
USMLE: Endocrinology
A 40-year-old female presents with altered mental status and confusion. Last year, she was diagnosed with rheumatoid arthritis, for which she is currently using indomethacin and methotrexate. Her temperature is 37.0C (98.6F), pulse is 75/min, blood pressure is 110/70, and respirations are 15/min. She is disoriented and irritable. Mucus membranes are moist. There is no jugular venous distention. Lungs are clear to auscultation. Abdomen is soft, nontender and not distended. There is no peripheral edema. Serum chemistry reveals: Sodium 122 mEq/L Potassium 3.7 mEq/L Bicarbonate 22 mEq/L Blood glucose 90 mg/dL BUN 9.0 mg/dL Uric acid 3.0 mg/dL Serum osmolality is 265mOsm/kg, while urine osmolality is 500 mOsm/kg. What is the most likely cause of this patient's hyponatremia?
Syndrome of inappropriate ADH secretion
Mineralocorticoid deficiency
Nephrotic syndrome
Advanced renal failure
Diabetes insipidus

A 50-year-old male comes to the office due to an ulcer in his right foot. He has type 2 diabetes, for which he takes glyburide. Laboratory investigations reveal an HbA1c of 9%, and random blood sugar of 180 mg/dl. X-ray of the leg/foot is normal. A picture of the foot ulcer is shown below. Which of the following is the most appropriate management of this patient's foot ulcer?
Perform thorough debridement of the wound
Amputation
Start aspirin and atorvastatin
. Prescribe oral antibiotics and follow-up as an outpatient
Prescribe tight-fitting shoes
A 50-year-old male presents for the evaluation of polyuria and polydipsia of two months duration. He also complains of weakness and fatigue. He had one episode of paralysis that resolved on its own. He has a 20 pack-year history of smoking. He does not drink alcohol. His past medical and family histories are not significant His pulse is 78/min, blood pressure is 150/96 mmHg and temperature is 37C (98.6 F). The rest of his examination, including the neurological examination, is unremarkable. Laboratory studies show: Plasma sodium 145 mEq/L Potassium 24 mEq/L Serum creatinine 0.8 mg/dl Plasma renin activity low Plasma aldosterone concentration high Which of the following is the most likely diagnosis?
Primary hyperaldosteronism
Renovascular hypertension
Hypokalemic periodic paralysis
Renin-secreting tumor
Congestive heart failure
65-year-old Caucasian male comes to the office because of bilateral foot pain, which is present at rest and worsens at night. He has been having this symptom for the past few months. Other accompanying symptoms are hyperesthesia and paresthesia in both lower limbs. His medical problems include diabetes for the past twenty years. His daily medication is insulin. Physical examination reveals bilateral loss of ankle reflexes, loss of vibratory sensation and altered proprioception below the knees. His HbA1c level is 9%. Urine is positive for microalbuminuria. Which of the following is the most appropriate treatment for his leg pain?
Amitriptyline
Oxycodone
Corticosteroids
Ketorolac
Acetaminophen
A 25-year-old woman comes into the office with a three-month history of weight loss, irritability, insomnia, and palpitations. Her past medical history is insignificant. She is not taking any current medications and denies drug abuse. Her blood pressure is 155/70 mmHg and heart rate is 110/min. Physical examination reveals lid retraction, fine tremor of the hands, and increased neck circumference. The most probable cause of hypertension in this patient is·
Hyperdynamic circulation
Increased peripheral vascular resistance
Decreased vascular compliance
Sodium retention
Increased intravascular volume
A 49-year-old African-American male comes to the office and complains of headaches which have been worsening for the last three months. His other complaints include diffuse joint pains, pain on the lateral half of his right hand, difficulty getting his wedding ring out due to finger swelling, and difficulty holding and gripping objects with his right hand. His past medical history is significant for hypertension, which has not been controlled well despite compliance with medications, very low salt diet, and regular exercise. His current medications are amlodipine, lisinopril, and hydrochlorothiazide. His blood pressure is 146/98 mmHg, pulse is 90/min, temperature is 36.7C (98F) and respirations are 14/min. His facial features appear coarse when compared to his driver's license photo, which was taken three years ago. His palms are sweaty and have a doughy feel. His skin is oily. There are multiple skin tags, particularly around his neck area. Hand examination reveals positive Tinel's and Phalen's sign. Which of the following will be the most helpful in confirming the clinical diagnosis?
Measuring growth hormone following an oral glucose load
Measuring fasting growth hormone levels
Performing TRH stimulation test
MRI of his pituitary gland
Measuring insulin-like growth factor (IGF-1) level
A 55-year-old African-American male comes to the office for a routine follow-up visit. His past medical history is significant for type 2 diabetes mellitus (OM), hypertension for the last 5 years, and an acute myocardial infarction 2 years ago. His mother died of a heart attack at the age of 72 years, and his father died in a motor vehicle accident at the age of 42 years. He has no siblings. He is currently on glyburide, captopril and baby aspirin. He is very compliant with his diet and medication. His glycemic control was very good until a few months ago, when he noticed that his blood sugar levels were running high. This morning, his finger stick reading was 200 mg/dl. He weighs 188 lbs and is 5'8" tall. His physical examination is otherwise unremarkable. His blood work done three days ago showed blood urea nitrogen of 14 mg/dl and a creatinine level of 1.0 mg/dl. His HBA1c one month ago was 8.0%. Which of the following is the most appropriate next step in management?
Add metformin to achieve better glycemic control.
Discontinue captopril since glyburide efficacy is reduced with simultaneous usage of captopril.
Add pioglitazone to achieve better glycemic control.
Discontinue captopril because it is known to produce diabeticogenic state.
Start the patient on human insulin 70/30.
A 55-year-old Caucasian male presents to the office for a routine check-up. He has no present complaints. His past medical history is significant for a long history of hypertension. He does not smoke or consume alcohol. His current medications are enalapril and hydrochlorothiazide. His blood pressure is 140/90 mm Hg and heart rate is 80/min. Physical examination reveals a moderately overweight man (BMI = 27 kg/m2) with a waist circumference of 41 inches. The laboratory studies show: Fasting blood glucose 112 mg/dl Total cholesterol 220 mg/dl LDL cholesterol 140 mg/dl Triglycerides 240 mg/dl Which of the following is the most important pathogenic factor for this patient's condition?
Insulin resistance
Impaired secretion of insulin
Sympathetic hyperactivity
Insulin-mediated vasodilatation
Low absolute values of insulin
A 24-year-old Caucasian female comes to the outpatient clinic and complains of heat intolerance and increased appetite. Her past medical history is insignificant. She denies use of over-the-counter medications. Her pulse is 110/min and regular, temperature is 37.2C (99F), and respirations are 14/min. Swelling is noted in the front of her neck, which moves with deglutition. Lab studies show: Total T4 Increased Free T4 Increased TSH Decreased Radioactive iodine uptake is decreased. The thyroid scan shows very low uptake of radioiodine. What is the most likely diagnosis?
Thyroiditis
Multinodular goiter
Struma ovarii
Toxic adenoma
Graves’ disease
A 34-year-old Caucasian female comes to the emergency department and complains that her heart is "racing out of control." She began to feel this way only this morning. She denies any chest pain or shortness of breath. Over the past few months, she has unintentionally lost 10 pounds. Her past medical history is significant for panic attacks, but she claims she has not had an attack for over 10 years. She is very concerned because her father died of a heart attack at the age of 40. The EKG reveals sinus tachycardia at a rate of 120/min. The initial labs show:
CBC:
Hb 12.9g/dL Ht 39% MCV 88 fl
Platelet count 200,000/cmm Leukocyte count 8,500/cmm Neutrophils 67%
Eosinophils 1%
Lymphocytes 24% Monocytes 8% Serum:
Serum Na 139 mEq/L Serum K 4.2 mEq/L Chloride 100 mEq/L Bicarbonate 25 mEq/L
BUN 10 mg/dL
Serum Creatinine 1.0 mg/dL Calcium 9.1 mg/dL
Blood Glucose 102 mg/dL TSH < 0.1 microU/mL
Free T4 4.6 ng/dL (N0.9-24)
Which of the following is the best immediate step to control this patient's symptoms?
Propanolol
Propylthiouracil
Subtotal thyroidectomy
Alprazolam
Radioactive Iodine
A 54-year-old male comes to the office for follow-up care of his foot ulcer. He has no complaints regarding the ulcer, but he has recently become polyuric and polydipsic. Fa sting blood work reveals elevated glucose levels. He is prescribed oral hypoglycemics, and counseled on self-monitoring at home. On his next follow-up visit, the patient proudly states that he has been "very compliant" with his medications, and that his glucose levels are "always well-controlled." Which of the following is the best way to determine whether this patient is telling the truth?
Glycosylated haemoglobin
Serum insulin levels
Serum C-peptide levels
Random blood glucose
Fasting urine glucose
A 48-year-old white male complains of generalized bone pain after undergoing bowel surgery for inflammatory bowel disease. His pain is more severe at the lower spine, pelvis, and lower extremities. Examination shows tenderness over the lower spine, pelvis, and lower extremities. Proximal muscle weakness is noted. X-rays of the lumbar spine show decreased bone density with blurring of the spine. X-rays of the femoral neck show pseudofractures, bilaterally. Which of the following lab abnormalities is consistent with this patient's diagnosis?
Low serum calcium, low serum phosphate, increased serum parathyroid hormone
Increased serum calcium, increased serum phosphate, low serum parathyroid hormone
Increased serum calcium, low serum phosphate, increased serum parathyroid hormone
Normal serum calcium, normal serum phosphate, normal serum parathyroid hormone
Low serum calcium, increased serum phosphate, low serum parathyroid hormone
A 24-year-old white female is brought to the emergency department (ED) by her mother due to altered mental status. According to her mother, she suffered from viral gastroenteritis 4 days ago. Since then, she has been on oral fluids. Over the past 2 days, her condition had been deteriorating, but she kept refusing admission to the hospital. Her past history is not significant, except for excessive thirst, water intake and weight loss over the past two months. Her blood pressure is 100/56 mm Hg, pulse is 120/min (regular and weak), temperature is 37.2C (99.F), and respirations are 28/min (rapid and deep). Pulse oximetry is 94% on room air. She is arousable and moves all her extremities. Her mucous membranes are very dry. Her neck is supple. The chest is clear on auscultation. Which of the following is the most appropriate next step in management?
Fingerstick glucose
Obtain electrocardiogram
Intubate the patient
Obtain arterial blood gases
Obtain CT scan of head
A 38-year-old Mexican male presents to the emergency department with a history of weight loss, fever, cough with sputum, nausea, abdominal pain, and postural dizziness for the last three months. Adrenal insufficiency is suspected, and cosyntropin (synthetic ACTH) stimulation test is performed. The rise of serum cortisol following an injection of cosyntropin is grossly subnormal. CT scan of the abdomen shows calcification of both adrenal glands. What is the most likely cause of this patient's adrenocortical insufficiency?
Tuberculosis
Human immunodeficiency virus infection
Adrenal tumor
Adrenal haemorrhage
Autoimmune adrenalitis
A 60-year-old male comes to the office due to edema of his face and ankles of two weeks duration. He denies any chest pain or breathlessness. He is a known diabetic for the past 15 years. His diabetes is being managed with exercise, dietary modification and glyburide. His glycosylated hemoglobin (HbA1C) level one month ago was 7.5%. His temperature is 37.0C (98.6F), pulse is 75/min, blood pressure is 146/87 mm Hg, and respirations are 15/min. Examination is unremarkable, except for bilateral pitting edema around the ankles and periorbital edema. Lab results show:
Serum sodium 140 mEq/L Potassium 4.3 mEq/L Bicarbonate 20 mEq/L Blood glucose120 mg/dl
Blood urea nitrogen 37 mg/dl Serum creatinine 24 mg/dl Total cholesterol 300 mg/dl
EKG is normal. 24-hour urine collection shows 3.7 g protein/day. To alter the course of this patient's diabeticnephropathy, what is the most appropriate next step in management?
Intensive blood pressure control
Aspirin therapy
Very low protein diet
Aggressive lipid management
Intensive glycemic control
A 17-year-old white female comes to the office for the evaluation of fatigue which has been present for the past 4 months. Her past medical history is insignificant. She denies the use of any drugs. Her pulse is 74/min, blood pressure is 110/70 mm Hg, and temperature is 36.7C (98.0F). Physical examination shows scars on the dorsum of her hands and dental erosions. Laboratory studies show: Plasma sodium 139 mEq/L Serum potassium 2.3 mEq/L Bicarbonate 40 mEq/L Urine chloride concentration is 15 mEq/L (Normal = 80-250 mEq/L). Based on these findings, what is the most likely diagnosis?
Surreptitious vomiting
Diuretic abuse
Bartter's syndrome
Chronic diarrhea
Primary hyperaldosteronism
A 21 -year-old female has a several month history of easy fatigability and palpitations. She also complains of excessive sweating. She follows a strict, low calorie diet in order to lose weight. Her blood pressure is 120/70 mmHg and her heart rate is 100/min. Her BMI is 19kg/m2 Thyroid function testing reveals the following findings: TSH decreased Total T4 high Total T3 high Radioiodine uptake is diffusely decreased over the thyroid gland. Which of the following is the most likely pathologic finding on biopsy of this woman's thyroid gland?
Follicular atrophy
Papillary neoplastic growth
Orphan Annie nuclei
Diffuse follicular hyperplasia
Dense lymphocytic infiltrate
A 60-year-old Caucasian male is brought to the emergency department by his daughter due to a 2-day history of confusion and lethargy. According to his daughter, he had been complaining of fatigue, anorexia, polyuria and constipation for the last several weeks. He smokes two packs of cigarettes daily, and consumes alcohol occasionally. His blood pressure is 130/90 mmHg and heart rate is 90/min. Physical examination reveals a somnolent patient who is not oriented in time. His lab values are: Serum Na 140 mEq/L Serum K 4.0 mEq/L Serum chloride 100 mEq/L Serum bicarbonate 22 mEq/L Serum creatinine 1.6 mg/dl Serum calcium 13.4 mg/dl Serum phosphorus 2.2 mg/dl Blood glucose 1 00 mg/dl Alkaline phosphatase 80 U/L Chest x-ray demonstrates a right middle lobe mass and perihilar adenopathy. What is the most probable cause of this patient's symptoms?
Parathyroid hormone-like peptide
Elevated PTH
Local cytokine production
Metastatic osteolysis
Increased vitamin D production
A 45-year-old white male patient presents for the evaluation of high blood pressure. He also complains of polyuria, polydipsia and fatigue. His past medical and family histories are unremarkable. He does not use tobacco, alcohol or drugs. His blood pressure is 180/100mmHg. Physical examination shows no abnormalities. Laboratory studies show low serum potassium and high plasma aldosterone levels. CT scan of the abdomen shows a small, right adrenal mass. Which of the following additional findings is most likely to be present in this patient?
Mild hypernatremia
Edema
Episodes of high blood pressure
Metabolic acidosis
Increased plasma renin activity
A 51 -year-old female comes to the office for a routine visit. She is apparently healthy and does not have any complaints. Physical examination reveals a thyroid nodule. She is surprised to hear about the nodule and asks, "How often does this happen? What could have caused this?" Which of the following is the most common cause of thyroid nodules?
Colloid nodule
Papillary carcinoma
Anaplastic carcinoma
Follicular carcinoma
Follicular adenoma
A 40-year-old white female presents with complaints of heat intolerance, sweating and palpitations. She also reports menstrual irregularities, increased appetite and diarrhea. She has had these symptoms for the past 4 Months. Her pulse is 102/min and regular, blood pressure is 116/80 mm Hg, temperature is 37.2C (99F), and respirations are 14/min. Physical examination reveals a non-tender, diffuse swelling in front of her neck; it moves upwards with deglutition. Her TSH level is 0.05 mU/L. Free T4 and T3 levels are increased. Radioactive iodine uptake at 24 hours is significantly increased. Pregnancy test is negative. Which of the following is the most appropriate long-term treatment modality for this patient?
Radioactive iodine therapy
Propranolol
Propylthiouracil
Surgery
Iodinated contrast agents
A 56-year-old female is admitted with a diagnosis of chronic renal failure from systemic lupus erythematosus and non-steroidal anti-inflammatory drug use. She has a history of recurrent kidney stones. Laboratory studies show the following: Serum calcium 10.6 mg/dl Serum albumin 3.9 g/L PTH 140 pg/ml Serum phosphorus 3.0 mg/dl Her baseline serum creatinine level ranges from 1.6 to 1.8 mg/dl. Her bone mineral density is measured by DXA scan, revealing a T score of-2.5 at the lumbar spine, which is consistent with osteoporosis. What is the most likely cause of this patient's hypercalcemia?
Primary hyperparathyroidism
Hypercalcemia of malignancy
Chronic renal failure
Milk-alkali syndrome
Sarcoidosis
A 50-year-old Caucasian male comes to the office for the evaluation of polyuria and polydypsia for the last two months. He also complains of weakness and fatigue. He had one episode of transient proximal muscle weakness which lasted 30 minutes. He has a 20-pack year history of smoking. He does not drink alcohol. His past medical and family histories are insignificant. His pulse is 78/min, blood pressure is 150/96 mm Hg and temperature is 36.7C (98F). The rest of the examination, including the neurological examination, is normal. Labs show: Plasma sodium 150 mEq/L Potassium 2.6 mEq/L Serum creatinine 0.8 mg/dL Which of the following is the most appropriate next step in the management of this patient?
Measurement of plasma renin activity and aldosterone concentration
Imaging of adrenals by CT scan
Measurement of 24-hour urinary potassium excretion
Adrenal vein sampling
Aldosterone suppression testing
A 78-year-old female is being evaluated for recent weight loss and fatigue. Laboratory tests reveal abnormal thyroid function. She begins treatment with a single agent, but soon after is hospitalized with new onset atrial fibrillation and hand tremor. Which of the following treatments had she most likely received?
Radioactive iodine
Propranolol
Propylthiouracil
Prednisone
Lopanoic acid
A 46-year-old male presents with swelling of his face that is especially prominent in the periorbital area. He also complains of bilateral ankle swelling. He denies shortness of breath, fever and discoloration of urine. He is a non-smoker and non-alcoholic. His past medical history is not significant. He is currently not taking any medication. His pulse is 78/min, blood pressure is 130/70mm Hg, respirations are 14/min and temperature is 37.1C (99.0F). Examination shows bilateral pitting ankle edema. Auscultation reveals clear lungs, normal heart sounds, and no murmurs. Dipstick urinalysis is positive for protein. 24-hour urine collection shows proteinuria of 4.6 g/day. Lab studies show: Total serum calcium 7.5 mg/dl Albumin 2.2 g/dl Phosphorus 3.5 mg/dl Magnesium 2.2 mg/dl Creatinine 0.8 mg/dl Which of the following is the most likely cause of his low serum calcium level?
Decreased 25-hydroxylation of vitamin D
Decreased 1-alpha-hydroxlation of 25-0 H vitamin D
Increase 25-hydroxylation of vitamin D
Decreased levels of parathyroid hormone
Decreased serum albumin
A 55-year-old male presents with complaints of an ulcer over the sole of his right great toe for one week. His medical problems include a ten-year history of hypertension, diabetes and hypercholesterolemia. His current medications are ramipril, aspirin, metformin, glibenclamide and pravastatin. He has a 20-pack year history of smoking and occasionally drinks alcohol. He denies illegal drug use or multiple sexual partners. Which of the following is most likely contributing to the development of his foot ulcer?
Diabetic neuropathy
Poor glycemic control
History of smoking
Peripheral vascular disease
Bony abnormality of the foot
A 36-year-old white male is brought to the emergency department because of dyspnea, tachypnea, crampy pain and paresthesias in his extremities. He gives an unclear history about how he "rapidly ascended to a height of 10,000 feet” His pulse is 70/min, blood pressure is 120/80 mm Hg, temperature is 36.7C (98.5F) and respirations are 24/min. The significant physical finding on examination is carpopedal spasm. At this point, the suspected diagnosis is acute respiratory alkalosis secondary to hyperventilation. Which of the following is true regarding this patient's serum calcium level?
Fall in calcium bound to inorganic anions
Fall in total plasma calcium
Increase in calcium bound to albumin
Fall in calcium bound to albumin
Increase in calcium bound to inorganic anions
A 28-year-old white female presents to the office for the evaluation of goiter. She denies any recent change in appetite or weight, diarrhea, constipation, heat or cold intolerance, dyspnea and hoarseness. Her menses are normal and regular. Examination shows a symmetrically enlarged, non-tender, firm and rubbery thyroid gland. There is no lymphadenopathy. The rest of the physical examination is normal. Laboratory studies reveal an elevated serum TSH level with normal T4 and T3 levels. Serological testing for Hashimoto's thyroiditis is ordered. Which of the following are the most prevalent antibodies in patients with Hashimoto's thyroiditis?
Anti-thyroid peroxidase antibodies
TSH-receptor blocking antibodies
Anti-smooth muscle antibodies
Anti-mitochondrial antibodies
Thyroid-stimulating immunoglobulins
A 23-year-old Caucasian male with muscular weakness, vomiting and abdominal pain is brought to the emergency department. He had a minor respiratory illness 2 days ago. His past medical history is significant for diabetes mellitus, type 1. He admits skipping his insulin shots yesterday and today because he had no appetite. His temperature is 37.8C (100F), blood pressure is 110/70 mm Hg, pulse is 110/min, and respirations are 27/min. His oral mucosa is dry. The laboratory values are: Serum sodium 132 mEq/L Serum potassium 5.4 mEq/L Serum calcium 8.9 mEq/L Serum chloride 96 mEq/L Serum bicarbonate 12 mEq/L Blood glucose 470 mg/dl BUN 19 mg/dl Serum creatinine 1.1 mg/dl Which of the following is the most likely cause of the increased potassium level in this patient?
Extracellular shift
Decreased gastrointestinal loss
Intracellular potassium excess
Increased renal reabsorption of potassium
Tissue destruction
. An elderly woman is brought to the emergency department (ED) by her husband in a semiconscious state. According to her husband, she had complained of feeling unwell "over the past day or so”, but he only became very concerned when he returned from work today and found her very drowsy and difficult to arouse. Her past medical history is significant for diabetes with diabetic nephropathy and hypothyroidism. Her medications include thyroxine, metformin, gliclazide and lisinopril. Her temperature is 37.3 C (99 F), blood pressure is 110/65 mm Hg, and pulse is 90/min. GCS = 13/15 (Motor 6, Verbal4, Eye3). She is confused and not oriented to time or place, but is able to follow commands. Physical examination reveals dry mucous membranes and decreased skin turgor. Neurological examination reveals weakness in the left arm. The rest of the examination is unremarkable. Urinalysis shows: Blood negative Glucose +++ Ketones negative Protein + Leukocyte esterase negative Nitrites negative WBC 10-20/HPF Which of the following is the most appropriate next investigation to perform?
Blood glucose
Head CT
Echocardiogram
Blood cultures
MRI of head
A 45-year-old female comes to the office for the evaluation of excessive hair growth over her face and body. Her hirsutism rapidly developed over a period of 3 months. She underwent bilateral tubal ligation 4 years ago. Her menstrual cycles were regular in the past, but for the last 3 months, she has not had a menstrual period. She denies any hot flashes or vaginal discomfort. On physical examination, her height is 5'2" (169 cm) and weight is 140 lbs (63.5kg). A large amount of coarse terminal hair is noted on her face, chest and lower abdomen. She appears masculine and has an enlarged clitoris. There is significant temporal balding. Which of the following is the most appropriate next step in management?
Serum testosterone and DHEAS
Selective adrenal and ovarian vein samplings
Serum LH and FSH
Serum 17- hydroxyprogesterone levels
CT scan of abdomen
A 31-year-old Hispanic female presents with palpitations and weight loss. Her past medical history is insignificant. Her family history is unremarkable. She recently moved from South America. She does not smoke cigarettes or drink alcohol. She is married and has three children. Her last delivery was four years ago. Her blood pressure is 140/90 mmHg, pulse is 102/min, temperature is 36.7C (98F) and respirations are 20/min. Her eye examination is unremarkable. Thyroid examination reveals a 2 x 2 cm left-sided thyroid nodule. Her T3 and T 4 are elevated, and TSH is undetectable. Radioactive iodine scan shows uptake only in the left thyroid nodule. Uptake in the rest of the thyroid is markedly reduced. Which of the following is the most likely diagnosis?
Toxic adenoma
Hashimoto's thyroiditis
Graves' disease
Painless thyroiditis
Toxic multinodular goiter
A 29-year-old white female presents to the emergency department with nausea, vomiting, severe generalized abdominal pain, and hypotension. She is subsequently admitted to the intensive care unit. Her past medical history is significant for hypothyroidism secondary to Hashimoto's thyroiditis, for which she has been taking levothyroxine. She denies smoking cigarettes, drinking alcohol, and using any intravenous drugs. Her mother also has hypothyroidism. Her blood pressure is 70/50 mm Hg, heart rate is 110/min, temperature is 98.4F (37.0C) and respiratory rate is 24/min. Physical examination reveals dry and pigmented mucous membranes. The skin creases also show increased pigmentation. Lab studies show: Serum chemistry: Serum Na 130 mEq/L Serum K 6.1 mEq/L Chloride 96 mEq/L Bicarbonate 18 mEq/L BUN 33 mg/dL Serum creatinine 1.3 mg/dL Blood glucose 56 mg/dL CBC: Hemoglobin 10.8 g/L Platelets 300,000/mm3 Leukocyte count 6,500/mm3 Neutrophils 70% Eosinophils 10% Lymphocytes 20% The random serum cortisol level is 3.2 mcg/dL (normal= 5 to 25 mcg/dL), and ACTH level is 142 pg/mL (normal= 9 to 52 pg/mL). What is the most likely involved pathophysiologic mechanism of this patient's disorder?
Autoimmune
Hemorrhagic
Infective
Congenital
Infiltrative
A 40-year-old male patient presents with a thyroid nodule. His other complaints are episodes of palpitations, anxiety and sweating. He denies heat intolerance. His weight and appetite are normal. He has a family history of thyroid cancer. His pulse is 80/min, and blood pressure is 160/ 100 mm Hg. Examination of the neck shows a 4-cm, hard, non-tender thyroid nodule. The urinalysis, serum sodium, serum potassium, serum calcium, serum creatinine, serum PTH, TSH, T3 and T 4 levels, and the EKG are all normal. The serum calcitonin level is elevated. The urinary levels of metanephrine and norepinephrine are increased as well. FNA biopsy of the thyroid nodule shows malignant cells. Genetic testing shows a mutation in the RETproto oncogene. Which of the following abnormalities is also present in most patients suffering from this disorder?
Mucosal neuroma
Pituitary adenoma
Parathyroid adenoma
Brain tumor
Pancreatic islet cell tumor
A 60-year-old female presents with transient loss of consciousness. She appears lethargic and confused. She also complains of hemoptysis and weight loss of 10 lbs (4 .5kg) over a period of 2 months. She has smoked one pack of cigarettes daily for the last 40 years. Her temperature is 37.0C (98.6 F), pulse is 75/min, blood pressure is 110/70, and respirations are 16/min. Her mucus membranes are moist. There is no jugular venous distention. Her neurological examination is non- focal, and cardiovascular examination is unrevealing. There is no ankle edema or ascites. Serum studies show: Sodium 115 mEq/L Potassium 3.7 mEq/L Bicarbonate 22 mEq/L Blood glucose 100 mg/dl BUN 10.0 mg/dl Serum osmolality is 250 mOsm/Kg, and urine osmolality is 500 mOsm/Kg. Urine sodium concentration is 40 mEq/L. Chest x-ray shows a mass in the right hilar region. What is the most appropriate next step in the management of this patient?
Hypertonic saline
Normal saline
Demeclocycline
Loop diuretics
Water restriction
A 36-year-old female presents with weight loss, palpitations, mild shortness of breath, heat intolerance, tremors, and increased sweating. She does not have any past medical problems. Her family history is unremarkable. Her blood pressure is 140/70 mm Hg, heart rate is 104/min and regular, temperature is 99.0F (37.2C) and respiratory rate is 22/min. Physical examination reveals a 2 x 2 cm nodule in her left thyroid lobe. The rest of her thyroid gland feels normal. There are no palpable lymph nodes in her neck. Eye examination reveals minimal lid lag, but no signs of proptosis or chemosis. She has tremors in both of her upper extremities. Her hands are moist and warm. Thyroid function testing reveals: Serum TSH <0.03 micro IU/ml Total T3 330 ng/dl Total T 4 14 mcg/dl Radioactive iodine scan shows uptake only in her left-sided nodule. Which of the following disorders is this patient at risk of developing if she is left untreated?
Bone loss
Thyroid cancer
Airway compression
Proptosis
Coronary artery disease
A 45-year-old female presents complaining of constipation and abdominal pain for the past two weeks. She also complains of urinary frequency and constant thirst. Her past medical history is significant for obesity. She tells you that she has been trying very hard to lose weight, and over the past six months has even attempted various fad diets. She assures you that she supplements her intake with numerous over-the counter vitamins and minerals. She has managed to lose 20 lbs during this time. Her medical history is also significant for atrial fibrillation for the past 4 years, for which she takes diltiazem. On physical examination, her temperature is 36.8°C (98.2.F), blood pressure is 120/70 mm Hg, pulse is 90/min, and respirations are 13/min. Her mucous membranes are dry, and her abdomen is soft and non-tender without rebound or rigidity. Bowel sounds are present. Urinalysis is within normal limits. Which of the following is most likely responsible for her current symptoms?
Vitamin D overdose
Vitamin A overdose
Diabetic ketoacidosis
Adrenal insufficiency
Diltiazem
A 36-year-old male comes to the office for the evaluation of fatigue and weakness for the last several weeks. He denies any change in appetite, change in weight, heat or cold intolerance, nausea, vomiting and constipation. He cannot recall any recent stressful events. His past medical and family histories are unremarkable. He does not have any medications. His pulse is 76/min, blood pressure is 120/70 mm Hg, respirations are 14/min, and temperature is 36.7C (98F). He is well-oriented to time, place and person. His neurological examination is nonfocal; the deep tendon reflexes are normal. Lab tests show: Hematocrit 43% WBC count 6,000/microl Platelet count 200,000/microl Serum calcium 11 mg/dl Serum albumin 4.5 g/dl 24-hour urinary calcium 200 mg Which of the following is the most likely cause of his symptoms?
Primary hyperparathyroidism
Malignancy
Familial hypocalciuric hypercalcemia
Increased calcium intake
Milk alkali syndrome
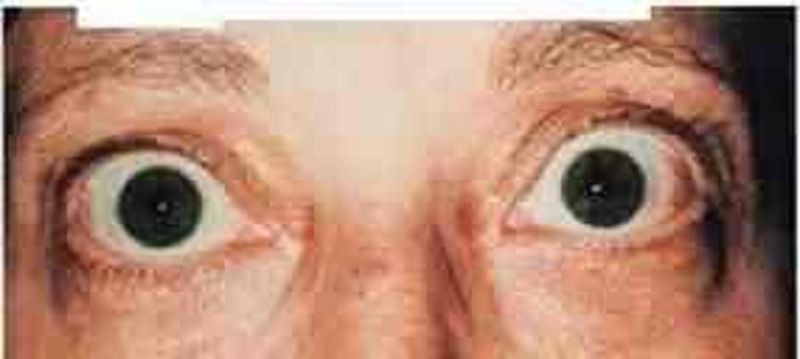
A 46-year-old female complains of a "sandy" sensation in her eyes. Review of systems is notable for a 6-pound weight loss over the last month. A picture of her eyes is shown on the slide below. Which of the following most likely underlies this finding?
Periorbital lymphocytic infiltration
Increased intracranial pressure
High circulating thyroxine level
Increased intraocular pressure
Bilateral facial nerve compression
A 63-year-old white female presents with a thyroid nodule. She denies any weight loss, change in appetite, diarrhea, heat or cold intolerance, menstrual irregularities, hoarseness and dyspnea. Her past medical history is unremarkable. There is no family history of thyroid cancer. She does not take any medications. Physical examination shows a 4-5 cm, fixed, hard, and non-tender thyroid nodule. There is cervical lymphadenopathy. Her serum TSH level is normal. Fine needle aspiration (FNA) of the thyroid shows malignant cells. Which of the following is the most likely expected pathology on FNA?
Lymphoma of the thyroid
Anaplastic carcinoma of the thyroid
Papillary carcinoma of the thyroid
Medullary carcinoma of the thyroid
Follicular carcinoma of the thyroid
A 36-year-old female presents with headaches and visual problems. She also complains of palpitations, heat intolerance and weight loss. Her past medical history is unremarkable. She is currently on no medications. Her blood pressure is 130/60 mmHg, heart rate is 100/min and regular, and weight is 152 lb (weight one year ago was 170 lb). Physical examination reveals a symmetrically enlarged thyroid gland without any tenderness. Auscultation of the chest reveals tachycardia. She has bitemporal hemianopsia on confrontation. The rest of the physical examination is unremarkable. Her lab investigations show: Serum T3 222 ng/ml Serum T 4 13.9 mcg/dl Serum TSH 7.9 IU/ml Alpha subunit level elevated Which of the following is the most likely diagnosis?
TSH-secreting pituitary adenoma
Graves' disease
Primary hypothyroidism
Toxic multinodular goiter
Generalized resistance to thyroid hormone
A 40-year-old African American female comes to the office for a routine medical check-up. She has no complaints. She has twenty pack-year smoking history but she stopped smoking one year ago. Her mother and one maternal uncle have diabetes. Her height is 5'7" inches, and weight is 150 lbs. Her blood pressure is 122/80 mmHg, pulse is 80/min, respirations are 14/min and temperature is 37C (98F). She agrees to have diabetes mellitus screening. Her plasma glucose level after an overnight fast is 130 mg/dl. What is the most appropriate next step in the management of this patient?
Repeat fasting blood glucose measurement
Recommend lifestyle changes
Perform 75 g oral glucose tolerance test
Start therapy with insulin
Start therapy with oral hypoglycemic agents
A 35-year-old male presents with complaints of weakness and fatigue of one year's duration. He is anorexic and has lost interest in all his activities. He also complains of cold intolerance and constipation. His blood pressure is 98/72 mm Hg, temperature is 37.1C (99F), respirations are 14/min, and pulse is 50/min. His skin is dry and rough, nails are brittle, and hair is thin. There is no hyperpigmentation of the skin. Delayed deep tendon reflexes are noted on neurological examination. Lab studies show: Hemoglobin 10.2 g/dL WBC count 5,000/micro-L Neutrophils 45% Monocytes 5% Eosinophils 10% Basophils 1% Lymphocytes 40% Serum sodium 135 mEq/L Serum potassium 4.0 mEq/L Which of the following is most consistent with this patient's findings?
Pituitary tumor
Autoimmune destruction of adrenal glands
Adrenoleukodystrophy
Adrenal tuberculosis
Adrenal CMV infection
A 22-year-old female presents with complaints of heat intolerance, sweating and palpitations. She also reports menstrual irregularities, increased appetite and diarrhea. Her pulse is 102/min and regular, blood pressure is 116/80 mm Hg, temperature is 37.2C (99F), and respirations are 14/min. Physical examination reveals a diffusely enlarged, nontender thyroid gland. TSH level is 0.05 mU/L. Free T4 and T3 levels are elevated. Radioactive iodine uptake at 24 hours is 50 percent. Thyroid stimulating immunoglobulins are present. She is started on propylthiouracil 300 mg daily in three divided doses. After two weeks, she returns and complains of a sore throat. Her pulse is 98/min and regular, temperature is 38.6C (101.5F), blood pressure is 115/76 mm Hg, and respirations are 15/min. The soft palate, pharynx, and tonsils are red and swollen. What is the most appropriate next step in the management of this patient?
Stop propylthiouracil
Throat culture
Oral penicillin
Increase propylthiouracil dose
Add propranolol
A 60-year-old male is admitted to the hospital because of right lower lobe pneumonia. His medical history is significant for hypertension, diabetes mellitus, severe degenerative disease of the spine, and longstanding lower back pain. He is a chronic smoker with a 40-pack year smoking history. During his hospitalization, the laboratory report shows decreased serum calcium levels and increased phosphate levels. Further evaluation reveals increased serum intact parathyroid hormone levels. Which of the following medical conditions is most likely responsible for this patient's abnormal lab findings?
Renal failure
Lung cancer
Plasma cells in marrow
Thyroidectomy
Primary hyperparathyroidism
A 43-year-old female presents to the physician's office with muscle cramps, polydipsia and polyuria. She has no other medical problems, and does not take any medications. She does not use tobacco, alcohol or drugs. Her father died from alcoholic liver disease at age 50. Her pulse is 75/min, respirations are 13/min, blood pressure is 160/100 mm Hg, and temperature is 37C (98.6F). Laboratory studies show: Blood glucose 115 mg/dl Serum sodium 142 mEq/L Serum potassium 2.7 mEq/L Plasma renin activity is low. What is the most likely diagnosis?
Adrenal adenoma
Atherosclerosis of renal artery
Fibromuscular dysplasia
Cirrhosis of liver
Congestive heart failure
A 19-year-old football linebacker is admitted following a motor vehicle accident. He had an extensive cerebral bleed, which led to a deep coma. He also has fractures of the C4 vertebra, pelvis, and right femur. Following admission, he is intubated and central lines are placed. During the next few days, he develops acute renal failure due to rhabdomyolysis. While he is recovering from acute renal failure, he is found to have a serum calcium level of 12.1 mg/dl. Other investigations are: Serum albumin 3.0 g/dl Serum creatinine 2.8 mg/dl Serum phosphorus 3.8 mg/dl Blood glucose 108 mg/dl PTH 9 pg/ml PTHrP undetectable 1, 25-dihyroxy vitamin D 19 pg/ml (normal 20-60 kg/ml) What is the most likely cause of this patient's hypercalcemia?
Lmmobilization
Malignancy
Primary hyperparathyroidism
Acute renal failure
Vitamin D intoxication
A 35-year-old female presents to the emergency department with a 30-minute history of severe headache, palpitations, abdominal pain, nausea, and vomiting. She had similar episodes twice during the last month, but those were not so severe and resolved spontaneously in 30-40 minutes. She visited a doctor recently, and hypertension with elevated urinary vanillylmandelic acid level was diagnosed. She is not taking anymedications, and denies substance abuse. Her blood pressure is 200/130 mmHg and heart rate is 130/min. She appears frightened. Physical examination reveals hand tremors and excessive sweating. Slow intravenous infusion of propranolol is started while waiting for the routine labs. What is the most probable reaction to the treatment given to the patient?
Blood pressure will rapidly increase
Heart rate will increase
Heart rate will not change
Blood pressure will rapidly decrease
Blood pressure will slowly decrease
A 65-year-old male comes to the office and complains of nausea and early satiety for the past several months. His other complaints are anorexia and abdominal bloating. He denies any heartburn or epigastric pain. He has diabetes, and has been taking insulin for the last fifteen 15 years. His blood glucose readings using the home blood glucose monitor range between 40 to 400 mg/dl. Most of the low blood glucose readings occur after meals. Which of the following is the most appropriate management of this patient's symptoms?
Metoclopramide
Promethazine
Ibuprofen
Ranitidine
Ondansetron
A 27-year-old Caucasian male is diagnosed with medullary thyroid carcinoma that is non-resectable. His past medical history is insignificant. He does not smoke or consume alcohol. His family history is significant for thyroid cancer and pheochromocytoma in his father. Which of the following tests could have been most effective in preventing this patient's non-resectable cancer?
Annual physical examination
Periodic serum calcium measurement
DNA testing
Frequent self-examination of the neck
Periodic stimulated serum calcitonin measurement
A 30-year-old Hispanic male presents to the office with complaints of palpitations, tremor, nervousness and headache. His past history is insignificant. His mother has type 2 diabetes, which is well-controlled with medications. His temperature is 37.0C (98.6F), pulse is 100/min, blood pressure is 150/80 mm Hg, and respirations are 16/min. He appears anxious, sweaty and shaky. His neurological examination is non-focal, and examination of other systems is unremarkable. His fingerstick blood glucose level is 38 mg/dl. Intravenous administration of a bolus of 50% dextrose leads to the improvement of his symptoms. He is then subjected to supervise prolonged fasting. After an overnight fast, laboratory studies reveal: Blood glucose 40 mg/dl Serum insulin 15 microU/L (normal value is < 6 microU/L with hypoglycemia) Serum pro-insulin 9 microU/L (normal value is < 20% of total immunoreactive insulin) C-peptide level 0.8 nmol/L (normal value is less than 0.2 nmol/L) Sulfonylurea Negative IGF-II Negative Based on the above information, what is the most likely cause of this patient's hypoglycemia?
Beta cell tumor
Exogenous insulin
Non-beta cell tumor
Glucagonoma
Sulfonylurea agents
A 35-year-old male presents to the family physician for bilateral gynecomastia. He observed a progressive increase in his breast size starting 6 months ago. He is sexually active and denies any drug use. Physical examination reveals bilateral gynecomastia and tenderness. The genito-urinary examination shows a 1 cm nodule in the right testis. Otherwise, the examination is within normal limits. The laboratory report shows: LH 3 U/L, FSH 2 U/L, testosterone 270 ng/dL (Normal 3-10 ng/dL), estradiol 115 pg/mL (Normal 20-60 pg/mL), beta HCG undetectable, AFP undetectable. Which is the most likely diagnosis?
Leydig cell tumor
Teratoma
Choriocarcinoma
Seminoma
Endodermal sinus tumor
A 35-year-old Caucasian male presents with weakness, fatigue, and weight loss over the past year. He is anorexic and has lost interest in all his activities. His temperature is 37.1C (99F), pulse is 84/min, blood pressure is 101/72 mm Hg, and respirations are 14/min. On physical examination, he does not appear to be in acute distress. Dark brown pigmentation is present on his skin creases and oral cavity mucous membranes. Laboratory studies show: Hemoglobin 10.3 g/dL WBC count 3,000/micro-L Neutrophils 60% Monocytes 5% Eosinophils 10% Basophils 1% Lymphocytes 24% Serum sodium 130 meq/L Serum potassium 5.5 meq/L Chest x-ray and PPD tests are normal. What is the most appropriate next step in the management of this patient?
Cosyntropin stimulation test
Begin intravenous hydrocortisone
Measure plasma ACTH level
Low-dose overnight dexamethasone suppression test
24-hour urinary free cortisol
A 56-year-old female comes to the office and complains of general malaise and headaches. Her other symptoms are episodic palpitations, throbbing headaches and diaphoresis. She feels "very anxious all the time." Her past medical history is unremarkable. Her deceased sister had very high blood pressure. Her blood pressure is 230/110 mm Hg and pulse is 110/min. Initial laboratory studies reveal: WBC 7,000/cmm Hb 11.2 g/L Platelets 325,000/cmm Calcium 11.9 mg/dl What is the best next step in the evaluation of this patient?
Serum calcitonin levels
Nuclear renal scan
Endoscopy to look for ulcer disease
Echography of liver
CT scan of the head
A 39-year-old woman comes to the physician because of a "pins and needles" sensation around her mouth for the last 2-3 weeks. She gets similar sensations in her feet sometimes, along with muscle cramps, especially at the end of the day. She has no similar episodes in the past and has always been healthy. She works as a waitress and has "clean habits." Her family history is not significant. She is currently not taking any medications, and is allergic to penicillin. Her vital signs are normal. Examination is unremarkable. The patient's labs reveal: CBC: Hb 12.4 g/dl WBC 6,000/cmm Serum: Serum Na 140 mEq/L Serum K 4.0 mEq/L Chloride 100 mEq/L Bicarbonate 24 mEq/L BUN 10 mg/dl Serum creatinine 0.8 mg/dl Glucose 100 mg/dl Calcium 6.5 mg/dl Phosphorus, inorganic 5.8 mg/dl Protein: Total 7.0 g/dl Albumin 3.8 g/dl Globulins 3.0 g/dl Which of the following is the most likely cause of her condition?
Primary hypoparathyroidism
Osteomalacia
Primary hyperparathyroidism
Osteoporosis
Familial hypocalciuria
A 45-year-old male, found unconscious, is brought to the emergency room. His airway is maintained, and oxygen is administered. His temperature is 39.0C (102.5F), pulse is 102/min, blood pressure is 90/65 mm of Hg and respirations are 23/min. Intravenous access is secured and blood and urine samples are drawn. Lab results are as follows: Sodium 134 mEq/L Potassium 5.9 mEq/L Chloride 101 mEq/L Bicarbonate 22 mEq/L Blood urea nitrogen 110 mg/dl Glucose 1000 mg/dl Serum calcium 10.2 mg/dl Amylase 100 U/L Aspartate aminotransferase 15 U/L Alanine aminotransferase 17 U/L Ammonia 15 micro-moi/L (Normal is 9-33 micro-moi/L) PT 13 sec APTT 30 sec Arterial blood gases: PH 7.40 PaCO2 38 mm Hg PaO2 90 mm Hg Which of the following is the most appropriate initial infusion you should order for this patient?
Normal saline
Potassium
0.45% saline
Regular insulin
5% dextrose
Four of your patients who came to the office today all have signs and symptoms of hyperthyroidism. After the appropriate evaluation, you decided to treat them with radioactive iodine. Hyperthyroid patients with which of the following disorders are most likely to develop hypothyroidism following radioactive therapy?
Graves' disease
Thyroid Cancer
Ectopic production of thyroid hormones
Toxic adenoma
Multinodular goiter
A 60-year-old Caucasian male presents to the office with erectile dysfunction that progressed slowly over the last several months. He finds it difficult to obtain an erection, and has noted a decrease in nocturnal erections. His past medical history is significant for diabetes mellitus, type 2 and benign prostatic hypertrophy (BPH). His current medications are glyburide and doxazosin. Physical examination is insignificant. HbA1c level measured two weeks ago was 7.5%. He is asking about a prescription for sildenafil. Which of the following is the best statement concerning the treatment of erectile dysfunction in this patient?
Sildenafil and doxazosin should be given with at least a 4-hour interval
Sildenafil should not be combined with glyburide
Tightening of glycemic control improves erectile dysfunction
Prostaglandins (alprostadil) are preferred in this patient
Sildenafil is not a drug of choice for diabetics with erectile dysfunction
A 58-year-old asymptomatic male is found to have elevated levels of serum alkaline phosphate. His serum calcium and phosphate levels are normal. He denies any bone pain or deformity. His liver function tests are normal. The urinary hydroxyproline levels are increased. Nuclear bone scan reveals an increased uptake in the right scapula. Plain radiography confirms Paget's disease. Which of the following is the most appropriate next step in the management of this patient?
No treatment is indicated at this stage
Treatment with calcium and vitamin D
Treatment with bisphosphonates
Treatment with nasal calcitonin
A CT scan of lung
A 56-year-old male presents in the emergency department with severe nausea, vomiting, polyuria, polydipsia, and constipation. His past medical history is significant for hypertension and type 2 diabetes mellitus. His home medications include metformin, atenolol, and hydrochlorothiazide. He has a 26-pack-year history of smoking. He drinks alcohol occasionally. He denies the use of recreational drugs. His father also has diabetes mellitus type 2. His blood pressure is 110/70 mmHg, pulse is 102/min, temperature is 36.7C (98F) and respirations are 16/min. His mucus membranes are dry. His lung examination reveals decreased breath sounds over the right base. The rest of the physical examination is unremarkable. The patient is subsequently admitted. Laboratory studies (obtained in the emergency department) are as follows: Serum calcium 14.8 mg/dl Albumin 4.0 g/dl PTH 9 pg/ml (normal 10-60 pg/ml) Serum creatinine 1.9 mg/dl BUN 54 mg/dl Blood glucose 180 mg/dl 25-hydroxyvitamin D 30 ng/ml (normal 20 to 60 ng/ml) 1,25-dihydroxyvitamin D 30 pg/ml (normal 15 to 65 pg/ml) What is the most likely cause of this patient's hypercalcemia?
Hypercalcemia of malignancy
Dehydration
Primary hyperparathyroidism
Sarcoidosis
Hydrochlorothiazide-induced
A 23-year-old man presents to your office complaining of occasional headaches, muscle weakness and fatigue. He also describes periodic numbness of his extremities. The symptoms started 6 months ago and have gradually progressed. His past medical history is insignificant. He is not taking any medication. His blood pressure is 165/104 mm Hg and heart rate is 80/min. His physical examination is within normal limits. Which of the following laboratory findings is the most specific for the patient's condition?
High aldosterone/renin ratio
Low plasma renin activity
Metabolic alkalosis
Low serum potassium level
High serum sodium level
A 63-year-old otherwise healthy male presents with a thyroid nodule. He denies any symptoms of anxiety, heat or cold intolerance, and recent changes in appetite or weight. He has hypertension, which is being treated with a beta-blocker. He does not have any other medical problems. He denies any family history of thyroid disease. His pulse is 79/min and blood pressure is 130/76 mmHg. Neck examination shows a hard, fixed, non-tender, 4 cm thyroid nodule in the right thyroid lobe. His serum TSH level is normal. Fine needle aspiration biopsy (FNAB) shows follicular cells. Follicular carcinoma is suspected. Which of the following is necessary to make a diagnosis of follicular thyroid cancer?
Invasion of the tumor capsule and blood vessels
Lymph node involvement
Presence of Hurthle cells on biopsy
Secretion of calcitonin
Presence of psammoma bodies
A 28-year-old avid mountain climber and his friend are vacationing in Andes, South America. During their mountain climbing expedition, the pair somehow manages to get lost. It has been over 16 hours since their food supply ran out. Their glycogen stores are becoming depleted, and their bodies are beginning to utilize the process of gluconeogenesis. Which of the following intermediates is alanine being converted into during this process?
Pyruvate
Citrate
Glycerol-3-phosphate
Lactate
Transketolase
A 38-year-old Caucasian female presents to the office complaining of lethargy, weight gain and fatigue. She denies headaches, pruritus or urine discoloration. She just gave birth 2 months ago via vaginal delivery; her baby is in good health and receives formula nutrition. Her delivery was complicated by vaginal bleeding that required blood transfusion, and postpartum endometritis that rapidly responded to antibiotics. She has not had any menstrual periods following delivery. Physical examination shows sparse pubic hair, dry skin and delayed tendon reflexes. Urinalysis shows no glucose or ketones. Which of the following is most likely to be responsible for this patient's condition?
Lschemic necrosis
Drug effect
Autoimmune tissue destruction
Neoplasia
Infiltrative disorder
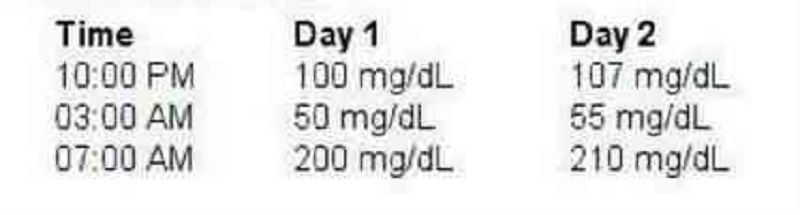
A 25-year-old female comes to the office for a follow-up visit. She was just diagnosed with type 1 diabetes mellitus a few days ago, when she presented at the emergency department with ketoacidosis. After successful management of her diabetic ketoacidosis (DKA), she was sent home on an insulin regimen with the following dosage: Before breakfast 10 units of NPH and 10 units of regular insulin Before supper 10 units of NPH and 4 units of regular insulin During this office visit, she shows the record of her fingerstick readings at home. Blood glucose levels were:. What is the most likely explanation for her 7:00 am blood glucose level?
Epinephrine, norepinephrine, & glucagon release
Decrease Insulin-secretor
Waning of insulin levels
Destruction of glucagon-secreting cells
Spikes of growth hormone release
A 58-year-old Caucasian male presents with polyuria and polydipsia for the past 4 months. He also reports easy bruising and difficulty in climbing stairs. He weighs 180 lbs (81.6kg) and is 5'7"(170cm) tall. His temperature is 37C (98.6F), pulse is 76/min, blood pressure is 155/100 mm Hg, and respirations are 15/min. Physical examination reveals significant proximal muscle weakness of all the extremities. Skin examination reveals significant pigmentation on the exposed areas. Lab studies show: Sodium 145 meq/L Potassium 2.9 meq/L Bicarbonate 30 meq/L Fa sting blood glucose 240 mg/dL Hemoglobin 13 g/dL WBC 14,000/micro-L Neutrophils 70% Lymphocytes 23% Monocytes 5% Basophils 1% Eosinophils 1% 24hr urinary free cortisol 1100 microgram Plasma ACTH 250 pg/mL (Normal 9-52 pg/mL). High dose dexamethasone suppression test did not decrease the 24 hr urinary cortisol excretion. Which of the following is consistent with this patient's findings?
Ectopic ACTH production
Cushing's disease
Exogenous glucocorticoids
Adrenal adenoma
Bilateral adrenal hyperplasia
A 56-year-old woman presents to the clinic with a 7-month history of headache and visual disturbance. Her past medical history is unremarkable. She is currently not taking any medications. She admits to smoking a pack of cigarettes daily for the last 15-years, and does not drink. On visual field examination, there is a small field defect noted in both eyes. MRI scan shows a pituitary tumor. Which of the following is the most common type of pituitary tumor?
Lactotroph adenoma
Thyrotroph adenoma
Somatotroph adenoma
Gonadotroph adenoma
Corticotroph adenoma
A 65-year-old Hispanic male comes to the office for a routine medical check-up. He has a history of diabetes for the past twenty years, and hypertension for the past ten years. His daily medications include insulin and ramipril. He was diagnosed with nonproliferative diabetic retinopathy at his last ophthalmologic visit. Reports from his previous laboratory studies show microalbuminuria. A detailed neurological examination is performed to check for any neuropathy. Which of the following is the most common type of neuropathy found in diabetics?
Symmetrical distal polyneuropathy
Proximal motor neuropathy
Mononeuropathy
Autonomic neuropathy
Mononeuropathy multiplex
A 46-year-old male comes to your office for a routine health examination. He has no current physical complaints and says he is compliant with his medications. His past medical history is significant for type 2 diabetes diagnosed two years ago that he has been able to control with diet, exercise and metformin. The patient also takes a daily aspirin. On physical examination, he has a temperature of 36.7C (98.F), a blood pressure of 140/86 mm Hg, a pulse of 80/min, and respirations of 14/min. His laboratory studies show: Total cholesterol 170 mg/dl High density lipoprotein (HDL) 50 mg/dl Low density lipoprotein (LDL) 65 mg/dl Triglycerides (TG) 150 mg/dl HbA1C 7.0 Serum chemistries are with in normal limits. Which of the following is the most appropriate next step in the management of this patient?
Add lisinopril
Add niacin
Add gemfibrozil
Add ezetimibe
Add insulin
A 60-year-old white male is hospitalized due to an acute myocardial infarction. His other medical problems include type 2 diabetes mellitus, hypertension, chronic obstructive pulmonary disease, and degenerative joint disease. He admits to smoking 2 packs of cigarettes daily for the past 20 years, as well as drinking 2 bottles of beer daily for the past 15 years. His medications include aspirin, glyburide, metoprolol, enalapril, heparin, and albuterol and ipratropium inhalers. His blood pressure is 140/80 mm Hg, pulse is 80/min, respirations are 16/min, and temperature is 36.7C (98.0F). During his stay in the hospital, a number of blood tests were ordered. Which of the following lab abnormalities is an indication for thyroid function testing?
Hyperlipidemia
Unexplained hypocalcemia
Unexplained hypernatremia
Thrombocytopenia
Neutropenia
A 60-year-old asymptomatic man presents to your office for a routine check-up. He has a 10-year history of type 2 DM, and a 12-year history of hypertension. His current medications include low- dose glyburide and a low-dose thiazide diureti His blood pressure is 140/90 mmHg and heart rate is 65/min. Physical examination shows a soft ejection systolic murmur at the base of the heart. Ophthalmoscopic evaluation reveals no abnormalities. ECG recorded 6 months ago showed left ventricular hypertrophy and non-specific ST segment and T-wave abnormalities. His recent fasting glucose level was in the range of 120 to 150 mg/dl, and HbA1c was 7.1 % (normal< 6%). 24-hour urine collection reveals microalbuminuria. Which of the following is the best measure to slow end- organ damage in this patient?
Increase the dose of glyburide
Increase the dose of thiazide diuretic
Switch to insulin
Add beta-blocker
Add ACE inhibitor
A 45-year-old unconscious male is brought to the emergency room. His airway is secured, oxygen is administered, and his vitals are as follows Temperature 364 C (97.8F); PR 102/min; BP 90/65 mm of Hg; RR 27/min. An IV line is secured and blood and urine samples are drawn. Lab results are as follows: Blood urea nitrogen 40 mg/dl Calcium 9.1 mg/dl ALT 50 U/L AST 60 U/L Ammonia 15 micro-mol/1 (Normal is 9-33 micro-mol/1) PT 13 sec APTT 30 sec Amylase 100 U/L Glucose 400 mg/dl Sodium 134 meq/L Potassium 5.2 meq/L Chloride 97 meq/L Bicarbonate 12 meq/L Arterial Blood Gases: PH 7.19 PaCO2 25 mm Hg PaO2 80 mm Hg Blood and urine are positive for ketones. A diagnosis of diabetic ketoacidosis (DKA) is made and IV infusion of normal saline and regular insulin are started. What will be a most reliable index for monitoring the response to treatment?
Serum anion gap
Urine glucose
Urine ketones
Serum osmolality
Serum ketones
A 27 -year-old woman presents to the office due to a significant amount of hair on her cheeks, chin and upper lips. This symptom developed over the past two months. Her last menstrual period was 12 weeks ago, but she did not seek medical help because her home pregnancy test was negative. Her medical history is unremarkable. She denies taking any medications other than oral contraceptive pills. Physical examination reveals acne on the forehead and cheeks; there is terminal hair on the upper lip, cheeks, chin, upper chest and lower abdomen. Examination of the genitals shows clitoromegaly. The abdominal exam is normal; the uterus is normal in size. Ultrasound reveals a normal uterus and ovaries, but there is a left adrenal mass. Which of the following measurements is most specific for this patient's condition?
Dehydroepiandrosterone-sulfate
Luteinizing hormone (LH)
Adrenocorticotropic hormone (ACTH)
Testosterone
Dihydrotestosterone
A 35-year-old white female presents with complaints of weight gain, lethargy and constipation for the last 2 months. She also complains of cold intolerance and oligomenorrhea. She is not taking any medication. She is a non-smoker, and does not drink alcohol. Her pulse is 67/min, and blood pressure is 130/90 mm Hg. She is afebrile. Her hands are dry and cold. There is a non-tender, diffuse rubbery enlargement of the thyroid gland without any discrete nodularity. She does not have exophthalmos, lid lag or lid retraction. Labs show decreased serum T4 levels, elevated serum TSH levels and positive anti-thyroperoxidase (TPO) antibodies. Which of the following complications may develop in this patient?
Lymphoma of the thyroid
Follicular carcinoma of the thyroid
Papillary carcinoma of the thyroid
Anaplastic carcinoma of the thyroid
Medullary carcinoma of the thyroid
A 35-year-old white female comes to her primary care physician for the evaluation of palpitations, weight loss, increased appetite and diarrhea for the past 2 months. She denies smoking cigarettes or drinking alcohol. Her temperature is 37.1C (98F), blood pressure is 135/80 mm Hg, respirations are 14/min, and pulse is 90/min. Physical examination shows exophthalmos, lid lag, lid retraction, and a diffusely enlarged, non-tender thyroid gland. Lab studies show very low levels of serum TSH, and increased levels of serum free T4 and T3. The diagnosis of Graves' disease is established. Various treatment options are discussed with the patient, and she opts for long-term treatment with propylthiouracil. Which of the following conditions is this patient at risk for developing?
Agranulocytosis
Hypocalcemia
Permanent hypothyroidism
Recurrent laryngeal nerve palsy
Thyroid cancer
A 16-year-old female presents to the office with her mother and complains of changes in her physical appearance over the past year. She first noted the appearance of dark hair on the cheeks, upper lips, around the nipples and umbilicus. Her menstrual cycles have always been irregular since her menarche at age 14. Her medical history is otherwise unremarkable. She denies taking any medications. She has a boyfriend, but claims that she is still not sexually active. Her blood pressure is 115/65 mm Hg, pulse is 80/min, respirations are 16/min, and temperature is 37 C (98F). Pelvic examination could not be performed, and abdominal examination is normal. Ultrasound is normal. Results of the initial work-up are as follows: Serum Na+ 140mEq/L Serum K+ 4.0mEq/L Serum Cl- 98 mEq/L Bicarbonate 25 mEq/L 1 7-alpha-hydroxyprogesterone elevated According to these findings, which of the following hormone deficiencies does this patient most likely have?
21-hydroxylase-deficiency
17 -alpha-hydroxylase-deficiency
11-beta-hydroxylase-deficiency
3-beta-hydroxysteroid-dehydrogenase deficiency
Cystathionine synthase deficiency
A 21-year-old man with type 1 diabetes mellitus presents to the emergency department with complaints of abdominal pain, nausea and vomiting. His temperature is 36.0C (97.0F), pulse is 110/min, blood pressure is 102/60 mm Hg, and respirations are 26/min. Lungs are clear to auscultation. Abdomen is soft, non-tender and non-distended. Chemistry panel shows: Sodium 130 mEq/L Potassium 5.2 mEq/L Chloride 90 mEq/L Bicarbonate 10 mEq/L Blood glucose 450 mg/dl Which of the following is the most appropriate next step in management?
Normal saline and regular insulin
5% dextrose and NPH insulin
0.45% saline and regular insulin
Normal saline and NPH insulin
Sodium bicarbonate
A 40-year-old female patient is brought to the office by her husband due to altered mental status and confusion of recent onset. According to her husband, she has been complaining of intense thirst, craving for ice water, and experiencing increased urination for the past few days. Her only medication is lithium for bipolar depression. Her temperature is 39.0C (102.5F), pulse is 102/min, blood pressure is 90/60 mm Hg, and respirations are 15/min. Physical examination reveals a disoriented patient with dry skin and mucous membranes. Blood chemistry panel reveals: Sodium 156 mEq/L Potassium 4.1 mEq/L Bicarbonate 26 mEq/L Blood glucose 1 02 mg/dl BUN 27 mg/dl Serum osmolality is 328mOsm/kg, and urine osmolality is 180mOsm/Kg. What is the most appropriate next step in the management of this patient?
IV infusion of normal saline
Water deprivation test
Plain water drinking
IV infusion of 5% dextrose
IV infusion of 045% saline
A 60-year-old Caucasian male presents to your office complaining of decreased hearing on the right side. He also feels that something is wrong with his head because his hat size had increased over the last two years. His past medical history is significant for hypertension and peptic ulcer disease. His current medications are hydrochlorothiazide and enalapril. He also takes ibuprofen for occasional headaches, and ranitidine for infrequent episodes of heartburn. Lab tests showed increased alkaline phosphatase levels. Which of the following is the most likely mechanism underlying this patient's condition?
Abnormal bone remodelling
Increased osteoid deposition
Bone demineralization
Abundant minerali zation of the periosteum
Fibrous replacement of the bone
A 40-year-old asymptomatic male comes to the office for a routine physical examination. His serum chemistry panel shows: Sodium 140 mEq/L Potassium 4.0 mEq/L Bicarbonate 25 mEq/L Chloride 101 mEq/L Calcium 11.8 mg/dL Albumin 4.0 g/dL Phosphorus 2.2 mg/dL 24-hour urine collection reveals a calcium level of 200 mg, and creatinine level of 1.7 g. Serum PTH level is increased. Bone mineral density by dual energy X-ray absorptiometry (DEXA) shows normal bone mineral density. Neck examination reveals no masses. What is the most appropriate next step in the management of this patient?
Surgical exploration of the neck
Bisphosphonate therapy
Medical surveillance
Thiazide diuretics
Loop diuretics
A 38-year-old woman presents with several months of decreased libido and a 4.5-kg (10-lb) weight gain. She has not had her menstrual period for the past 3 months. Physical examination is unremarkable except that a small amount of white discharge is manually expressed from the nipples bilaterally. The serum prolactin level is 300 ng/mL. Which of the following is the most appropriate first-line treatment?
Bromocriptine
Cortisol
Methyldopa
Metoclopramide
Octreotide
A 72-year-old woman presents to her physician complaining of fatigue, malaise, weight loss, and salt cravings. The patient has chronic obstructive pulmonary disease and is intermittently treated with corticosteroids but is not using home oxygen. Her oxygen saturation is 97% on room air with a blood pressure of 115/65 mm Hg, which is significantly lower than her baseline of 125/78 mm Hg. On auscultation she has good breath sounds bilaterally without wheeze, although the expiratory phase is slightly prolonged. Five weeks ago she received a corticosteroid treatment for an acute chronic obstructive pulmonary disease exacerbation, for which she was hospitalized and given 3 L of oxygen via nasal cannula. However, she admits that after discharge she was having continued difficulty breathing and did not follow the taper of the corticosteroids. The patient has smoked one pack of cigarettes per day for the past 51 years. Which of the following is the appropriate first step in the management of this patient?
Restart corticosteroids and follow a strict taper
3 L of oxygen via nasal cannula
X-ray of the chest
CT scan of the chest
Intravenous fluids
An obese patient with a long-standing history of type 2 DM presents to his primary care physician. On examination he has decreased sensation in both lower extremities. Upon questioning of his compliance with his prescribed medications, he reports that he has stopped taking one medication because it gave him flatulence and abdominal pain. Which of the following did this man most likely stop taking?
An α-glucosidase inhibitor
Sulfonylurea
Meglitinide
Thiazolidinedione
Metformin
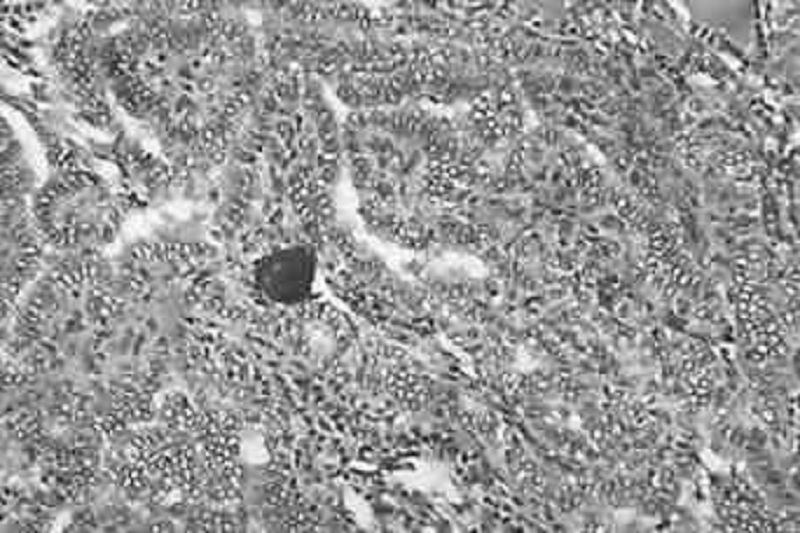
A 19-year-old G1P0 woman at 32 weeks’ gestation presents for scheduled prenatal appointment. The pregnancy has been uncomplicated to date. However, she mentions that she recently noticed a hard lump on her neck. She denies pain or difficulty swallowing, speaking, or breathing. Physical examination reveals a firm, nontender, immobile, solitary nodule on the left hemithyroid. Ultrasound reveals a solid 2-cm mass. There is no cervical lymphadenopathy. Thyroid function tests reveal a thyroid-stimulating hormone level of 1.2 μU/mL and free thyroxine level of 0.9 ng/dL. Results of fine-needle aspiration biopsy are shown in the image. Which of the following is the best next step in management?
Monitor until after delivery
Start methimazole
Left hemithyroidectomy
Radioablation therapy
Start propylthiouracil
A 49-year-old man presents to the clinic for a health maintenance visit. He has a family his- tory of type 2 DM. His medical history is significant for gastroesophageal reflux disease, for which he takes omeprazole and over-the-counter antacids. He smokes one pack of cigarettes per day and drinks an average of two beers per night. The patient’s body mass index is 32 kg/ m². Which of the following most greatly reduce(s) the patient’s risk of future coronary artery disease, renal failure, and retinopathy?
Weight loss and exercise
Alcohol avoidance
Daily multivitamin
Diet rich in fruit and vegetables
Smoking cessation
A 37 -year-old white female presents with galactorrhea and amenorrhea for the past 7 months. She denies any headaches, visual problems, vaginal dryness or dyspareunia. She is married, has two children, and remarks that her family is "complete." She does not use tobacco, alcohol or drugs. Her blood pressure is 120/80 mmHg, pulse is 72/min, temperature is 36.7C (98F) and respirations are 14/min. Visual field testing is within normal limits. Pregnancy test is negative. Her serum prolactin level is 150ng/ml. Pituitary MRI shows a 6mm pituitary adenoma. Which of the following is the most appropriate next step in the management of this patient?
Treatment with cabergoline
Radiotherapy
Treatment with estrogens
Surgery
Monitoring by serum prolactin and MRI
A 6-year-old boy presents to his pediatrician for a routine physical examination. His mother reports no problems over the past year except that he seems to be shorter than the other boys in his class. His mother is 163 cm (5'4") tall and experienced menarche at age 12 years, and his father is 178 cm (5'10") tall and went through puberty at approximately age 14 years. On his growth curve, the boy’s height was at the 10th percentile at birth, at the sixth percentile by age 3 years, and at the third percentile now. His weight is currently at the 25th percentile. Which of the following is most important in this patient’s evaluation?
Insulin-like growth factor-1 level
Chromosomal analysis
Colonoscopy
Growth hormone level
No further evaluation is necessary
A 32-year-old man presents to his primary care physician complaining of diffuse muscle weakness, dry and puffy skin, and patchy areas of hair loss on his scalp. He also notes numbness around his mouth and a tingling sensation in his hands and feet. He has a history of seizure disorder, and has been taking carbamazepine for the past 5 years. On physical examination he has dry skin and coarse, brittle hair with patchy alopecia. Tapping his right cheek causes contraction of the muscles at the corner of his mouth, nose, and eye on the right side. Which of the following could best have prevented the development of the patient’s current problem?
Vitamin D supplementation
Magnesium supplementation
Parathyroidectomy
Thyroid hormone
Vitamin C supplementation
A 16-year-old obese Hispanic girl presents to her physician’s office complaining of ugly skin around my neck‖ and having to wear turtlenecks. On examination the physician notes darkening and thickening of the skin, which has a velvety appearance. Which of the following is the most appropriate course of action?
Obtain a serum glucose test
Obtain a CT scan of the abdomen
Obtain a punch biopsy of the affected skin
Obtain a shave biopsy of the affected skin
Obtain liver function tests
A 24-year-old woman comes into the emergency department with recurrent episodes of palpitations, headache, and tremor. Her blood pressure is 155/95 mm Hg, heart rate is 135/ min, temperature is 37.9°C (100.2°F), and respiratory rate is 12/min. A CT of the abdomen shows a suprarenal mass. After confirming the diagnosis with a laboratory test, the physician informs the patient that she will require immediate therapy and surgical resection of the mass within the next few weeks. In order to achieve short-term control of her blood pressure, which of the following agents is most appropriate?
Prazosin
Furosemide
Hydralazine
Phenelzine
Propanolol
A 30-year-old Caucasian female comes to the physician's office because of polyuria and polydipsia of recent onset. She has no other medical problems. She does not use tobacco, alcohol or drugs. She has no known drug allergies. Her mother has diabetes. Her temperature is 36.7C (98F), pulse is 75/min, blood pressure is 110/70 mm Hg, and respirations are 15/min. The initial lab results are: Hb 12.7 g/dl WBC 5,000 /cmm Platelets 380,000/cmm Blood glucose 90 mg/dl Serum sodium 142 mEq/L Serum potassium 4.0 mEq/L Bicarbonate 26 mEq/L BUN 15 mg/dl Serum creatinine 0.9 mg/dl Serum uric acid 9 mg/dl Serum osmolality 295 mOsm/kg Urine osmolality 160 mOsm/kg After 12 hours of water deprivation, lab testing reveals: Serum sodium 151 mEq/L Serum potassium 4.2 mEq/L Bicarbonate 26 mEq/L Serum osmolality 300 mOsm/kg Urine osmolality 186 mOsm/kg One hour after the subcutaneous administration of arginine vasopressin, the urine osmolality is 400mosm/kg. Which of the following is the most appropriate treatment for this patient?
Intranasal desmopressin acetate
Psychotherapy
Indomethacin
Hydrochlorothiazide
Demeclocycline

A 30-year-old female complains of palpitations, fatigue, and insomnia. On physical examination, her extremities are warm and she is tachycardia. There is diffuse thyroid gland enlargement and proptosis. There is thickening of the skin in the pretibial area. Mild clubbing of digits is present. Which of the following laboratory values would you expect in this patient?
Increased free thyroxine, decreased TSH
Increased free thyroxine (free T4), increased TSH
Increased free thyroxine, normal TSH
Normal free thyroxine, elevated triiodothyronine (T3), normal TSH
Normal free thyroxine, decreased TSH
A 45-year-old woman with chronic alcohol abuse admitted 3 days ago for nausea and severe diarrhea now complains of perioral and finger tingling. She was admitted for hydration after 1 week of severe watery diarrhea. She has been receiving intravenous hydration and dextrose but has not been able to take oral nutrition secondary to continued nausea. Her blood pressure is 130/74 mm Hg, pulse is 68/min, and respiratory rate is 16/min. She is afebrile. Physical examination is significant for facial twitching on percussion of her facial nerve just anterior to the ear, as well as the induction of carpal spasm after the inflation of a blood pressure cuff on her arm. Which of the following is most likely to have caused these findings?
Hypomagnesemia
Azotemia
Hypernatremia
Hypophosphatemia
Hypouricemia
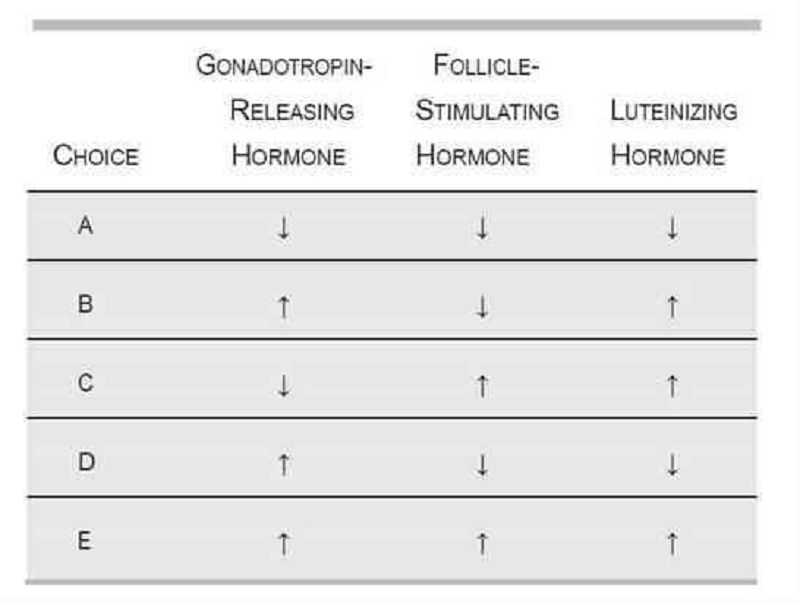
A 17-year-old girl has never had a menstrual period. On physical examination, she has minimal breast development and no axillary or pubic hair. She is color blind and has had a diminished sense of smell since birth. Laboratory evaluation would most likely reveal which of the following?
A
B
C
D
E
A 65-year-old black female presents for an annual examination. Physical examination is unremarkable for her age. In completing the appropriate screening tests, you order a dual x-ray absorptiometry (DXA) to evaluate whether the patient has osteoporosis. DXA results reveal a T-score of -3.0 at the total hip and −2.7 at the spine, consistent with a diagnosis of osteoporosis. Since her Z- score is -2.0, you proceed with an initial evaluation of secondary osteoporosis. Laboratory evaluation reveals: Calcium: 9.7 mg/dL Cr: 1.0 mg/dL Bun: 19 mg/d Glucose: 98 mg/dL 25,OH vitamin D: 12 ng/mL (optimal > 25) WBC: 7700/μL Hg: 12 g/dL HCT: 38 g/dL PLT: 255,000/μL Based on the above information, additional laboratory would most likely reveal which of the following?
Elevated iPTH, normal ionized calcium, elevated alkaline phosphatase
Elevated iPTH (intact parathormone), low ionized calcium, normal alkaline phosphatase
Normal iPTH, normal ionized calcium, elevated alkaline phosphatase
Normal iPTH, low ionized calcium, elevated alkaline phosphatase
Elevated iPTH, low ionized calcium, normal alkaline phosphatase
A 58-year-old male is referred to your office after evaluation in the emergency room for abdominal pain. The patient was diagnosed with gastritis but a CT scan with contrast performed during the workup of his pain revealed a 2-cm adrenal mass. The patient has no history of malignancy and denies erectile dysfunction. Physical examination reveals a BP of 122/78 with no gynecomastia or evidence of Cushing syndrome. His serum potassium is normal. What is the next step in determining whether this patient’s adrenal mass should be resected?
Plasma metanephrines and dexamethasone-suppressed cortisol level.
Plasma aldosterone/renin ratio.
Estradiol level.
Repeat CT scan in 6 months.
Testosterone level.
A 42-year-old woman with no significant past medical history presents for a routine health maintenance visit. On physical examination a solitary nodule is palpated in the thyroid. She denies pain, dysphagia, or hoarseness. She also denies fatigue, weight change, heat or cold intolerance, diarrhea, or constipation. There is no family history of thyroid cancer. Her serum thyroid-stimulating hormone level is normal. Which of the following is the most appropriate next step in evaluation?
Fine-needle aspiration
MRI
Radionuclide scan
Thyroid lobectomy
Ultrasonography
A 60-year-old man presents to his primary care physician for routine medical care. He has no complaints, takes no medications, and has a family history of DM. Examination is unremarkable. A screening laboratory test reveals a fasting blood glucose level of 152 mg/dL. One week later the test is repeated and a value of 144 mg/dL is obtained. Which of the following is the most likely cause of these findings?
Peripheral insulin resistance
Autoimmune destruction of pancreatic islet cells
Pancreatitis
Patient’s findings represent normal laboratory values
Surreptitious insulin injection
A 65-year-old man presents with a 1-day history of hematuria and sharp flank pain (rated 10 of 10) radiating toward the groin on the right side. Past medical history is significant for three prior episodes of nephrolithiasis over the past 5 years, all of which presented with a similar clinical picture. He is not taking any medication. There is no family history of renal calculi, renal disease, or endocrine disorders. His temperature is 36.9°C (98.5°F), heart rate is 125/ min, and blood pressure is 132/86 mm Hg. He is in obvious distress and cannot sit still on the bed. Physical examination is significant for a soft, nontender abdomen and extreme costovertebral angle tenderness on the right. Laboratory values show: Na+: 142 mEq/L K+: 4.8 mEq/L Cl−: 104 mEq/L HCO −: 24 mEq/L Ca2+: 11.0 mg/dL PO4: 1.4 mg/dL Mg2+: 2.0 mg/dL Blood urea nitrogen: 12 mg/dL Creatinine: 1.0 mg/dL Glucose: 118 mg/dL Intact parathyroid hormone: 300 pg/mL Which of the following is the most likely diagnosis?
Primary hyperparathyroidism
Malignancy
Milk-alkali syndrome
Sarcoidosis
Secondary hyperparathyroidism
A 90-year-old male complains of hip and back pain. He has also developed headaches, hearing loss, and tinnitus. On physical examination the skull appears enlarged, with prominent superficial veins. There is marked kyphosis, and the bones of the leg appear deformed. Serum alkaline phosphatase is elevated. Calcium and phosphorus levels are normal. Skull x-ray shows sharply demarcated lucencies in the frontal, parietal, and occipital bones. X-rays of the hip show thickening of the pelvic brim. Which of the following is the most likely diagnosis?
Paget disease
Multiple myeloma
Vitamin D intoxication
Osteitis fibrosa cystica
Metastatic bone disease
A 35-year-old white male presents with fatigue, decreased appetite, weight gain, constipation and cold intolerance. He cannot recall any stressful event. He does not take any medications. He is a non- smoker and non-alcoholi His pulse is 47/min and blood pressure is 145/91 mmHg. Physical examination reveals cool, pale skin, coarse hair, and brittle nails. There is delayed relaxation of deep tendon reflexes. The thyroid gland is normal on palpation. Laboratory studies reveal increased serum free T3 and T 4 levels, and normal serum TSH level. Which of the following is the most likely diagnosis?
Generalized resistance to thyroid hormones
Primary hypothyroidism
Secondary hypothyroidism
Subclinical hypothyroidism
Graves' disease
A 36-year-old white female comes to the office due to swelling in front of her neck. She denies any hoarseness, dysphagia, fever, chills, diarrhea, constipation, heat or cold intolerance, and changes in appetite or weight. Her menstrual cycles are regular. She does not have any history of head and neck irradiation. Her family history is negative for thyroid problems. Her blood pressure is 130/80mm Hg, pulse is 80/min, respirations are 16/min, and temperature is 36.7C (98.0F). Examination of the neck shows a 2 x 2 cm, discrete, non-tender, firm, mobile nodule in the left thyroid lobe. There is no cervical lymphadenopathy. The rest of the examination is normal. Which of the following is the most appropriate next step in the evaluation of this patient?
Measurement of TSH
Measurement offree T4 and anti-thyroid antibodies
Radionuclide scan with iodine 131
Fine needle aspiration biopsy
Ultrasound of the thyroid gland
A 65-year-old diabetic male with acute myocardial infarction complicated by cardiogenic shock is admitted in the coronary care unit. His hospital course was complicated by acute renal failure and lower GI bleeding from anticoagulation therapy. His thyroid hormone studies are abnormal. He does not have any previous history of thyroid disease. Physical examination of the thyroid gland is normal. Labs show: Triiodothyronine (T3), serum 1.4 nmol/L (normal 1.8-29 nmol/L) Thyroxine (T 4), serum 6.0 micro-g/dL (normal 5-12 micro-g/dL) Thyroid-stimulating hormone, serum 2.0 micro-U/mL Which of the following is the most likely diagnosis?
Sick euthyroid syndrome
Primary overt hypothyroidism
Subclinical hypothyroidism
Central hypothyroidism
Reidels thyroiditis
A 45-year-old male presents to your office because his "hands are getting thick and swollen." He is also having difficulty with wearing shoes because his feet have become large. His blood pressure is 150/90 mm Hg. On examination, he has enlarged, swollen hands and feet. He has coarse facial features, with prominent frontal bones and jaws. While you are discussing the most likely diagnosis, he appears worried and asks about the complications and risk of death associated with his condition. What is the most common cause of death in patients with this condition?
Congestive cardiac failure
Hypertensive nephropathy
Stroke
Brain tumor
Adrenal failure
A 40-year-old African American female comes to you for her routine medical check-up. She admits to smoking one pack of cigarettes daily for the last 20 years. Her mother and one maternal uncle have diabetes. Her height is five feet six inches, and weight is 130 lbs. Her blood pressure is 122/80 mm Hg, pulse is 80/min, respirations are 16/min, and temperature is 37C (98F). What is the most appropriate screening test for diabetes mellitus?
Blood glucose measurement after an 8 hour fast
Random blood glucose measurement
50 g glucose tolerance test
75 g glucose tolerance test
100 g glucose tolerance test
A 41-year-old woman presents to the emergency department with palpitations. On questioning she notes heat intolerance, nervous- ness, and insomnia. On physical examination the physician notes a fine tremor, diffuse non-pitting edema of the anterior lower leg, and bulging of both of her eyes. What finding on blood test would confirm the diagnosis?
Anti-thyroid-stimulating hormone receptor antibodies
Decreased thyroid-stimulating hormone levels
Increased creatine kinase-myocardial bound
Increased thyroid-stimulating hormone levels
Positive antinuclear antibody
A 17-year-old girl presents to the clinic because she has not yet menstruated and does not have significant breast development. Family history is significant only for some cousins who are color blind. The patient denies ethanol, tobacco, and illicit drug use and sexual activity. Physical examination reveals a normal-appearing girl in no acute distress with minimal breast development and a lack of pubic hair. She is 168 cm (5'6") tall and weighs 61.2 kg (135 lb). Cardiac examination reveals no murmurs, rubs, or gallops, with point of maximal impulse at the left mid-clavicular line between the third and fourth intercostal space. Gynecologic examination reveals a vagina without rugae and a cervix that is easily visualized. There is no discharge. A urine test is negative for β- human chorionic gonadotropin. Which of the following is the most likely diagnosis?
Kallmann’s syndrome
Androgen insensitivity syndrome
Gonadal dysgenesis
Kartagener’s syndrome
Pregnancy
A 26-year-old man presents with increased thirst, urinary frequency, and nocturia over the past several months. Physical examination is unremarkable. Twenty-four-hour urine osmolarity is <300 mOsm/L. A fluid deprivation test does not result in an increased urine osmolarity. Administration of 0.03 μg/kg of desmopressin results in a urine osmolarity of 450 mOsm/L after 2 hours. Which of the following is the most likely diagnosis?
Central diabetes insipidus
Diabetes mellitus
Nephrogenic diabetes insipidus
Psychogenic polydipsia
Syndrome of inappropriate secretion of ADH

A 6-year-old boy is brought to his pediatrician for a routine check-up. He has not been seen by a physician for the past 3 years. Recently, he has developed some patchy areas of hair loss on his scalp. The mother also notes he has had many colds over the past year. She says he has developed normally, although he started walking later than her other two children. On physical examination his wrists appear enlarged, and he has bowing of the forearms and legs. X-ray of the boy’s legs is shown in the image. Laboratory tests show a calcium level of 7.1 mg/dL, phosphate of 1.8 mg/dL, and intact parathyroid hormone of 130 pg/mL (normal: 10–65 pg/mL). Vitamin D level is normal. Treatment with vitamin D does not correct the patient’s hypocalcemia. Which of the following disorders best explains this patient’s findings?
Vitamin D-resistant rickets
Dietary vitamin D deficiency
Hypoalbuminemia
Primary hyperparathyroidism
Pseudohypoparathyroidism
A 28-year-old woman presents to her gynecologist for her annual examination. She mentions that she and her husband have been trying to conceive for 9 months without success and that her menstrual cycles have become irregular. Her gynecologist suggests that she and her husband continue to try to conceive and that the woman return in 3 months for some laboratory studies if she still has not become pregnant. In the interim, a routine visit to the ophthalmologist reveals bitemporal hemianopsia. Which of the following is the most likely cause of this woman’s infertility?
Suppression of ovulation
Ectopic endometrial tissue
Failure of implantation
Hostile cervical mucus
Ovarian unresponsiveness to gonadotro- pins
A 4-year-old boy is brought to the pediatrician by his worried mother. She notes that he urinates 10 times a day and is always drinking water. She also reports that despite eating more than either of his brothers did at the same age, he is not gaining any weight. Which of the following human leukocyte antigen (HLA) types is associated with the most likely diagnosis for this child?
HLA-DR3
HLA-B27
HLA-B51
HLA-D11
HLA-DR2
A patient comes to your office for a new-patient visit. He has moved recently to your city due to a job promotion. His last annual examination was 1 month prior to his move. He received a letter from his primary physician stating that laboratory workup had revealed an elevated alkaline phosphatase and that he needed to have this evaluated by a physician in his new location. On questioning, his only complaint is pain below the knee that has not improved with over-the-counter medications. The pain increases with standing. He denies trauma to the area. On examination you note slight warmth just below the knee, no deformity or effusion of the knee joint, and full ROM of the knee without pain. You order an x-ray, which shows cortical thickening of the superior fibula and sclerotic changes. Laboratory evaluation shows an elevated alkaline phosphatase of 297 mg/dL with an otherwise normal metabolic panel. Which of the following is the treatment of choice for this patient?
Bisphosphonate
Melphalan and prednisone
Nonsteroidal anti-inflammatory
Ursodeoxycholic acid (UDCA)
Observation
Your patient is a 48-year-old Hispanic male with a 4-year history of diabetes mellitus type 2. He is currently utilizing NPH insulin/Regular insulin 40/20 units prior to breakfast and 20/10 units prior to supper. His supper time has become variable due to a new job and ranges from 5 to 8 PM. In reviewing his glucose diary, you note some very low readings (40-60 mg/dL) during the past few weeks at 3 AM. When he awakens to urinate, he feels sweaty or jittery so has been checking a fingerstick blood glucose. Morning glucose levels following these episodes are always higher (200- 250) than his average fasting glucose level (120-150). Which change in his insulin regimen is most likely to resolve this patient’s early AM hypoglycemic episodes?
Change regimen to glargine at bedtime with lispro prior to each meal.
Increase morning NPH and decrease evening NPH.
Discontinue both NPH and regular insulin; implement sliding scale regular insulin with meals.
Decrease morning NPH and decrease evening regular insulin.
Change regimen to glargine at bedtime and continue morning and evening regular insulin.
A 40-year-old alcoholic male is being treated for tuberculosis, but he has not been compliant with his medications. He complains of increasing weakness, fatigue, weight loss, and nausea over the preceding three weeks. He appears thin, and his blood pressure is 80/50 mm Hg. There is increased pigmentation over the elbows and in the palmar creases. Cardiac examination is normal. Which of the following is the best next step in evaluation?
Early morning serum cortisol and cosyntropin stimulation
CBC with iron and iron-binding capacity
Erythrocyte sedimentation rate
Esophagogastroduodenoscopy (EGD)
Blood cultures
A 48-year-old woman presents to her primary care physician because of 2 weeks of neck pain. The pain is constant and sharp (rated at 10 of 10) and is felt in the anterior portion of her neck. She also notes several weeks of loose stools and fatigue. Past medical history is significant for a viral upper respiratory infection about 1 month ago. She has a temperature of 37.9°C (100.2°F), heart rate of 96/min, and blood pressure of 136/82 mm Hg. On neck examination there is diffuse enlargement of the thyroid and it is exquisitely tender to even mild palpation. Laboratory tests show a total tri- iodothyronine level of 280 ng/dL, total thyroxine of 25 μg/dL, and thyroid-stimulating hormone of 2 μU/mL (normal: 0.4–4 μU/L). Which of the following is the most likely diagnosis?
Subacute granulomatous thyroiditis
Acute infectious thyroiditis
Drug-induced thyroiditis
Hashimoto’s thyroiditis
Riedel’s thyroiditis
A 74-year-old woman is brought to the emergency department by her daughter. The daughter states that her mother lives alone and has no significant medical problems. She says that she last saw her mother a month prior, before she left on an extended business trip. When she returned, she found her mother appeared restless and very nervous. She also appeared to have lost a noticeable amount of weight. The patient told her daughter that she had been having increased frequency of bowel movements, and felt like her heart was beating fast and funny, and that she felt like she might be coming down with a cold. Initial evaluation in the emergency department reveals sinus tachycardia and a painful, enlarged thyroid. Which of the following is the most likely etiology of her symptoms?
Subacute granulomatous thyroiditis
Autoimmune thyroiditis
Graves’ disease
Medication-induced hyperthyroidism
Toxic multinodular goiter
An 18-year-old woman presents to the emergency department with acute mental status changes, rapid and deep breathing, abdominal pain, and vomiting. On examination she is tachypneic and tachycardic, her abdomen is soft and nontender, and her mucous membranes are dry. Laboratory values are notable for a potassium level of 5.5 mEq/L, bicarbonate of 12 mEq/L, and serum glucose of 400 mg/dL. Which of the following is the most appropriate strategy during the first 24 hours?
Intravenous fluids, insulin, and potassium
Intravenous fluids, insulin, and strict potassium restriction
Diuresis, strict potassium restriction, and insulin
Diuresis and ventilatory support
Intravenous fluids, loop diuretic, and potassium
A 32-year-old G2P1 woman at 16 weeks’ gestation presents to her obstetrician complaining of fatigue, anxiety, and palpitations. She says she has been feeling warm, even in her air-conditioned home, and has been having three or four loose stools per day, as compared to one or two prior to her pregnancy. She has a temperature of 37.1°C (98.9°F), heart rate of 105/min, and blood pressure of 128/76 mm Hg. Neck examination reveals mild diffuse enlargement of the thyroid gland with no lymphadenopathy. Relevant laboratory findings include a total triiodothyronine level of 400 ng/dL, free thyroxine of 6.8 ng/dL, and thyroid-stimulating hormone of 0.01 μU/mL (normal: 0.4–4 μU/L). Results of a thyroid- stimulating hormone-receptor antibody test are positive. Which of the following is the most appropriate therapy for this patient?
Propylthiouracil
High-dose iodine therapy
Methimazole
Radioiodine ablation
Surgical resection
A 32-year-old woman undergoes a cesarean section because of failure of labor to progress, and delivers a healthy baby boy. The procedure is complicated by significant intraoperative blood loss and hypotension, but the patient is successfully resuscitated. Postoperatively she experiences dull, aching, non-localized abdominal pain and nausea, but denies headache, visual changes, or abnormal edema. On postoperative day three she is passing flatus and remains afebrile, but becomes hypotensive to 90– 100 mm Hg systolic and 40–50 mm Hg diastoli She has not begun lactating despite her attempts to breast-feed her infant. Laboratory values indicate that she is hyponatremic and mildly hyperkalemi Urinalysis and liver enzymes are normal. Which of the following is the most likely cause of her symptoms?
Sheehan’s syndrome
Postoperative infection
Appendicitis
HELLP syndrome
Toxic shock syndrome
A 50-year-old obese female is taking oral hypoglycemic agents. While being treated for an upper respiratory infection, she develops lethargy and is brought to the emergency room. Neurological examination is nonfocal; she does not have neck rigidity. Laboratory results are as follows: Na: 134 mEq/L K: 4.0 mEq/L HCO3: 25 mEq/L Glucose: 900 mg/dL BUN: 84 mg/dL Creatinine: 3.0 mg/dL HgA1c: 6.8% BP: 120/80 lying down, 105/65 sitting Which of the following is the most likely cause of this patient’s coma?
Hyperosmolar coma
Diabetic ketoacidosis
Inappropriate ADH
Bacterial meningitis
Noncompliance with medication
A 24-year-old white male presents with a persistent headache for the past few months. The headache has been gradually worsening and not responding to over-the-counter medicines. He reports trouble with his peripheral vision which he noticed while driving. He takes no medications. He denies illicit drug use but has smoked one pack of cigarettes per day since the age of 18. Past history is significant for an episode of kidney stones last year. He tells you no treatment was needed as he passed the stones, and he was told to increase his fluid intake. Family history is positive for diabetes in his mother and a brother (age 20) who has had kidney stones from too much calcium and a “low sugar problem.” His father died of some type of tumor at age 40. Physical examination reveals a deficit in temporal fields of vision and a few subcutaneous lipomas. Laboratory results are as follows: Calcium: 11.8 mg/dL (normal 8.5-10.5) Cr: 1.1 mg/dL Bun: 17 mg/dL Glucose: 70 mg/dL Prolactin: 220 μg/L (normal 0-20) Intact parathormone: 90 pg/mL (normal 8-51) You suspect a pituitary tumor and order an MRI which reveals a 0.7 cm pituitary mass. Based on this patient’s presentation, which of the following is the most probable diagnosis?
Multiple endocrine neoplasia Type 1 (MEN 1)
Tension headache
Primary hyperparathyroidism
Multiple endocrine neoplasia Type 2A (MEN 2A)
Prolactinoma
A 53-year-old woman presents to the clinic with complaints of headache and blurred vision for the past several months. She also says her family has commented that her face looks different, and her nose is bigger than it used to be. In addition, she says her shoes feel tighter. On physical examination she has coarse facial features with a prominent mandible and widely spaced incisors. MRI of the brain reveals a mass in the pituitary. This patient may be at increased risk of developing which of the following malignancies?
Colon cancer
Hepatocellular carcinoma
Lung cancer
Malignant brain tumor
Pancreatic adenocarcinoma
A 13-year-old boy is brought to the pediatrician by his mother because of increasing body hair. Several months earlier he had been diagnosed with 17α-hydroxylase deficiency and treated with hydrocortisone. Physical examination reveals an overweight boy with a moderate amount of both chest and genital hair, and some facial hair growth. His physical examination is otherwise unremarkable. Which of the following is the best treatment for this patient?
Add dexamethasone
Add cosyntropin
Add spironolactone
Increase hydrocortisone
Keep the current dose of hydrocortisone
A 72-year-old man with atrial fibrillation presents with complaints of fatigue and feeling cold. He also notes constipation and dry skin. His daughter states he has seemed more forgetful over the past several months. His temperature is 37.3°C (99.1°F), heart rate is 48/min, and blood pressure is 130/82 mm Hg. Cardiac examination shows bradycardia but normal rhythm, and normal S1 and S2 with no murmurs; the lungs are clear to auscultation bilaterally and the abdomen is soft and nontender. The patient’s extremities are cool and puffy with dry, coarse skin. Laboratory studies show a thyroid- stimulating hormone level of 32 μU/L, free thyroxine of 0.3 ng/dL, and total tri-iodothyronine of 30 ng/dL. What medication is the patient likely taking for his atrial fibrillation?
Amiodarone
Flecainide
Lithium
Methimazole
Sotalol
A 50-year-old female is 5 ft 7 in tall and weighs 185 l There is a family history of diabetes mellitus. Fasting blood glucose (FBG) is 160 mg/dL and 155 mg/dL on two occasions. HgA1c is 7.8%. You educate the patient on medical nutrition therapy. She returns for reevaluation in 8 weeks. She states she has followed diet and exercise recommendations but her FBG remains between 130 and 140 and HgA1C is 7.3%. She is asymptomatic, and physical examination shows no abnormalities. Which of the following is the treatment of choice?
Metformin
Encourage compliance with medical nutrition therapy
Observation with repeat HgA1C in 6 weeks.
Thiazolidinediones
Insulin
A 58-year-old postmenopausal female presents to your office on suggestion from a urologist. She has passed 3 kidney stones within the past 3 years. She is taking no medications. Her basic laboratory work shows the following: Na: 139 mEq/L K: 4.2 mEq/L HCO3: 25 mEq/L Cl: 101 mEq/L BUN: 19 mg/dL Creatinine: 1.1 mg/dL Ca: 11.2 mg/dL A repeat calcium level is 11.4 mg/dL; PO4 is 2.3 mmol/L (normal above 2.5). Which of the following tests will confirm the most likely diagnosis?
Intact parathormone (iPTH) level
Serum ionized calcium
Thyroid function profile
24-hour urine calcium
Liver function tests
A 49-year-old woman presents to her physician’s office with a long-standing history of polydipsia, polyuria, central obesity, and hyperlipidemia. She is currently taking metformin, a sulfonylurea, and an angiotensin-converting enzyme (ACE) inhibitor. ACE inhibitors are most beneficial in preventing or slowing the progression of which of the following diabetic complications?
Diabetic nephropathy
Diabetic ketoacidosis
Diabetic neuropathy
Diabetic retinopathy
Peripheral vascular disease
A 42-year-old woman presents to her physician with complaints of fever (38.2°C [100.8°F]) and mild-to-moderate anterior neck pain. On examination the physician finds her to be tachycardic and sweating, and to have an exquisitely tender thyroid gland. Her blood work shows a depressed thyroid- stimulating hormone level and increased free thyroxine. Which of the following is the most appropriate treatment at this time?
Ibuprofen
Acetaminophen
Levothyroxine
Prednisone
Radioactive iodine
A 53-year-old woman suffers from long-standing obesity complicated by DJD of the knees, making it difficult for her to exercise. Recently her fasting blood glucose values have been 148 mg/dL and 155 mg/dL; you tell her that she has developed type 2 diabetes. She wonders if diet will allow her to avoid medications. In addition, her daughter also suffers from obesity and has impaired fasting glucose, and the patient wonders about the management of her prediabetes. Which of the following is a correct statement based on the American Diabetes Association 2008 guidelines regarding nutrition recommendations and interventions for diabetes?
Outcomes studies show that medical nutrition therapy (MNT) can produce a 1 to 2-point decrease in hemoglobin A1c in type 2 diabetics.
Low-carbohydrate diets such as “South Beach” and “Atkins” should be avoided.
Prediabetic patients should be instructed to lose weight and exercise but a referral to a medical nutritionist is not necessary until full-blown diabetes is diagnosed.
Bariatric surgery may be considered for patients with type 2 diabetes and a BMI of > 30 kg/m2.
Very low-calorie diets (< 800 cal/day) produce weight loss that is usually maintained after the diabetic patient returns to a self-selected diet.
A 45-year-old G2P2 female presents for annual examination. She reports regular menstrual cycles lasting 3 to 5 days. She exercises 5 times per week and reports no difficulty sleeping. Her weight is stable 140 lbs and she is 5 ft 8 in tall. Physical examination is unremarkable. Laboratory studies are normal with the exception of a TSH value of 6.6 mU/L (normal 0.4-4.0 mU/L). Which of the following represents the best option for management of this patient’s elevated TSH?
Repeat TSH in 3 months and reassess for signs of hypothyroidism.
Begin low dose levothyroxine (25-50 μg/d).
Recommend dietary iodide supplementation
Measure thyroid peroxidase antibodies (TPOAb).
Order thyroid uptake scan.
A 26-year-old man with a history of kidney stones presents with 1 week of severe burning epigastric pain. He also notes several days of diarrhea and nausea but denies emesis or fever. His family history is remarkable for a paternal uncle with pancreatic cancer. His temperature is 37°C (98.6°F), heart rate is 88/min, respiratory rate is 16/min, and blood pressure is 125/85 mm Hg. Abdominal examination is significant for tenderness in the mid-epigastrium. Upper endoscopy reveals a 1cm ulceration in the first part of the duodenum. This is the third episode of confirmed peptic ulcers in this patient. Laboratory studies show: Na+: 140 mEq/L K+: 4.9 mEq/L Cl−: 105 mEq/L HCO −: 25 mEq/L Ca2+: 12.0 mg/dL PO4: 1.4 mg/dL Mg2+: 2.0 mg/dL Blood urea nitrogen: 10 mg/dL Creatinine: 1.0 mg/dL Glucose: 87 mg/dL Which of the following is most likely to be found in this patient?
Prolactinoma
Medullary thyroid carcinoma
Papillary thyroid carcinoma
Pheochromocytoma
Squamous cell lung cancer
An obese 18-year-old woman is brought to the emergency department by her mother, who noted that she had been lethargic all day, and suffered a brief, seizure-like episode. One month earlier, the patient had been started on medication for type 2 DM. Lactic acid levels are normal. Which of the following medications most likely played a role in the patient’s current presentation?
A sulfonylurea
A statin
A thiazolidinedione
An α-glucosidase inhibitor
Metformin
A 75-year-old woman is brought to the emergency department after being found unresponsive at her home. She was last spoken to by her daughter on the phone 24 hours earlier, at which time she complained of chills, lethargy, and weakness. The woman has had a heart at- tack in the past, she has high blood pressure, and she had a total thyroidectomy performed a decade ago for cancer. The daughter had re- turned from several months out of town, and is unsure if the patient was taking her medications. Her temperature is 34.9°C (94.9°F), pulse is 48/min, blood pressure is 110/65 mm Hg, oxygen saturation is 99% on 100% oxygen, and glucose is 85 mg/dL. On examination the patient is unresponsive, obese, and edematous with periorbital edema. Her cardiac and pulmonary examinations are normal. CT of the head reveals no signs of trauma or increased intracranial pressure, and ECG demonstrates no acute ischemic changes. Blood is drawn for laboratory testing. Which of the following is most appropriate for treating the patient’s mental status change?
Levothyroxine
Aspirin
Glucagon
Hemodialysis
Metoprolol
A family brings their 82-year-old grandmother to the emergency room stating that they cannot care for her anymore. They tell you, “She has just been getting sicker and sicker.” Now she stays in bed and won’t eat because of stomach pain. She has diarrhea most of the time and can barely make it to the bathroom because of her weakness. Her symptoms have been worsening over the past year, but she has refused to see a doctor. The patient denies symptoms of depression. Blood pressure is 90/54 with the patient supine; it drops to 76/40 when she stands. Heart and lungs are normal. Skin examination reveals a bronze coloring to the elbows and palmar creases. What laboratory abnormality would you expect to find in this patient?
Low serum Na+
Low serum Ca+
Low serum K+
Normal serum K+
Microcytic anemia
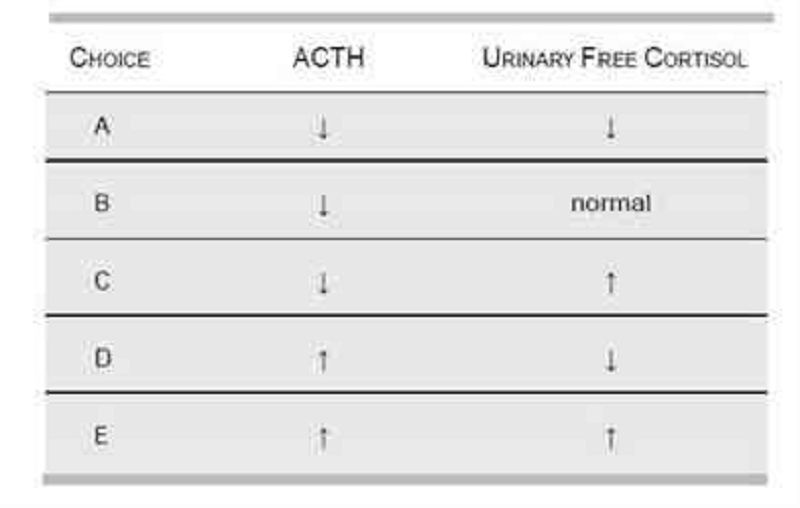
A 14-year-old boy presents at the pediatric clinic for a routine check-up. The patient had developed end-stage renal disease over the previous 2 years, and was successfully treated with a renal transplant 6 months prior. Since his operation, he has developed purple striae on his back and arms, central obesity, and an increasingly round face. During the subsequent blood analysis, which of the following results would be most likely?
A
B
C
D
E
A 64-year-old man presents to the emergency department after a motor vehicle crash and receives a CT of the abdomen that shows a finding of a unilateral mass in the left adrenal gland. He is unharmed from the accident, feels well, and has never smoked. His blood pressure is 155/90 mm Hg, deep tendon reflexes are 3/4, and muscle strength is 4/5. Laboratory studies show: Na+: 150 mEq/L K+: 3.0 mEq/L Cl−: 105 mEq/L HCO −: 36 mEq/L Plasma renin activity is also decreased. Which of the following is most likely to be increased?
Aldosterone
Anion gap
Carcinoembryonic antigen
Prostate-specific antigen
Troponin
A 28-year-old patient with known Addison’s dis- ease presents with abdominal pain and is hypotensive to a systolic pressure of 88 mm Hg. He has a 2-week history of progressively worse nonproductive dry cough, sore throat, malaise, and headache. He has not checked his temperature at home but complains of constant chills. Which of the following is the best initial management?
Intravenous fluids
Azithromycin
Check serum glucose
Hydrocortisone
X-ray of the chest
A generally healthy 74-year-old woman who recently moved into the area visits the physician’s office for her first well-visit. She states that her previous doctor had been treating her with propylthiouracil (PTU) for subclinical hyperthyroidism, but that her prescription ran out several months ago. Laboratory studies reveal that her free thyroxine and triiodothyronine levels are normal, but her thyroid-stimulating hormone is depressed. PTU therapy is most important in this patient to prevent the development of which disorder?
Cardiac dysrhythmias
Hypothyroidism
Pretibial myxedema
Thyroid cancer
Thyroid storm
A 58-year-old woman presents to her physician because of neck discomfort and difficulty swallowing. She first began to have difficulty with swallowing solids 2 years ago, but the problem is getting progressively worse. She denies hemoptysis, hematemesis, abdominal pain, or change in bowel habits. She is a nonsmoker and past medical history is significant only for mild hypertension. Her temperature is 36.9°C (98.4°F), heart rate is 72/min, and blood pressure is 132/78 mm Hg. She has an asymmetrically enlarged thyroid gland that is particularly firm on the right, with poorly palpable borders. Laboratory evaluation reveals a free thyroxine level of 4.1 ng/dL and thyroid- stimulating hormone of 5μU/mL. Based on the results of a radioisotope scan and a fine needle aspiration biopsy, the physician decides to perform surgery. For which of the following is the patient at increased risk postoperatively?
Hypocalcemia
Bone metastases
Hypercalcemia
Hypophosphatemia
Pheochromocytoma
A 19-year-old man with insulin-dependent diabetes mellitus is taking 30 units of NPH insulin each morning and 15 units at night. Because of persistent morning glycosuria with some ketonuria, the evening dose is increased to 20 units. This worsens the morning glycosuria, and now moderate ketones are noted in urine. The patient complains of sweats and headaches at night. Which of the following is the most appropriate next step in management?
Obtain blood sugar levels between 2:00 and 5:00 AM
Measure blood glucose levels at bedtime.
Increase the evening dose of NPH insulin further.
Add regular insulin to NPH at a ratio of 2/3 NPH to 1/3 regular.
Add lispro via a calculated scale to each meal; continue NPH.
A 52-year-old man presents to the primary care clinic for the first time. He states that he has been in good health throughout his life and takes no medications. He was once athletic but has noted a dramatic decrease in his muscle strength and exercise tolerance over the past year. On examination the patient is moderately hypertensive, with a tanned, round, plethoric face; large supraclavicular fat pads; and significant truncal obesity. He has no focal cardiovascular, pulmonary, or neurologic findings. His fasting blood sugar is 200 mg/dL. Which of the following is the most common etiology of this condition?
ACTH-secreting pituitary adenoma
Adrenal tumor
Ectopic ACTH-secreting tumor
Primary adrenal hyperplasia
Small cell lung cancer
A 48-year-old high school teacher with no prior medical history presents to his primary care physician after feeling extremely fatigued for >1 month. Previously an avid runner, he has recently experienced dyspnea on moderate exertion. Although he denies vomiting, he admits to intermittent episodes of diarrhea. His blood pressure is 73/37 mm Hg and he is afebrile. On physical examination his skin is warm and erythematous, and his jugular venous pressure is elevated. Cardiac examination reveals a systolic murmur near the right border of the sternum that is accentuated with inspiration. Which of the following is most consistent with these findings?
Elevated urinary excretion of 5-hydroxyin-doleacetic acid
Elevated urinary excretion of vanillylman-delic acid
Peaked T waves on ECG
Pseudomonas species grown from blood cultures
Severe pulmonary congestion on x-ray of the chest
A 3-year-old girl is brought to the pediatrician’s office because of an abdominal mass. Physical examination reveals short stature, coarse facial features, a protruding tongue, and an easily reducible umbilical hernia. The girl has difficulty walking and knows six words, although she is unable to form a sentence. Her mother reports no health problems and an uncomplicated pregnancy. What is the most likely cause of the patient’s condition?
Congenital hypothyroidism
Cushing’s syndrome
Neuroblastoma
Phenylketonuria
Turner’s syndrome
A 3010-g (6.6-lb) boy was born to a 37-year-old primagravida by spontaneous vaginal delivery after an uncomplicated pregnancy. On examination he has cyanotic extremities and a significant right precordial heave, a single S2, and a harsh systolic ejection murmur along the sternal border. He also has a prominent squared nose and cleft palate. An echocardiogram is subsequently performed and demonstrates tetralogy of Fallot. Corrective surgery is performed without complications. At 2 months of age the infant is diagnosed with Pneumocystis jiroveci pneumonia, and at 3 months he is diagnosed with fungal septicemia. Additional work-up of this child should include which of the following tests?
Serum calcium
Hemoglobin electrophoresis
Nitroblue tetrazolium
Quantitative immunoglobulin levels
Renal ultrasound
You recently evaluated a 28-year-old woman who presented with complaints of shakiness and heat intolerance. The patient plans to have children and is currently using no contraception. On examination you noted tachycardia with an HR of 102, a fine tremor, a diffuse goiter, and proptosis. You now have the laboratory results and note a TSH < 0.001, elevated total T4 of 17.8, and increased T3 uptake. Radionuclide uptake by the thyroid gland is elevated. You tell her that she has Graves’ disease. What is the best treatment plan for this patient?
Propylthiouracil
Radioactive iodine
Propranolol
Oral corticosteroids
Thyroid surgery
A 56-year-old woman presents to the outpatient clinic for a routine visit. On physical examination a 1-cm nodule is palpated in her thyroid. Her physical examination is otherwise unremarkable. Her heart rate is 70/min and regular, blood pressure is 126/82 mm Hg, and temperature is 36.7°C (98.0°F). Which of the following is a poor prognostic indicator for the thyroid nodule?
Hoarseness
Female gender
Palpitations
Patient age of 56 years
Slow growth of nodule
A 52-year-old African-American woman with type 2 diabetes mellitus (DM) presents to her physician’s office and states that she has been feeling lousy in the morning. She notes that she reliably checks her blood glucose levels, and is frustrated at the fact that she often has a blood sugar level in the 120s at night, followed by a level in the 170s to 180s the following morning. The patient’s primary care physician increased her nightly dose of neutral protamine Hagedorn insulin 1 month ago, but her morning glucose levels have only become more elevated. She has recently begun to limit her carbohydrate intake at night, with no effect. This patient’s morning hyperglycemia might most likely be alleviated by which of the following?
Decreasing neutral protamine Hagedorn insulin at night
Increasing regular insulin at night
Increasing neutral protamine Hagedorn insulin at night
Increasing regular insulin in the morning
Increasing neutral protamine Hagedorn insulin in the morning
A 26-year-old G1P0 woman at 12 weeks’ gestation presents to her obstetrician for her first visit. Her pregnancy thus far has been notable only for some mild nausea and vomiting that lasted throughout her first trimester. She reports feeling overly tired lately and very weak. Her past medical history is significant for pernicious anemia. On physical examination she is an anxious-appearing, thin woman. Her blood pressure is 130/85 mm Hg, heart rate is 115/ min, and respiratory rate is 18/min. Fetal heart tones are present at 135/min. The uterine fundus is at 12 cm. The woman has a diffuse, non- tender goiter, a resting tremor, and poor global muscle strength. Which is the most likely mechanism underlying this woman’s condition?
Autoantibodies against thyroid-stimulating hormone receptor
Iodine overdose
The mechanism of this disease is unknown
Uncontrolled cell growth
Viral infection
A 50-year-old female is evaluated for hypertension. Her blood pressure is 130/98. She complains of polyuria and mild muscle weakness. She is on no blood pressure medication. On physical examination, the PMI is displaced to the sixth intercostal space. There is no sign of congestive heart failure and no edema. Laboratory values are as follows: Na+: 147 mEq/dL K +: 2.3 mEq/dL Cl−: 112 mEq/dL HCO3: 27 mEq/dL The patient denies the use of diuretics or over-the-counter agents to decrease fluid retention or promote weight loss. She does not eat licorice. Which of the following tests is most useful in establishing a diagnosis?
Ratio of serum aldosterone to plasma renin activity
24-hour urine for cortisol
Renal angiogram
Urinary metanephrine
Plasma renin activity
A 36-year-old female complains of inability to lose weight despite low calorie diet and daily exercise. She has also noticed that she is cold intolerant. She is wearing a jacket even though it is summer. She also reports constipation and hair loss. These symptoms have been worsening over the past 2 to 3 months. An elevated TSH and low total and free T4 confirm your suspicion of hypothyroidism. You suspect the etiology of this patient’s hypothyroidism to be autoimmune thyroiditis. What is the best test to confirm the diagnosis of autoimmune thyroiditis?
Thyroid peroxidase antibody (TPOAb)
Antinuclear antibody
24-hour radioactive iodine uptake
Thyroid aspiration
Thyroid ultrasound
A 60-year-old woman recently diagnosed with type 2 DM complains of daily headaches and double vision that have gradually worsened over the previous month. An MRI shows a large pituitary adenoma. Which of the following is most likely being secreted by this tumor?
Growth hormone
ACTH
Luteinizing hormone
Prolactin
Thyroid-stimulating hormone
A 61-year-old obese man with a history of chronic alcohol abuse is diagnosed with type 2 DM. In addition to diet modification and exercise, his physician recommends he begin therapy with a hyperglycemic agent. Several days after starting therapy, his wife comes home from work and finds him sitting on the couch staring into space and breathing rapidly. When she speaks to him, she finds he is quite confused, and immediately takes him to the emergency department. Arterial blood gas analysis shows: pH: 7.2 HCO −: 19 mEq/L Partial carbon dioxide pressure: 32 mm Hg Partial oxygen pressure: 80 mm Hg Lactate: 6 mmol/L Which of the following drugs is most likely responsible for this patient’s symptoms?
Metformin
Acarbose
Glipizide
Insulin
Rosiglitazone
A moderately overweight 34-year-old woman presents to the emergency department with excessive sweating, flushing, tachycardia, and nervousness. Presuming that she might be suffering from thyrotoxicosis, the physician checks her blood levels of thyroid hormones, and finds that her free thyroxine and triiodothyronine levels are elevated, while her thyroid-stimulating hormone is decreased. Her radioactive iodine uptake test shows a complete absence of iodine uptake. Which of the following is the most likely diagnosis?
Factitious thyrotoxicosis
Graves’ disease
Thyroid-stimulating hormone-secreting pituitary tumor
Toxic adenoma
Toxic multinodular goiter
A 72-year-old man with end stage renal disease secondary to hypertension presents with several months of back pain. He denies fever, weight loss, difficulty walking, altered sensation in his legs, or incontinence. He was diagnosed with renal disease 20 years ago and was managed medically for many years. However, 2 years ago he began hemodialysis because of a progressive decline in renal function. There is no family history of renal disease or malignancy. Physical examination is unremarkable. X-ray of the chest shows ill-defined bands of increased bone density adjacent to the vertebral endplates. What laboratory abnormalities is most likely in this patient?
Elevated parathyroid hormone
Bence-Jones protein in urine
Decreased parathyroid hormone
Decreased phosphate
Elevated bone-specific alkaline phosphatase
{"name":"USMLE: Endocrinology", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"A 40-year-old female presents with altered mental status and confusion. Last year, she was diagnosed with rheumatoid arthritis, for which she is currently using indomethacin and methotrexate. Her temperature is 37.0C (98.6F), pulse is 75\/min, blood pressure is 110\/70, and respirations are 15\/min. She is disoriented and irritable. Mucus membranes are moist. There is no jugular venous distention. Lungs are clear to auscultation. Abdomen is soft, nontender and not distended. There is no peripheral edema. Serum chemistry reveals: Sodium 122 mEq\/L Potassium 3.7 mEq\/L Bicarbonate 22 mEq\/L Blood glucose 90 mg\/dL BUN 9.0 mg\/dL Uric acid 3.0 mg\/dL Serum osmolality is 265mOsm\/kg, while urine osmolality is 500 mOsm\/kg. What is the most likely cause of this patient's hyponatremia?, A 50-year-old male comes to the office due to an ulcer in his right foot. He has type 2 diabetes, for which he takes glyburide. Laboratory investigations reveal an HbA1c of 9%, and random blood sugar of 180 mg\/dl. X-ray of the leg\/foot is normal. A picture of the foot ulcer is shown below. Which of the following is the most appropriate management of this patient's foot ulcer?, A 50-year-old male presents for the evaluation of polyuria and polydipsia of two months duration. He also complains of weakness and fatigue. He had one episode of paralysis that resolved on its own. He has a 20 pack-year history of smoking. He does not drink alcohol. His past medical and family histories are not significant His pulse is 78\/min, blood pressure is 150\/96 mmHg and temperature is 37C (98.6 F). The rest of his examination, including the neurological examination, is unremarkable. Laboratory studies show: Plasma sodium 145 mEq\/L Potassium 24 mEq\/L Serum creatinine 0.8 mg\/dl Plasma renin activity low Plasma aldosterone concentration high Which of the following is the most likely diagnosis?","img":"https://cdn.poll-maker.com/10-464509/untitled.jpg?sz=1200"}