmol/L et Hb = 125 g/L. La bandelette urinaire montre : sang (-), protéines traces, leucocytes +++, nitrites +, cétones +++, glucose +++. La glycémie capillaire : Hi. Quel est l’ensemble des actes thérapeutiques en urgence pour sauver cette malade ?
Insuline rapide IV continue, réhydratation et ATB contre bacilles gram (-)
Insuline rapide IV continue, restriction hydrique et ATB contre bacilles gram (-)
Insuline rapide IV continue, réhydratation et ATB contre bacilles gram (+)
Insuline rapide IV continue, restriction hydrique et ATB contre bacilles gram (+)
Insuline rapide IV continue, réhydration et ATB contre bacilles gram (-) et (+)
Monsieur M, 60 ans, est adressé aux urgences pour altération de l’état général. Il est hypertendu, suivi régulièrement par son médecin traitant. Il présente depuis trois jours des diarrhées liquides. A l’examen clinique, la pression artérielle est à 90/60 mmHg, la fréquence cardiaque à 130/min. Le patient a perdu 3 kg depuis le début des diarrhées. L’auscultation cardiaque et pulmonaire est sans particularité. L’examen abdominal révèle une sensibilité diffuse, sans défense ni contracture. Il présente de légères marbrures, un pli cutané persistant et réclame toutes les 15 minutes un verre d’eau. Il est apyrétique. Le bilan biologique montre : urée = 1.65mg/L, créatinine = 210μmol/L, Bicarbonate = 17 mmol/L, Na⁺ = 152mmol/L, K⁺ = 7.2 mmol/L, calcémie = 86 g/L, phosphore = 35 mg/L, albuminémie = 50g/L. La numération globulaire est sans particularité. Le bilan biologique réalisé il y a trois mois était sans particularité. Sa diurèse des 12 dernières heures est évaluée à 200ml. Quel sera votre traitement en urgence ?
Kayexalate
Bicarbonate de sodium
Antibiothérapie
Bétabloquant
Furosemide
Monsieur M, 60 ans, est adressé aux urgences pour altération de l’état général. Il est hypertendu, suivi régulièrement par son médecin traitant. Il présente depuis trois jours des diarrhées liquides. A l’examen clinique, la pression artérielle est à 90/60 mmHg, la fréquence cardiaque à 130/min. Le patient a perdu 3 kg depuis le début des diarrhées. L’auscultation cardiaque et pulmonaire est sans particularité. L’examen abdominal révèle une sensibilité diffuse, sans défense ni contracture. Il présente de légères marbrures, un pli cutané persistant et réclame toutes les 15 minutes un verre d’eau. Il est apyrétique. Le bilan biologique montre : urée = 1.65mg/L, créatinine = 210μmol/L, Bicarbonate = 17 mmol/L, Na⁺ = 152mmol/L, K⁺ = 7.2 mmol/L, calcémie = 86 g/L, phosphore = 35 mg/L, albuminémie = 50g/L. La numération globulaire est sans particularité. Le bilan biologique réalisé il y a trois mois était sans particularité. Sa diurèse des 12 dernières heures est évaluée à 200ml. Quelle est l’indication à l’hémodialyse en urgence ?
Elévation de la créatinine
Elévation de l’urée
Hyperkaliémie menaçante
Acidose métabolique
Oligo-anurie
Monsieur M, 60 ans, est adressé aux urgences pour son médecin traitement pour hypercalcémie à 120mg/L. Quel est le traitement d’une hypercalcémie sévère ?
Hydratation IV
Hydratation PO
Calcitriol
Kayexalate
Furosémide
Un homme de 50 ans est amené aux urgences pour crise convulsive avec perte de conscience 30 minutes auparavant. A l’arrivée il est confus et agité. Sa famille a signalé trois crises pendant les dix dernières années. Quel est votre prise en charge initiale pour ce patient?
EEG en urgence
Scanner cérébral en urgence
Glycémie capillaire
Diazépam en IV
Antiépileptique tout de suite
Vous êtes de garde aux urgences. Vous avez été appelé pour une céphalée aiguë modérée sans net soulagement par Doliprane 1g. L’examen physique retrouvait PA 130/70 mmHg, FC 90/min, T°37,2, FR 20/min, SpO2 98% en air. L’examen neurologique est sans particularité, notamment : conscience bonne, pas de raideur méningé, ni d’atteinte des paires crâniennes. Autres appareils sont normaux. Concernant la stratégie d’examens paracliniques, quel est votre premier choix?
Ponction lombaire en urgence pour éliminer une hémorragie sous arachnoïdienne
Scanner cérébral en urgence sans produit de contraste
Surveillance clinique sans examen complémentaire en urgence
Scanner cérébral avec injection pour augmenter la sensibilité
Réaliser une IRM cérébrale à H+10 pour rechercher un anévrisme
M. H. Chan 72ans, 1m65, 79kg, droitier, consulte au service de neurologie à 10h15 du 26 Juin 2016 pour troubles de la parole depuis ce matin. Dans ses antécédents, on retrouve un diabète de type II depuis plus 5 ans, un tabagisme actif à deux paquets par jour, une dyslipidémie. Il ne suit aucun traitement régulier. Au cours des 3 dernières semaines, avant, vous apprenez qu’il a également présenté une perte vision de l’oeil gauche à deux reprises, épisodes entièrement résolutif en moins de 24heures.C’est sa femme qui vous explique ce qui est arrivé à M.H.Chan. Au réveil à 6h20 de même jour sans facteur déclenchant, il a présenté des troubles de la parole à type de manque du mot, apparu brutalement. A l’interrogatoire, il semble comprendre ce que vous lui demandez, et il énerve de ne pas trouver ses mots. De plus vous notez une faiblesse de l’hémicorps droit, prédominant au niveau brachio-facial. L’auscultation cardio-pulmonaire est sans particularité. La pression artérielle est à 185/90 mmHg. Quel l’examen à réaliser en urgence?
Scanner cérébral non injecté
IRM Encéphalique
Echo-Doppler trans crânien
Artériographie cérébral
IRM cérébral
Une jeune femme vendeuse de 23 ans venant de Takeo étant diagnostiquée un lupus érythémateux systémique grave est hospitalisé dans un service de réanimation. Ses symptômes ont commencé depuis 6 mois avec quelques épisodes de rémission sans traitement particulier. Elle a un antécédent de pneumonie bactérienne il y a six ans. Parmi Ces symptômes suivants, lequel évoquez-vous la gravité de votre patiente ?
Amaigrissement
Fièvre à 38 C
Chute des cheuveux
Convulsion
Polyarthite chronique
Vous avez diagnostiqué une goutte chez un patient de 45 ans venant de Kampong Thom devant une arthrite du genou droit avec hyperuricémie à 98 mg/L. Quelle est une complication grave et fréquente de la goutte ?
Insuffisante rénale aiguë
Insuffisance rénale chronique
Hypertension artérielle
Anémie chronique
Trouble hydro-électrolytique
Une femme ménagère de 50 ans venant de Kampong Cham vient vous voir pour une induration scléreuse des teguments évoluée depuis 9 mois. En basant sur les critères diagnostiques d’ARA en 1980, une sclérodermie systémique est diagnostiquée. Quel est un argument en faveur d’une gravité de cette maladie ?
Atteinte musculaire
Atteinte articulaire
Atteinte hépatique
Atteinte oesophagienne
Atteinte rénale
Un patient de 30 ans venant de Kandal vient vous consulter pour lombalgies inflammatoires, arthrite des deux genoux, de la cheville gauche, du poignet droit et uvéite bilatérale évoluées depuis 4 mois. Le diagnostic de spondylarthrite ankylosante est suspecté. Le bilan initial montre hémoglobine 12g/dl, leucocytes 18000/mm³, plaquette 658 000/mm³, VS 60 mm à la première heure, CRP 110 mg/L et HLA-B27 positif. Parmi les propositions suivantes, laquelle représente la gravité de cette maladie ?
Atteinte extra-articulaire
Atteinte poly-articulaire
Importance du syndrome inflammatoire
Importance de l’hyperplaquettose
Positivité de HLA-B27

Vous recevez un home âgé de 57 ans, pour une dyspnée fébrile. Il est dyspnéique, se plaint d’une toux non productive et de douleurs thoraciques postérieur droite apparues en même temps que la fièvre qui était d’emblée à 39,9°C depuis 24 heures. Son élève qui l’emmène à l’hôpital dit qu’il a une diarrhée et une fébrile. A l’examen : fréquence respiratoire à 32/min, TA à 90/50 mmHg, la fréquence cardiaque à 137 par min, la température à 39°C, SpO2 à 87% en air ambiant. Le score de Glasgow est à 13, perte de conscience pendant le transport, râles crépitants bi basales. Dentition en mauvais état. ECG : rythme régulier et sinusal, tachycardie à 128. La biologie : créatininémie 80 μmol/L; Na 138 mEq/L; Cl 100 mEq/L; K 3.1 mEq/L; glucose 0,8g/L; CRP 125 mg/L; GB 12 800 103/ml; PNN : 9500 103/ml; D-dimères 500 ng/ml. Quel critère le plus important selon le score Pneumonia Severity Index ?
Le score de Glasgow à 13
Son âge
L’isolement social
Le risque d’inobservance
Le sexe féminin
Vous êtes interne du 1er année, appelé au lit d’un patient de 53 ans aux antécédents de broncho-pneumopathie chronique obstructive (BPCO) qui présente une déstresse respiratoire aigu (DRA) avec des signes d’arrêt cardio respiratoire (ACR) imminent. Le conscience somnolence, la tension artérielle 96 /56 mmHg, la fréquence cardiaque 143 par min, la fréquence respiratoire 32/min L’examen: distension thoracique, silence auscultatoire, tympanisme unilatéral. Vous suspectez à un pneumothorax. Quel est votre prise en charge en urgence ?
Vous réalisez une exsufflation dans le 2 espace intercostal
Vous demandez une radiographie thorax en urgence avant d’exsuffler
Vous appelez un réanimateur pour exsuffler le pneumothorax
Vous augmentez l’oxygénothérapie 2 à 6 litres/min
Vous vérifiez la coagulation avant d’exsuffler
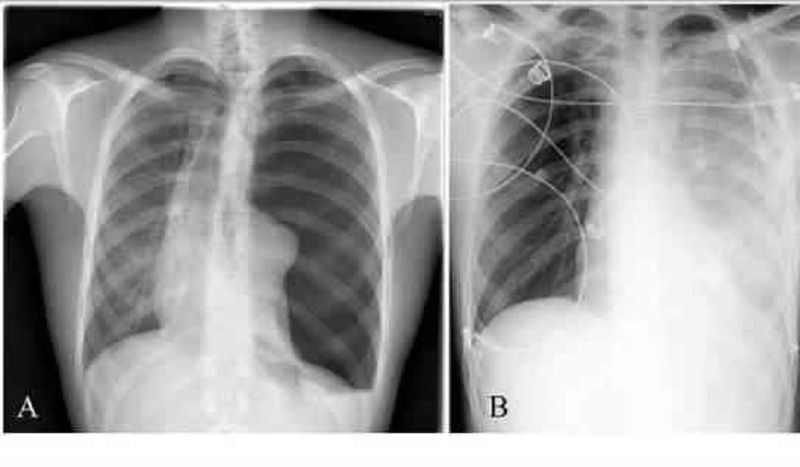
A 67 year-old-man with chest pain and dyspnea. The chest radiography showed findings suggestive of the left tension pneumothorax (The Figure A). Thoracentesis in the aspiration. 4 hours later coughing and had tachypnea and tachycardia, with right lung crackles heard on physical examination. The SaO2 82% roomt air. The (Figure B) chest x ray post procedure: near-immediate reexpension of the lung with new infiltrates in the whole lung. What is the diagnosis most likely complicate post procedure?
Reexpension pulmonary edema
Hospital acute pneumonia
Intra alveolar haemorrhages
Left pleural effusion
Right tension pneumothorax
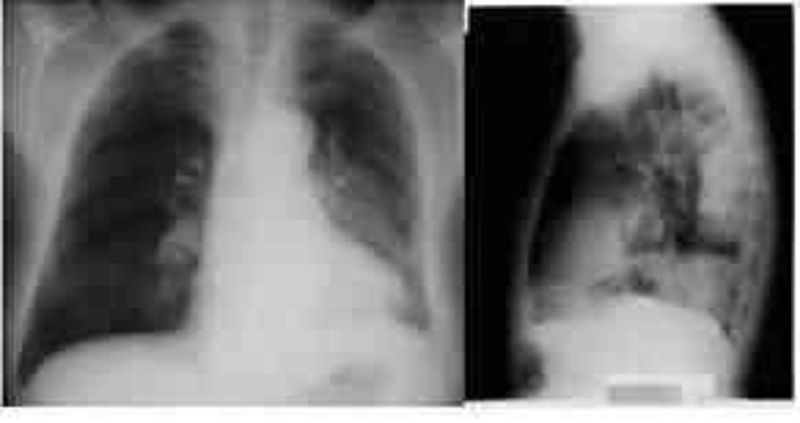
Vous recez en hospitalisation d’un homme âgé 60 ans a le métier à risque la maladie professionnelle. Il vous dit qu’il touche depuis 6 mois et la dyspnée au moins d’effort a remonté à 2 semaines et douleurs basithoracique gauche. La conscience normal, la tension artérielle 120/67 mmHg, la fréquence cardiaque 120 par min, la fréquence respiratoire 14/min et la murmure vésiculaire diminuée et diminution vibration vocale à côté gauche. Le cliché de radiographie du thorax face et profil ci-joints. Quelle est la pathologie professionnelle non cancéreuse liée à l’amiante?
Pneumopathie d’hypersensibilité
Plaques pleurales
Adénocarcinome pulmonaire
Mésothéliome pleurale
Hémorragie alvéolaire
Vous recevez un homme de 49 ans pour toux aiguë et dyspnée. Il ne fume pas. Il a un métier identifié. Le symptôme a brutalement apparu pendant l’exposition au travail. Tension artérielle 120/76 mmHg, la fréquence respiratoire 28 par min et SpO2 92 % en air ambiant. Vous pensez à une pneumopathie professionnelle. Quel profession exposé le plus risqué en faveur une complication d’une pneumopathie d’hypersensibité?
Coiffeurs
Fermiers
Peintres industriels
Employés des piscines
Prothésistes

Vous recez en hospitalisation d’un homme âgé 60 ans a le métier à risque la maladie professionnelle. Il vous raconte d’apparition la toux et dyspnée brutale, pas de bronchospasme et associé à un syndrome pseudo grippal. Le cliché de radiographie du thorax ci-joint. Quel est le secteur d’activité est principalement responsable des pneumopathies d’hypersensibilités d’origine professionnelle?
Secteur minier
Secteur agricole
Secteur textile
Secteur bâtiment
Secteur automobile
Vous recevez une femme de 45 ans en hospitalisation pour fièvre prolongée avec abcès du coude. Elle n’a pas d’antécédent particulier. Vous avez effectué un prélèvement du pus abcédée et labo vous appel la présence de Burkholderia pseudomallei, donc votre diagnostic mélioïdose confirmée. Quelle est la complication la plus souvent rencontrée chez un sujet atteinte une Mélioïdose?
Surinfection
Hémoptysie
Guérison
Choc septique
Rechute
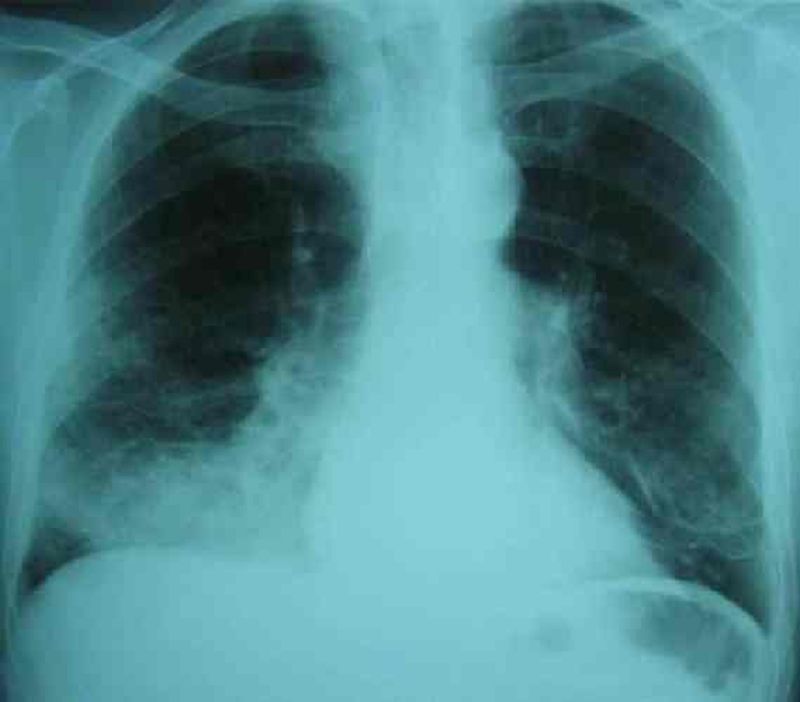
Vous êtes appelé en réanimation traumatologie au sujet de jeune homme âgé de 18 ans a été traumatisme crânien avec coma profonde. Ce patient a été bénéficié une intubation endotrachéale dès à l’admission. Au bout de 10 jours de l’intubation, la fièvre 38,8°C apparue et la sécrétion endotrachéale devenue verdâtre. Le cliché de radiographie thoracique ci-joint. Vous pensez à une pneumonie nosocomiale tardive. Quel est le taux mortalité d’une pneumonie nosocomiale de ce patient?
Mortalité : 20 %
Mortalité : 10 %
Mortalité : 50 %
Mortalité : 30%
Mortalité : 60 %

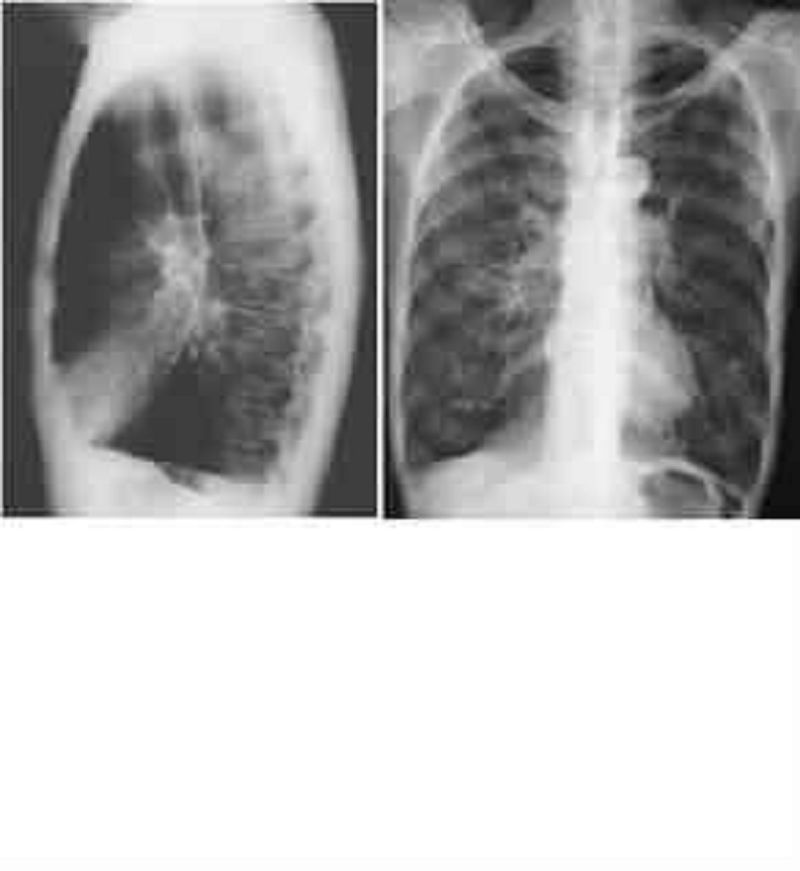
A 67-year-old-man with advanced alcoholic cirrhosis, progressive dyspnea, chest radiography showed findings suggestive of a large right pleural effusion (Panel A). Thoracentesis in the aspiration of 1500 ml 4 hours later coughing and had tachypnea and tachycardia, with right lung crackles heard on physical examination. The SaO2 82% ambiant air. The CT of the chest: diffuse areas of consolidation and ground-glass opacity in the right lung reexpansion pulmonary edema (Panel B).What is the mechanism this lung edema most likely ?
Decreased microvascular oncotic pressure
Increased microvascular hydrostatic pressure
Increased permeability of capillaries
Obstruction to lymphatic drainage
Decreased interstitiel space pressure
Vous recevez un homme de 57 ans aux urgences pour dyspnée intense et fébrile. Il a principal antécédent bronchite chronique post tabagique connu et diabète sucré type 2 avec traitement irrégulier depuis 2 ans. La maladie a remonté il y a 12-24 heures : dyspnée intense avec fièvre 39,7°C et frisson. Vous trouvez le patient est en état réanimation. Quelle est l’indication d’assistance ventilatoire ?
Respiration de Cheyne-Stokes
Respiration superficielle rapide
Respiration par bouche ouverte
Respiration d’hyperventilation
Respiration abdominale paradoxale
Un patient de 65 ans, vous consulte pour toux et altération de d’état général depuis 2 mois. Il a une tuberculose avec traitement irrégulier il y a 1 an. Il se plaint aussi d’asthénie intense avec dyspnée au repos. Il ne fume pas. Le contrôle 2eme mois BAAR positive. Quel est votre prise en charge en charge en 1er intension?
Examiner coloration urine
Compter les pilules
Education therapeutique
Dosage acide urique sanguine
Direct observe therapy
Une patiente de 59 ans cuisinière, vit avec la famille, vous suivez pour une bronchopneumopathie chronique obstructive (BPCO) biomasse consulte aux urgences pour une dyspnée d’apparition progressive. Vous évoquez donc une exacerbation bronchopneumopathie chronique obstructive (BPCO). Cliniquement, vous trouvez une légère cyanose des extrémités et des sueurs, fréquence respiratoire : 26/min, la tension artérielle 140/90 mmHg, la fréquence cardiaque : 90 par min. Les premiers gaz du sang sont les suivants : pH : 7,30 PaCO2 50 mmHg, PaO2 : 56 mmHg, HCO3 : 29 mmol/l. Quelle est la condition plus importance probable hospitaliser cette patiente?
Sans comorbidités associé
Vit avec la famille
Maladie chronique
Signes de gravités
Sujet âgé plus de 60 ans
Une patiente de 62 ans cuisinière, vit seule sans famille, vous suivez pour une bronchopneumopathie chronique obstructive (BPCO) biomasse stade 3 GOLD, consulte aux urgences pour une dyspnée d’apparition progressive. Vous évoquez donc une exacerbation bronchopneumopathie chronique obstructive (BPCO). Cliniquement, vous trouvez une légère cyanose des extrémités et des sueurs, la fréquence respiratoire : 26/min, la tension artérielle 140/90 mmHg, la fréquence cardiaque : 90 par min. Quelle est la complication possible de cette maladie?
Emphysème pulmonaire
Cancer du sein
Pleurésie
Cardiopathie embolie gène
Insuffisance respiratoire restrictive
Une patiente de 62 ans cuisinière, vit seule sans famille, vous suivez pour une bronchopneumopathie chronique obstructive (BPCO) biomasse stade 3 GOLD, consulte aux urgences pour une dyspnée d’apparition progressive.Vous évoquez donc à une exacerbation une bronchopneumopathie chronique obstructive (BPCO). Cliniquement, vous trouvez une légère cyanose des extrémités et des sueurs, fréquence respiratoire : 26/min, la tension artérielle 140/90 mmHg, la fréquence cardiaque : 90 par min. Quel est le facteur de risque de decompensation necessite hospitalisation en reanimation?
Tabagisme sevré
Dyspnée expiratoire
Insuffisance respiratoire chronique
Prise de β2 mimétique de long d’action
Plus une exacerbation par an
Vous recevez aux urgences Melle. X., 22 ans, pour une dyspnée aigue. A l’examen clinique, vous trouvez des sibilants diffus, ainsi qu’une cyanose. Les constantes sont suivantes : fréquence cardiaque : 110/min la tension artérielle : 120/80 mmHg, la fréquence respiratoire : 35/min, SpO2: 95% en air ambiant. Son mari vous montre son ordonnance qui comprend: Formeteropl et Beclomethasone. Le diagnostic asthme exacerbé retenu le plus vraisemblablement. Quel est le signe de gravité non présents dans l’énonce, recherchez vous ?
Murmure vésiculaire augmenté
Débit expiratoire point inférieur à 60%
PaO2 inferieur à 80 mmHg
Augmentation des sibilants
PaCO2 superieur à 35 mmHg
Vous recevez aux urgences Mr. Y, 24 ans, pour une dyspnée expiratoire intermittente. Il a une notion d’asthme depuis enfant.A l’examen clinique, vous trouvez des sibilants diffus. Les constantes sont suivantes : la fréquence cardiaque : 140/min Tension artérielle: 130/92 mmHg, fréquence respiratoire: 35/min, SpO2 : 92% en air ambiant. Son mari vous montre son ordonnance qui comprend: Formeteropl et Beclomethasone. Le diagnostic asthme aigu grave retenu le plus vraisemblablement. La prise en charge thérapeutique immédiate : Oxygénothérapie SpO2 supérieur à 94% et corticothérapie systémique. 2 heures plus tard, le patiente se plainte de douleurs dans les 2 jambes. Quelle est la condition le plus vraisemblable ?
Hypoalbuminémie
Hypocalcémie
Hypoglycémie
Hypokaliémie
Hyponatrémie
Vous recevez en hospitalisation un chauffeur âgé de 27 ans pour sensation d’étouffement. Poids 109 Kg pour taille 1m62, la tension artérielle: 143/98 mmHg, poules 98 par min, fréquence respiratoire : 21/min et la SpO2 96% en état éveil et 84% en dorment avec ronflement. Il n’a pas antécédent particulier ni acromégalie ni hypothyroïdie. Il a deux accidents de voie publique par rapport au somnolence. Vous pensez à syndrome d’apnée du sommeil. Quelle est la complications du syndrome d’apnée obstructive du sommeil?
Hypertension artérielle pulmonaire liée à l’hypoxémie
Risque accidentogène lié à l’hyper somnolence diurne
Polysurie du à la sécrétion nocturne d’hormone croissance
Syncope du au sommeil non réparateur
Insuffisance cardiaque du à la sécrétion accrue de facteur atrial natriurétique
Vous recevez en hospitalisation une patiente âgée de 57 ans pour sensation d’étouffement. Poids 86 Kg pour taille 1m52. La tension artérielle: 123/68 mmHg, poules 98 par min, la fréquence respiratoire : 23/min et la SpO2 96% en état éveil et 84% en dorment avec ronflement. Il a antécédent des épisodes fatigue et dysphagie associées dysphonie et tombé paupières vespérales. Vous pensez à un syndrome d’apnée du sommeil et la confirmation du diagnostic syndrome d’apnée obstructive du sommeil. Quelle est la pathologie est associée à un syndrome d’apnée du sommeil avec hypercapnie ?
Myasthénie atteinte diaphragmes
Bronchite chronique tabagique
Syndrome hépato pulmonaire
Asthme non contrôle
Emphysème centro lobulaire
Un patient de 23 ans en hospitalisation pour dyspnée de repose. Vous retrouvez une HTAP sans cardiopathie ni pneumopathie thromboembolique ni maladie systémique signaler. Néanmoins, vous retrouve une hyper éosinophile sanguine, donc la cause parasitaire est le piste à dépister. Quel est le parasite responsable d’une hypertension artérielle pulmonaire (HTAP) peut-on retrouver d’oeufs dans les selles, urines, biopsie rectale, ou biopsie pulmonaire ?
Tænia
Bilharzies
Ascaris
Ankylostome
Paragonimus
Un patient de 23 ans en hospitalisation pour fièvre et frisson depuis une semaine. Il est le gardien de la forêt Koh Kong. Vous pensez à une parasitose pulmonaire à protozoaire. Quel est le parasite le grave peut-on retrouver ce patient?
Amibiase
Plasmodium
Toxoplasma
Pneumocystis
Leishmanie
Vous recevez en consultation une femme noire de 40 ans pour amaigrissement et fièvre prolongée. Elle est mariée sans enfant. Le poids est de 45 Kg pour taille 167cm, la tension artérielle est 130/87 mmHg et poules 102 par fréquence respiratoire 25/min SpO2 97% en air ambiant. Le cliché de radiographie thoracique révèle des opacités hilaires et interstitielles bilatérale. Vous pensez à une sarcoïdose. Quelle est la sérologie doit être systématiquement proposée?
Sérologie hépatite B -C
Sérologie VIH
Sérologie toxoplasmose
Sérologie syphilis
Sérologie cysticercose
Vous recevez en consultation une femme noire de 45 ans pour toux chronique et dyspnée d’effort. Elle est mariée sans enfant. Le poids est de 48 Kg pour taille 157cm, la tension artérielle est 130/87 mmHg et poules 102 par fréquence respiratoire 25/min SpO2 97% en air ambiant. Le cliché de radiographie thoracique révèle des opacités hilaires et interstitielles bilatérale. Vous pensez à une sarcoïdose. Quelle est la principale complication respiratoire évolutive de cette maladie?
Pneumothorax compressif
Fibrose pulmonaire
Hémoptysie itérative
Dilatation des bronches
Hémorragie alvéolaire
Vous recevez Mr S.K âgé de 67 ans, tabagique à 50 paquets-année en hospitalisation , a une toux et une expectoration chronique depuis plusieurs années. Il vient consulter pour une dyspnée d’effort aggravation progressive. Le bilan initial montre une distension thoracique à radiographie pulmonaire, l’exploration fonctionnelle respiratoire donne comme suivant : Capacité vital lent (CV) : 2500 mL soit 84% de la théorique ; Volume expiratoire maximal par seconde (VEMS) : 1100 mL inchangé après inhalation de salbutamol ; le rapport de Tiffeneau (VEMS/CV) est évalué à 44% et la capacité pulmonaire totale (CPT) : 5300 mL soit 128% de la théorique. Quel est le pourcentage le tabac est un facteur de risque de bronchopneumopathie chronique obstructive (BPCO)?
50 – 60 %
40 – 50 %
70 – 80 %
60 – 70 %
80 – 90 %

Vous recevez Mr J âgé de 65 ans, tabagique à 60 paquets-année en hospitalisation, pour fièvre et expectoration purulente. Le patient que vous connaissez au service. Le bilan a une distension thoracique à radiographie pulmonaire. L’exploration fonctionnelles respiratoires donne comme suivant : Capacité vital lent (CV) : 2500 mL soit 84% de la théorique ; Volume expiratoire maximal par seconde (VEMS) : 1100 mL inchangé après inhalation de salbutamol ; le rapport de Tiffeneau (VEMS/CV) est évalué à 44% et la capacité pulmonaire totale (CPT) : 5300 mL soit 128% de la théorique. Quel diagnostic évoquez-vous?
Asthme chronique
Bronchite chronique
Bronchite chronique obstructive
Bronchite aiguë dyspnéique
Bronchite chronique obstructive exacerbée
Vous recevez le résultat explorations fonctionnelles respiratoires (EFRs) un patient âgé de 65 ans, tabagique à 50 paquets-année en état respiratoire stable. Ce patient vous connaissez au service. L’exploration fonctionnelles respiratoires donne comme suivant : Capacité vital lent (CV) : 2500 mL soit 84% de la théorique ; Volume expiratoire maximal par seconde (VEMS) : 1100 mL inchangé après inhalation de salbutamol ; le rapport de Tiffeneau (VEMS/CV) est évalué à 44% et la capacité pulmonaire totale (CPT) : 5300 mL soit 128% de la théorique. Quel est le stade de sévérité de cette maladie ?
Stade de sévérité 1
Stade de sévérité 0
Stade de sévérité 3
Stade de sévérité 2
Stade de sévérité 4
Mr. Z., 58 ans vous est adressé pour douleur du membre supérieur droit à type de décharges électriques, qui surviennent le plus souvent la nuit et résistent aux antalgiques usuels. Ces douleurs intéressent la face antéro-interne de l’avant-bras droit ainsi que 2 derniers doigts. Vous observez une amyotrophie de l’éminence hypothénar. Mr. Z. Vous signale également une toux apparue depuis 3 mois accompagnée d’une une grande asthénie et amaigrissement. C’est un patient tabagique à 30 PA. Il vous apporte une radiographie thoracique révèle une opacité masse arrondie au sommet droit. Vous suspectez à un syndrome de Pancoast Tobias et la biopsie de la tumeur bronchique révèle de cancer bronchique de type adénocarcinome. Quel est le syndrome paranéoplasique le plus probable peut-on retrouver dans ce cancer ?
Syndrome de Pierre Marie Foix
Syndrome de Pancoast Tobias
Syndrome de Lofgren
Syndrome de pénétration
Syndrome cave supérieur
Un homme âgé de 56 ans en hospitalisation pour oedème cervico brachiale. Il a principale une BPCO post tabagique 40 paquet-année. La maladie a remonté il y a 2 semaines : céphalées matinales et vertige. Le patient vous raconte un gonflement du bras puis comblement du creux sus claviculaire et oedème cervico brachiale. L’examen : circulation veineuse collatérale et turgescence jugulaire. Quel syndrome le plus probable ?
Syndrome Claude Bernard Horner
Syndrome de Pancoast Tobias
Syndrome de pénétration
Syndrome de Lofgren
Syndrome cave supérieur
Mrs. W is 33 years old, lives in Svay Rieng province, married, garment worker. The previous 4 years, she had been seeking at medical setting because she believed she was having a heart attack. The disorder began 2 months after the delivery of her only child. She suddenly increase in her heartbeat, chest pain and had difficulty breathing. She started 1-2 times a month of sweating and trembling and feared of dying from a heart attack and currently unable to leave home alone. BP140/ 86- 150/ 90 mmhg, Pulse= 92/mn. Which is the most emergency parameter checkup first?
Electroencephalographic.
Electrocardiographic.
Glucose parameters.
Calcium parameters.
The thyroid parameters.

Une femme âgée de 72 ans est présentée aux Urgences pour une douleur de l’aine droite, suite à une chute de sa hauteur il y a une semaine. Comme ATCD, elle est sous traitement antihypertenseur depuis des années. A domicile, elle a été traitée par médicaments antalgiques et AINS et la douleur est calmée de manière intermittente. La raisons pour laquelle elle a été emmenée à hôpital. L’examen clinique révèle une douleur intense de la hanche droite avec impotence fonctionnelle du membre. Il est en position de rotation externe et adduction avec raccourcissement de 4cm. La radiographie du bassin a été faite. Le cliché hanche droite de face est comme ça. La fracture est classée en?
GARDEN II
GARDEN I
GARDEN IV
GARDEN III
Aucune des réponses précédentes
Un jeune homme de 34 ans est transféré de province de Banteay Meanchey pour une fracture ouverte de jambe droite causée par accident de la voie publique. L’accident s’est déroulé il y a 12 heures et il est transféré directement à l’hôpital. L’examen clinique révèle un délabrement très importent des parties molles avec exposition osseuse au niveau de la jambe droite. Il y a une grande plaie environ 8cm, lésions extensives de masse musculaire avec presence de débris de terre dans la plaie. Les pouls distaux sont perceptibles, la radiographie montre une fracture au 1/3 moyen avec petite comminution osseuse et déplacement en chevauchement. Classification de Gustilo de cette fracture?
Type II
Type I
Type IIIb
Type IIIa
Type IIIc
Un jeune de l’homme 20 ans, accident par chute sur le moignon de l’épaule gauche, il a très mal de l’épaule gauche, impotence fonctionnelle du membre supérieur gauche avec attitude vicieuse, et à l’inspection un fragment de la clavicule est basculé en haut. La radiographie montre une fracture de la clavicule gauche avec déplacement en chevauchement importance. Avec les types de fractures ci-dessous, quel type de fracture de la clavicule habituellement les plus déplacées?
Fracture bifocale
Fracture de l’extrémité distale
Fracture du tiers moyen
Fracture associées à une disjonction acromio-claviculaire
Fracture de l’extrémité proximale
Un jeune l’homme 20 ans, ayant un accident par chute sur le moignon de l’épaule gauche, il a très mal de l’épaule gauche, impotence fonctionnelle du membre supérieur gauche avec attitude vicieuse, et à l’inspection on constate un fragment fracturaire de la clavicule gauche est basculé en haut. Radiographie montre une fracture de la clavicule gauche avec un chevauchement importance. Concernant le déplacement de la fracture, quell est le muscle qui attire le fragment proximal en haut?
Sous clavier
Sterno-cléido-Mastoïdien
Scalène
Deltoïde
Trapèze
Vous avez reçu un patient de 40 ans, qui présente une douleur de l’épaule droite avec impotence fonctionnelle et déformation à la suite de traumatisme par chute sur épaule. Vous suspectez une luxation antérieure de l’épaule droite. Radiographie montre une luxation antérieure gléno-humérale droite avec arrachement du trochiter. Parmis les tendons suivantes lequel est plus probablement abîmé?
Tendon subscapulaire
Tendon du biceps
Tendon sus épineux
Tendon sous épineux
Tendon Petit rond
{"name":"ECN and Teachers' Questions page 345-387 part 9", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"A 27-year-old man is referred by his GP with progressively painful swelling of his left knee following a minor football injury some weeks ago. The radiograph shows a 5-cm ill-defined lytic lesion within the left distal femoral metaphysis, with a permeative pattern of bone loss and areas of cloud-like ossification. There is an extensive periosteal reaction, predominantly orientated perpendicular to the cortex. What is the most likely diagnosis?, An 80-year-old woman is admitted to hospital following a fall. The patient had a right mastectomy and axillary dissection 5 years ago to treat an invasive ductal carcinoma. The pelvic radiograph reveals a left hip fracture. Which fracture site would be most suggestive of a pathological fracture?, A 19-year-old student returns to the UK following 4 months’ travelling around the world. Radiographs reveal multiple oval areas of calcification, up to 1 cm in long axis, aligned in the direction of muscle fibres. What is the most likely diagnosis?","img":"https://cdn.poll-maker.com/10-474794/35.jpg?sz=1200"}
More Quizzes
Lesson #4 Questions
20100
Fun Birthday Party Quiz
12612
Grilă TDEE
58290
Pop Culture Challenge Quiz
1587
Tennis Rules - Test Your Knowledge of Scoring & Calls
201018919
Loner Personality: Loner or People-Pleaser?
201018565
Adjacency Matrix for Interior Design - Free
201030049
You Supply Air to the Trailer Tanks By: CDL Air Brakes
201025089
Alberta Trivia - How Well Do You Know the Province?
201018565
Stroke Knowledge - Free Online Practice Questions
201027896
Which Bollywood Actress Are You? Take the Free
201022174
Free Road Safety for Students - Test Your Knowledge
201019789