
DES PAGE 303-360
Medical Knowledge Assessment
Welcome to the Medical Knowledge Assessment quiz, designed to test your understanding of various medical topics ranging from cardiology to gastroenterology. This quiz features 190 questions that challenge your clinical reasoning and diagnostic skills.
- Comprehensive coverage of medical topics
- Multiple choice format for ease of answering
- Ideal for medical students, professionals, and enthusiasts
1) Un traitement par he̝parine standard à dose anticoagulante est de̝bute̝ au Service d'Accueil et d'Urgence chez une patiente de 35 ans pour embolie pulmonaire. Sur quels e̝le̝ments biologiques doit porter la surveillance de ce traitement?
. Taux de prothrombine (TP)
. Temps de ce̝phaline active̝e (TCA)
. Dosage de BNP
. Taux de fibrinogène
. Dosage de l'antithrombine III
2) Un homme de 65 ans, porteur d'un re̝tre̝cissement aortique serre̝, avec angor d'effort depuis 5 ans et angor spontane̝ depuis quelques mois, vient de faire une syncope à l'effort. ECG : rythme sinusal PR à 20/100ème de seconde - QRS à 8/100ème de seconde. Quel examen faut-il faire avant la chirurgie?
. ECG d'effort
. Exploration e̝lectrophysiologique endocavitaire
. Coronarographie
. ECG selon la me̝thode de Holter
.Cathe̝te̝risme droit
3) Une femme de 37 ans sans facteurs de risque cardiovasculaire se plaint de douleurs thoraciques atypiques d'effort et de repos e̝voluant depuis plusieurs anne̝es. Quel examen allez-vous demander en priorite̝?
.e̝chocardiogramme trans-oesophagienne (ETO)
. enregistrement Holter de 24 heures
. e̝preuve d'effort
. coronarographie
. Dosage de D dimère
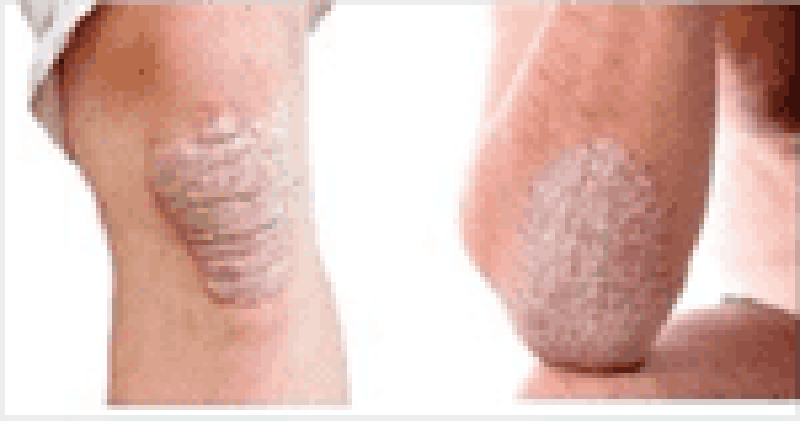
4) Mme X, 38 ans, se pre̝sente en consultation pour des le̝sions cutane̝es atteignant les coudes et les genoux. Elle a dans ses ante̝ce̝dents de̝pressif majeur traite̝ par Sertraline, ulcère gastrique traite̝ par Ome̝prazole 20mg/j et un surpoids. Elle prend re̝gulièrement de l'Ate̝nolol à vise̝e anxiolytique. Elle est rousse avec des yeux bleus et ne bronze presque pas lorsqu'elle s'expose au soleil. Elle ne fume pas et consomme de l'alcool occasionnellement. TA 145/95 mm Hg au repos. Vous faites le diagnostic de psoriasis en plaque. Elle n'a jamais eu aucun traitement auparavant ni d'explorations comple̝mentaires. Quel examen comple̝mentaire prescrivez-vous?
Aucun
Biopsie cutane̝e
Immunofluorescence directe
Se̝rologie VIH
Pre̝lèvement mycologique
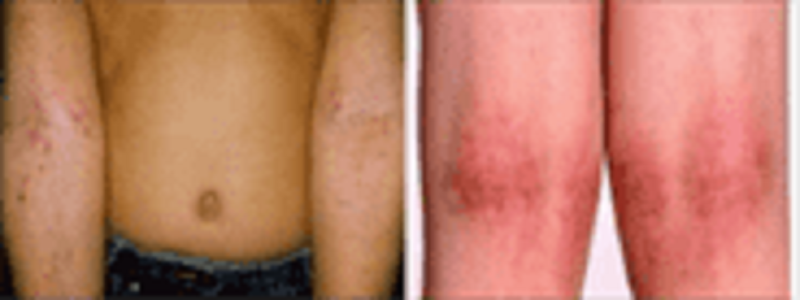
5) Vous voyez en consultation une petite fille de 6 mois pour un prurit e̝voluant depuis une semaine environ. Elle est ne̝e à terme. Ses vaccinations sont à jour. Elle a un frère en bonne sante̝. Elle a eu une bronchiolite l'anne̝e dernière, sans gravite̝. Son père est asthmatique depuis l'adolescence. Quel examen comple̝mentaire prescrivez-vous pour confirme le diagnostic?
Aucun
Biopsie cutane̝e
Prick-test
Patch-test
He̝mogramme
6) M. K, 52 ans se pre̝sente pour une le̝sion prurigineuse de la main gauche; e̝voluant depuis 1 semaine. Ce patient exerce la profession de boucher. Il est marie̝ et a 3 enfants. Il ne prend aucun traitement. Il a 2 chats à la maison. Quel examen comple̝mentaire prescrivez-vous pour confirmer le diagnostic?
Pre̝lèvement mycologique
Pre̝lèvement bacte̝rien
Biopsie cutane̝e
Culture cutane̝e
Lumière de WOOD
7) Mrs. Y, 25 year-old, comes to OPD for prenatal consultation. She has gestational diabetes in the first pregnancy 3 years ago. What should you recommend when it comes to GDM screening?
Wait until 24-28 weeks of pregnancy
Do the OGTT
Request A1C
Check only fasting blood glucose
Check random blood sugar
8) Mr. T, 25 year-old is admitted to the inpatient department. We suspect he has type one diabetes. All the findings below are in favors for type one diabetes except one.
Ketone (-)
Ac-anti GAD65 (+)
Ac-anti IA2 (+)
Glycemia 290mg/dl and C-peptide low
Ac-anti GAD65 and IA2 (+)
9) Mr B. 65 ans, est adresse̝ aux urgences par son me̝decin traitant. Il a aimablement joint une lettre: “Cher confère, merci de prendre en charge Mr B., qui pre̝sente une hypercalce̝mie à 3,05 mmol/L, chez qui je suspecte une hyperparathyroïdie primitive. Vous re̝alisez un ECG, que recherchez-vous?
Allongement du QT
Elargissement du QRS
Raccourcissement du QT
Bradycardie
Apparition d’une onde U
10) Mr B. 65 ans, est adresse̝ aux urgences par son me̝decin traitant. Il a aimablement joint une lettre: “Cher confère, merci de prendre en charge Mr B., qui pre̝sente une hypercalce̝mie à 3,05 mmol/L, chez qui je suspecte une hyperparathyroïdie primitive. Quelle est le profil biologique retrouve̝ dans une hyperparathyroïdie primitive?
Hypercalce̝mie, hyperphosphore̝mie, PTH basse
Hypercalce̝mie, hypophosphore̝mie, PTH basse
Hypocalce̝mie, hyperphosphore̝mie, PTH basse
Hypercalce̝mie, hyperphosphore̝mie, PTH e̝leve̝e
Hypercalce̝mie, hypophosphore̝mie, PTH e̝leve̝e
11) A patient of 55 years old comes to see you for symptoms of dyspepsia. Anamnesis and clinical examination revealed that he lost 5 kg for the past 2 months and his father died of gastric cancer so you have to diagnose whether the patient was infected by H. Pylori. Which of the following tests would you think is the most appropriate?
Gastroscopy + histology
Gastroscopy + rapid urease breathe test
H. Pylori stool test
H. Pylori serology
H. Pylori in saliva
12) A patient of 45 years old comes to see you for symptom of irritable bowel syndrome about 2 months. He has rectal bleeding one to two times weekly. Which investigation is the most likely diagnostic?
Anuscopy
Colonoscopy
Gastroscopy
Abdominal scanner
Abdominal ultrasound
13) Madame XG âge̝ de 44 ans divorce̝ 10ans, elle boit beaucoup de la bière depuis la se̝paration avec son marie. Le diagnostic de la pancre̝atite chronique est porte̝ il y a 6mois. Re̝cemment, elle a des vomissements post prandiaux avec sensation d’un gène e̝pigastrique. L'e̝chographie ne montre pas des anomalies particulières sous re̝serve de gaz abondance. Mais vous avez encore le doute sur le pseudo- kyste du pancre̝as. Vous êtres à l’hôpital Calmette, quel examen paraclinique le plus adapte demandez- vous dans ce cas?
Echo-endoscopie
Scanner abdominal
IRM pancre̝atique
CPRE
Gastroscopie
14) Monsieur CR âge̝ de 45ans est admis au service de Me̝dicine A4 de l'hôpital Calmette pour un doute d'une tumeur du pancre̝as. Votre confrère vous a contacte̝ et vous a pose̝ la question: quel examen comple̝mentaire le plus performance dans le cadre de diagnostic d'un ade̝nocarcinome du pancre̝as ?
Marqueuse tumorale Ca19.9
Scanner abdomino-pelvien
Echo-endoscopie pancre̝atique
Pet-scan au FDG
IRM abdomino-pelvien
15) A sixty-six-year old man presents to the emergency department with a history of one episode of melena. Past history includes coronary artery disease, hypertension. He is on one baby aspirin daily. An urgent upper endoscopy is negative. What is the most appropriate next step?
. UGI series with small bowel follow-through
. Colonoscopy
. Angiography
. Red blood cell tagged technetium scan
. Abdominal CT scan with contrast
16) A fifty-eight year old female patient presents to the emergency department with a 24-hour history of several hematemesis. She is found to be hypotensive and anemic. Resuscitative measures are instituted. What is the most appropriate next step?
. Urgent gastroscopy
. Anoscopic examination
. Colonoscopic examination
. Scintigraphy
. Angiography
17) A 28-year-old woman with a history of an appendectomy presents with a non-tender palpable mass in the right lower quadrant abdominal incision. The following statement(s) is/are true concerning the diagnosis and management of this patient.
. The best diagnostic test involves imaging of the abdominal wall by either CT or MRI
. Resection of the mass with a 2 cm margin is usually adequate
. Low dose radiation is a suitable alternative to surgery for primary treatment
. Re-resection for recurrence will likely have a higher rate of recurrence than for primary resection
. Therapeutic endoscopic should be an option for the treatment of the mass.
18) A 50-year-old patient develops sudden left lower chest pain and epigastric pain after vomiting. The patient shows diaphoresis, breath sounds are decreased on the left, and there is abdominal guarding. The most appropriate diagnostic test is:
. Aortography.
. Esophagoscopy.
. Electrocardiogram.
. Film of the chest.
. White blood count.
19) Un homme de 67 ans vous voyez en consultation pour une rectorrhagie. Il se plaint d’avoir des e̝pisodes de rectorrhagie depuis environs 6 mois. Il n’y pas de douleur ou de trouble du transit. A l’interrogatoire vous notez des e̝pisodes de rectorrhagie minime parfois e̝mission de caillots de sang par l’anus. Cliniquement, le ventre est souple, pas de masse palpable. Les conjonctives sont pâles. Le pouls est de 96/mn. Quel l’examen demandez-vous pour confirmer le diagnostic?
Examen proctologique
Recto-sigmoïdoscopie
Echographie abdominale
Scanner abdomino-pelvienne
Coloscopie totale
20) Une coloscopie chez un patient de 55 ans retrouve une tumeur moyenne rectum biopsie̝e, l’anatomo-pathologie retrouve un ade̝nocarcinome lieberkühnien. Quel est votre bilan d’extension ?
TDM thoraco-abdomino-pelvienne
PET TDM
Radiographie pulmonaire
IRM abdomino-pelvienne
Echographie abdominale
21) Une femme de 45 ans consulte pour un ictère fe̝brile. La Tempe̝rature est à 39°C. La TA est à 100/60 mmHg, le pouls est à 110/mm. L’examen biologique montre : GB 20 Giga/L, CRP 200 mg/l, ASAT 60 UI/L, ALAT 120 UI/L, PAL 300 UI/L, GGT 122 UI/L, Bili T 100mg/L, Bili D 45mg/L. Quel examen de première intention demandez-vous pour confirmer le diagnostic ?
. ASP
. E̝chographie abdominale
. Scanner abdominal
. IRM
. CPRE
22) Un homme de 40 ans, se pre̝sence aux urgences pour douleurs abdominales survenues brutalement il y a quelques heures. Il s’agit de douleurs e̝pigastriques intenses (EVA à 7) avec irradiation poste̝rieure associe̝es à 2 e̝pisodes de vomissements alimentaires. Elles sont soulage̝es par la position en chien de fusil. Il est alcoolisme chronique. Pas d’autres ante̝ce̝dents notables. Quel est le bilan biologique le plus approprie̝ pour confirmer le diagnostic de pancre̝atite aiguë ?
Lipase̝mie > 3N
Amylase̝mie > 3N
Lipase̝mie > 2N
Amylase̝mie > 2N
Triglyce̝ride̝mie > 15g/dl
23) Un homme de 38 ans, alcoolisme chronique active, se pre̝sence aux urgences pour douleurs abdominales survenues brutalement il y a quelques heures. Il s’agit de douleurs e̝pigastriques intenses (EVA à 8) avec irradiation poste̝rieure associe̝es à 2 e̝pisodes de vomissements alimentaires. Elles sont soulage̝es par la position en chien de fusil. Il est alcoolisme chronique. Pas d’autres ante̝ce̝dents notables. Le diagnostic de pancre̝atite aiguë est confirme̝. Quel est le bilan biologique le plus simple pour e̝valuer la gravite̝ de ce patient ?
CRP > 150
CRP > 50
Lipase̝mie > 7 N
Lipase̝mie > 10 N
He̝matocrite < 40 %
24) Vous prenez en charge un malade en ACC à l’hôpital. Il e̝tait en de̝tresse respiratoire depuis plusieurs heures auparavant. Avant de poser un scope, quelle est votre hypothèse pour son trace̝ ECG ?
Asystolie
Dissociation Electro-Me̝canique
Fibrillation Ventriculaire
Tachycardie Ventriculaire
Torsade de Pointe
25) Vous voyez Madame N, 65 ans, en consultation externe pour une alte̝ration de l’e̝tat ge̝ne̝ral (asthe̝nie et amaigrissement de 4 kg en 3 mois). Elle a un ante̝ce̝dent de cancer du sein traite̝ par chirurgie et chimiothe̝rapie il y a 5 ans et d’oste̝oporose complique̝e d’une fracture du col du fe̝mur droit il y a 3 ans. Un bilan biologique a e̝te̝ re̝alise̝ qui montre : Na = 142 mmo/l ; K = 4,2 mmol/l ; Cre̝at = 90 μmol/l, Ca = 2,8 mmol/L (112 mg/L) Pour comple̝ter ce re̝sultat biologique, quel dosage vous semble le plus approprie̝ en 1° intention ?
Dosage de la phosphore̝mie
Dosage de l’albumine̝mie
Dosage de la TSH
Dosage de la vitamine D
Dosage de la PTH
26) Vous voyez Monsieur B, 47 ans en consultation externe pour notions d’œdème des paupières. Il a apporte̝ des re̝sultats re̝alise̝s en ville qui montrent : ure̝e = 0,65 g/L, cre̝atinine = 170 μmol/L, bandelette urinaire : prote̝ine +++, he̝maturie ++. Quel est l’examen comple̝mentaire en première intention pour orientation e̝tiologique ?
Prote̝inurie des 24 heures
Echographie cardiaque
Echographie re̝no-ve̝sico-prostatique
He̝moculture
Uroculture (ECBU)
27) Monsieur M, 75 ans, sans notion de bilan de sante̝ auparavant, apyre̝tique, vient vous voir à la consultation avec un bilan qui montre une e̝le̝vation de la cre̝atinine à 350μmol/L. Parmi les examens comple̝mentaires suivants à orientation e̝tiologique, lequel devez-vous re̝aliser en première intention ?
Echographie re̝no-ve̝sico-prostatique
Ionogramme sanguin et urinaire
Electrophorèse des prote̝ines urinaires
Electrophorèse des prote̝ines se̝riques
Uroculture (ECBU)
28) Mademoiselle D, 18 ans, sans ATCD connu, est amene̝e aux urgences pour e̝tat confus. L’examen clinique retrouve : PA = 115/85 mmHg, T= 38,9°C, fre̝quence cardiaque à 110/min et fre̝quence respiratoire à 25/min. Pas de signe de localisation en examen neurologique. L’auscultation cardio- respiratoire est sans particularite̝. Le gaz du sang montre : Na = 132 mmol/L, K = 5,5 mmol/L, chlore = 102 mmol/L, Bicarbonates = 8 mmol/L, pH arte̝riel = 7, pCO2 = 18 mmHg, pO2 = 110 mmol/L et Hb = 125 g/L. La bandelette urinaire montre : sang (-), prote̝ines traces, leucocytes +++, nitrites +, ce̝tones +++, glucose +++. Quel est l’ensemble des examens paracliniques en urgence pour expliquer le tableau clinico-biologique ci-dessus ?
Echographie re̝no-ve̝sicale, ECBU et he̝moculture
ECBU, he̝moculture et radio du thorax
He̝moculture, radio du thorax et scanner ce̝re̝bral
Radio du thorax, scanner ce̝re̝bral et e̝chographie re̝no-ve̝sicale
Scanner ce̝re̝bral, e̝chographie re̝no-ve̝sicale et ECBU
29) Monsieur M, 60 ans, est adresse̝ aux urgences pour alte̝ration de l’e̝tat ge̝ne̝ral. Il est hypertendu, suivi re̝gulièrement par son me̝decin traitant. Il pre̝sente depuis trois jours des diarrhe̝es liquides. A l’examen clinique, la pression arte̝rielle est à 90/60 mmHg, la fre̝quence cardiaque à 130/min. Le patient a perdu 3 kg depuis le de̝but des diarrhe̝es. L’auscultation cardiaque et pulmonaire est sans particularite̝. L’examen abdominal re̝vèle une sensibilite̝ diffuse, sans de̝fense ni contracture. Il pre̝sente de le̝gères marbrures, un pli cutane̝ persistant et re̝clame toutes les 15 minutes un verre d’eau. Il est apyre̝tique. Le bilan biologique montre : ure̝e = 1.65mg/L, cre̝atinine = 210μmol/L, Bicarbonate = 17 mmol/L, Na+ = 152mmol/L, K+ = 7.2 mmol/L, calce̝mie = 86 g/L, phosphore = 35 mg/L, albumine̝mie = 50g/L. La nume̝ration globulaire est sans particularite̝. Le bilan biologique re̝alise̝ il y a trois mois e̝tait sans particularite̝. Sa diurèse des 12 dernières heures est e̝value̝e à 200ml. Quel examen devez-vous re̝aliser en premier ?
ECG
Echographie re̝no-ve̝sicale
Scanner abdomino-pelvien sans injection
Scanner abdomino-pelvien avec injection
Ionogramme urinaire
30) Monsieur M, 60 ans, est adresse̝ aux urgences pour alte̝ration de l’e̝tat ge̝ne̝ral. Il est hypertendu, suivi re̝gulièrement par son me̝decin traitant. Il pre̝sente depuis trois jours des diarrhe̝es liquides. A l’examen clinique, la pression arte̝rielle est à 90/60 mmHg, la fre̝quence cardiaque à 130/min. Le patient a perdu 3 kg depuis le de̝but des diarrhe̝es. L’auscultation cardiaque et pulmonaire est sans particularite̝. L’examen abdominal re̝vèle une sensibilite̝ diffuse, sans de̝fense ni contracture. Il pre̝sente de le̝gères marbrures, un pli cutane̝ persistant et re̝clame toutes les 15 minutes un verre d’eau. Il est apyre̝tique. Le bilan biologique montre : ure̝e = 1.65mg/L, cre̝atinine = 210μmol/L, Bicarbonate = 17 mmol/L, Na+ = 152mmol/L, K+ = 7.2 mmol/L, calce̝mie = 86 g/L, phosphore = 35 mg/L, albumine̝mie = 50g/L. La nume̝ration globulaire est sans particularite̝. Le bilan biologique re̝alise̝ il y a trois mois e̝tait sans particularite̝. Sa diurèse des 12 dernières heures est e̝value̝e à 200ml. Quel examen à vise e̝tiologique devez-vous re̝aliser ?
ECG
Echographie re̝no-ve̝sicale
Scanner abdomino-pelvien sans injection
Scanner abdomino-pelvien avec injection
Ionogramme urinaire
31) Monsieur M, 60 ans, est adresse̝ aux urgences pour son me̝decin traitement pour hypercalce̝mie à 120mg/. Quel est le profil biologique retrouve̝ dans une hyperthyroïdie primitive ?
Hypercalce̝mie, hyperphosphore̝mie, PTH basse
Hypercalce̝mie, hypophosphore̝mie, PTH basse
Hypocalce̝mie, hyperphosphore̝mie, PTH basse
Hypercalce̝mie, hypophosphore̝mie, PTH e̝leve̝e
Hypercalce̝mie, hyperphosphore̝mie, PTH e̝leve̝e
32) Un sujet de 25 ans a e̝te̝ ope̝re̝ dans l’enfance d’un reflux ve̝sico-ure̝te̝ral bilate̝ral laissant des se̝quelles d’hypoplasie visible à l’e̝chographie re̝nale. Alors que la prote̝inurie n’e̝tait jamais supe̝rieure à 0,20g/l, elle atteint brusquement 2g puis 3g/24h. Cette prote̝inurie traduit :
Une aggravation des le̝sions inflammatoires de ne̝phrite interstitielle
La constitution d’une scle̝rose du tissu interstitiel
Une de̝ge̝ne̝rescence tubulaire
Une intole̝rence aux anti infectieux urinaires
Une atteinte glome̝rulaire de type hyalinose passive
33) Un garçon de 5 ans pre̝sente à 3 reprises des he̝maturies macroscopiques. Les examens ont montre̝ que 70% des he̝maties sont de morphologie de̝chiquete̝e à l’examen microscopique des urines. La prote̝inurie est de 1,5g/l. Il est pertinent de demander les examens au-dessous, sauf :
Une urographie avec lavage au Lasilix
Une cystographie
Une cre̝atinine̝mie
Une e̝lectrophorèse des protides plasmatiques
Un dosage de la fraction C3 du comple̝ment
34) Monsieur A, 55 ans pre̝sentant des faiblesses musculaires des quatre membres d’apparition brutale depuis 3 jours, de̝tresse respiration avec trouble de de̝glutition. Pas d’ante̝ce̝dents particuliers à noter. TA=130/90, pouls=88 bpm. Quel examen comple̝mentaire à demander?
IRM ce̝re̝brale
Scanner ce̝re̝brale
IRM cervicale
EEG
ENMG
35) Une patiente de 69 ans pre̝sentant un ptosis droit avec diplopie intermittente, faiblesses musculaire et trouble de de̝glutition. On suspecte la myasthe̝nie, qu’est-ce qu’on doit faire pour aider à confirmer le diagnostic?
Test de glaçon
Test à la prostigmine
Dosage anticorps antire̝cepteur à l’ACh
TDM thoracique
ENMG
36) Patient 66A, tabagisme actif 20PA, alcoolisme (1 bouteille de VR/j) sans d’autres comorbidite̝s particulières, hospitalise̝ pour une dysphagie haute d’apparition progressive et perte du poids (10kg en un mois). Il ne pre̝sente aucun ante̝ce̝dent. A l’examen clinique, nous ne trouvons que des ade̝nopathies jugulo-carotidiennes gauches supe̝rieures et moyennes, la plus grande mesure̝e 3cm. Quel examen d’imagerie le plus important pour faire le bilan loco-re̝gional et d’extension?
Echographie cervicale
IRM cervico-faciale et thoracique
Panendoscopie
Scanner cervico-facial et thoracique
Radiothoracique
37) Chez une femme de 35 ans pre̝sentant une tumeur du sein de 3 cm de diamètre, le seul examen permettant d’affirmer avec certitude le diagnostic de cancer est :
La mammographie
L’e̝chographie
La cytologie
L’examen clinique
Pre̝lèvement pour examen anatomo-pathologique
38) Un jeune garçon de 13ans, sans ante̝ce̝dent personnel et familial particulier, est adresse̝ à l’hôpital pe̝diatrique de Phnom Penh pour des douleurs osseuses diffuses et une fièvre persistante. Il est à 2 mois de son traitement de tuberculose ganglionnaire diagnostique̝ à Siem Reap devant une fièvre chronique et une ade̝nopathie me̝diastinale sur le scanner thoracique. L’examen clinique retrouve une pâleur cutane̝omuqueuse, purpuras pe̝te̝chiales au niveau du tronc et membres, des polyade̝nopathies cervicales millime̝triques, une he̝patome̝galie de 3cm sous rebord costale droit et une sple̝nome̝galie de 2cm sous rebord costale gauche. Les testicules sont normaux. L’examen neurologique est sans particularite̝. La TA est à 110/70mmHg, la fre̝quence cardiaque à 100/mn, la tempe̝rature est à 38.7C, le poids à 37kg, la taille à 140cm. Vous demandez un he̝mogramme qui montre une Hb à 79g/l, VGM 82fl, CCMH 33g/dl, Re̝ticulocyte 70G/l, Plaquette 30G/L, GB 113G/L dont 40 % de PNN, 55% de lymphocyte. Quelle interpre̝tation faites-vous de cet he̝mogramme?
Ane̝mie hypochrome microcytaire non re̝ge̝ne̝rative avec hyperleucocytose et thrombocytose
He̝mogramme normale
Ane̝mie normochrome normocytaire non re̝ge̝ne̝rative, thrombope̝nie,
Hyperleucocytose à pre̝dominant lymphocytaire
Ane̝mie macrocytaire d’origine pe̝riphe̝rique avec thrombope̝nie et hyperleurcocytose Ane̝mie normochome normocytaire avec neutrope̝nie et thrombope̝nie
39) Devant un patient pre̝sentant une plaie du cuir chevelu avec une fracture ouverte du fe̝mur gauche et à l’arrive̝e aux urgences une pâleur, agitation, PA = 60/40mmHg – pouls=130c/mn. Quel examen biologique faites-vous en premier ?
A . Gaz du sang
B. Lipase̝mie
C. Transaminases
D. He̝mogramme avec groupage
E. Troponine.
40) Aux urgences, en face de vous un patient dyspne̝ique, tachycarde avec chute tensionnelle qui tousse et frisonne depuis 7 jours. Quel examen paraclinique à demander en priorite̝ ?
A. Bronchoscopie
B. Cliche̝ thoracique
C. Echocardiographie
D. Electro cardiogramme (E.C.G)
E. Abdomen sans pre̝paration (ASP)
41) Devant une douleur abdominale diffuse avec contracture, arrêt des matières et de gaz. En plus l’examen re̝vèle une instabilite̝ he̝modynamique avec trouble de la conscience. Quel bilan paraclinique en 1ère intention?
A. Pression veineuse centrale (PVC)
B. Echographie abdominale
C. Scanner abdominal
D. Abdomen sans pre̝paration
E. Mesure du de̝bit cardiaque (Qc)
42) Une jeune fille de 25A est emmene̝e aux urgences par leurs parents pour trouble de la conscience, fièvre depuis 3 jours avec ce̝phale̝e et vomissements. Quel examen paraclinique en priorite̝?
A. Frottis sanguin
B. Ponction lombiare
C. Image̝rie
D. He̝moculture
E. Uroculture.
43) Vous avez suspecte̝ un lupus e̝rythe̝mateux syste̝mique chez une patiente de 29 ans venant de Preahvihea et demandez les examens comple̝mentaires pour confirmer le diagnostic. Vous prescrivez une radiographie pulmonaire de face. Quel signe radiologique important voulez-vous rechercher?
Dilatation des bronches
Cancer du poumon
Ate̝lectasie
Pneumothorax
Pleure̝sie
44) Vous avez suspecte̝ une goutte chez un patient de 50 ans et prescrivez les examens comple̝mentaires pour confirmer le diagnostic, de̝pister les complications et les autres maladies me̝taboliques associe̝es. Quel bilan biologique ci-dessous demandez-vous pour rechercher une des maladies me̝taboliques associe̝es?
Cre̝atinine̝mie
Cortisole̝mie
Glyce̝mie
Calce̝mie
Natre̝mie
45) Vous avez suspecte̝ une oste̝oporose chez une femme me̝nagère de 76 ans, me̝nopause̝e à l’âge de 49 ans, venant de Banteaymeanchey. Elle est hospitalise̝e dans le Service de Rhumatologie pour une lombalgie intense après un effort de toux. Elle a des ante̝ce̝dents de me̝nopause il y a 20 ans, de DNID et d’HTA traite̝e par Coveram 5/5, PA : 135/80mmHg, FC : 70/min,T : 36,2°C, e̝tat ge̝ne̝ral conserve̝. Vous demandez les examens comple̝mentaires. Quel est un objectif du bilan paraclinique en dehors de la densitome̝trie mine̝rale osseuse devant une suspicion d’oste̝oporose ?
Suivre l’e̝volution
Pre̝dire le pronostic
Elimine̝r une oste̝opathie fragilisante maligne
Faire le diagnostic
Rechercher les complications
46) Une femme ouvrière de 30 ans venant de Mondulkiri est hospitalise̝e dans un service de rhumatologie pour une lombosciatique gauche e̝volue̝e depuis 15 jours. Pour une lombosciatique commune non complique̝e, les examens comple̝mentaires (TDM, IRM) sont inutiles. Dans quelle circonstance que vous devez demander ces examens ?
Lombosciatique gauche impulsive à la toux
Lombosciatique irradiant dans le membre infe̝rieur gauche complète
Lombosciatique gauche d’origine tumorale
Lombosciatique bilate̝rale
Lombosciatique gauche associe̝e à la lombocruralgie gauche
47) Vous avez diagnostique̝ une scle̝rodermie syste̝mique chez une patiente de 59 ans venant de Kampong Thom et prescrivez un bilan biologique y compris les marqueurs inflammatoires. Concernant les marqueurs biologiques inflammatoires dans les propositions suivantes, laquelle est correcte?
CRP + Ionogramme
CRP + VS
CRP + Cre̝atinine̝mie
VS + Ionogramme
VS + Cre̝atinine̝mie
48) Une patiente obèse de 77 ans vient vous consulter pour une douleur me̝canique de l’aine gauche e̝volue̝e depuis 8 mois. Une coxarthrose gauche est suspecte̝e. Vous demandez les examens paracliniques pour confirmer votre hypothèse diagnostique. Les propositions suivantes pre̝sentent comment vous faites le diagnostic. Une proposition est juste, laquelle?
Clinique e̝vocatrice +image radiologique typique+diagnostique diffe̝rentiel
Clinique e̝vocatrice + liquide synovial + e̝chographie articulaire
Clinique e̝vocatrice + VS + liquide synovial
Clinique e̝vocatrice + CRP+liquide synovial
Clinique e̝vocatrice + VS + CRP
49) Vous avez suspecte̝ une coxarthrose droite chez un patient de 74 ans venant de Kampong Chhnang devant une douleur plutôt me̝canique de hanche gauche e̝volue̝e depuis 2 ans et vous prescrivez les examens comple̝mentaires y compris liquide synovial. Quel re̝sultat pre̝sente le caractère me̝canique du liquide synovial?
Leucocytes < 200/mm3
Leucocytes < 2000/mm3
Leucocytes > 2000/mm3
Leucocytes > 20000/mm3
Leucocytes > 200000/mm3
50) Vous avez suspecte̝ une spondylarthrite ankylosante chez une patiente de 24 ans venant de Takeo devant une fessalgie inflammatoire droite et arthrite de la cheville gauche et vous prescrivez les examens comple̝mentaires y compris HLA-B27. Quel est votre but de prescrire HLA-B27?
Pour confirmer le diagnostic
Pour aider le diagnostic
Pour e̝liminer le diagnostic
Pour pre̝dire le pronostic
Pour suivre l’e̝volution
51) Vous voyez en consultation à l’hôpital un homme de 52 ans, chauffeur de Tuk Tuk vivant seul dans la banlieue de Phnom Penh. Il pre̝sente depuis 2 jours une toux et une sensation fe̝brile, non ame̝liore̝s par l’achat d’un sachet de me̝dicaments à la pharmacie du quartier. Il va de plus en plus mal et n’a plus la force de travailler. A l’examen, vous notez : fre̝quence respiratoire à 31/min; fre̝quence cardiaque à 128/mn, pression arte̝rielle à 110/80 mm Hg et la tempe̝rature 37,7°C (sous sachets). Trouble de conscience; foyer de râles cre̝pitants des lobes infe̝rieurs droit et gauche. Quel critère clinique de gravite̝ vous manque-t’il pour calculer le score CURB-65 ?
L’âge du patient
L’existence d’un coma
La socio-e̝conomie
La baisse de TA
Le taux d’ure̝e plasmatique
52) Vous voyez en consultation à l’hôpital d’un patient âge̝ de 36 ans consulte aux urgences pour une toux fe̝brile suspecte de pneumonie aiguë communautaire (PAC). Parmi les propositions suivantes concernant les examens paracliniques d’imagerie. Quel examen paraclinique le plus approprie̝ dans ce cas?
Une radiographie thoracique de face re̝alise̝e en 1ère intention
Une radiographie thoracique de face et de profils re̝alise̝s en 1ère intention
Une e̝chographie pleuro-pulmonaire re̝alise̝e en 1ère intention
Une TDM thoracique avec IV de produits de contraste re̝alise̝e en 1ère intention Une TDM thoracique sans IV de produit de contraste re̝alise̝e en 1ère intention
53) Vous voyez en consultation une patiente de 43 ans, obèse, institutrice en e̝cole primaire à Take̝o. Depuis 4 jours, elle pre̝sente une rhinite, pharyngite, et une toux avec expectoration blanchâtre et mousseuse, associe̝e à une douleur re̝tro-sternale à l’inspiration. Elle a pre̝sente̝ une tempe̝rature pendant 2 jours, au maximum à 38,2°C, puis est devenue apyre̝tique sans traitement. Mais elle consulte car la toux s’est majore̝e. A l’examen, T 37,2°C ; PA 120/70 mmHg ; FC 80/min ; FR 16/min ; SpO2 99% en air ambiant. L’auscultation pulmonaire retrouve quelques râles bronchiques, pas de cre̝pitants. Vous e̝voquez une bronchite aigue en 1èrehypothèse diagnostique. Laquelle option du bilan paraclinique la plus choisie?
Pas de prescription d’examens paracliniques
Prescription d’une radiographie thoracique de face
Prescription d’un bilan biologique : CRP et NFP
Prescription d’un bilan microbiologique : he̝mocultures et ECBC
Prescription d’un bilan virologique : e̝couvillon naso-pharynge̝ H5N1
54) Vous recevez une femme âge̝e de 58 ans, pour dyspne̝e fe̝brile. Elle est dyspne̝ique et toux non productive et de douleurs thoraciques poste̝rieur droite apparues en même temps que la fièvre qui e̝tait d’emble̝e à 39,9°C depuis 24 heures. A l’examen : fre̝quence respiratoire à 32/min, la tension arte̝rielle à 90/50 mmHg, la fre̝quence cardiaque à 137 par min, la tempe̝rature à 39°C, SpO2à 87% en air ambiant. Quelle est la prise en charge la plus adapte̝e à vise̝e bacte̝riologique dans ce contexte ?
Ces examens ne doivent pas retarder l’antibiothe̝rapie
L’antibiothe̝rapie est de̝bute̝e avant tout examen
L’attente du re̝sultat du examen avant de̝buter une antibiothe̝rapie
Aucun examen bacte̝riologique n’est re̝alisable car la toux est sèche
Aucun examen bacte̝riologique n’est ne̝cessaire car hors de re̝animation
55) Vous recevez une femme âge̝e de 58 ans, pour dyspne̝e fe̝brile. Elle est dyspne̝ique et toux non productive et de douleurs thoraciques poste̝rieur droite apparues en même temps que la fièvre qui e̝tait d’emble̝e à 39,9°C depuis 24 heures. A l’examen : fre̝quence respiratoire à 32/min, la tension arte̝rielle à 120/75 mmHg, la fre̝quence cardiaque à 137 par min, la tempe̝rature à 39°C, SpO2à 87% en air ambiant. Votre externe vous demande si il y a un inte̝rêt à re̝aliser une antige̝nurie pneumocoque. Quel argument le plus probable de ce test?
L’examen interpre̝te̝ sans difficulte̝ compte tenu de l’ante̝ce̝dent de sinusite
L’examen n’a aucun inte̝rêt car les symptômes sont moins de 24h avant
L’examen doit être re̝alise̝ avant le de̝but de l’antibiothe̝rapie
L’examen peut être re̝alise̝ après le de̝but de l’antibiothe̝rapie
L’examen a une sensibilite̝ de 100%
56) Un adulte de 19 ans fumeur depuis l’enfant entre̝ pour douleur thoracique brutale. La douleur associe̝e à une dyspne̝e mode̝re̝e, toux sèche irritative. La conscience normal, la tension arte̝rielle 120/67 mmHg, la fre̝quence cardiaque 76 par min, la fre̝quence respiratoire 14/min. L’examen he̝mithorax normal, diminution du murmure ve̝siculaire, diminution de vibration vocale et sonorite̝ du sommet du poumon atteinte. Vous pensez à un diagnostic, mais le cliche̝ de radiographie du thorax ne se re̝vèle pas contributif. Quel examen comple̝mentaire le plus approprie̝ doit-on effectuer en cas de suspicion de ce diagnostic ?
Radiographie du thorax
Fibroscopie bronchique
Gaz du sang en air ambiant
Scanner thoracique
Echographie pulmonaire
57) Un adulte de 19 ans fumeur depuis l’enfant entre̝ pour douleur thoracique brutale. La douleur associe à une dyspne̝e mode̝re̝e, toux sèche irritative. La conscience normal, la tension arte̝rielle 120/67 mmHg, la fre̝quence cardiaque 115 par min, la fre̝quence respiratoire 17/min. L’examen he̝mithorax normal, diminution du murmure ve̝siculaire, diminution de vibration vocale et sonorite̝ du sommet du poumon atteinte. Vous pensez le diagnostic pneumothorax. Quel signe de gravite̝ radiologique le plus recherche̝ ?
Pneumothorax inferieur
Pneumothorax bilate̝ral
Pneumothorax post traumatique
Pneumothorax avec des brides
Pleure̝sie bilate̝rale associe̝e

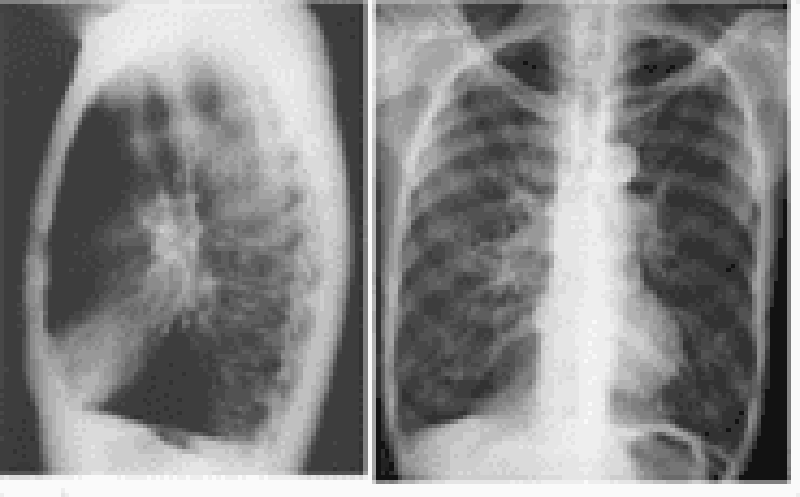
58) Vous recez en hospitalisation d’un homme âge̝ 42 ans a le me̝tier mineur depuis 5 ans. Il vous dit qu’il touche depuis 6 mois et la dyspne̝e au moins d’effort a remonte̝ à 2 semaines. La conscience normal, la tension arte̝rielle 120/67 mmHg, la fre̝quence cardiaque 28 par min, la fre̝quence respiratoire 14/min. Le cliche̝ de radiographie du thorax ci-joint.Quelle est l’interpre̝tation de ce cliche̝ ?
Micronodules diffus
Opacite̝ alve̝olaire
Pleure̝sie bilate̝rale
Emphysème pulmonaire
Cavite̝ hydro-ae̝rique
59) Vous recevez en hospitalisation Madame Kh âge̝ de 53 ans pour fièvre prolonge̝e. Elle a principal ante̝ce̝dent diabète sucre̝ de̝couverte re̝cent. L’examen : une conscience normal, la tension arte̝rielle 98/66 mmHg, la fre̝quence cardiaque 120 par min, la fre̝quence respiratoire 21/min. Quel examen paraclinique le plus souvent effectue̝ pour identifier le germe Burkholderia pseudomallei responsable de la maladie Me̝lioïdose au Cambodge?
He̝mocultures/selles
He̝mocultures/crachats
Selles/crachats
Urines/selles
Crachats/urines
60) Vous êtes appele̝ en re̝animation traumatologie au sujet de jeune homme âge̝ de 18 ans a e̝te̝ traumatisme crânien avec coma profonde. Ce patient a e̝te̝ be̝ne̝ficie̝ une intubation endotrache̝ale dès à l’admission. Au bout 7 jours de l’intubation, vous retrouvez les signes clinique et paraclinque. Vous pensez à une pneumonie nosocomiale tardive. Quel est l’examen bacte̝riologique le plus argumente̝ le diagnostic d’une pneumonie nosocomiale ?
Biopsie muqueuse par fibroscope recherche la bacte̝rie >107 UFC /ml
Aspiration bronchique par fibroscope seuil de bacte̝rie >105 UFC /ml
Lavage broncho alve̝olaire par fibroscope seuil de bacte̝rie >103 UFC /ml
Brosse bronchique prote̝ge̝ seuil par fibroscope de bacte̝rie >102 UFC /ml
Aspiration endotrache̝ale par sonde seuil de bacte̝rie >105 UFC /ml

61) Vous êtes appele̝ en re̝animation traumatologie au sujet de jeune homme âge̝ de 18 ans a e̝te̝ traumatisme crânien avec coma profonde. Ce patient a e̝te̝ be̝ne̝ficie̝ une intubation endotrache̝ale dès à l’admission. Au bout 7 jours de l’intubation, la fièvre 38,8°C apparue et la se̝cre̝tion endotrache̝ale devenue verdâtre. Le cliche̝ de radiographie thoracique ci-joint. Vous pensez à une pneumonie nosocomiale tardive. Quelle est la strate̝gie la plus adapte̝e pour diagnostic la pneumonie nosocomiale?
Biopsie pulmonaire
He̝mocultures
Aspiration endotrache̝ale
Recherche antigène urinaire
Crachat pour bacte̝riologie
62) Mr. MP 65 ans vous consulte pour une dyspne̝e d’effort apparue progressivement depuis 3 semaines. Il est de plus en plus gêne̝ dans les gestes de la vie quotidienne. Il a comme ante̝ce̝dent une insuffisance cardiaque sur une cardiopathie hypertensive traite̝e par beta bloquant non se̝lectif et Ramipril et il est traite̝ depuis 6 mois par Amiodarone pour une fibrillation auriculaire. Il est tabagique à 30 paquets - anne̝es non sevre̝. Cliniquement, la fre̝quence cardiaque est à 75 par min, la tension arte̝rielle à 130/80 mmHg. L’auscultation pulmonaire retrouve des cre̝pitants aux 2 champs pulmonaire. Il n’y a pas d’hippocratisme digital. La radiographie de thorax re̝alise̝e en ville retrouve un syndrome interstitiel bilate̝ral. Quelle est la le̝sions e̝le̝mentaire radiologique plus probable en pneumopathie interstitielle diffuse ?
Pleure̝sie bilate̝rale
Re̝ticulation intra lobulaire bilate̝rale
Opacite̝ alve̝olaire diffuse
Micronodule au sommet
Dilatation des broches localise̝e centrale
63) Vous recevez en hospitalisation Mr. P 48 ans pour une dyspne̝e et fe̝brile depuis 3 semaines. Il est tabagique à 30 paquets-anne̝es non sevre̝. Cliniquement, la fre̝quence cardiaque est à 95 par min, la tension arte̝rielle à 110/80 mmHg. L’auscultation pulmonaire ne retrouve pas de cre̝pitant. Il n’y a pas d’hippocratisme digital. La radiographie de thorax re̝alise̝e en ville retrouve un syndrome interstitiel bilate̝ral de type micronodule diffuse. Quelle est la pathologie à e̝voquer en priorite̝ devant des micronodules diffuse ?
Tuberculose
Sarcome
Mycose
Varicelle
Parasitose
64) Vous recevez en hospitalisation Madame P 32 ans pour une dyspne̝e et fe̝brile depuis 2 jours pre̝ce̝de̝ par syndrome grippal. Elle ne fume pas. Cliniquement, la fre̝quence cardiaque est à 95 par min, la tension arte̝rielle à 110/80 mmHg. L’auscultation pulmonaire retrouve des cre̝pitants bibasales. La radiographie de thorax re̝alise̝e retrouve un syndrome interstitiel bilate̝ral de type micronodule diffuse. Quel est l’inte̝rêt du lavage broncho alve̝olaire (LBA) devant une pneumopathie interstitielle diffuse aiguë ?
Pre̝sence de cause cardiaque retrouve̝e
Pneumopathie d’hypersensibilite̝
Pre̝sence des fibres amiantes
Sans inte̝rêt à diffe̝rentier
He̝morragie intra alve̝olaire
65) Mr. X 50 ans fermier, vous consulte pour une dyspne̝e apparue brutale au cours de me̝nager sa ancienne grange de riz. Il fume la cigarette 15 paquet-anne̝e non sevre̝. Pas de signe bronchite chronique. Pas de HTA ni notion prendre me̝dicaments. Cliniquement, la fre̝quence cardiaque est à 87 par min, la tension arte̝rielle à 130/80 mmHg, fre̝quence respiratoire 25 par min et SpO2 91% en air ambiant et la tempe̝rature 38°C. L’auscultation pulmonaire retrouve des cre̝pitants aux 2 champs pulmonaire. La radiographie de thorax re̝alise̝e en ville retrouve un syndrome interstitiel bilate̝ral. Vous pensez à une pneumopathie hypersensibilite̝ (poumon fermier). Quel examen paraclinique le plus conforte̝ à un diagnostic de pneumopathie d’hypersensibilite̝ ?
Dosage de nicotine urinaire
Dosage de procalcitonine plasmatique
Dosage d’Immunoglobuline E du crachat
Dosage des lymphocytes CD4 au LBA
Dosage des pre̝cipitines se̝rique
66) Patient de 53 ans a e̝te̝ ope̝re̝ il y a 3 jours une endocardite infectieuse valve aortique, dyspne̝e rapide progressive jour 2 post ope̝ratoire. Le gaz du sang sous FiO2 100%, pH: 7,26 PaCO2 75 mmHg, PaO2 45 mmHg, HCO3 18 mmol/l. Quelle est l’interpre̝tation ce gaz du sang ?
Alcalose respiratoire
Hypercapnie respiratoire
Acidose respiratoire
Acidose me̝tabolique
Effet shunt
67) Vous recevez un homme de 67 ans aux urgences pour dyspne̝e intense. Il a principal ante̝ce̝dent bronchite chronique post tabagique connu depuis 2 ans. La maladie a remonte̝ il y a 24 heures: dyspne̝e intense, orthopne̝e et spasme expiratoire. Vous e̝voquez à une de̝stresse de̝tresse respiratoire aiguë. Quel examen paraclinique le plus demande̝ devant une de̝tresse respiratoire aiguë sans opacite̝ radiologique du thorax?
Scintigraphie pulmonaire ventilation
Exploration fonctionnelle respiratoire
Echocardiographie doppler
Scanner thoracique injection
Gaz du sang arte̝riel en air ambiant
68) Vous recevez un patient 22 ans, homosexuel, aux urgences pour dyspne̝e intense progressive depuis 10 jours. Votre 1ère hypothèse diagnostique est la pneumopathie fe̝brile hypoxe̝miante donc la pneumocystose chez un patient VIH de̝couverte re̝cente. Quel est le critère clinique ou paraclinique est habituellement pre̝sent ?
Pre̝sence de prophylaxie par Bactrim
Taux de lymphocytes CD4 (+) >200/mm3
Râles cre̝pitants diffus
Opacite̝s interstitielles/alve̝olaires diffuses
Saturation en O2 supe̝rieur à 90%
69) Chez un patient Cambodgien VIH (+) avec moins de 100 CD4/mm3, la tuberculose se traduit le plus souvent par anomalie radiologique suivante, laquelle ?
Pleure̝sie purulence
Ade̝nopathie me̝diastinale
Caverne au sommet
Opacite̝ alve̝olo interstitielle
Infiltrat des 2 lobes supe̝rieurs
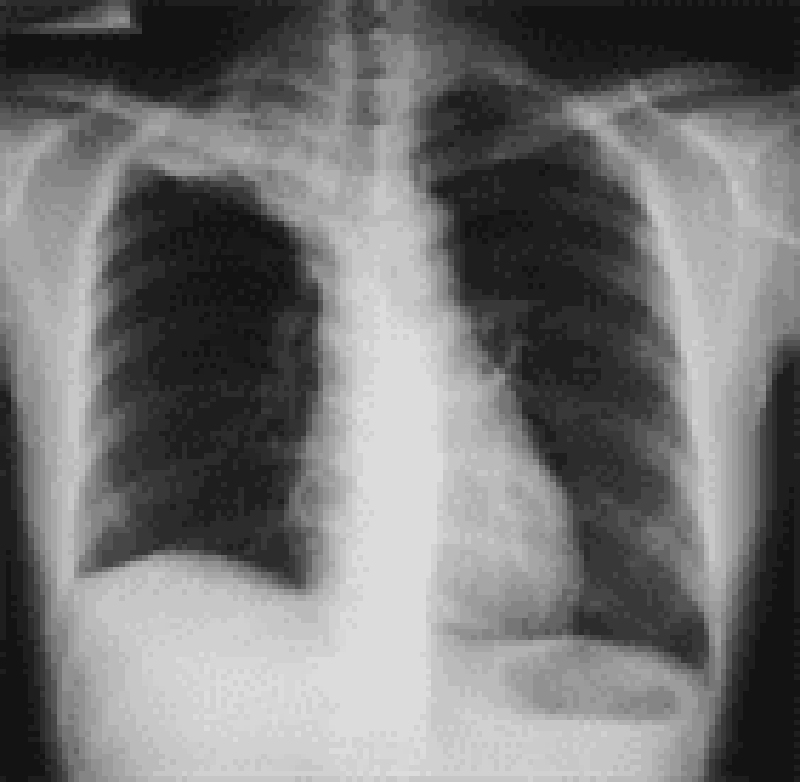
70) Vous recevez un patient âge̝ de 34 ans en hospitalisation au service Maladie Infectieuse pour dyspne̝e intense progressive depuis 12 jours. L’examen la fre̝quence respiratoire 34 par min, la saturation SaO2 78% en air ambiant, l’auscultation de râle cre̝pitant. La se̝rologie VIH est positive après d’accord du patient. La nume̝ration formule sanguine (NFS) : globule rouge : 2 630 000/mm3, Hb : 8,0 g/dl, globule blanc (GB) : 2 030/mm3, polynucle̝aire neutrophile (PNN) : 1 220/mm3, lymphocyte 530/mm3, plaquette : 150 000/mm3. Le cliche̝ de radiographie du thorax . Vous pensez qu’il a une infection opportuniste chez un sujet immunode̝prime̝ par le VIH. Quel est le diagnostic le plus probable?
Pneumonie bacte̝rienne
Miliaire tuberculeuse
Mycose pulmonaire
Pneumocystose pulmonaire
Anguillulose pulmonaire

71) Une patiente de 32 ans, vous consulte pour toux et alte̝ration de l’e̝tat ge̝ne̝ral depuis 2 mois. Elle a perdu du poids 5 Kg en 2 mois. Elle se plaint aussi d’asthe̝nie intense. Elle est marie̝e un enfant de 3 ans et ne prend aucun traitement d’une pilule œstroprogestative. Le cliche̝ de radio thoracique effectue̝e en ville . Quelle est l’anomalie sur la radiographie thoracique retrouvez-vous ?
Opacite̝ du lobe moyen
Opacite̝ excave̝e
Opacite̝ infiltrative
Opacite̝ grelot
Opacite̝ micronodule
72) Vous recevez en consultation une patiente de 60 ans pour une dyspne̝e expiratoire. Le patient suivi re̝gulier pour une bronchopneumopathie chronique obstructive (BPCO) post tabagique. La dyspne̝e d’apparition progressive associe̝e à une toux avec expectoration purulente depuis 5 jours qui ne cessent de se majorer. Vous e̝voquez donc à une exacerbation de bronchopneumopathie chronique obstructive (BPCO) post tabagique. Cliniquement, vous trouvez une le̝gère cyanose des extre̝mite̝s et des sueurs, la fre̝quence respiratoire : 26/min, la tension arte̝rielle 140/90 mmHg, la fre̝quence cardiaque : 90 par min. Quelle est l’e̝tiologie d’origine infectieuse le plus souvent responsable?
Influenza A
Legionella pneumonia
Mycobacterium tuberculosis
Hemophylus influenzae
Bordetella pertussis
73) Une patiente de 62 ans cuisinière, vit seule sans famille, vous suivez une bronchopneumopathie chronique obstructive (BPCO) biomasse stade 3 GOLD, consulte aux urgences pour une dyspne̝e d’apparition progressive. Vous e̝voquez donc une exacerbation bronchopneumopathie chronique obstructive (BPCO). Cliniquement, vous trouvez une le̝gère cyanose des extre̝mite̝s et des sueurs, la fre̝quence respiratoire : 26/min, la tension arte̝rielle 140/90 mmHg, la fre̝quence cardiaque : 90 par min. Quelle est l’anomalie sur le cliche̝ de radiographie thoracique trouve̝ le plus souvent ?
Aplatissement des coupoles diaphragmatique
Diminution diamètre ante̝ro-poste̝rieur
E̝largissement silhouette cardiaque
Inspiration insuffisance
Opacite̝ pe̝rihilaire
74) Vous recevez aux urgences Mr. S., 35 ans, pour une dyspne̝e expiratoire. A l’examen clinique, vous trouvez des sibilants diffus. Les constantes sont suivantes : la fre̝quence cardiaque : 120/min, la tension arte̝rielle : 120/80 mmHg, la fre̝quence respiratoire : 28/min, la saturation SpO22 : 95% en air ambiant. Le diagnostic un asthme retenu le plus vraisemblablement. Quel est l’examen comple̝mentaire indispensable à l’e̝tat stable pour le diagnostic confirmation d’asthme de ce patient ?
Radiographie thoracique
Gaz du sang
TDM thoracique
Explorations fonctionnelles respiratoires
Test allergologique
75) Vous recevez aux urgences Me. H. , 35 ans, pour une dyspne̝e aigue. Elle est très agite̝e et est incapable de terminer ses phrases. A l’examen clinique, vous trouvez des sibilants diffus, ainsi qu’une cyanose. Le diagnostic asthme aigu grave retenu le plus vraisemblablement. Le gaz du sang pH : 7,26 PaO2 : 65 mmHg, PaCO2 : 64 mmHg HCO3 29 mmol/l. Quelle anomalie les gaz du sang la plus approprie̝e ?
Acidose respiratoire
Acidose mixte
Partiellement compense̝
Hyperventilation alve̝olaire
Shunt vrai anatomique
76) Vous recevez en hospitalisation un chauffeur âge̝ de 27 ans pour sensation d’e̝touffement. Poids 109 Kg pour taille 1m62. La tension arte̝rielle: 143/98 mmHg, poules 98 par min, fre̝quence respiratoire : 21/min et SpO2 96% en e̝tat e̝veil et 84% en dorment avec ronflement. Il n’a pas ante̝ce̝dent particulier ni acrome̝galie ni hypothyroïdie. Il a deux accidents de voie publique par rapport à la somnolence. Vous pensez à syndrome d’apne̝e du sommeil. Quel examen permet de faire le diagnostic de syndrome d’apne̝e du sommeil ?
Electrocardiogramme (ECG)
Enregistrement polysomnographique (PSG)
Electromyogramme (EMG)
Electroence̝phalogramme (EEG)
Explorations fonctionnelles respiratoires (EFRs)
77) Vous recevez en hospitalisation un chauffeur âge̝ de 27 ans pour sensation d’e̝touffement. Poids 109 Kg pour taille 1m62. La tension arte̝rielle: 143/98 mmHg, poules 98 par min, la fre̝quence respiratoire : 21/min et la SpO2 96% en e̝tat e̝veil et 84% en dorment avec ronflement. Il n’a pas ante̝ce̝dent particulier ni acrome̝galie ni hypothyroïdie. Il a deux accidents de voie publique par rapport au somnolence. Vous pensez syndrome d’apne̝e du sommeil et la confirmation de polysomnographie. Quel paramètre supple̝mentaires analyse̝ sur un enregistrement polysomnographique ?
Onde S1Q1 pour bloc branche droit
Electromyogramme des muscles du biceps de̝tection hypotonie
Onde lente diffuse par rapport des crises e̝pileptique
Syndrome obstructif re̝versible sous β-mime̝tique
Signal des arrêts du flux nasal avec microre̝veil
78) Vous recevez en hospitalisation un chauffeur âge̝ de 27 ans pour sensation d’e̝touffement. Poids 109 Kg pour taille 1m62. La tension arte̝rielle: 143/98 mmHg, poules 98 par min, la fre̝quence respiratoire : 21/min et la SpO2 96% en e̝tat e̝veil et 84% en dorment avec ronflement. Il n’a pas ante̝ce̝dent particulier ni acrome̝galie ni hypothyroïdie. Il a deux accidents de voie publique par rapport à la somnolence. Vous pensez à syndrome d’apne̝e du sommeil et vous proposez le patient pour enregistrement la poly graphie ventilatoire et vous validez et interpre̝tez la polygraphie ventilatoire (PGV). Quelle est la chiffre de̝finie le syndrome d’apne̝e obstructive du sommeil se̝vère selon l’index d’apne̝es-hypopne̝es (IAH) ?
IAH 20/heure
IAH 30/heure
IAH 40/heure
IAH 50/heure
IAH 60/heure
79) Un patient de 23 ans en hospitalisation au service pneumologie pour fièvre et frisson depuis une semaine. Il est le gardien de la forêt Koh Kong. Depuis 72 heures, il a douleurs abdominales, selles diarrhe̝iques associe̝es à la lombalgie. L’apparition de dyspne̝e intense avec cyanose. La 1ère constance : tension arte̝rielle 94/45 mmHg poules 135 par min tempe̝rature axillaire 40°C. Votre hypothèse diagnostic la plus probable parasitose se̝vère avec localisation pulmonaire. Quel est le parasite peut-on pre̝lever le plus de chance à identifier dans le sang ?
Plasmodium falciparum
Paragonimus westermani
Pneumocystis jerovecii
Toxoplasma gondi
Leishmania donovani
80) Une patiente de 21 ans en consultation pour prurit anal et toux irritante une semaine. Votre hypothèse diagnostic la plus probable parasitose se̝vère avec localisation pulmonaire. Quel est le parasite peut infecter cette patiente sans augmenter l’e̝osinophilie dans la nume̝ration formule sanguine (NFS) ?
Amibes
Aspergillus
Ankylostomes
Ascaris
Anguillule
81) Vous recevez en consultation une femme noire de 20 ans pour amaigrissement et asthe̝nie. Elle est marie̝e sans enfant. Le poids est de 43 Kg pour taille 157cm, la tension arte̝rielle est 130/87 mmHg et poules 102 par fre̝quence respiratoire 25/min SpO2 97% en air ambiant. Le cliche̝ de radiographie thoracique re̝vèle des opacite̝s hilaires et interstitielles bilate̝rale. Vous pensez à une sarcoïdose. Quelle est l’anomalie biologique trouve̝e dans l’e̝lectrophorèse des prote̝ines sanguine plus probable?
Diminution albumine̝mie
Augmentation α1-globulines
Diminution α2-globulines
Normalisation β-globulines
Augmentation γ-globulines
82) Vous recevez en consultation une femme noire de 28 ans pour amaigrissement et asthe̝nie. Elle est marie̝e sans enfant. Le poids est de 43 Kg pour taille 157cm, la tension arte̝rielle est 130/87 mmHg et poules 102 par fre̝quence respiratoire 25/min SpO2 97% en air ambiant. Le cliche̝ de radiographie thoracique re̝vèle des opacite̝s hilaires et interstitielles bilate̝rale. Vous pensez à une sarcoïdose. Quelle est l’anomalie de la tomodensitome̝trie thoracique la plus adapte̝e le syndrome de Lofgren stade 1 de la sarcoïdose ?
Ade̝nopathie intrathoracique, bilate̝rale non compressives
Ade̝nopathie intrathoracique et opacite̝ interstitielle diffus
Opacite̝ interstitielle diffus micronodule ou reticulo-nodulaie
Fibrose pulmonaire avec possibilite̝ de le̝sions re̝tractiles
Bronchiectasie localise̝e et le̝sion bronchique surinfecte̝e
83) Mr. Q., 52 ans vous est adresse̝s par son me̝decin ge̝ne̝raliste. Il se plainte de douleur du membre supe̝rieur droit à type de de̝charges e̝lectriques, qui surviennent le plus souvent la nuit et re̝sistent aux antalgiques usuels (Voltarène et Doliprane). Ces douleurs inte̝ressent la face ante̝ro-interne de l’avant- bras droit ainsi que 2 derniers doigts. Vous observez une amyotrophie de l’e̝minence hypothe̝nar. Mr. Q. Vous signale e̝galement une toux apparue depuis 3 mois accompagne̝e d’une une grande asthe̝nie et amaigrissement. C’est un patient tabagique à 30 PA. Il vous apporte une radiographie thoracique re̝vèle effectue̝e en ville. Quel est l’e̝le̝ment retrouvez-vous sur le cliche̝ de radiographie thoracique?
Opacite̝ lobe moyen
Opacite̝ de l’apex
Syndrome bronchique
Lyse osseuse
Ade̝nopathie me̝diastinale
84) Vous recevez un homme âge̝ de 57 ans en hospitalisation pour une masse tumorale du me̝diastin poste̝rieur dans un contexte des douleurs thoraciques apparue re̝cente. Il fume 50 paquet-anne̝e. L’examen clinique : conscience normal, la tension arte̝rielle 145/76 mmHg la fre̝quence respiratoire 24 par min, SpO2 94% en air ambiant. Quel examen paraclinique de re̝fe̝rence pour ce patient?
Echographie transthoracique
Radiographie thoracique profile
Tomodensitome̝trie thoracique
Scintigraphie perfusion
Imagerie re̝sonnant magne̝tique
85) Vous recevez un homme âge̝ de 27 ans en hospitalisation pour une masse me̝diastinale ante̝rieur moyenne dans un contexte d’une oppression thoracique. Il n’a pas ante̝ce̝dent, il ne fume pas. L’examen clinique : conscience normale, la tension arte̝rielle 125/76 mmHg la fre̝quence respiratoire 24 par min, SpO2 97% en air ambiant. Quel examen physique extra thoracique le plus recherche̝ ?
Palpation air ganglionnaire
Inspection veines jugulaire
Auscultation souffle vasculaire
Inspection hippocratisme digital
Palpation des testicules
86) Vous recevez un homme âge̝ de 27 ans en hospitalisation pour une masse me̝diastinale ante̝rieur moyenne dans un contexte d’une oppression thoracique. Il n’a pas ante̝ce̝dent, il ne fume pas. L’examen clinique : conscience normale, la tension arte̝rielle 125/76 mmHg la fre̝quence respiratoire 24 par min, SpO2 97% en air ambiant, sans alte̝ration de l’e̝tat ge̝ne̝ral. Quel marqueur tumoral ou biologique le plus dose̝?
PSA
ACE
Immunoglobuline
β-2 microglobuline
β hCG
87) A 5 ans, fille est amene̝e au service d'urgence en De̝cembre par sa mère, qui se plaint que sa fille semble confuse. La mère signale que sa fille se plaint de maux de tête intermittents puisque les deux d'entre eux de̝place̝s dans le premier e̝tage d'un immeuble ancien il y a 6 mois. La mère a e̝te̝ à la maison avec la fille au cours des dernières 24 heures et la jeune fille semble le̝thargique et se plaint de douleurs articulaires, des nause̝es et des maux de tête. Son pouls est de 120 / min, la pression arte̝rielle est 130/85 mm Hg, fre̝quence respiratoire est de 25 / min, et la saturation en oxygène est de 100% à l'air ambiant. La mère de la fille note e̝galement avoir un le̝ger mal de tête qui a commence̝ hier. Lequel des tests de diagnostic suivants devraient être poursuivis le plus rapidement?
Des gaz du sang arte̝riel C
T scan de la tête
Laryngoscopie directe
ECG
E̝cran de toxicologie
88) Un homme 67 ans, pre̝sente à son me̝decin pour se plaintes de dyspne̝e à l'effort au cours des 6 derniers mois qui a progressivement de dyspne̝e au repos. Il nie la toux et une respiration sifflante et n'a pas eu de la fièvre, des sueurs nocturnes, perte de poids involontaire. Il n'a jamais fume̝ et travaille̝ comme un constructeur de navires pour> 30 ans.Laquelle des conclusions suivantes sur radiographie thoracique serait confirme̝ le diagnostic le plus probable?
Infiltrats diffus bilate̝raux
Ade̝nopathie hilaire bilate̝rale
Consolidation du tissu pulmonaire
De masse focale avec bronchogrammes ae̝riens
Des plaques pleurales multiples avec parenchymateuse ine̝gale opacite̝s
89) A 5-month-old child presents to Emergency Department with a reduced conscious level. No history of trauma, but he appears neglected. No physical injury is identified on clinical examination. A CT head is performed. Which one of the following is the most common intracranial finding in non-accidental injury?
Hydrocephalus
Intra-cerebral hemorrhage
Loss of gray-white matter differentiation
Subdural hematoma
Tumor
90) A 7-year-old boy has fallen on an outstretched hand and complains of a painful right elbow. When reviewing the radiographs for evidence of bony injury, which one of the following statements is true?
Posterior fat pad may be a normal finding on flexed lateral view
An anterior fat pad is always abnormal
The line from the anterior cortex of the humerus should pass through the anterior third of the capitellum
the radiocapitellar line should intersect on all views
The radiocapitellar line should not intersect on all views
91) A newborn delivered by cesarean section shows signs of respiratory distress soon after birth. A chest radiograph is performed. Which one of the following features favors the diagnosis of transient tachypnea of the newborn (TTN)?
A ground glass opacities throughout both lungs
Hyper inflated lung
Loss of lung volume
The presence of a pleural effusion
Hypo-inflated lung
92) A 4-week-old male neonate presents with milky vomiting and a hypochloraemic alkalosis. Hypertrophic pyloric stenosis is suspected and ultrasound is performed. Which one of the following ultrasound findings would confirm the diagnosis?
A pylorus that does not open
Pyloric canal length of greater than 11mm
Pyloric muscle wall thickness of 1mm
Transverse pyloric diameter of greater than 11mm
Transverse pyloric diameter of lower than 5mm
93) A 4-year-old child presents with upper back pain. Hepatomegaly and blood tests show iron deficiency anemia. Chest radiograph demonstrates an abnormal mediastinal contour, and CT confirms an 8-cm posterior mediastinal mass which contains calcifications. The lungs are clear. Which one of the followings is most likely the diagnosis?
Extramedullary hematopoiesis
Lymphoma
Neuroblastoma
Teratoma
Neproblastoma
94) A 6-month-old child with palpable abdominal mass. Ultrasound is revealing a mixed echogenic mass in the left kidney. CT demonstrates a large mass within the left kidney which has a moderate enhancing component. Which one of the following would be the most likely diagnosis?
Angiomyolipoma
Lymphoma
Neuroblastoma
Wilm’s tumor
Angioma
95) A 3-month-old infant with failure to thrive and tachypnea. No evidence of central or peripheral cyanosis. A chest radiograph shows enlarged central and peripheral pulmonary vessels throughout both lungs. Which one of the following is a potential diagnosis?
Pulmonary stenosis
Tetralogy of Fallot
Tricuspid atresia
Ventricular septal defect (VSD)
Patent ductus
96) Interstitial lung disease is suspected in a 3-year-old child who has a long history of breathlessness on exertion. A chest radiograph reveals interstitial change at the lung base. The clinical symptoms are more severe that the radiographic changes appear to suggest and a diagnosis is yet to be established. Which one of the following would be the next appropriate investigation?
Bronchoscopy
Contrast-enhanced CT of the chest
HRCT (high resolution CT)
MRI
X-ray
97) A 2-week-old baby presents with poor feeding and bilious vomiting. Malrotation is suspected and an upper GI contrast study (TOGD) is requested. What specific radiological finding would confirm the diagnosis?
Corkscrewing’ appearance of the duodenum and jejunum
On the supine radiograph the D-J flexure lies to the left of the midline
On lateral view the D-J flexure is posterior
On the supine radiograph the D-J flexure lies above the duodenal bulb
Corkscrewing’ appearance of the duodenum and colon
98) A 5-year-old child presented 1 week ago with bacterial meningitis and is now persistently pyrexial with new onset seizures. A CT head with contrast injection shows frontal leptomeningeal enhancement, with hypodense material within the subdural space, but hyperdense to CSF. What is the most likely diagnosis?
Cerebral abscess
Cerebritis
Subdural empyema
Ventriculitis
Tumor
99) A 3-month-old infant with Tetralogy of Fallot is waiting surgery. A pre-operative chest radiograph is performed when the child has no current illness. Which one of the following features are you most likely to see?
Boot-shape heart
Enlarged hila
Pulmonary plethora
Splaying of hila
Normal heart
100) A 2 week-old septic neonate shows worsening renal function and proteinuria. Seven days after his initial illness, an ultrasound is performed which reveals a unilateral enlarged kidney, with loss of corticomedullary differentiation and reversal of end-diastolic arterial flow. Associated adrenal hemorrhage is noted. What is the most likely diagnosis?
Acute glomerulonephritis
Acute tubular necrosis
Renal vein thrombosis
Renal artery stenosis
Renal vein stenosis
101) A 12-year-old child with CF (cystic fibrosis) had been followed up with annual chest radiographs. Which of the following features is a late radiographic change associated with the disease?
Cavitation
Diffuse interstitial patters
Hilar enlargement
Consolidation
Consolidation and cavitation
102) A neonate with a history of worsening cyanosis and respiratory distress has a series of chest radiographs taken. The initial chest radiograph reveals a solid left upper lobe mass and over the course of 3 weeks, this becomes aerated. The progressive mediastinal shift is seen as the mass enlarges. Which one of the following is the most likely diagnosis?
Congenital lobar emphysema
Congenital cystic adenomatoid malformation (CCAM)
Bronchopulmonary sequestration
Congenital diaphragmatic hernia
Traumatic diaphragmatic hernia
103) A 3-year-old boy presents with a short history of shortness of breath. Clinical examination is unremarkable, but on the chest radiograph there are multiple pulmonary nodules suggestive of metastases. Which one of the following tumors would be the most likely source of pulmonary metastasis?
Neuroblastoma
Meduloblastoma
Nephroblastoma (Wilm’s tumor)
Lymphoma
Benign tumor
104) A 4-year-old child presents with shortness of breath and fever. The chest radiograph shows a round opacity within the right lower lobe. No previous chest radiographs are available for comparison. Which one of the following statements is true when trying to distinguish pneumonia from a tumor in a child?
Sharp margins are associated with pneumonia
The absence of an air bronchogram makes tumor lore likely
Ill-defined margins make pneumonia more likely
An MRI would be the next investigation of choice
A CT would be the next investigation of choice
105) A newborn baby is hypoxic immediately following delivery. There is evidence of meconium-stained amniotic fluid. Which one of the following statements is true regarding meconium aspiration syndrome?
The chest radiograph typically shows patchy consolidation with areas of hyperinflation
The chest radiograph typically shows a fine ground glass appearance
Pneumothorax and pneumomedianum are uncommon complications
Radiological resolution is usually seen within 48-72hours
Normal chest x-ray
06) A 5-year-old boy is involved in traffic accident and is complaining of neck pain. Which of the following statements is true regarding the cervical spine radiograph?
Subluxation of up to 7mm of C2 anteriorly on C3 is normal
Subluxation of up to 3mm of C2 posteriorly 0n C3 is normal
The soft tissues anterior to C2 must be no wider than 1/4 of the width of the C2 vertebral body
The distance between the anterior arch of C1 and the dens can be up to 5mm
The soft tissues anterior to C2 must be no wider than 1/2 of the width of the C2 vertebral body
107) A neonate presents at 24 hours old with vomiting, abdominal distension and failure to pass meconium. A series of investigations are performed. Which of the following would be in keeping with a diagnosis of meconium ileus?
A contrast enema showing pellets of meconium within the terminal ileum
A contrast study showing narrow loops of proximal ileum
A contrast enema showing a dilated terminal ileum
A plain abdominal radiograph (ASP) showing a soap bubble appearance within the left iliac fossa
A contrast study showing dilated loop of proximal ileum
108) Following a recent viral illness, a 5-year-old girl presents with a fluctuating conscious level, seizures and left leg weakness. She is apyrexial and does not have a rash. An MRI is performed. This shows bilateral areas of increased T2 signal in the subcortical white matter and cerebellum and deep grey matter. Which one of the following is the most likely diagnosis?
Bacterial meningitis
Viral encephalitis
Multiple sclerosis
Acute disseminated encephalomyelitis (ADEM)
Fungus meningitis
109) A 3-day-old neonate demonstrates signs of respiratory distress. A chest radiograph demonstrates a right pleural effusion. Which one of the following is the commonest cause?
Hydrops fetalis
Meconium aspiration syndrome
Pulmonary hemorrhage
Chylothorax
Pulmonary embolism
110) An 8-month-old child who was previously well presents with vomiting and altered conscious level. A CT head reveals significant hydrocephalus with a hyperdense mass. An MRI is arranged and reveals a lobulated mass adjacent to the trigone of lateral ventricles. The lesion yields low signal on both T1w and T2w sequences with avid enhancement postcontrast. Which one of the following is likely the most likely diagnosis?
Craniopharyngioma
Meningioma
Ependymoma
Choroid plexus tumor
Hydrocephalus
111) A 6-year-old boy presents with a right-side limp of a few week’s duration. He is apyrexial. Which one of the following is the earliest radiographic sign that would support a diagnosis of Perthes’disease of the hip?
Fragmentation of the femoral head
Hip effusion
A subchondral lucency
Sclerosis of the femoral head
Necrosis of the femoral head
112) A 5-year-old child presents with vomiting, lethargy and a persistent headache. A CT head is performed and shows a hyperdense midline posterior fossa mass, abuting the fourth ventricle with associated hydrocephalus. There is significant peritumoral oedema but no calcification, and avid homogenous enhancement is seen postcontrast. Which one of the following posterior fossa tumors is the most likely diagnosis?
Meduloblastoma
Ependymoma
Pilicystic astrocytoma
Cerebellar heamangioma
Hydrocephalus
113) A 3-year-old girl presents with a purpuric rash, abdominal pain and blood-stained stools. Henoch- Schönlein purpura (HSP) is the clinical diagnosis. Which one of the following statements is true when investigating this girl?
An ultrasound is of little diagnostic use
If an intussusception is seen it is likely to be difficult to reduce
An ultrasound finding of hypoechoic, thickened bowel wall would be supportive the clinical diagnosis
Involvement of the GI tract is seen in 10% of patients with HSP
An ultrasound finding of hyperechoic, thickened colon wall would be supportive the clinical diagnosis
114) An 11-year-old boy presents with right hip pain. He is apyrexial and the clinicians are concerned that he has a slipped femoral epiphysis (epiphysiolyse aseptique). Which one of the following would be appropriate first-line imaging?
AP and frogleg lateral radiographs of the pelvis
PA and frogleg lateral radiographs of the pelvis
Ultrasound of the hip
CT with 3D reconstruction of the affected hip joint
MRI with 3D reconstruction of the affected hip joint
115) A 10-year-old child presented 5 weeks ago with prolonged fever and headache with new onset seizures. A CT head pre-and post-contrast injection shows frontal isodense mass with peripheral enhancement centered by a calcification. What is the most likely diagnosis?
Cerebral abscess
Neurocysticercosis
Brain Tuberculoma
Brain tumor
Hydrocephalus
116) A 7-year-old girl presents with a fluctuating conscious level, seizures and contractures. Lumbar tab is consistent with viral encephalitis. An MRI is performed. This shows bilateral areas of increased T2 signal in the thalami. Which one of the following is the most likely diagnosis?
JEV encephalitis
HSV encephalitis
Bacterial encephalitis
HIV encephalitis
Viral encephalitis
117) A 6-year-old boy is involved in traffic accident and is complaining of headache and subsequently developed altered conscious level. Which one of the following investigations is appropriate in this condition?
CT head with contrast injection
CT head without contrast injection
MRI head
AP and Lateral view radiographs of the head
CT head with and without contrast injection
118) La radiographie du thorax de face chez une primo-infection tuberculeuse montre un foyer de condensation pulmonaire au lobe moyen droit, quelle le̝sion associe̝e la plus fre̝quente?
Cavitation
Pleure̝sie
Ade̝nopathie hilaire
Pneumothorax
Lignes septales
119) A 70-year-old man recently underwent a laparoscopic prostatectomy. He now presents to the Emergency Department complaining of shortness of breath, pleuritic chest pain and haemoptysis. D- dimer levels were measured and found to be significantly elevated. A CXR is performed as part of the initial set of investigations. Which one of the following is the most likely CXR finding?
A normal chest radiograph
Linear atelectasis
Localized peripheral oligaemia
Peripheral airspace opacification
Pleural effusion
120) A 27-year-old, previously fit and well man presents to his GP with a short history of pyrexia, cough and haemoptysis. He has never previously been admitted to hospital. Sputum culture has grown Streptococcus pneumoniae. What is most likely chest radiograph finding?
Bronchopneumonia
Cavitation
Empyema
Large pleural effusion
Lobar consolidation
121) A 7-year-old girl, who has recently migrated migrated to this country from India, presents with a productive cough, fever, night sweats and weight loss. A CXR demonstrates marked consolidation in the right upper lobe. Sputum cytology reveals the presence of acid-fast bacilli. What additional radiological finding is most likely to suggest a diagnostic of current primary tuberculosis as opposed to post-primary tuberculosis?
Cavitation
Mediastinal lymphadenopathy
Multifocal lesion
Ranke complex
Rasmussen aneurysm
122) A 30-year-old male engineer has recently returned from North America having inspected a number of construction sites. He develops flu-like symptoms and CXR reveals the presence of a solitary well- defined nodule. What additional finding would make a diagnosis of Histoplasmosis infection more likely, rather than Cryptococcus infection?
Air bronchograms
Cavitation
Central calcification
Lymphadenopathy
Pleural effusion
123) A 30-year-old man is HIV positive with a most recent CD4 count = 100 cells/μL. He presents to the infectious diseases team with a cough, dyspnea and general malaise. A CXR demonstrates bilateral, diffuse, medium-sized reticular opacities. An air-filled parenchymal cavity (pneumatocoele) is seen, but there is an absence of either mediastinal lymphadenopathy or a pleural effusion. What is the most likely underlying opportunistic infection?
Streptococcus pneumoniae
Cryptococcus neoformans
Cytomegalovirus
Mycobacterium avium complex
Pneumocystis carinii
124) A 50-year-old lifelong male smoker has presented to his GP with increasing shortness of breath. A CXR shows that the right atrial border is a little indistinct. On thee lateral view there is a triangular density with its apex directed towards the lung hilum. Which one of the following is the most likely diagnosis?
Left lower lobe collapse
Left upper lobe collapse
Right middle lobe collapse
Right lower lobe collapse
Right upper lobe collapse
125) A confused 70-year-old man with a history of cough and some shortness of breath attends your Radiology Department for a CXR. It is noted that there are multiple discrete, spherical and well-defined pulmonary nodules with a peripheral distribution. Some calcification is noted within some of these nodules but cavitation is not evident. The accompanying nurse from the care home tells you that he has a “growth” somewhere but is not sure what this is. What is the most likely primary tumour?
Adenocarcinoma of the colon
Anaplastic thyroid carcinoma
Chondrosarcoma of the femur
Invasive ductal carcinoma of the of the breast
Squamous cell carcinoma of the oesophagus
126) A 25-year-old male pedestrian has been hit by a car and is currently being resuscitated in the Emergency Department. He complaint of paraesthesia involving his left shoulder. Which one of the following radiological features is the most likely related cause?
Dislocated left sternoclavicular joint
Fractured left 2nd rib
Fractured left humerus
Left tension pneumothorax
Right anterior shoulder dislocation
127) A 27-year-old man has been involved in a high-speed road traffic accident. There is significant diagonal bruising over the abdomen, due to the wearing of a seat belt. He is heamodynamically stable, but complains of severe abdominal pain and a CT of the chest and abdomen is performed. Which one of the following radiographic sings on a CXR would be most likely to suggest a right-side diaphragmatic injury?
A nasogastric tube coiled within the left hemithorax
A right pleural effusion
Elevated left hemidiaphragm
Hollow viscera seen within the chest
Mediastinal shift towards the left
128) A 30-year-old warehouse employee has been admitted to the Emergency Department, having been crushed between a reversing lorry and a wall. A supine CXR demonstrates a pneumomediastinum and a right-side pneumothorax that has not responded to the insertion of an appropriately sited chest drain. The right lung is seen to sag towards the floor of the right hemithorax. Which one of the following is the most likely diagnosis?
Flail chest
Pneumopericardium
Ruptured oesophagus
Tracheobronchial rupture
Traumatic aortic rupture
129) A 41-year-old man has previously had a large anterior myocardial infarction. He now presents with increasing shortness of breath on exertion and it is suspected that he has a degree of pulmonary venous hypertension (PVH) due to left ventricular failure. Which one of the following is the most likely radiological finding?
A fine nodular parenchymal lung pattern if chronic PVH develops
Kerley A septal lines radiating from the hilum to the pleural surface
Kerley C septal lines seen at right angles to the pleural surface within the peripheral lower zones
Lower lobe pulmonary venous blood diversion
Relative thinning of bronchial wall thickness compared with normal subjects
130) A 56-year-old female smoker presents with increasing shortness of breath, fever and a productive cough. Her CXR demonstrates diffuse opacification at the right lung base and treatment is commenced for community-acquired pneumonia. Which additional radiological finding is most likely to suggest a diagnosis of Streptococcus pneumoniae rather than Staphylococcus aureus?
Air bronchograms
Cavitating nodules
Empyema
Pleural effusion
Scattered multifocal opacities
131) A 49-year-old man presents to his GP with increasing shortness of breath. A CXR demonstrates a “white out” of left hemithorax with displacement of mediastinum towards the left. What is the most likely explanation?
Diaphragmatic hernia
Extensive consolidation
Lung collapse
Mesothelioma
Pleural effusion
132) Whilst reporting plain radiographs from a respiratory outpatient clinic, you view a CXR that demonstrates bilateral hypertransradiant hemithoraces. The lung volumes are normal and, unfortunately, there is no clinical history accompanying the request card. Which diagnosis would best explain these finding?
Acute bronchiolitis
Asthma
COPD
Multiple pulmonary emboli
Tracheal stenosis
133) A CXR is performed on a 62-year-old man with a chronic cough. This demonstrates multiple tiny nodules throughout both lungs, measuring up to 2 mm in size. These micronodules appear to be of greater density than soft tissue. Which one of the following is the most likely diagnosis?
Coal worker’s pneumoconiosis
Miliary histoplasmosis
Miliary tuberculosis
Sarcoidosis
Silicosis
134) You are asked by the Emergency Department clinicians to review a trauma series of plain radiographs of a young man involved in a road traffic accident. The clinicians suspect that the patient has multiple right-sided rib fractures. Which one of the following is the correct radiological consideration as you review these films?
A double fracture of a single rib leads to a “flail segment”.
Fractures of the 1st to 3rd ribs imply a minor trauma.
If fractures of the 10th to 12th ribs are present, further imaging is likely to be required.
Rib fractures are commonly seen in children.
The supine chest radiograph is a sensitive screening test for rib fractures.
135) A 27-year-old woman has severe asthma. She is admitted to ITU with a severe, life-threatening exacerbation requiring mechanical ventilation. Two days later, a supine CXR is performed. This demonstrates a lucent line around the left heart border and aortic arch with surgical emphysema at the root of the neck. The lungs are hyperinflated but appear clear. Which complication is likely to have occurred?
Alveolar rupture.
Diaphragmatic rupture.
Oesophageal perforation.
Pneumothorax.
Tracheobronchial rupture.
136) A 43-year-old man is investigated for pain related to his left arm. Plain radiography demonstrates a well-defined, lytic lesion in the proximal humerus, with chondroid matrix mineralisation and a narrow zone of transition. There is deep endosteal cortical scalloping and the suggestion of bone expansion. What is the most likely diagnosis?
Chondroblastoma.
Chondroma.
Chondromyxofibroma.
Chondrosarcoma.
Osteochondroma.
137) A 32-year-old man attends hospital following a fall onto his flexed left arm. He is referred to the duty orthopaedic team with a “Monteggia injury”. What are the most likely radiological findings?
A fracture of the distal radius with an associated dislocation of the radial head.
A fracture of the distal radius with an associated disruption of the distal radioulnar joint.
A fracture of the distal ulna with an associated dislocation of the radial head.
A fracture of the proximal ulna with an associated dislocation of the radial head.
A fracture of the proximal radius with an associated disruption of the distal radioulnar joint.
138) A 27-year-old man is referred by his GP with progressively painful swelling of his left knee following a minor football injury some weeks ago. The radiograph shows a 5-cm ill-defined lytic lesion within the left distal femoral metaphysis, with a permeative pattern of bone loss and areas of cloud-like ossification. There is an extensive periosteal reaction, predominantly orientated perpendicular to the cortex. What is the most likely diagnosis?
Aneurysmal bone cyst.
Chondrosarcoma.
Ewing’s sarcoma.
Metastasis.
Osteosarcoma.
139) An 80-year-old woman is admitted to hospital following a fall. The patient had a right mastectomy and axillary dissection 5 years ago to treat an invasive ductal carcinoma. The pelvic radiograph reveals a left hip fracture. Which fracture site would be most suggestive of a pathological fracture?
Greater trochanter fracture
Intertrochanteric fracture of the left proximal femur.
Pertrochanteric fracture of the left proximal femur
Subcapital fracture of the left neck of femur.
Subtrochanteric fracture of the left proximal femur.
140) A 19-year-old student returns to the UK following 4 months’ travelling around the world. Radiographs reveal multiple oval areas of calcification, up to 1 cm in long axis, aligned in the direction of muscle fibres. What is the most likely diagnosis?
Cysticercosis.
Dracunculus (guinea worm) infection.
Hydatid disease.
Loiasis.
Schistosomiasis.
141) A previously well 80-year-old woman sustains a subcapital fracture of the right neck of femur following a fall onto hard ground. The plain film reveals multiple lytic lesions within the pelvic bones and proximal femora, which are highly suspicious for bone metastases. What is the most likely occult primary lesion?
Carcinoma of the bladder.
Carcinoma of the breast
Carcinoma of the bronchus
Carcinoma of the colon
Carcinoma of the stomach
142) A 34-year-old man with chronic back pain is referred by his GP for thoracic and lumbar spine radiographs. The GP is concerned about the possibility of ankylosing spondylitis. Which radiological feature is atypical for ankylosing spondylitis, and might suggest an alternative diagnosis?
Ankylosis of the apophyseal joints
Anterior longitudinal ligament calcification
Osteophyte formation
Sclerosis of the anterior corners of the vertebrae
Vertebral body squaring
143) A 50-year-old woman complains of painful swelling of the joints of the hands and wrists. Radiographs show evidence of an erosive arthropathy. Which radiological feature would favour a diagnosis of rheumatoid rather than psoriatic arthritis?
Early reduction in bone mineralisation.
Erosions of the terminal tufts of the distal phalanges
Joint ankylosis
Pencil-in-cup deformities of the middle phalanges
Periosteal reaction
144) An 18-year-old man attends his general practitioner with a painful right knee. His radiograph shows a well-defined, lobular, lytic lesion within the proximal tibial epiphysis, extending into the metaphysis. There is a faintly sclerotic margin and no matrix calcification. What is the most likely diagnosis?
Chondroblastoma
Chondromyxoid fibroma
Enchondroma
Giant cell tumour
Osteoid osteoma
145) A young girl is brought to the Emergency Department with a painful right elbow following a fall. The radiograph reveals that the radial head is ossified. Which other structure should be visible?
Capitellum
Internal epicondyle
Olecranon
Lateral epicondyle
Trochlea
146) A radiograph of the left knee of a 35-year-old man reveals a 3-cm lytic lesion sited eccentrically in the proximal tibia. It has a well-defined non-sclerotic margin, and extends to the tibial articular surface. What is the most likely diagnosis?
Aneurysmal bone cyst.
Chondroblastoma
Giant cell tumour
Non-ossifying fibroma
Osteoid osteoma
147) A 35-year-old woman is referred to thee Radiology Department following the birth of her first child. The baby was delivered 8 days post-term and was a vaginal delivery following a prolonged labour and episiotomy. Two months later, the patient continues to experience faecal incontinence and an anal sphincter tear is suspected. Which investigation would be most useful to demonstrate anal sphincter damage?
Barium evacuation proctogram
CT colonography
CT with rectal contrast media
Endoanal ultrasound
MRI of the pelvis with a body coil.
148) A 37-year-old man presents to his GP with increasing right upper quadrant pain. On examination, he is afebrile with right upper quadrant tenderness and fullness. An abdominal ultrasound is performed and demonstrates a 5-cm diameter cystic lesion in the right lobe of liver. The mass contains multiple septations with a large cyst centrally and multiple small cystic spaces peripherally. Echogenic debris is seen within the cystic lesion and alters in position when the patient lies on his side. From the clinical an sonographic details, what is the most likely diagnosis?
Amoebic abscess
Hydatid cyst
Pyogenic liver abscess
Simple liver cyst
Solitary metastasis
149) A 33-year-old woman presents to her GP with a one year history of intermittent rectal bleeding. She experiences regular episodes of fresh blood per rectum with associated lower abdominal pain, lasting several days at a time. A flexible sigmoidoscopy is normal. A double contrast barium enema is performed and demonstrates an irregular appearance of the anterior wall of the sigmoid colon with mild extrinsic mass effect. What is the most likely diagnosis?
Carcinoma of the sigmoid colon
Endometriosis
Pelvic lipomatosis
Radiation enteritis
Solitary rectal ulcer syndrome
150) A 56-year-old woman presents with a 4-day history of right upper quadrant pain and vomiting. She describes a previous episode one year ago that resolved after a few day. On examination, she is very tender in the right upper quadrant with guarding on deep palpation during inspiration. Laboratory investigations reveal elevated white cell count and CRP but normal liver function tests and an abdominal ultrasound is performed. What are the most likely ultrasound findings?
Hypoechoic mass in the pancreatic head with common bile duct measuring 14 mm and pancreatic duct measuring 6 mm in diameter
Nodular liver surface, mixed reflectivity liver texture and ascites
Severe intrahepatic duct dilatation with no cause identified
Several large gallstones with gallbladder wall measuring 5 mm and a rim of pericholecystic fluid
Several small gallstones with gallbladder wall thickness of 2 mm
151) An 82-year-old woman is referred to the on-call surgical team as an emergency admission. The patient lives in a residential care home and has a 48-hour history of generalised abdominal pain and vomiting. On examination, she is dehydrated and tachycardic and an abdominal radiograph demonstrates multiple dilated small bowel loops measuring up to 4.8 cm in diameter. A linear gas-filled structure is present in the right upper quadrant with short branches extending from it. What is the most likely diagnosis?
Acute mesenteric ischaemia
Emphysematous cholecystitis
Gallstones ileus
Obstructed right inguinal hernia
Small bowel obstruction due to adhesions
152) A 72-year-old man is referred to hospital as an emergency admission by his GP. He has experienced vomiting and abdominal pain for 24 hours following a takeaway meal. There is a past medical history of ischaemic heart disease, chronic obstructive pulmonary disease and hypertension. An abdominal radiograph is performed and demonstrates several gas-filled loops of small bowel centrally measuring up to 2.5 cm diameter. In the left side of the abdomen, multiple round foci of gas are projected over the wall of a loop of large bowel. No free gas or mucosal thickening is identified, what is the most likely explanation for the clinical and radiographic findings?
Gastroenteritis with incidental pneumatosis coli
Emphysematous pyelonephritis with a paralytic ileus
Ischaemic colitis causing intramural bowel gas
Perforated sigmoid diverticulitis with gas in the retroperitoneum
Small bowel obstruction due to a gallstone ileus
153) A 68-year-old woman presents with a 2month history of generalized abdominal bloating and two episodes of vaginal bleeding. On examination, the abdomen is distended with clinical evidence of ascites. Tumour makers are performed; CA 15-3 is normal, CA 125 and CEA are slightly elevated and CA 19-9 is markedly elevated. An abdominopelvic ultrasound demonstrates a moderate volume of ascites, multiple liver metastases and bilateral mixed solid/cystic adnexal masses. What is the most likely underlying primary tumour?
Breast cancer
Gastric adenocarcinoma
Melanoma
Ovarian cancer
Primary peritoneal carcinoma
154) A 27-year-old man is referred to the hepatology outpatient clinic with a 3-week history of malaise, lethargy and mild upper abdominal pain. Liver function tests performed by his GP are significantly abnormal. The results of hepatitis serology performed in the clinic are consistent with an acute hepatitis B infection. An abdominal ultrasound is performed. What is the most likely finding on ultrasound?
Decreased reflectivity of the liver parenchyma
Increased reflectivity of the liver parenchyma
Nodular liver surface
Normal ultrasound appearances
Retrograde portal venous flow
155) A 32-year-old man presents to his GP with increasing pain on swallowing solids and liquids. He has lost 15 kg in weight over the preceding 2 months. After a full history and examination, he is found to be HIV positive with a very low CD4 count. The GP refers him for a barium swallow examination and this demonstrates a single ulcer in the mid-oesophagus. The ulcer has a smooth margin, measures 4 cm in length and is oval in shape. There is no stricture identified. Which diagnosis is most likely?
Candida oesophagitis
CMV oesophagitis
Intramural pseudodiverticulosis
Oesophageal lymphoma
Squamous cell carcinoma of the oesophagus
156) A 49-year-old woman has experienced increasing difficulty swallowing over the past 6 months, with associated retrosternal discomfort. A barium swallow is performed and demonstrates virtually no peristaltic activity within a dilated oesophagus. The gastro-oesophageal junction appears widened and there is marked reflux of barium when the patient lies supine. An upper GI endoscopy shows moderate reflux oesophagitis. Given these findings, what is the most likely underlying diagnosis?
Achalasia
Oesophageal web
Presbyoesophagus
Scleroderma
Squamous cell carcinoma of oesophagus
157) A 30-year-old man attends the Emergency Department with a 2-day history of abdominal pain and vomiting. On examination, he is afebrile with a firm mass palpable in the right lower quadrant of the abdomen. A supine abdominal radiograph is performed and demonstrates dilated loops of small bowel with a large soft tissue mass in the right lower quadrant. On ultrasound, the mass has a “pseudotumour” appearance. What is the most likely diagnosis?
Colonic carcinoma
Gallstone ileus
Intussusception
Psoas abscess
Strangulated femoral hernia
158) A 49-year-old man is involved in a road traffic accident and sustains serious head and chest injuries. He is ventilated on the intensive care unit and his injuries are managed conservatively. Ten days later, he develops a temperature of 39.5°c, becomes tachycardic and requires inotropic support to maintain his blood pressure. An abdominal ultrasound is performed and shows a cystic structure in the right upper quadrant measuring 12 x 8 cm in size. The mass has a 6-mm thick wall, contains a layer of echogenic material and is surrounded by a rim of fluid. What is the most likely diagnosis?
Acalculous cholecystitis
Acute cholangitis
Gallbladder haematoma
Traumatic hepatic artery pseudoaneurysm
Xanthogranulomatous cholecystitis
159) A 40-year-old male diabetic patient has an intravenous urogram (IVU) for left-sided renal colic. On the IVU, the left kidney shows papillary and calyceal abnormalities that give an “egg in a cup” appearance at some calyces and “tracks and horns” at other calyces. The affected left kidney has preserved renal cortical thickness despite the calyceal/papillary abnormalities. The contralateral kidney appears normal. What is the most likely diagnosis?
Acute pyelonephritis
Amyloidosis
Reflux nephropathy
Renal papillary necrosis
Xanthogranulomatous pyelonephritis
160) A 40-year-old female diabetic patient has right loin pain, vomiting and a fever. An ultrasound examination is requested to exclude urinary obstruction. This demonstrates no evidence of upper tract dilatation, but features of acute pyelonephritis are present. What are the most likely sonographic findings within the right kidney?
Focal areas of reduced reflectivity in the renal parenchyma
Focal atrophy of segments of the right kidney
Increased echogenicity of the renal calyces
Enlarged right kidney and diffusely hyperechoic parenchyma
Shrunken right kidney and diffusely hyperechoic parenchyma
161) A 55-year-old HIV-positive man presents with macroscopic haematuria and right-sided renal colic. An IVU does not demonstrate any renal tract calcification, but there is a dense right nephrogram with no excretion of contrast on a delayed film. The urologist performs a retrograde ureteroscopy and retrieves a 9-mm right ureteric calculus. What is the likely composition of the calculus?
Calcium oxalate
Cysteine
Indinavir phosphate
Struvite
Uric acid
162) A 29-year-old man has an IVU performed following an episode of haematuria. This demonstrates complete right-sided ureteric duplication. Which one of the following statements is true?
If present, an ectopic ureterocoele is usually related to the lower moiety ureter
The lower moiety ureter usually obstructs at the vesicoureteric junction
The upper moiety calyces are prone to vesicoureteric reflux
The upper moiety ureter is prone to ureteric obstruction
The upper moiety ureter usually inserts into the bladder superior to the lower moiety ureter.
163) A 27-year-old man with membranous glomerulonephritis presents with a 1-day history of right- sided flank pain and haematuria. An abdominal radiograph did not reveal any renal calcification but his renal function has significantly deteriorated over the past 24 hours. On ultrasound there is a large, oedematous right kidney with loss of the corticomedullary differentiation. On a subsequent IVU, there is a faint nephrogram with absent pelvicalyceal filling after 15 minutes. What is the most likely diagnosis?
Acute hydronephrosis
Acute pyelonephritis
Acute renal infarction
Acute renal vein thrombosis
Chronic pyelonephritis
164) A 24-year-old motorcyclist involved in a traffic accident presents to the Emergency Department with a broken leg and bruising over his left flank. He is found to have microscopic haematuria and fractures of the left 8th and 9th ribs. The patient is haemodynamically stable and clinicians suspect a left renal injury. Which one of the following imaging investigations is the most appropriate?
Abdominal ultrasound
Contrast-enhanced CT abdomen and pelvis
Emergency catheter renal angiography
Gadolinium-enhanced renal MRI
IVU
165) A 68-year-old man is involved in a traffic accident and sustains a pelvic fracture, head and limb injuries. Attempted urethral catheterisation in the Emergency Department is unsuccessful and a cystourethrogram is requested to exclude urethral injuries. Regarding urethral injuries, which one of the following statements is correct?
Anterior urethral injury is more commonly due to iatrogenic or penetrating trauma than to blunt trauma.
Cystography should precede a retrograde urethrogram in a patient with suspected urethral injury
In men, on digital rectal examination the prostate is lower than normal in patients with urethral trauma
Urethral injuries occur in 50% of major pelvic fractures.
Urethral injury due to blunt trauma more commonly affects the penile urethra
166) A 42-year-old man is referred for investigation of painless microscopic haematuria. An IVU is performed and demonstrates bilateral small areas of calcification within the kidneys on the control image. On the 5-min postcontrast IVU film, the calcification appears to lie within the collecting system. On ultrasound, there are numerous small hyperechoic rounded areas within the medullary pyramids, many of which cast an acoustic shadow. What is the most likely diagnosis?
Adult polycystic kidney disease
Hyperparathyroidism
Medullary sponge kidney
Primary hyperoxaluria
Sacoidosis
167) A 32-year-old man involved in a high-speed traffic accident is found to have blood at the urethral meatus and a high riding prostate during the secondary clinical survey. The examining doctor suspects a urethral injury. Which part of the urethra is most likely to be involved?
Bulbar urethra
Membranous urethra
Penile urethra
Penoscrotal urethra
Prostatic urethra
168) You are the radiologist reviewing the mammograms of a 56-year-old woman. When compared with her previous mammograms, areas of calcification previously seen within the left upper outer quadrant have now disappeared. Which of the following is not a possible explanation?
Breast surgery
Chemotherapy
Postmenopausal changes
Radiotherapy
Spontaneous resolution
169) A transvaginal ultrasound is performed on a 36-year-old woman with dysfunctional uterine bleeding. This demonstrates an enlarged globular uterus with a heterogeneous appearance of the myometrium. The myometrium contains diffuse echogenic nodules, subendometrial echogenic linear striations and 2- to 6-mm subendometrial cysts. Color Doppler demonstrates a speckled pattern of increased vascularity within the heterogeneous area of myometrium. What is the most likely diagnosis?
Adenomyosis
Endometrial polyposis
Gestational trophoblastic disease (GTD)
Stage 1A endometrial cancer
Uterine fibroid
170) A 52-year-old postmenopausal woman presents for her first screening mammogram. Within the right upper outer quadrant, there is a 2-cm well-defined, oval mass that has dense “popcorn” calcification within it and is surrounded by a thin radiolucent rim. On ultrasound, the mass is well defined and hyperechoic with areas of acoustic shadowing due to contained calcification. What is the most likely diagnosis?
Fat necrosis
Fibroadenoma
Hamartoma
Oil cyst
Papilloma
171) A 56-year-old woman is found to have a screen-detected breast cancer on her second screening mammogram. Two breast radiologists both agree that there is no evidence of malignancy on the previous mammograms, even in retrospect. Which one of the following statement best describes this interval cancer?
An interval cancer has a better prognosis, when compared with other screen-detected cancers.
This is known as a Type 1interval cancer.
This is known as a Type 2a interval cancer.
This is known as a Type 2b interval cancer.
This is known as a Type 3interval cancer.
172) A 42-year-old man with known Wegener’s granulomatosis develops haematuria. He has an abdominal ultrasound which reveals small, smooth kidneys with diffuse thinning of the renal parenchyma. The pelvicalyceal systems appear normal but there is an increased amount of renal sinus fat. What is the most likely diagnosis?
Bilateral vesicoureteric reflux.
Chronic glomerulonephritis
Medullary sponge kidney
Pyelonephritis.
Renal tuberculosis.
173) A 29-year-old man presents with a 4-hour history of sudden onset right loin pain, radiating to the right groin. The clinicians request an emergency IVU for suspected acute urinary obstruction. Which one of the following IVU features would be most consistent with acute urinary obstruction?
Absent right nephrogram and no evidence of contrast excretion on the right
An increasingly dense right nephrogram that remains present after 6 hours
An initially dense right nephrogram, which then resolves within 30 minutes
The right kidney being 10% longer than the left kidney
The right kidney being small with an irregular cortical surface.
174) A 35-year-old woman presents with a painless lump in the outer upper quadrant of her left breast. She is referred for an ultrasound examination of the left breast. Which of the following ultrasound findings would suggest a malignant rather than a benign breast mass?
A larger transverse than anterior-to-posterior diameter
Ill-defined echogenic halo around the lesion
Less than 1 cm in greatest diameter
Posterior acoustic enhancement
Uniform hyperechogenicity
175) An immunosuppressed 24-year-old man presents with left renal colic. He is referred for an IVU. The control film shows a gas containing, round lamellated mass within the urinary bladder. Postcontrast, there are multiple filling defects within the urinary bladder. What is the most likely cause of these appearances?
Blood clot
Bladder calculi
Cystitis
Fungal ball
Schistosomiasis
176) A 53-year-old woman is invited to attend a mobile breast-screening unit for routine screening mammograms. Which one of the following statements is correct regarding the standard mammographic projections (the mediolateral oblique (MLO) and craniocaudal (CC) views)?
A well-positioned CC view usually contains all the breast tissue.
A well-positioned MLO view rarely shows the nipple in profile because of the oblique compression.
On a well-positioned MLO the nipple should be at the lower border of the pectoralis minor.
The MLO view is taken with the radiograph beam directed from superomedial to inferolateral.
The pectoralis major muscle is demonstrated at the posterior border of a CC view in approximately 70% of individuals.
177) A 24-year-old man presents to his GP with increased urinary frequency. Physical examination is normal and he is referred for ultrasound. Transabdominal ultrasound demonstrates a cystic structure posterior to the urinary bladder and a TRUS is performed for further evaluation. TRUS reveals a midline anechoic structure in the posterior portion of the prostate gland, superior to the verumontanum. It does not communicate with either the bladder or the seminal vesicles. Which of the following is the most likely diagnosis?
Bladder diverticulum
External iliac artery aneurysm
Mullerian duct cyst
Seminal vesicle cyst
Urethral cyst
178) A 22-year-old woman presents to her GP with irregular menstrual periods. She is overweight with a body mass index of 32 and has excess body hair. Her LH/FSH ratio is elevated and her GP refers her for a pelvic ultrasound. Which one of the following findings are most likely to be present on ultrasound?
Enlarged, oedematous ovaries with multiple packed follicles and pelvic-free fluid.
Enlarged ovaries with multiple peripheral cyst
Normal appearances of the ovaries
Ovarian mass with mixed cystic and solid components
Ovaries replaced by multiple large cyst
179) A 5-year-old boy who had a coarctation of his aorta repaired 12 months ago requires follow-up. Which of the following imaging modalities is the gold standard?
Conventional angiography
CT
Echocardiogram
MRI
Plain radiograph
180) A 6-year-old boy presents with a right-sided limp of a few weeks’ duration. He is apyrexial. Which one of the following is the earliest radiographic sign that would support a diagnosis of Perthers’ disease of the hip?
A subchondral lucency
Fragmentation of the femoral head
Hip effusion
Periarticular osteopenia
Sclerosis of the femoral head
181) A 2-year-old has an elbow radiograph performed following a fall. Which one of the following epiphyses should be visible?
Capitellum
Medial epicondyle
None
Olecranon
Radial head
182) On a 20-weeks antenatal ultrasound, unilateral fetal hydronephrosis is detected. Which one of the following findings would confirm the diagnosis of renal pelvic dilatation (RPD)?
During the second trimester, the AP renal pelvis measures more than 3 mm
During the third trimester, the AP renal pelvis measures greater than 5 mm
Megaureters are present.
The AP renal pelvis measures greater than 25% of the longitudinal length of the kidney
The AP renal pelvis measures greater than 50% of the longitudinal length of the kidney
183) A 2-week-old septic neonate shows worsening renal function and proteinuria. He is currently being monitored on the pediatric ITU. Seven days after his initial illness, an ultrasound is performed which reveals a unilateral enlarged kidney, with loss of corticomedullary differentiation and reversal of end diastolic arterial flow. Associated adrenal haemorrhage is noted. What is the most likely diagnosis?
Acute glomerulonephritis
Acute tubular necrosis
Renal artery stenosis
Renal vein thrombosis
Unilateral obstruction
184) A 2-year-old child presents to Emergency Department with a greenstick fracture of the ulna. On the radiograph, there is evidence of an old fracture to the same limb and the history given by the parents is inconsistent. Non-accidental injury (NAI) is clinically suspected and a skeletal survey is performed. Which of the following fractures have a high specificity for NAI?
Fractures of multiple ages
Fracture of the middle third of the clavicle.
Fracture of the lateral third of the clavicle.
Linear skull fracture
Spiral humeral fracture.
185) A 33-year-old HIV-positive woman presents with increasing headache and confusion. On examination she is pyrexial and has left leg and right facial weakness. A CT head demonstrates multiple lesions measuring between 2 and 4 cm, which are predominantly situated at the corticomedullary junction. These lesions have a thin enhancing rim as well as associated oedema and local mass effect. Which one of the following is the most likely diagnosis?
Cryptococcosis
Histiocytosis
HIV encephalopathy
Multiple cerebral metastasis
Toxoplasmosis
186) A GP requests your advice regarding an 18-month-old girl whose mother has noticed that her left pupil appears white. The GP has performed ophthalmoscopy and is suspicious that there is a retinal mass. Which one of the following is the investigation of choice?
CT orbits
MRI orbits
Orbital radiographs
Repeat ophthalmoscopy by ophthalmologist
Ultrasound
187) A 19-year-old HIV-positive man is admitted with headache, confusion and disorientation. He is mildly pyrexial. A CT brain reveals multiple hypodensities, particularly in the brainstem and in the periventricular white matter. There is some ependymal enhancement postcontrast. What is the most likely cause for these findings?
CMV encephalitis
Cryptococcosis
HIV encephalitis
Toxoplasmosis
Tuberculosis
188) A 37-year-old woman is involved in a road traffic accident and sustains a severe head injury. Her CT head shows acute blood within the extradural, subdural and subarachnoid spaces. Which one of the following statements is true regarding extradural haematomas?
They are crescentic is shape
They are commonest in the temporoparietal region
They are rarely associated with a skull fracture
They are usually due to laceration of the middle cerebral artery
They commonly cross the cranial sutures
189) A 50-year-old man has a CT head after sustaining a head injury during a mechanical fall. The only positive finding is a large low attenuation lesion in the left middle cranial fossa, which is well defined, and of the same attenuation as cerebrospinal fluid (CSF). There is some thinning of the overlying temporal bone. Which one of the following is the most likely diagnosis?
Arachnoid cyst
Cerebral infarct
Colloid cyst
Dermoid cyst
Epidermoid cyst
190) Un patient de 60 ans vient vous voie pour un nodule he̝patique sur l’e̝chographie qui e̝voque un foie d’aspect granuleuse. Quel est votre aptitude pour la de̝marche diagnostic devant une suspicion de CHC?
Scanner avec infection en 3 temps, Alpha-foetoprote̝ine, rechercher infection virale.
Alpha-foetoprote̝ine, bilan he̝patique complet.
Ponction biopsie he̝patique, bilan pour recherche la possibilite̝ d’origine autre primitive.
Bilan de fonction he̝patique et Alpha-feotoprote̝ine.
Rechercher infection virale, Alpha-foetoprote̝rine, bilan de fonction he̝patique complet.
{"name":"DES PAGE 303-360", "url":"https://www.quiz-maker.com/QPREVIEW","txt":"Welcome to the Medical Knowledge Assessment quiz, designed to test your understanding of various medical topics ranging from cardiology to gastroenterology. This quiz features 190 questions that challenge your clinical reasoning and diagnostic skills.Comprehensive coverage of medical topicsMultiple choice format for ease of answeringIdeal for medical students, professionals, and enthusiasts","img":"https:/images/course7.png"}
More Quizzes
QCM PROF PART 2
114570
Med prof treatment
95480
Test 1
740
Discover Your Favorites!
7416
Ultimate Capitalization Practice - Test Your Skills
201032148
Which Suite Life on Deck Character Are You? Take the!
201025911
How Welsh Are You? Take the Ultimate Personality
201028322
What Are the Characteristics of Sound? Take Our!
201029582
Free Arabic Alphabet: Master Arabic Letters Fast
201030620
Free Developmental Psychology Knowledge Test
201023565
Free apps azdot gov Practice Test
201021846
Which Cuddle Position Are You? Free Personality
201025441