
Dx P3 C q 200 to 243 * 43 qcm fb

Nephrology Challenge Quiz
Test your knowledge in nephrology with our comprehensive quiz featuring 35 detailed questions. This quiz covers various renal pathologies, diagnostic approaches, and management strategies essential for students, healthcare professionals, and enthusiasts alike.
Engage in learning through:
- Multiple-choice questions
- In-depth explanations
- Interactive and Educational experience
201) A 27-year-old man comes to the physician because of a 2-day history of periorbital swelling. He was treated with oral dicloxacillin for a skin infection 3-weeks ago. His urine has turned darker. His temperature is 37.4°C (99.4°F), blood pressure is 150/90 mm Hg, pulse is 80/min, and respirations are 15/min. Examination shows periorbital swelling. Urinalysis shows 8 RBCs/HPF with RBC casts and a mild proteinuria. Laboratory studies show low serum C3 levels; BUN is 40 mg/dl and serum creatinine is 2 mg/dl. Which of the following is the most likely diagnosis?
. Drug-induced acute interstitial nephritis
. Acute pyelonephritis
. Post streptococcal glomerulonephritis
. Membranoproliferative glomerulonephritis
. IgA nephropathy
202) A 27-year-old man comes into the emergency department because of a 2-week history of hemoptysis, breathing difficulty, ankle edema, and dark urine. His past medical history is insignificant. He is not taking any medication. He does not use tobacco, alcohol, or drugs. Laboratory studies show: Hb 10.5 g/dl, Serum Na 135 mEq/L, Serum K 4.8 mEq/L, BUN 36 mg/dl, Serum creatinine 2.8 mg/dl. Urinalysis shows numerous dysmorphic red blood cells/HPF, moderate proteinuria, and red cell casts. Chest x-ray reveals bilateral alveolar infiltrates. Diagnosis of which of the following pulmonary-renal syndromes require emergency plasmapheresis?
. Good pasture's syndrome
. Wegener's granulomatosis
. SLE-associated nephritis
. Polyarteritis nodosa
. Idiopathic rapidly progressive glomerulonephritis (RPGN)
203) A 64-year-old man is scheduled for hemodialysis due to end stage renal disease. He has a several year history of hypertension, diabetes, coronary artery disease, hypercholesterolemia, peripheral vascular disease, gout, and diverticulosis. Six months ago, he was admitted for urosepsis. Recently, his haemoglobin has ranged between 8.5 to 9.5 g/dl. He has already been on iron therapy, and now you are considering erythropoietin injections twice weekly. Which of the following is most likely to be seen following erythropoietin therapy?
. Worsening of his hypertension
. Increase in insulin requirement
. Increased susceptibility to infections
. Deterioration in renal function
. Flare-up of gout
204) A 70-year-old man is brought to the hospital by his son because of worsening fatigue. His son states that his father does not like seeing doctors and has not seen a physician in the past 20 years. He has no medical problems. Physical examination of the prostate shows no abnormalities. Laboratory studies show: Hb 10.5 g/dl, WBC 7,400/cmm, Platelets 160,000/cmm, Serum Na 135 mEq/L, Serum K 5.0 mEq/L, BUN 50 mg/dl, Serum creatinine 3.0 mg/dl. Ultrasonogram of the abdomen shows bilateral small kidneys and no evidence of hydronephrosis. Kidney biopsy shows intimal thickening and luminal narrowing of renal arterioles with evidence of sclerosis. Which of the following is the most likely cause of this patient's findings?
. Hypertension
. Diabetes mellitus
. Multiple myeloma
. Analgesic abuse
. Renal lithiasis
205) A 35-year-old woman who recently emigrated from Russia comes to the physician because of hematuria. She has a history of frequent headaches. Extensive evaluation did not reveal the cause of her headaches. They occur almost every day, and she tried various analgesics to relieve them. Her family history is significant for hypertension and diabetes mellitus. She does not use tobacco, alcohol, or drugs. Her blood pressure is 120/70 mm Hg and heart rate is 80/min. Physical examination shows no abnormalities. Urinalysis shows numerous unchanged red blood cells/hpf. Which of the following is the most likely cause of this patient's condition?
. Malignancy
. Glomerular injury
. Papillary necrosis
. Infection
. Nephrolithiasis
206) A 55-year-old woman comes to the physician for an annual physical examination. She has no new complaints, except fatigue. She has an 8-year history of chronic low back pain; severe degenerative joint disease has been documented on MRI. She had an anterior wall myocardial infarction four years ago. Her current medications include naproxen, acetaminophen, oxycodone, aspirin, atenolol, and simvastatin. Her blood pressure is 130/80 mm Hg and pulse is 72/min. Laboratory studies show: Hb 10 g/dl, WBC 6,000/cmm, Blood sugar 82 mg/dl, BUN 36 mg/dl, Serum creatinine 2.0 mg/dl. Urinalysis : Protein 2+, Glucose Absent, RBC AbsentWBC 10-15/HPF, Nitrite Negative, Esterase Negative, Sediment WBC casts. Serum protein electrophoresis is negative for monoclonal gammopathy. Two years ago, her BUN level was 22 mg/dl, and creatinine level was 1.6 mg/dl. Which of the following is the most likely pathology involved in this patient's renal failure?
. Acute tubular necrosis
. Chronic glomerulonephritis
. Tubulointerstitial nephritis
. Recurrent pyelonephritis
. Renal tuberculosis
207) A 50-year-old man comes to the physician for a routine follow-up visit. He has hypertension, diabetes mellitus, secondary hyperparathyroidism, and end-stage renal disease. He has been on hemodialysis for the past three years. He was admitted three months ago for line sepsis, which was treated with antibiotics. He had a right below-the-knee amputation two years ago following a non-healing foot ulcer. Physical examination shows a right carotid bruit. If this patient dies within the next five years, what would be the most likely cause of his death?
. Cardiovascular disease
. Stroke
. Infection
. Cancer
. Withdrawal from dialysis
208) A 15-year-old boy comes to the physician because of hematuria and lower abdominal pain. This is his third episode of hematuria in the past 2 years. He has a family history of renal disease. His temperature is 37.1°C (98.9°F), blood pressure is 140/90 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows mild sensorineural deafness bilaterally. Urinalysis shows hematuria and proteinuria. Laboratory studies show BUN of 50 mg/dl and serum creatinine of 3.1 mg/dL; serum complement levels are normal. Renal biopsy shows foam cells, and immunofluorescence shows no immunoglobulins or complement. Electron microscopy shows alternating areas of thinned and thickened capillary loops with splitting of GBM. Which of the following is the most likely diagnosis?
. Alport's syndrome
. Acute interstitial nephritis
. Acute post infectious glomerulonephritis
. Anti-glomerular basement membrane disease
. Benign recurrent hematuria
209) A 17-year-old African American man comes to the physician after an episode of gross hematuria that resolved spontaneously. He has no other complaints. His past medical history is insignificant. He takes no medications. He smokes occasionally. He does not use drugs or alcohol. His temperature is 36.7°C (98°F), blood pressure is 120/70 mm Hg, pulse is 70/min, and respirations are 14/min. Physical examination shows no abnormalities. Urinalysis shows many unchanged red blood cells/HPF, but is otherwise normal. Laboratory studies show a creatinine level of 0.9 mg/dl. Which of the following is the most likely diagnosis?
. Coagulopathy
. Acute cystitis
. Acute glomerulonephritis
. Acute interstitial nephritis
. Sickle cell trait
210) A 30-year-old woman comes to the physician due to several weeks history of generalized edema, fatigue, and decreased appetite. She has no other medical problems. She takes no medications. She does not use tobacco, alcohol, or drugs. Her temperature is 36.7°C (98°F), blood pressure is 110/70 mm Hg, pulse is 80/min, and respirations are 18/min. Physical examination shows generalized edema. Laboratory studies show a low serum albumin level. HBsAg is positive, and liver fun
. Membranoproliferative glomerulonephritis
. Minimal change disease
. Focal segmental glomerulosclerosis
. Diffuse proliferative glomerulonephritis
. Membranous glomerulonephritis
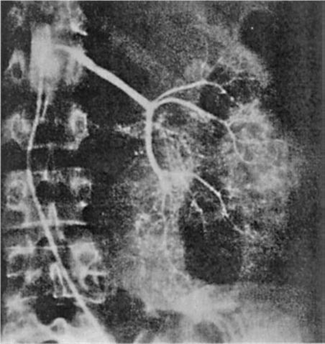
211) A 64-year-old man is admitted for hematuria after slipping on an icy pavement. His physical examination is normal. A selective angiogram of the left kidney is shown in Fig. Which of the following is the most likely diagnosis?
Image

Renal cell carcinoma
Kidney contusion and laceration
Transitional cell carcinoma
Renal hamartoma
Renal hemangioma
212) A 64-year-old man presents with weight gain, shortness of breath, easy bruising, and leg swelling. On examination, his blood pressure is 140/80 mm Hg, pulse 100/min, JVP 4 cm, heart sounds normal, and lungs are clear. There is a 3+ pedal and some periorbital edema. Investigations include a normal chest x-ray (CXR), electrocardiogram (ECG) with low voltages, anemia, high urea and creatinine, and 4 g/day of protein in the urine. A renal biopsy, which shows nodular deposits that have an apple-green birefringence under polarized light when stained with Congo red. Which of the following is the most likely diagnosis?
Amyloidosis
Multiple myeloma
Diabetic nephropathy
Minimal change disease
Immunoglobulin A (IgA) nephropathy
213) A 25-year-old man is referred to you because of hematuria. He noticed brief reddening of the urine with a recent respiratory infection. The gross hematuria resolved, but his physician found microscopic hematuria on two subsequent first-voided morning urine specimens. The patient is otherwise healthy; he does not smoke. His blood pressure is 114/72 mm Hg and the physical examination is normal. The urinalysis shows 2+ protein and 10 to 15 RBC/hpf, with some dysmorphic erythrocytes. No WBC or casts are seen. What is the most likely cause of his hematuria?
. Kidney stone
. Renal cell carcinoma
. Acute poststreptococcal glomerulonephritis
. Chronic prostatitis
. IgA nephropathy (Berger disease)
214) A 17-year-old man is brought to the emergency room with confusion and incoordination. He is uncooperative and refuses to provide further history. Physical examination reveals an RR of 30; the vital signs are otherwise normal as is the general physical examination. Laboratory values are as follows: Na: 135 mEq/L, K: 2.7 mEq/L, HCO3: 15 mEq/L, Cl: 110 mEq/L. Arterial blood gases: PO2 92, PCO2 30, pH 7.28 Urine: pH 7.5, glucose—negative, Ca: 9.7 mg/dL, PO4: 4.0 mg/dL. Which of the following is the most likely cause of the acid base disorder?
. GI loss owing to diarrhea
. Proximal renal tubular acidosis
. Disorder of the renin-angiotensin system
. Distal renal tubular acidosis
. Respiratory acidosis
215) A 28-year-old woman presents with a recent episode of coughing up some blood, frequent nosebleeds, and now decreased urine output. A nasal mucosa ulcer was seen on inspection. Her urinalysis is positive for protein and red cells consistent with a GN. The CXR shows two cavitary lesions and her serology is positive for antineutrophil cytoplasmic antibodies (ANCA). Which of the following is the most likely diagnosis?
Wegener’s granulomatosis
Bacterial endocarditis
Goodpasture’s syndrome
Lupus erythematosus
Poststreptococcal disease
216) A 74-year-old woman develops acute sepsis from pneumonia and is admitted to the intensive care unit because of hypotension. She is started on antibiotics, and her blood pressure is supported with intravenous normal saline. Despite this she remains oliguric and develops ARF. Her urinalysis has heme-granular casts and the urine sodium is 56 mEq/L. Which of the following is the most likely cause of her ARF?
Nephrotoxic antibiotics
Acute infectious GN
Acute tubular necrosis (ATN)
Contrast nephropathy
Cholesterol emboli
217) A 76-year-old man presents to the emergency room. He had influenza and now presents with diffuse muscle pain and weakness. His past medical history is remarkable for osteoarthritis for which he takes ibuprofen, and hypercholesterolemia for which he takes lovastatin. Physical examination reveals blood pressure of 130/90 mm Hg with no orthostatic change. The only other finding is diffuse muscle tenderness. Laboratory data include: BUN: 30 mg/dL, Creatinine: 6 mg/dL, K: 6.0 mEq/L, Uric acid: 18 mg/dL Ca: 6.5 mg/dL, PO4: 7.5 mg/dL, UA: large blood, 2+ protein. Microscopic study shows muddy brown casts and 0 to 2 rbc/hpf (red blood cells/high power field).Which of the following is the most likely diagnosis?
. Nonsteroidal anti-inflammatory drug-induced acute kidney injury (AKI)
. Volume depletion
. Rhabdomyolysis-induced acute kidney injury
. Urinary tract obstruction
. Hypertensive nephrosclerosis
218) A 73-year-old man undergoes abdominal aortic aneurysm repair. The patient develops hypotension to 80/50 mm Hg for approximately 20 minutes during the procedure according to the anesthesia record. He received 4 units of packed red blood cells. Postoperatively, his blood pressure is 110/70 mm Hg, heart rate is 110, surgical wound is clean, and a Foley catheter is in place. Over the next 2 days his urine output slowly decreases. His creatinine on post-op day 3 is 3.5 mg/dL (baseline 1.2). His sodium is 140 mEq/L, K 4.6 mEq/L, and BUN 50 mg/dL. Hemoglobin and hematocrit are stable. Urinalysis shows occasional granular casts but otherwise is normal. Urine sodium is 50 mEq/L, urine osmolality is 290 mosmol/L, and urine creatinine is 35 mg/dL. The FENa (fractional excretion of sodium) based on these data is 3.5. What is the most likely cause of this patient’s acute renal failure?
. Acute glomerulonephritis
. Acute tubular necrosis
. Prerenal azotemia
. Contrast induced nephropathy
. Acute interstitial nephritis
219) A 73-year-old woman with arthritis presents with confusion. Neurologic examination is nonfocal, and CT of the head is normal. Laboratory data include: Na: 140 mEq/L, K: 3.0 mEq/L, Cl: 107 mEq/L, HCO3: 12 mEq/L. Arterial blood gases: PO2 62, PCO2 24, pH 7.40. What is the acid-base disturbance?
. Respiratory alkalosis with appropriate metabolic compensation
. High anion-gap metabolic acidosis with appropriate respiratory compensation
. Combined metabolic acidosis and respiratory alkalosis
. No acid-base disorder
. Hyperchloremic (normal anion gap) metabolic acidosis with appropriate respiratory compensation
220) A 63-year-old man alcoholic with a 50-pack-year history of smoking presents to the emergency room with fatigue and confusion. Physical examination reveals a blood pressure of 110/70 mm Hg with no orthostatic change. Heart, lung, and abdominal examinations are normal and there is no pedal edema. Laboratory data are as follows: Na: 110 mEq/L, K: 3.7 mEq/L, Cl: 82 mEq/L, HCO3: 20 mEq/L, Glucose : 100 mg/dL, BUN : 5 mg/dL, Creatinine: 0.7 mg/dL Urinalysis: normal Specific gravity: 1.016. Which of the following is the most likely diagnosis?
. Volume depletion
. Inappropriate secretion of antidiuretic hormone
. Psychogenic polydipsia
. Cirrhosis
. Congestive heart failure
221) A 65-year-old white female comes to the ER because of persistent vomiting and epigastric pain. She has been suffering from left knee osteoarthritis for the past 6 years, and has been taking ibuprofen for the past year. She also has a history of chronic obstructive pulmonary disease but is well controlled on her current medications. She quit smoking a few years ago. Her laboratory results are given below: ABG: pH 7.55, PCO2 46 mm Hg. Chemistry panel: Serum sodium 132 mEq/L, Serum potassium 3.0 mEq/L, Chloride 88 mEq/L, Bicarbonate 38 mEq/L, Serum creatinine 0.8 mg/dl. Which of the following would describe her primary acid-base status?
. Normal profile
. Metabolic acidosis
. Metabolic alkalosis
. Respiratory acidosis
. Respiratory alkalosis
222) A 36-year-old male is brought to the emergency department due to confusion, nausea and decreased arousal. He is unable to answer questions and no other history is available. His temperature is 36.7ׄ°C (98.2°F), respirations are 22/min and pulse is 86/min. His ABG and serum electrolyte levels are shown below: pH 7.21, PaO2 96 mmHg, PaCO2 28 mmHg, Serum sodium 140 mEq/L, Serum potassium 3.6 mEq/L, Chloride 90 mEq/L, Bicarbonate 12 mEq/L, Blood urea nitrogen (BUN) 30 mg/dl, Serum creatinine 1.2 mg/dl. What is the most likely primary acid-base disorder in this patient?
. Non-anion gap metabolic acidosis
. Anion gap metabolic acidosis
. Metabolic alkalosis
. Respiratory alkalosis
. Respiratory acidosis
223) A 56-year-old male comes to the emergency room because of a 2-day history of fever, chills, shortness of breath and productive cough. He also threw up once in the emergency room. He has been smoking for several years and occasionally drinks alcohol. On admission, his BP was 90/60, but with one liter of normal saline it improved to 120/80 mm Hg. His temperature is 38.8°C (102°F). His arterial blood gas (ABG) analysis is as follows: Blood pH 7.53, PaO2 70 mmHg, PaCO2 30 mmHg, HCO3- 22 mEq/L. Which of the following best describes his primary acid-base status?
. Respiratory acidosis
. Respiratory alkalosis
. Metabolic acidosis
. Metabolic alkalosis
. Normal acid base status
224) A 67-year-old male is brought to the ER because of increasing abdominal pain and nausea for the past few hours. He has multiple medical problems including type-2 diabetes, hypertension, hyperlipidemia, coronary artery disease, cerebrovascular accident, peripheral vascular disease, ischemic cardiomyopathy and atrial fibrillation. He has not been on anticoagulation because of recurrent bleeding peptic ulcer disease. He has had a cholecystectomy. He takes multiple medications at prescribed doses and lives at home with his family. He quit smoking 10 years ago and does not use alcohol or drugs. His temperature is 37.8°C (100.0°F), blood pressure is 150/90 mm Hg, pulse is 110/min and respirations are 22/min. Physical examination shows an elderly male in acute distress. Lungs have few crackles at the bases. Heart rate is irregular. Bowel sounds are decreased and diffuse tenderness is present. There is no peripheral edema. Initial laboratory studies show the following: Serum sodium 140 mEq/L, Chloride 103 mEq/L, Bicarbonate 14 mEq/L, Blood urea nitrogen (BUN) 20 mg/dl, Serum creatinine 0.8 mg/dl, Blood glucose 198 mg/dl, Amylase 255 U/L. Which of the following is the most likely diagnosis in this patient?
. Diabetic ketoacidosis
. Bowel ischemia
. Acute pancreatitis
. Acute appendicitis
. Peptic ulcer perforation
225) A 56-year-old male with a history of type-2 diabetes presents for a routine office visit. His blood work from two months ago showed hyperkalemia, and at that time his physician discontinued lisinopril. His repeat blood work done today is shown below: Chemistry panel: Serum sodium 136 mEq/L, Serum potassium 5.6 mEq/L, Chloride 110 mEq/L,Bicarbonate 18 mEq/L, Blood urea nitrogen (BUN) 26 mg/dl, Serum creatinine 1.9 mg/dl. He currently takes glipizide, furosemide, nifedipine and aspirin. His blood pressure is 150/90 mmHg. Examination is unremarkable. Which of the following is the most likely cause of his low bicarbonate and elevated potassium?
. Chronic renal failure
. Renal tubular acidosis
. Furosemide
. Glipizide
. Nifedipine
226) A 33-year-old woman is brought to the emergency room because of altered mental status. En route to the ER, she suffers a generalized tonic clonic seizure, and once at the hospital she is confused and no further history can be obtained. You know only that she has a history of schizophrenia. On physical examination, her temperature is 36.7°C (98°F), blood pressure is 130/76 mm Hg, pulse is 80/min, and respirations are 14/min. Examination shows normal pupils. Her chest is clear to auscultation and her heart sounds are normal. Her abdomen is soft and nontender. Extremities have no edema. Laboratory studies show: Serum sodium 118 mEq/L, Serum creatinine 0.8 mg/dL, Serum calcium 8.4 mg/dL, Serum glucose 98 mg/dL, Urine osmolality 100 mosm/kg, Urine specific gravity 1.002. Which of the following is the most likely cause of her symptoms?
. Primary polydipsia
. Drug-induced ADH resistance
. Increased ADH production
. Drug-induced water retention
. Deficient ADH secretion'
227) A 56-year-old male comes to the emergency room because of increasing shortness of breath for the last 3 days. He had a cold recently, and since then his symptoms have been worse. He has a mild productive cough but denies fever or chills. He has a several year history of smoking and has been diagnosed with emphysema. He also has a history of diabetes, hypertension, hyperlipidemia, and hypothyroidism. He takes glipizide, metformin, lisinopril, furosemide, aspirin, atorvastatin and levothyroxine. Physical examination shows trace bilateral lower extremity edema and a diffuse decrease in breath sounds along with wheezing. Heart sounds are distant. His arterial blood gas shows the following: Blood pH 7.23, PaO2 88mm Hg, PaCO2 40 mm Hg, HCO3- 16mEq/L. Which of the following best describes the acid-base status of this patient?
. Metabolic acidosis
. Respiratory acidosis
. Mixed metabolic and respiratory acidosis
. Mixed metabolic acidosis and respiratory alkalosis
. Normal acid-base balance
228) A 45-year-old male is brought to the emergency department in a stuporous state. He appears agitated and disoriented. His temperature is 37.2°C (99°F), respirations are 22/min, pulse is 90/min and blood pressure is 110/70 mm of Hg. His lab findings are as follows: Blood pH 7.21, PaO2 100 mmHg, PaCO2 30 mmHg, HCO3- 13 mEq/L, Serum osmolarity 350 mOsm/L, Blood glucose 90 mg/dl, Na+ 141 mEq/L, K+ 4.6 mEq/L, Cl- 100 mEq/L, BUN 28mg/dl, Creatinine 2.5 mg/dl. His urine shows the presence of rectangular, envelope-shaped crystals. His creatinine three months ago was 1.2 mg/dl. What is the most likely cause of this lab abnormality in this patient?
. Aspirin ingestion
. Ethylene glycol poisoning
. Methyl alcohol poisoning
. Uremic acidosis
. Lactic acidosis
229) A 21-year-old female comes to the office for the evaluation of fatigue and weakness. She first noticed these symptoms nine months ago. She says, "I can't exercise a lot anymore because I get fatigued very easily, but after resting for a while, I feel better, and my fatigue disappears." She then describes a recent episode of weakness while swimming in a pool, where she experienced double vision (especially when she did not look straight ahead), difficulty raising her eyelids, and swallowing problems. What is the most likely diagnosis?
. Amyotrophic lateral sclerosis
. Myasthenia gravis
. Brain tumor
. Multiple sclerosis
. Duchenne muscular dystrophy
230) A 27-year-old woman presents to the ER with severe vomiting and abdominal pain that started several hours ago. She describes her emesis as "yellowish." She has a history of alcohol and cocaine use. Her temperature is 36.7°C (98°F), pulse is 98/min, respirations are 16/min, and blood pressure is 140/86 mmHg. Physical examination reveals dryness of the oral mucosa. Her abdomen is soft, non-distended, and without hepatosplenomegaly. Mild epigastric tenderness is present on deep palpation. Bowel sounds are increased. No rebound or rigidity is noted. She is treated with intravenous normal saline and metoclopramide. Several hours later she complains of neck pain and her neck muscles are noted to be stiff and tender. Which of the following best explains this patient's current complaints?
. Meningeal irritation
. Fat necrosis
. Medication side effect
. Eosinophilic myositis
. Nerve root compression
231) A 55-year-old Caucasian male comes to the office because of numerous falls for the past few weeks. Yesterday, he felt so dizzy that he fell on the ground and hurt his knees. He has also noticed dry mouth, dry skin, and erectile dysfunction over this period. His past medical history is significant for the recent onset of resting tremors. He was diagnosed with diabetes six months ago, which is controlled with diet. His blood pressure is 120/80 mmHg supine, and 90/60 mmHg standing. Physical examination reveals rigidity and bradykinesia. What is the most likely diagnosis of this patient?
. Idiopathic orthostatic hypotension
. Horner's syndrome
. Familial dysautonomia (Riley-Day syndrome)
. Diabetic neuropathy
. Shy-Dragger syndrome
232) A 65-year-old, obese, white female comes to the office for the evaluation of her progressively worsening memory. She considers herself "very independent," and lives alone; however, the development of her new symptoms is causing her some distress, as she often forgets to pay her bills. A detailed review of systems reveals no other symptoms, except for mild urinary incontinence. She has hypertension controlled with a beta-blocker and type 2 diabetes mellitus controlled with diet. She does not use tobacco, alcohol or drugs. Her blood pressure is 130/90 mmHg, pulse is 72/min, temperature is 36.7°C (98°F) and respirations are 14/min. Lungs are clear to auscultation and percussion. A grade 2/6, systolic ejection murmur is heard. Abdominal examination shows no tenderness or masses. Neurological examination shows broad-based, shuffling gait and a right-sided carotid bruit. Complete blood count and serum chemistry panel are within normal limits MRI shows enlarged ventricles. What is the most likely diagnosis?
. Parkinsonism
. Normal pressure hydrocephalus
. Multi-infarct dementia
. Pick's disease
. Alzheimer's disease
233) A 12-year-old boy is brought to the clinic for a routine health maintenance exam. He has no complaints, but mentions some spots on his back, which he noticed during his physical education class. He does not know how long they have been there. He denies any allergies. He remembers having a few seizures some years ago, which have not recurred since. He does not take any medication. The physical examination reveals several white spots and nodules measuring 2x3 cm on his back. There are freckles on his face and axilla. Closer examination reveals some nodules on his iris. What is the concerning complication that this boy is prone to?
. Hemoptysis
. Pancreatitis
. Tumors
. GI bleed
. Early dementia
234) A 25-year-old woman comes to the office and complains of intermittent dizziness and an unsteady gait for the last few days. Her symptoms worsen with exercise. Her past medical history is significant for tingling and numbness of her right foot that lasted 3-4 days (1 year ago), and visual loss in her right eye which spontaneously resolved (3 years ago). She is currently nursing her 2-month-old baby. Her obstetrical history was uncomplicated. Her neurological examination shows right hyperactive deep tendon reflexes. On attempted left gaze, her left eye abducts and exhibits horizontal jerk nystagmus, but her right eye remains stationary. When she attempts to look to the right, her right eye abducts and exhibits horizontal jerk nystagmus, but her left eye remains stationary. The patient is able to converge both eyes together, without any associated nystagmus. The facial muscles show no signs of weakness. Where is the most likely site of this patient's lesion?
. Optic nerve
. Optic tract
. Optic chiasma
. Optic radiations
. Medial longitudinal fasciculus
235) A 60-year-old male complains of recent onset gait imbalance and visual illusion of to-and-fro environmental motion. The symptoms are constant. He has no associated nausea or vomiting. His past medical history includes diabetes, hypertension, and chronic renal failure, and recent enterococcal endocarditis for which he is taking ampicillin and gentamicin. On physical examination, his temperature is 36.7°C (98°F), blood pressure is 120/76 mm Hg, pulse is 80/min, and respirations are 16/min. Neurologic examination shows 5/5 power and 2+ reflexes in all four extremities. Cranial nerve examination is normal. There is no nystagmus. Which of the following is the most likely cause of his current condition?
. Drug toxicity
. Vertebrobasilar insufficiency
. Hypoglycemia
. Meniere's disease
. Cerebellar infarction
{"name":"Dx P3 C q 200 to 243 * 43 qcm fb", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"Test your knowledge in nephrology with our comprehensive quiz featuring 35 detailed questions. This quiz covers various renal pathologies, diagnostic approaches, and management strategies essential for students, healthcare professionals, and enthusiasts alike.Engage in learning through:Multiple-choice questionsIn-depth explanationsInteractive and Educational experience","img":"https:/images/course1.png"}
More Quizzes
Part 47 (141)
141700
(NEW)part8(1957-2000)......(1785-2039)6breetpit
108540
Fundamentals of Digital Marketing
1580
Titanic Quiz
1059
Advanced Gas Dynamics
15821867
Free Personal Event Trivia
201024371
Ultimate Thomas Edison IQ Test: Prove Your Genius
201080207
Test Your Knowledge: Ecosystem Competition & Survival
201086956
Free Media Studies YouTube Vlogging
201026930
Free End Semester Test: Integrated Physics & Chemistry
201027196
What Tattoo Should I Get? Free to Find Your Perfect Ink
201027749
Can You Ace the American Vision Textbook?
201029922